

Abstract
A number of minimally invasive spine surgeries (MISSs) have been developed to address the drawbacks of open spine surgery. Their advantages include small skin incisions, reduction in tissue damage, quick recovery, and short hospital stay. However, the clinical outcomes are comparable to open surgery. There was a cap on the number of indications that could be set for all spinal illnesses. The indications for MISSs have been expanding owing to mechanical and technological advances in medical equipment. Thus, this review presents the various MISSs developed to date, surgical indications, surgical techniques, and their advantages and disadvantages.
Keywords: Minimally invasive spine surgery, Microscopy, Endoscopy, Surgical navigation systems, Augmented reality navigation
Introduction
In the field of spine surgery, minimally invasive spine surgery (MISS) has advanced significantly in recent years [1-4]. It has clinical and radiological outcomes comparable to open spine surgery, can reduce approach-related harm (a drawback of open surgery), and preserves normal anatomy. Thus, postoperative recovery and return to regular life is quick [5,6]. The benefits of MISS include less bleeding during the procedure, quicker recovery period, and fewer postoperative complications [7].
The development of MISS may have begun with lumbar discectomy under a microscope [8,9], which led to numerous microscope-assisted surgical methods for decompression and fusion [1,10]. One of them is a combination of the use of an endoscope and a microscope that allows continuous saline irrigation and a larger surgical field of view, unlike the purely microscopic approach [11]. MISSs is further developed using technological advancements to involve navigation, robotics, and augmented reality (AR) [2-4]. In addition to neural decompression, surgeries for spine tumors, spine trauma, and fusion become possible, thus broadening the range of surgical indications. Implants used in spine surgery have been improved owing to advances in materials engineering, which makes access to challenging spinal pathologies easier by performing MISSs. In this review, we aimed to present the latest MISS trends and the indications, surgical approaches, strengths, and weaknesses of various MISSs.
Minimally Invasive Spine Surgery Techniques
1. Lumbar posterior decompression
Decompression or discectomy using the posterior route is necessary when conservative measures fail to relieve lumbar spinal stenosis, lumbar disk herniation, burst fracture, or spine metastasis [12-15]. Surgery can be performed using the traditional open surgical approach, although minimally invasive procedures have been increasingly gaining popularity [2]. The use of either an endoscope or a microscope is based on the discretion of the operator (Fig. 1). Despite the variations among different approaches, scars or fibrosis can be avoided postoperatively by avoiding damage to healthy tissues; the epidural blood supply can be maintained by safeguarding the epidural vessels via a minimally invasive approach compared with open surgery. Several studies have demonstrated the excellent clinical outcomes in surgeries employing a transforaminal approach or an interlaminar approach using a microscope and an endoscope. MISS is a viable option for treating lumbar disk herniation, lumbar spinal stenosis, and infectious spondylitis. In case of a massive herniated disk, it may be that severe fibrotic adhesion occurs from the previous surgery, or the bony structure deviates significantly from normal structure due to severe arthritic alterations; it may be challenging to perform MISSs. Therefore, to achieve an accurate patient evaluation, surgical indications for MISS should be considered before the surgery [16].
Fig. 1.
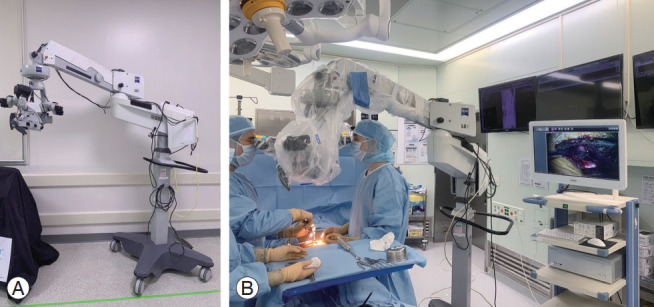
(A, B) Surgical field for minimally invasive spinal surgery using a microscope.
