

Abstract
Purpose.
There is a lack of research on the association between identity concealment and mental health among sexual and gender minority (SGM) adolescents and how social support may attenuate this association. Further, research typically neglects the day-to-day variability in concealment experiences of SGM adolescents. Therefore, we examined the association between daily sexual orientation and gender identity concealment and positive and negative affect and the moderating role of family and peer support on this association among SGM adolescents.
Methods.
A 21-day daily diary study among 94 SGM adolescents (M age =16.10, SD = 1.50; 31.9% gender minority; 44.7% people of color) was conducted. Multilevel regression analyses tested the association between daily concealment and positive and negative affect and a cross-level interaction was used to assess the moderating effect social supports.
Results.
Daily concealment was associated with higher negative but not with positive affect. Family support was associated with lower daily negative affect but not with positive affect. Peer support was not significantly associated with negative or positive affect. Moderation results indicated that the association between daily concealment and negative affect was significant for adolescents who reported low or average levels of family support but was no longer significant for adolescents who reported high levels of family support.
Conclusions.
Daily identity concealment is positively associated with negative affect and that this association was attenuated by family support. Future research and interventions should target families to improve the lives of SGM adolescents and help reduce and eliminate mental health disparities.
Keywords: Concealment, Family support, Peer support, Sexual minority, Gender minority, Adolescents, Affect
Sexual and gender minority (SGM) adolescents report poorer mental health than their heterosexual and cisgender peers [1]. This disparity is often explained by the minority stress framework and its extensions [2,3], which states that SGM people experience chronic distal (e.g., discrimination) and proximal (e.g., expectations of discrimination, concealment) stressors related to their sexual or gender minority identity in addition to general stressors, which have detrimental health effects. One form of proximal minority stress is the concealment of one’s sexual or gender identity [2,3], which are described as a concealable stigmas [4]. Although there are differences in sexual and gender identity concealment, both groups may conceal their identity as a mean of safety or coping with stigma [3,4]. Considering that a recent meta-analysis found that concealing one’s sexual orientation especially impacts the mental health of young sexual minority people [5], a better understanding of how concealment affects the mental health of SGM adolescents is needed. Examining factors that are related to mental health among SGM adolescents is also important because poor mental health in adolescence negatively influences health later in life [6].
Concealment is often conflated with disclosure/outness. Concealment refers to the active prevention of one’s stigmatized identity from being known by others, while disclosure/outness is understood as the extent that one has revealed one’s stigmatized identity to others [7]. Thus, concealment is not only the absence of disclosure/outness, but the active prevention of disclosure/outness [8]. Studies often research disclosure/outness [7], despite that concealment is associated with negative health outcomes [8].
Focusing on the association between concealment and health, a recent meta-analytic study found a small positive association between sexual orientation concealment and internalizing mental health problems [5]. However, studies among sexual minority adolescents are scarce [5], even more so for gender minority adolescents, and do not often assess concealment [7]. For example, more disclosure was associated with lower mental distress among sexual minority youth [9] and more outness with less depressive symptoms among SGM youth [10]. Further, gender identity concealment was identified as a source of stress in a qualitative study among gender minority adults [11]. Thus, despite few empirical research on concealment among SGM adolescents, research suggests that concealment of one’s sexual or gender identity might negatively affect mental health. Although when it is done to prevent, for instance, discrimination or victimization, it could also be seen as a protective factor [12].
Studying concealment in adolescence is especially relevant because sexual orientation and gender identity exploration, disclosure, and concealment are a key part of this developmental period [6]. However, SGM adolescents may conceal or disclose their identities to different individuals at different time points in varying contexts [e.g., school, home; 13]. Thus, depending on the social context, SGM adolescents may conceal part their identity [14], resulting in variability in concealment on a day-to-day basis. However, research on concealment often uses a between-person approach, neglecting the day-to-day variability in concealment experiences and how this is associated with mental health among SGM people. Taking a within-person approach can deepen our understanding of the impact of daily variations in concealment on mental health among SGM adolescents.
As indicators of mental health, within-person research often assesses positive and negative affect, which represent orthogonal mood states with positive affect reflecting an enthusiastic active mood while negative affect reflects a mood of distress [15]. Although affect and depression are different constructs, low positive and high negative affect play a role in the development of depression and research has found that they are associated with depression [15]. A better understanding of factors that influence affect among SGM adolescents is therefore important to better understand health disparities in this population.
Social support
Social support is associated with better mental health [16]. Considering the vital role of parents and peers during adolescence [17], both are considered important sources of support for SGM adolescents. A recent literature review found that, in general, lower levels of social support were associated with higher levels of mental health problems among SGM adolescents [18]. Sexual minority youth that received social support from friends but not from parents reported poorer mental health than youth who received social support from both friends and parents [19]. Further, peer and especially parental support were inversely associated with depression among sexual minority youth [20], and parental support was associated to fewer depressive symptoms in a small sample of transgender youth [21].