Endoscopic lumbar surgery can be performed using a single port or two ports, while microscopic lumbar surgery through a midline or paraspinal approach. The choice of surgical approach depends on the patient’s condition and the surgeon’s decision. The lumbar posterior approach involves two primary methods using an endoscope: the interlaminar approach used to treat spinal stenosis on both contralateral and ipsilateral sides and the transforaminal approach used to treat foraminal stenosis. Surgical difficulty can also be reduced by selecting an appropriate method based on the location and direction of disk herniation [17]. Therefore, surgical strategy should be appropriately established through precise assessment of the patient’s condition before the surgery [18,19].
Compared with open lumbar surgery, the minimally invasive lumbar posterior decompression surgery has the following disadvantages: steep learning curve, limited field of view, and narrow surgical field. Therefore, it is necessary to be completely familiar with the orientation of bony anatomy visually and to be able to feel the anatomical structures through tactile perception [20]. While it is not easy to perform MISSs well right from the beginning, the learning curve of surgeons practicing this may be improved, and with a larger field of view, good clinical results can be obtained through sufficient decompression and control of bleeding and normal tissue. With proper training, the advantages of MISS can be maximized while minimizing its disadvantages.
2. Lumbar interbody fusion
If the patient’s condition cannot be resolved with a relatively straightforward lumbar posterior decompression surgery, lumbar fusion surgery may be necessary. For example, decompression and fusion are required in case of segmental instability, a significant bone spur, severe arthritic alterations in the facet joints, or both spinal and foraminal stenosis. Sufficient decompression and fusion are possible with conventional posterolateral fusion (PLF) and posterior lumbar interbody fusion (PLIF). However, PLF has a risk of postoperative complications due to tissue injury and failure to remove the disk material; in PLIF, a reasonably large cage cannot be inserted. We present a minimally invasive lumbar interbody fusion technique that can compensate for this deficiency.
The transforaminal lumbar interbody fusion (TLIF) approach can directly decompress the neural foramen by removing the facet joint through direct approach to unilateral facet joint. In addition, access to the disk space is possible through this route, allowing discectomy and interbody cage insertion. Since the angle of insertion of the interbody cage is relatively gentle compared to the coronal orientation of human body, this technique allows insertion of a larger cage. TLIF can be performed through a minimally invasive approach using a microscope with a tubular retractor or an endoscope. Compared with PLIF, minimally invasive TLIF can minimize damage to structures that contribute to posterior stability such as interspinous ligaments, contralateral facet joints, and paravertebral muscles [21].
3. Posterior approach: transforaminal lumbar interbody fusion
In the microscopic TLIF (MI-TLIF) approach, the first step is to check the spinal level for surgery by fluoroscopy, as well as the coronal position of the pedicle for the intended approach site. The, a skin incision of approximately 1 cm is made on the lateral side of the pedicle and secured by gradually expanding the surgical field using a tubular retractor. In the endoscopic TLIF (E-TLIF) approach, the spinal level for surgery is confirmed by fluoroscopy and 1-cm incisions are made at disk levels cranial and caudal to the level intended for fusion. These serve as a viewing portal and a working portal. After bringing the camera and shaver tip together, tactile sense is used to recognize the approximate bony anatomy, and paravertebral muscle debridement is performed to an appropriate extent. When the target facet and lamina are exposed, the desired range of surgical field is secured through an appropriate approach for both MI-TLIF and E-TLIF. Facetectomy, ligamentum flavectomy, discectomy, and body endplate preparation are sequentially performed, similar to the sequence followed for open TLIF. Subsequently, a cage of appropriate size and a percutaneous bilateral pedicle screw are inserted.
Several studies have compared the surgical and clinical outcomes of traditional open TLIF, MI-TLIF, and E-TLIF. MI-TLIF and E-TLIF have reported similar fusion rates compared to open TLIF. Very few surgery-related complications include greater operation time, higher blood loss, delayed return to daily life, and longer hospital stay [22]. However, MI-TLIF has a high rate of rehospitalization and reoperation. Considering the steep learning curve for MI-TLIF, the advantage of this technique is not significant. Therefore, long-term studies are required to corroborate these findings.
4. Anterior approach: lateral lumbar interbody fusion and anterior lumbar interbody fusion
In 2001, an approach to the thoraco-lumbar interbody space through the retroperitoneal space was developed, and lateral lumbar interbody fusion (LLIF) was modified [23,24]. Approaches from the anterior psoas muscle and direct lumbar interbody fusion (DLIF) using the trans-psoas approach are some of the examples of these oblique lumbar interbody fusion advances [25]. Through the aforementioned methods, the anterior part of the vertebral column can be accessed laterally from the lower thoracic level to the lumbar level. However, in case of the L5–S1 level, the anterior part of the column is hidden by the iliac crest, which makes this lateral approach difficult due to proximity to various important structures such as the abdomino-pelvic vessels and lumbar plexus [26]. In such cases, the anterior lumbar interbody fusion should be considered: the retroperitoneal space is approached from the anterior aspect, and the interbody space is accessed through the interbody space where the iliac vessels are bifurcated. Through LLIF, a cage larger than that used in PLIF and TLIF can be used, several levels of disk space can be accessed with relatively small incisions. Not only is this approach effective for obtaining a corrective angle during surgery for adult spinal deformity, it is also applicable for patients who need correction due to lateral listhesis or those who need reoperation due to an adjacent spinal disorder [27,28]. However, LLIF may not be appropriate for patients who require direct neural decompression or large correction (severe stenosis of the central canal, severe foraminal stenosis, or severe spondylolisthesis). Therefore, the causative level should be accurately identified by careful analysis of the patient’s history before surgery and correlating it with radiographs and magnetic resonance imaging findings. Moreover, it is important to evaluate whether the iliac crest interferes with the surgical approach, whether there are anatomic variations in the abdomino-pelvic vessels, whether the position of these vessels interferes with access to the disk space, whether there is an anterior or lateral bony spur or bone bridge, and whether there is a previous retroperitoneal area. Surgical history should be checked carefully before the procedure to confirm the suitability of LLIF.
According to several studies, fusion rate following LLIF is 90%. The fusion rate between LLIF and MI-TLIF is not significantly different, but the complication rate is slightly higher in LLIF than in MI-TLIF, and clinical outcomes such as Visual Analog Scale pain score and Oswestry Disability Index score were reported to be low [24,27]. LLIF has the following complications: insufficient decompression due to the nature of the technique and neurologic deficits after surgery due to the presence of the lumbar plexus in the surgical field [23,27]. Insufficient decompression can be prevented by clearly establishing a surgical indication to determine if appropriate decompression can be achieved with the indirect method. Intraoperative neuromonitoring can prevent postoperative neurologic deficits.
Minimally Invasive Spine Surgery Technology
1. Endoscopy
MISS aims to minimize damage to normal tissues [29]. Compared with conventional open surgery, a small incision is initially made using a microscope, a narrow surgical field is secured using a tubular retractor or a Taylor retractor, and decompression or fusion surgery is performed using specialized instruments to obtain the desired result. In addition to the classic posterior approach, approaches involving a different direction such as LLIF and DLIF have been developed. The use of endoscope has been introduced in spine surgery, which is considered the most innovative development in the field. Due to many pioneering efforts to treat various spine diseases using an endoscope, the current endoscope-based technique has become a universal surgical method in spine surgery [15,30-32].
By endoscopy using a high-magnification camera, normal and pathologic structures can be clearly distinguished through an enlarged field of view [33-35]. In addition, unlike a microscope, various viewing angles such as 0°, 30°, and 70° can be applied. Thus, structures that cannot be visualized with conventional approaches can be clearly observed [36-38]. For example, if the camera is positioned toward the disk space and in the lateral recess, foraminal, and far lateral, the degree of endplate preparation can be checked in real time (Fig. 2).
Fig. 2.