Besides directly affecting mental health, parental and peer support may attenuate the adverse effects of minority stressors, such as identity concealment, on mental health [16,22]. However, research primarily focuses on social support’s buffering role against the effects of distal minority stressors (e.g., discrimination) on mental health [e.g., 24,25] but has not adequately studied how it may attenuate adverse effects of proximal stressors such as concealment. One cross-sectional study among sexual minority youth found that sexual orientation-specific support by family members and friends attenuated the relation between minority stress, including concealment, and emotional distress [22]. Although concealment might limit access to supports (e.g., avoidance of certain social supports in order to conceal one’s identity), on a daily basis, SGM adolescents might conceal part of their identity in one social context but are later that day able to receive support in a different social context, which can minimize the effect of concealment on mental health. Thus, limited research assesses how parents’ and peers’ support may moderate the relation between concealment and mental health among SGM adolescents.
The present study
We aimed to study the association between within-person identity concealment and positive and negative affect and how social support from family and peers moderated this association among SGM adolescents. We expected that daily experiences with concealment would be associated with greater negative affect and lower positive affect, despite that concealment might protect against the negative effects of, for instance, discrimination. Further, we expected that greater levels of social support from family and peers would attenuate the adverse effect of daily concealment on mental health. Specifically, we hypothesized that the associations between daily concealment and mental health would be attenuated for SGM adolescents with greater social support from family and peers compared to SGM adolescents with lower social support.
Methods
Procedures
Participants were recruited from the community in a Mid-Atlantic metropolitan city as part of a larger study of SGM adolescents’ wellbeing (Author citation). Adolescents were screened for inclusion criteria and potentially eligible youth were invited to an in-person meeting. Inclusion criteria were self-identification as lesbian, gay, bisexual, transgender, or queer (LGBTQ) and age 12 to 18 years old. Study procedures were explained and 18-year-old youth provided written consent and youth under 18 years of age provided written assent. Parental consent was waived to mitigate potential risks related to disclosure of one’s sexual orientation or gender identity. The second authors’ Institutional Review Board approved the protocol.
Ninety-six adolescents completed the baseline survey and were invited to participate in the daily diary portion of the study; 94 agreed to participate in the 21-day daily diary. Participants then received instructions for completing the daily diary surveys. They received an individual, personalized email with a link to their daily diary survey every evening at 7:30 p.m. and tailored feedback regarding their progress in the study. Participants received a reminder at 9:30 p.m. if they had not completed the survey. Uncompleted surveys expired at 5 a.m. the next morning and were considered missed reports. Participants were asked to reflect on the past 24 hours when completing the questions. Participants received daily incentives and a weekly bonus for participating in the form of gift cards. Detailed procedures are provided elsewhere (author Citation).
In total, 94 SGM adolescents ages 12 to 18 years (M = 16.10, SD = 1.50) participated in the study. Detailed demographic information is presented in Table 1.
Table 1.
Descriptive Statistics of Key Variables
| M (SD) / % | Min - Max | N missing (%) | |
|---|---|---|---|
| Positive affect1 | 1.52 (0.76) | 0.11 – 3.92 | 0 (0.0%) |
| Negative affect1 | 1.06 (0.65) | 0.11 – 3.60 | 0 (0.0%) |
| Concealment1 | 0.88 (1.05 | 0 – 4 | 0 (0.0%) |
| Support family | 17.72 (5.93) | 4 – 28 | 0 (0.0%) |
| Support friends | 20.64 (6.98) | 4 – 28 | 0 (0.0%) |
| Age | 16.1 (1.50) | 12 – 18 | 1 (1.1%) |
| Total number of days participated | 17.33 (4.28) | 1 – 21 | 0 (0.0%) |
| Sexual identity | 0 (0.0%) | ||
| Gay | 12.8 | ||
| Lesbian | 17.0 | ||
| Bisexual | 35.1 | ||
| Heterosexual | 0.0 | ||
| Queer | 10.6 | ||
| Pansexual | 16.0 | ||
| Asexual | 5.3 | ||
| Not sure | 3.2 | ||
| Gender identity | 0 (0.0%) | ||
| Cisgender male | 9.6 | ||
| Cisgender female | 58.5 | ||
| Transgender male | 12.8 | ||
| Transgener female | 0.0 | ||
| Genderqueer | 11.7 | ||
| Other gender identity | 7.4 | ||
| Sex assigned at birth | 0 (0.0%) | ||
| Male | 9.6 | ||
| Female | 90.4 | ||
| Race/Ethnicity | 1 (1.1%) | ||
| White | 54.3 | ||
| People of color | 44.7 | ||
| Reduced Lunch | 0 (0.0%) | ||
| No | 66.0 | ||
| Yes | 34.0 |
Note. M = mean. SD = standard deviation.
Mean levels over all days are given for within-person variables.
Measures
Concealment.
Daily concealment of sexual orientation and/or gender identity in the 21-day daily diary monitoring period was assessed with one-item (“I hid part of my LGBTQ identity from another person or other people”). The item was developed for this study based on prior measures of identity concealment [25–27]. The item was rated from 0 = not at all true to 4 = very true.