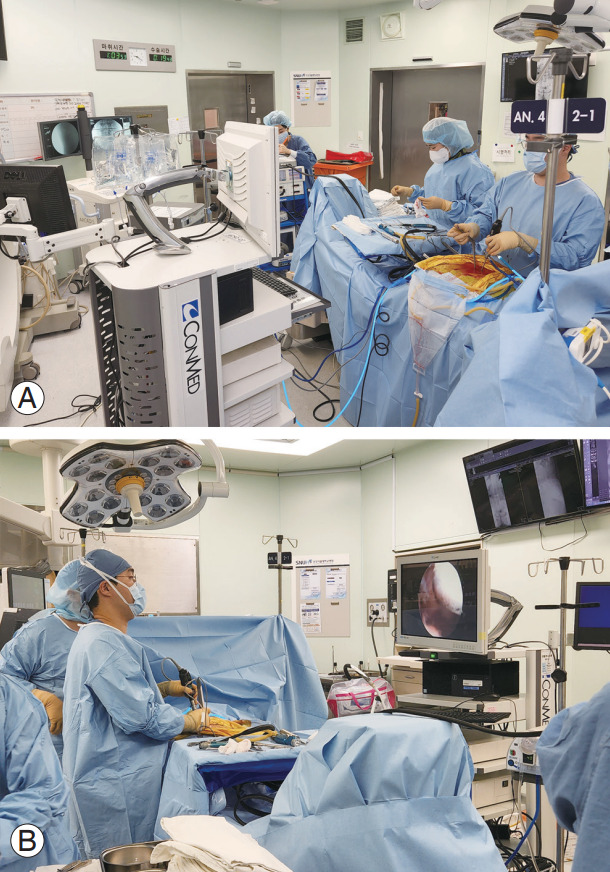
(A, B) Surgical field for minimally invasive spinal surgery using an endoscope.
Despite the steep learning curve for endoscopy, surgeons can overcome this with the development of systematic education methods [3,35]. With advances in technology and consequent expansion in the indications for this technique, the clinical and surgical outcomes are expected to improve.
2. Navigation
Damage to important structures such as nerves and blood vessels can result in serious consequences for patients. A navigation system that uses real-time images is a technological advancement that improves surgical accuracy and stability [39,40]. Using the O-arm system, a high-quality computed tomography (CT) scan can be performed after the patient under general anesthesia was placed in the operative position (Medtronic Sofamor Danek, Memphis, TN, USA) (Fig. 3). Surgeons can perform intraoperative three-dimensional (3D) spine anatomical mapping in real time by integrating it with a real-time anatomical tracking tool [41]. Spine surgeons initially use navigation systems for percutaneous pedicle screw fixation [42]. In many MISSs, intraoperative fluoroscopy is performed to achieve percutaneous pedicle screw fixation. However, despite its excellent accuracy, both the surgeons and patients are exposed to radiation. By contrast, CT-based navigation systems can significantly improve precision for pedicle screw fixation and may lower the risk of radiation exposure to surgeons and patients by more than 90%. Due to the excellent reliability and safety of navigation systems, percutaneous pedicle screw fixation is frequently used in MISSs, particularly in MI-TLIF and MI-LLIF. The reliability of current CT-based navigation systems has been confirmed by several studies, and these may be used with the majority of MISSs to reduce surgery-associated complications including reoperation rates [43]. However, the use of navigation systems is expensive, which should be addressed with increasing utilization rates of these systems.
Fig. 3.
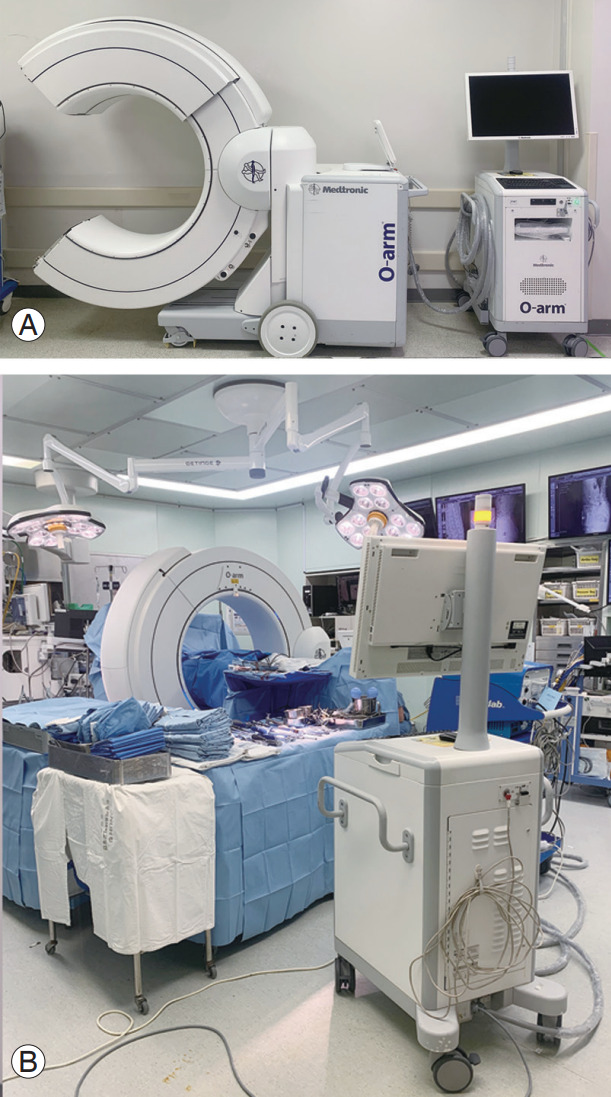
(A, B) The O-arm system (Medtronic Sofamor Danek, Memphis, TN, USA). The O-arm is used to recreate the intended surgical anatomy during the surgery according to the patient’s posture.
3. Robotics
Robotic spinal systems are increasingly used in spine surgery owing to their ability to execute precise, dependable, and efficient procedures [44,45]. Robotic technologies provide a greater precision in pedicle screw fixation and less soft tissue abrasion than other modalities when used with navigation systems [46,47], for example, the fixation of pedicle screws [48]. Although there is a lack of clinical data addressing the use of robotics in spine surgery, some studies have observed that the precision of pedicle screw fixation achieved by robotic systems is better than that achieved through free-hand (FH) approach or C-arm fluoroscopy-guided pedicle screw fixation [42,44,46]. Robotic spine surgery can help avoid physical and mental exhaustion of the surgeons, which could lead to better surgical, radiologic, and clinical outcomes [49]. Nevertheless, robotic systems are rarely used, since they are expensive [50]. However, the use of robotics in spine surgery may increase when the associated costs are reduced.
4. Augmented reality-assisted spine surgery
Compared with traditional FH surgical approaches, AR-assisted spine surgery has been demonstrated to increase the accuracy of pedicle screw placement and thus gaining popularity [51,52]. Despite the established benefits of ARassisted spine surgery, its deployment in spine surgery has lagged behind similar cranial applications, partly because the setup for spine surgeries is more time-consuming and intricate [53]. To validate anatomical and surgical landmarks using a virtual 3D reconstruction, surgeons using traditional navigation must gaze away from the operating field toward a dedicated navigation screen (Fig. 4) [54,55]. Studies on AR navigation are still in their early stages. Some have produced the first published work on an AR application that was later used in clinical studies [52,56,57]. This method uses a monitor to display an ARenhanced video stream in the operating room as well as in other subsequent preclinical and clinical investigations. Recent studies focused on placing AR systems directly in the surgeon’s field of view using head-mounted displays rather than monitors. For spine surgery, AR results in significant improvements compared with FH surgery and conventional navigation techniques. The surgical field is improved using radiological guidance to maintain the surgeon’s focus. Between AR and FH or traditional navigation approaches, AR systems have superior workflow and accuracy and result in lower radiation exposure for the surgeons and patients.
Fig. 4.