Social support from family and peers.
Participants completed the 4-item family (“My family really tries to help me” ”; α = .90) and 4-item peers (“I can count on my friends when things go wrong”; α = .95) subscales of the Multidimensional Social Support Scale at baseline [28]. Answer options ranged from 1 = very strongly disagree to 7 = very strongly agree and the sum score for each scale was calculated.
Daily positive and negative affect.
Items from the Positive and Negative Affect Scale (PANAS-X) assessed daily positive and negative affect [15]. Three items from the PANAS-X assessed positive affect (i.e., excited, proud, inspired) and eight items assessed negative affect (i.e., upset, guilty, scared, irritable, ashamed, nervous, jittery, stressed). Participants rated items using a 5-point scale from 0 = very slightly or not at all to 4 = extremely and the scales were averaged. A previous study using the same data set reported adequate between- and within-person alpha reliability coefficients for positive (αwithin = .63 and αbetween = .90) and negative (αwithin = .73 and αbetween = .94) affect (Author citation).
Covariates:
Total number of days participated in the daily diary study, sexual identity (0 = gay or lesbian, 1 = bisexual, queer, or pansexual, 2 = other (i.e., asexual and not sure), gender identity (0 = cisgender and 1= gender minority), sex assigned at birth (0 = male and 1 = female), race/ethnicity (0 = White and 1 = people of color), age, and reduced lunch (0 = no and 1 = yes) were assessed and included as covariates in the models.
Analytic strategy
Linear multilevel regression analyses were estimated in Mplus version 8.3 [29]. The within-person predictor was daily concealment and at the between-person level predictor variables were between-person level concealment (the average of daily concealment across all completed days), family support, peer support, sexual identity, gender identity, sex assigned at birth, race/ethnicity, age, reduced lunch, and the total number of days participated. Daily within-person concealment was centered at each participant’s mean, and between-person level concealment, family support, and peer support were centered at the overall mean [30]. The outcome variables were positive and negative affect and were predicted simultaneously in all models.
Four multilevel regression models were estimated. First, Model 0 included no predictor variables, in which the intraclass correlation (ICC) of positive and negative affect was calculated. Second, in Model 1, the direct effect of daily concealment on positive and negative affect was estimated, controlling for between-person level concealment, sexual identity, gender identity, sex assigned at birth, race/ethnicity, age, reduced lunch, and the total number of days participated. Third, in Model 2, family support and peer support were added as predictors in the model. Last, in Model 3, the cross-level interaction effects between family support and peer support with daily concealment were estimated. For significant interaction terms, simple slope analyses were conducted [31].
At the between-person level, there were missing data for race/ethnicity and age (see Table 1). At the within-person level, there were missing data for positive affect (n = 2), negative affect (n = 2), and concealment (n = 2). As missing data analyses indicated that data were missing completely at random (MCAR). Multiple imputation was used to take into account missing data [32]. Ten imputed data sets were estimated using the IMPUTATION option in Mplus. Data for skipped days were not imputed as participants were allowed to skip a day per study design.
Results
Table 2 presents the results from the linear multilevel regression analyses with positive and negative affect as outcome variables. The ICC obtained from Model 0 (not presented in Table 2) indicated that for positive affect 44.7% and for negative affect 56.9% of the variance can be explained by differences between participants. Model 1 indicated that on days on which participants concealed their sexual or gender identity they reported greater negative affect (b = 0.07, se = 0.02, p < .01); no significant association for positive affect was found (b = 0.01, se = 0.03, p = .87). Further, gender identity was associated with negative affect, in which gender minority adolescents had higher scores on negative affect compared to cisgender adolescents (b = 0.31, se = 0.14, p = .02); gender identity was not associated with positive affect (b = 0.13, se = 0.15, p = .40). In Model 2, receiving family support was associated with lower scores on negative affect (b = −0.03, se = 0.01, p = .02) but was not associated with positive affect (b = 0.01, se = 0.01, p = .63).
Table 2.
Results from Multilevel Linear Regression Analyses with Positive Affect and Negative Affect as Outcome Variables
| Predictors | Model 1 | Model 2 | Model 3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Negative affect | Positive affect | Negative affect | Positive affect | Negative affect | Positive affect | |||||||
| b | se | b | se | b | se | b | se | b | se | b | se | |
| Level 1 (within-person) | ||||||||||||
| Daily concealment | 0.07 | 0.02 | 0.01 | 0.03 | 0.07 | 0.02 | 0.01 | 0.03 | 0.07 | 0.02 | 0.00 | 0.03 |
| Level 2 (between person) | ||||||||||||
| Person level concealment | 0.10 | 0.06 | 0.00 | 0.07 | 0.09 | 0.06 | 0.00 | 0.08 | 0.09 | 0.06 | 0.00 | 0.08 |
| Support family | −0.03 | 0.01 | 0.01 | 0.01 | −0.03 | 0.01 | 0.01 | 0.01 | ||||
| Support peers | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 | 0.01 | ||||
| Sexual identity (Ref = Monosexual) | ||||||||||||
| Plurisexual | 0.02 | 0.16 | −0.05 | 0.16 | 0.06 | 0.15 | −0.06 | 0.16 | 0.05 | 0.15 | −0.07 | 0.16 |
| Other | 0.36 | 0.24 | 0.03 | 0.26 | 0.34 | 0.25 | 0.03 | 0.25 | 0.35 | 0.25 | 0.04 | 0.25 |
| Gender identity (Ref = Cisgender) | ||||||||||||
| Gender minority | 0.31 | 0.14 | 0.13 | 0.15 | 0.27 | 0.12 | 0.14 | 0.15 | 0.27 | 0.12 | 0.14 | 0.15 |
| Sex assigned at birth (Ref = Male) | ||||||||||||
| Female | −0.05 | 0.20 | −0.13 | 0.26 | −0.05 | 0.21 | −0.13 | 0.26 | −0.05 | 0.21 | −0.13 | 0.26 |
| Race/Ethnicity (Ref = White) | ||||||||||||
| People of color | −0.07 | 0.14 | −0.22 | 0.15 | −0.01 | 0.15 | −0.23 | 0.15 | −0.01 | 0.15 | −0.23 | 0.15 |
| Reduced Lunch (Ref = No) | ||||||||||||
| Yes | −0.19 | 0.13 | 0.01 | 0.19 | −0.27 | 0.14 | 0.03 | 0.20 | −0.27 | 0.14 | 0.03 | 0.20 |
| Age | −0.02 | 0.04 | 0.00 | 0.05 | −0.02 | 0.04 | 0.01 | 0.05 | −0.02 | 0.04 | 0.01 | 0.05 |
| Total number of days participated | −0.06 | 0.02 | −0.06 | 0.02 | −0.07 | 0.02 | −0.06 | 0.02 | −0.07 | 0.02 | −0.06 | 0.02 |
| Cross-level interaction | ||||||||||||
| Daily concealment × Support family | −0.01 | 0.00 | 0.00 | 0.01 | ||||||||
| Support peers | 0.00 | 0.00 | 0.00 | 0.00 | ||||||||
| Deviance | 6929.42 | 6919.85 | 6909.02 | |||||||||
| Decrease in deviance (compared with Model 2) | 10.83 (df = 2) p < .01 | |||||||||||
Note. Ref = reference group. Bold b’s indicate significance at p < .05
The results of the simple slope analyses for the cross-level interaction support family × daily concealment:
1 SD below the mean of family support: b = 0.14, se = 0.03, p < .01
Mean level of family support: b = 0.07, se = 0.02, p < .01
1 SD above the mean of family support: b = −0.05, se = 0.03, p = .86
The cross-level interaction effects between family support and daily concealment and peer support and daily concealment were added in Model 3 and resulted in a significant model improvement (χ2(2) = 10.83, p = .01). The interaction between family support and daily concealment was significant in predicting negative affect (b = −0.01, se = 0.00, p < .01; see Figure 1) but the interaction between peer support and daily concealment was not significant (b = 0.00, se = 0.00, p = .19; see Figure 2). Simple slope analyses were conducted to better understand the significant interaction between family support and daily concealment. The conditional effects of daily concealment on negative affect were tested for three levels of family support, one SD below the mean, at the mean, and one SD above the mean. Daily concealment was significantly associated with negative affect when family support was one SD below the mean (b = 0.14, se = 0.03, p < .01), at the mean (b = 0.07, se = 0.02, p < .01), but not when family support was one SD above the mean (b = −0.05, se = 0.03, p = .86). Thus, simple slope analyses indicated that family support buffers the association between daily concealment and negative affect. The cross-level interactions between family support and daily concealment and peer support and daily concealment were not significant in predicting positive affect.
Figure 1.
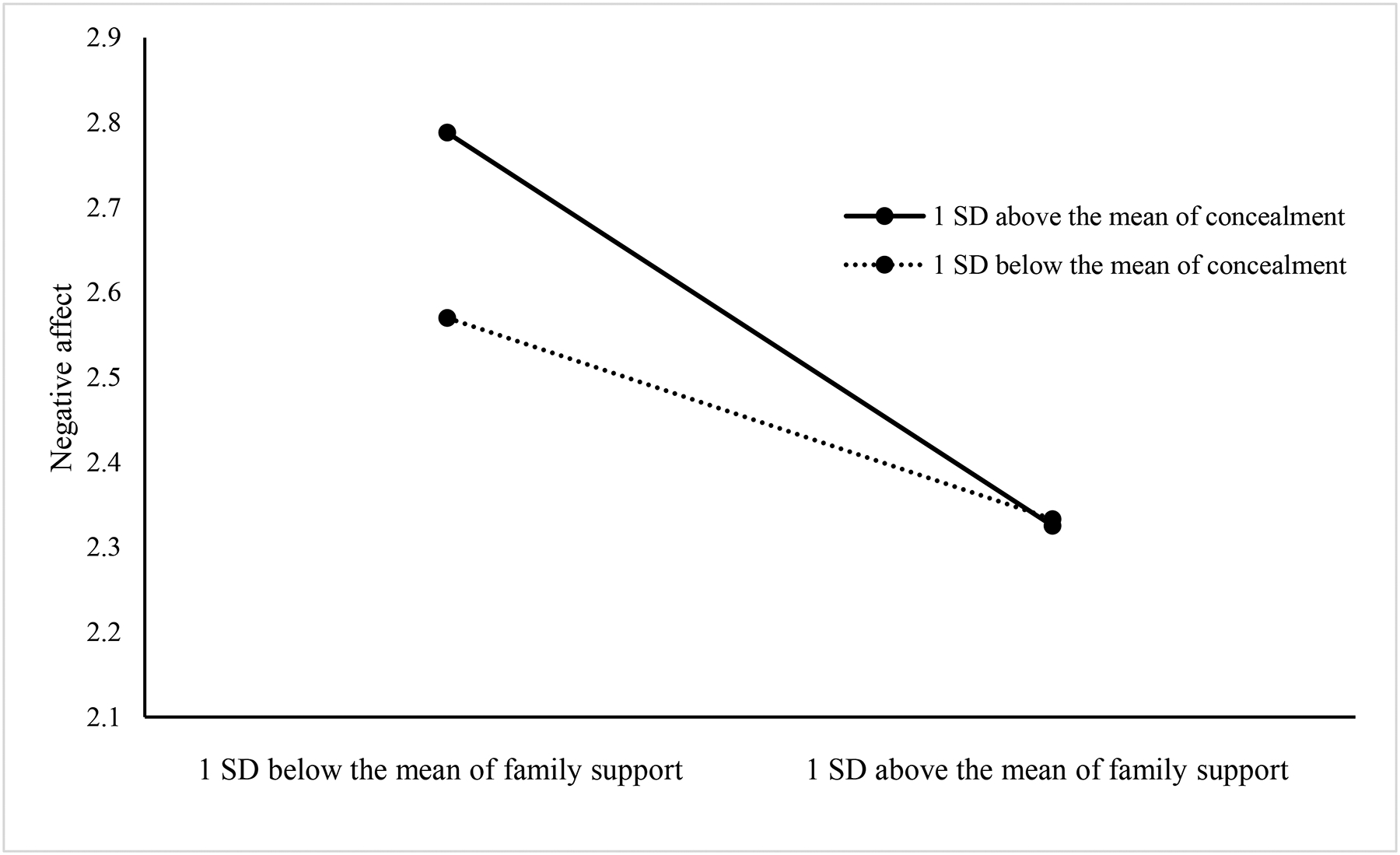
Visual representation of the Cross-level Interaction Effect for Concealment and Family Support
Figure 2.
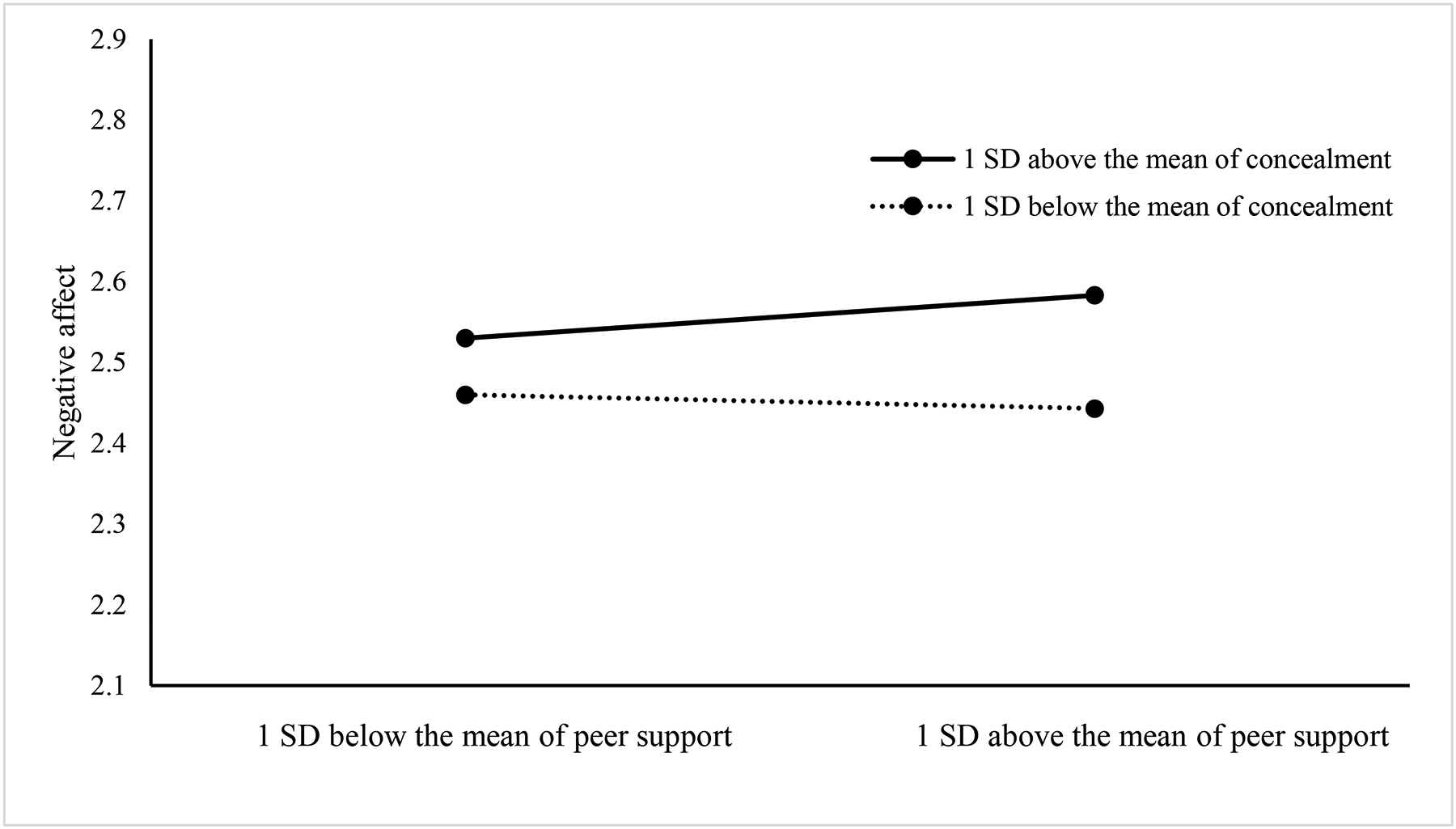
Visual representation of the Cross-level Interaction Effect for Concealment and Peer Support
Robustness check
Models were rerun separately for family support and peer support to assess independently how they moderate the association between daily concealment and positive and negative affect (see Table S1A and S1B in the online supplementary). Models yielded similar results compared to models in which the moderating effect of family support and peer support was assessed simultaneously.
Discussion
The aim of this study was twofold. First, we examined the within-person associations between daily identity concealment and positive and negative affect among SGM adolescents. Second, we tested if and how family and peer support attenuate the associations between concealment and positive and negative affect. As expected, the results indicate that daily concealment was associated with higher negative affect, however not with positive affect. This is in line with prior work on the association between concealment and mental health among sexual minority youth and adults [5] and extends these findings to SGM adolescents. Although not hypothesized, gender minority adolescents had higher daily negative affect over the daily diary monitoring period, which is consistent with previous studies that document poorer mental health for gender minority adolescents compared to their cisgender peers [33]. Further, family support was associated with lower negative affect, whereas peer support was not significantly associated with negative affect.
Our moderation results indicated that the association between daily concealment and negative affect was no longer significant when SGM adolescents reported higher levels of family support but was significant for adolescents who reported low or average levels of family support. This finding is crucial as it shows that having a supportive family may protect SGM adolescents from the negative impact of daily minority stress experiences, such as concealing one’s sexual or gender identity, on their mental health. Previous studies among sexual minority youth have also suggested that family support may attenuate the adverse effects of minority stress on mental health [22,24] We extend this literature by focusing on concealment, an understudied minority stressor among SGM adolescents, and move beyond cross-sectional studies by understanding the impact of fluctuations of concealment on mental health in the daily lives of SGM adolescents. These findings are informative for prevention efforts as they show that the family can play a role in coping with the adverse effects of minority stressors among SGM adolescents.
Although previous research points to the protective role of peer support [20,34,35], we did not find a direct association between peer support and positive or negative effect, nor did we find that peer support moderated the association between daily concealment and positive or negative affect. These null findings could be explained by the operationalization of peer support. We used a general measure of peer support. However, research among sexual minority people has distinguished between support for general life problems, referred to as general support, and support for sexual identity-related concerns (e.g., minority stress), referred to as sexual identity specific support [22]. Identity specific support may differently relate to SGM adolescent’s mental health. We also did not assess the sexual orientation or gender identity of peers, despite that sexual minority peers have been pointed to as especially important in providing sexual identity-specific support compared to heterosexual peers [22,36]. Thus, the type, quality, and source of support could influence the protective role of peer support on the association between daily concealment and affect. Future research should consider the type of support (general or identity specific) and the source of support (heterosexual and sexual minority; cisgender and gender minority) when studying peer support for SGM adolescents.
No significant associations between daily concealment and positive affect were identified. Our study adds to research that also found no significant associations between minority stressors and daily positive affect among adolescents and young adults [37,38]. It has been hypothesized that negative events are specifically associated with negative affect and not with positive affect [38], which could explain the lack of significant associations between daily concealment and positive affect in our study. Further, the present study included three out of the ten positive affect items [15], which might have biased our results. The null finding with regard to positive affect could also reflect that concealment was measured instead of disclosure. Concealment is often hypothesized to be associated with negative health outcomes, whereas disclosure is often hypothesized to be associated with positive health outcomes [8].
Although research indicates that concealment is associated with poorer health among SGM people [5], perceived stigma might confound this association. When SGM adolescents perceive an environment as more stigmatizing, they may be more likely to conceal their sexual or gender identity. Thus, perceived stigma may affect mental health and future work should study this confounding effect.
Lastly, although we tested social support as a moderator, social support could also be operationalized as mediator. By concealing one’ sexual or gender identity, it could be that one receives less sexual or gender identity related support, which is associated to worse mental health. Future research should study this mechanism to better understand how social support relates to mental health.
Limitations
The findings of this study should be interpreted in light of some limitations. First, our concealment measure conflated sexual and gender identity. Thus, we were not able to discern differences in the impact of sexual or gender identity concealment on positive and negative affect. Second, this study uses a community sample which may have biased the results. For example, the present sample primarily consisted of cisgender females but was relatively diverse concerning race/ethnicity, socioeconomic status, and sexual identity. Additionally, in nonprobability samples there is often an overrepresentation of sexual minority people who are out [5], making the sample less representative and potentially affecting the number of adolescents that concealed their sexual or gender identity. Future studies using probability samples are therefore needed to study the association between concealment and mental health. Third, despite the longitudinal design of the study, no inferences about causal associations can be made. Fourth, general family support was measured whereas previous studies often assess the role of parental support specifically [e.g., 21]. To better understand the importance of different family members in providing support, future research should assess support for specific family members. Fifth, we could not study the difference in association between daily concealment and mental health by sexual or gender identity. This is especially important considering that a recent meta-analysis showed that the association between concealment and internalizing mental health problems was smaller in bisexual samples [5] and differences for gender identity are currently understudied.
Conclusion
This study examined the within-person associations between daily concealment and positive and negative affect among SGM adolescents. Findings suggested that daily concealment is positively associated with negative affect and that this association was attenuated by family support but not by peer support. Future research and interventions that target families are needed to improve the lives of SGM adolescents and help reduce and eliminate their mental health disparities.
Supplementary Material
Implications and Contribution.
This study examined the associations between daily experiences of identity concealment and affect and how family and peer support buffered this association among sexual and gender minority adolescents. Daily concealment was associated with negative affect and this association was attenuated by family support.
Funding:
This work was supported by the National Institute on Alcohol Abuse and Alcoholism (K08AA025011 [PI: Mereish]). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
List of abbreviations:
- SGM
Sexual and gender minority
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of interest:
None to declare.
References
- [1].Fish JN, Baams L, McGuire JK. Sexual and gender minority health among children and youth. In: Rothblum ED, editor. Oxford Handb. Sex. Gend. Minor. Ment. Heal, Oxford University Press; 2020, p. 1–28. [Google Scholar]
- [2].Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol Bull 2003;129:674–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Hendricks ML, Testa RJ. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the minority stress model. Prof Psychol Res Pract 2012;43:460–7. [Google Scholar]
- [4].Pachankis JE. The psychological implications of concealing a stigma: A cognitive-affective-behavioral model. Psychol Bull 2007;133:328–45. [DOI] [PubMed] [Google Scholar]
- [5].Pachankis JE, Mahon CP, Jackson SD, et al. Sexual orientation concealment and mental health: A conceptual and meta-analytic review. Psychol Bull 2020;146:831–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Russell ST, Fish JN. Mental health in lesbian, gay, bisexual, and transgender (LGBT) youth. Annu Rev Clin Psychol 2016;12:465–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Meidlinger PC, Hope DA. Differentiating disclosure and concealment in measurement of outness for sexual minorities: The Nebraska Outness Scale. Psychol Sex Orientat Gend Divers 2014;1:489–97. [Google Scholar]
- [8].Jackson SD, Mohr JJ. Conceptualizing the closet: Differentiating stigma concealment and nondisclosure processes. Psychol Sex Orientat Gend Divers 2016;3:80–92. [Google Scholar]
- [9].Shilo G, Savaya R. Mental health of lesbian, gay, and bisexual youth and young adults: Differential effects of age, gender, religiosity, and sexual orientation. J Res Adolesc 2012;22:310–25. [Google Scholar]
- [10].Kosciw JG, Palmer NA, Kull RM. Reflecting resiliency: openness about sexual orientation and/or gender identity and its relationship to well-being and educational outcomes for LGBT students. Am J Community Psychol 2015;55:167–78. [DOI] [PubMed] [Google Scholar]
- [11].Rood BA, Maroney MR, Puckett JA, et al. Identity concealment in transgender adults: A qualitative assessment of minority stress and gender affirmation. Am J Orthopsychiatry 2017;87:704–13. [DOI] [PubMed] [Google Scholar]
- [12].Pasek MH, Filip-Crawford G, Cook JE. Identity concealment and social change: balancing advocacy goals against individual needs. J Soc Issues 2017;73:397–412. [Google Scholar]
- [13].Dewaele A, Van Houtte M, Cox N, et al. From coming out to visibility management-A new perspective on coping with minority stressors in LGB youth in Flanders. J Homosex 2013;60:685–710. [DOI] [PubMed] [Google Scholar]
- [14].Goldbach JT, Gibbs JJ. A developmentally informed adaptation of minority stress for sexual minority adolescents. J Adolesc 2017;55:36–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Watson D, Clark LA. The Panas-X. Man. postive Negat. Affect Sched form, vol. 277, The University of Iowa; 1994, p. 1–27. [Google Scholar]
- [16].Turner RJ, Brown RL. Social support and mental health. In: Scheid TL, Brown TN, editors. A handboook study Ment. Heal. Soc. Context. Theor. Syst, Cambridge University Press; 2010, p. 200–12. [Google Scholar]
- [17].Wreder, Kerr M, Stattin H, Biesecker G, et al. Relationships with parents and peers in adolescence. In: Lerner RM, Easterbrooks MA, Mistry J, editors. Dev. Psuchology Handb. Psychol Vol. 6, John Wiley & Sons; 2003, p. 245–62. [Google Scholar]
- [18].McDonald K Social support and mental health in LGBTQ adolescents: A review of the literature. Issues Ment Health Nurs 2018;39:16–29. [DOI] [PubMed] [Google Scholar]
- [19].McConnell EA, Birkett MA, Mustanski B. Typologies of social support and associations with mental health outcomes among LGBT youth. LGBT Heal 2015;2:55–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Watson RJ, Grossman AH, Russell ST. Sources of social support and mental health among LGB youth. Youth Soc 2019;51:30–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Simons L, Schrager SM, Clark LF, et al. Parental support and mental health among transgender adolescents. J Adolesc Heal 2013;53:791–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Doty ND, Willoughby BLB, Lindahl KM, et al. Sexuality related social support among lesbian, gay, and bisexual youth. J Youth Adolesc 2010;39:1134–47. [DOI] [PubMed] [Google Scholar]
- [23].Kaufman TML, Baams L, Dubas JS. Microaggressions and depressive symptoms in sexual minority youth: The roles of rumination and social support. Psychol Sex Orientat Gend Divers 2017;4:184–92. [Google Scholar]
- [24].Mustanski B, Newcomb ME, Garofalo R. Mental health of lesbian, gay, and bisexual youths: A developmental resiliency perspective. J Gay Lesbian Soc Serv 2011;23:204–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Balsam KF, Beadnell B, Molina Y. The daily heterosexist experiences questionnaire: measuring minoirty stress among lesbian, gay, bisexual, and transgender adults. Meas Eval Couns Dev 2013;46:3–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Larson DG, Chastain RL. Self-concealment: Conceptualization, measurement, and health implications. J Soc Clin Psychol 1990;9:439–55. [Google Scholar]
- [27].Testa RJ, Habarth J, Peta J, et al. Development of the gender minority stress and resilience measure. Psychol Sex Orientat Gend Divers 2015;2:65–77. [Google Scholar]
- [28].Zimet GD, Dahlem NW, Zimet Sara G, et al. The multidimensional scale of perceived social support. J Pers Assess 1988;52:30–41. [Google Scholar]
- [29].Muthén LK, Muthén BO. Mplus User’s Guide. 7th ed. Los Angeles, CA: 2012. [Google Scholar]
- [30].Enders CK, Tofighi D. Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychol Methods 2007;12:121–38. [DOI] [PubMed] [Google Scholar]
- [31].Stride CB, Gardner S, Catley N, et al. Mplus code for mediation, moderation, and moderated mediation models. Available at: http://www.offbeat.group.shef.ac.uk/FIO/mplusmedmod.htm.
- [32].Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychol Methods 2002;7:147–77. [PubMed] [Google Scholar]
- [33].Guz S, Kattari SK, Atteberry-Ash B, et al. Depression and suicide risk at the cross-section of sexual orientation and gender identity for youth. J Adolesc Heal 2021;68:317–23. [DOI] [PubMed] [Google Scholar]
- [34].Sheets RL, Mohr JJ. Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. J Couns Psychol 2009;56:152–63. [Google Scholar]
- [35].Shilo G, Savaya R. Effects of family and friend support on LGB youths’ mental health and sexual orientation milestones. Fam Relat 2011;60:318–30. [Google Scholar]
- [36].Mereish EH, Poteat VP. The conditions under which growth-fostering relationships promote resilience and alleviate psychological distress among sexual minorities: Applications of relational cultural theory. Psychol Sex Orientat Gend Divers 2015;2:339–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Mereish EH, Miranda R, Liu Y, et al. A daily diary study of minority stress and negative and positive affect among racially diverse sexual minority adolescents. Kournal Couns Psychol 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Mohr JJ, Sarno EL. The ups and downs of being lesbian, gay, and bisexual: A daily experience perspective on minority stress and support processes. J Couns Psychol 2016;63:106–18. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.