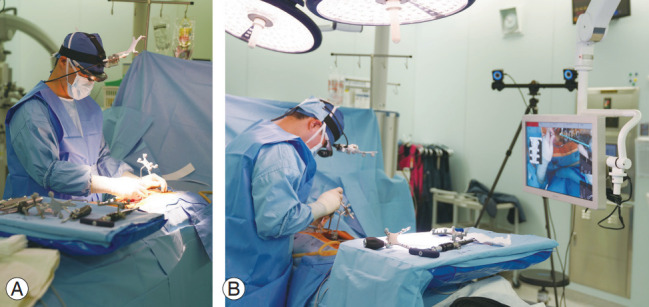
(A, B) Augmented reality assisted spine surgery.
Conclusions
The primary objectives of MISS are to reduce muscle and ligament injury during surgery and preserve normal architecture, which enable a higher postoperative recovery rate and a better quality of life. These objectives have become attainable due to considerable technological and technical breakthroughs over the last few decades. Currently, safe pedicle screw fixation can be achieved with navigation and robotic systems. Endoscopic methods have sufficiently increased the visualization of the surgical field to enable precise procedures. A variety of minimally invasive decompression and fusion surgeries can now be performed due to the development of transforaminal and retroperitoneal anterior and lateral approaches, from a straightforward herniated disk to complex spinal diseases such as spinal deformity, burst fractures, and spinal tumors. Technological advancements and development of novel surgical techniques should be continuous given the transition from classical open surgery to MISS, in order to provide patients with the choice of a minimally invasive approach. Future research and development should concentrate on enhancing workflow optimization and virtual information presentation options for AR system installation and on determining the effects of AR systems on clinical outcomes and complications.
Footnotes
No potential conflict of interest relevant to this article was reported.
Author Contributions
JYC is first author who carried out the literature survey and wrote the manuscript; SMP, HJK, JSY participated in the design and had primary responsibility for the final manuscript and helped to revise the manuscript; and all authors read and approved the final manuscript.
References
- 1.Vaishnav AS, Othman YA, Virk SS, Gang CH, Qureshi SA. Current state of minimally invasive spine surgery. J Spine Surg. 2019;5(Suppl 1):S2–10. doi: 10.21037/jss.2019.05.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Spetzger U, Von Schilling A, Winkler G, Wahrburg J, Konig A. The past, present and future of minimally invasive spine surgery: a review and speculative outlook. Minim Invasive Ther Allied Technol. 2013;22:227–41. doi: 10.3109/13645706.2013.821414. [DOI] [PubMed] [Google Scholar]
- 3.Park J, Ham DW, Kwon BT, Park SM, Kim HJ, Yeom JS. Minimally invasive spine surgery: techniques, technologies, and indications. Asian Spine J. 2020;14:694–701. doi: 10.31616/asj.2020.0384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chang PY, Wang MY. Minimally invasive spinal deformity surgery: current state and future direction. Neurosurgery. 2016;63 Suppl 1:43–51. doi: 10.1227/NEU.0000000000001296. [DOI] [PubMed] [Google Scholar]
- 5.Sharma A, Shakya A, Singh V, et al. Incidence of dural tears in open versus minimally invasive spine surgery: a single-center prospective study. Asian Spine J. 2022;16:463–70. doi: 10.31616/asj.2021.0140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang X, Borgman B, Vertuani S, Nilsson J. A systematic literature review of time to return to work and narcotic use after lumbar spinal fusion using minimal invasive and open surgery techniques. BMC Health Serv Res. 2017;17:446. doi: 10.1186/s12913-017-2398-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Goldstein CL, Macwan K, Sundararajan K, Rampersaud YR. Perioperative outcomes and adverse events of minimally invasive versus open posterior lumbar fusion: meta-analysis and systematic review. J Neurosurg Spine. 2016;24:416–27. doi: 10.3171/2015.2.SPINE14973. [DOI] [PubMed] [Google Scholar]
- 8.Cervellini P, De Luca GP, Mazzetto M, Colombo F. Micro-endoscopic-discectomy (MED) for far lateral disc herniation in the lumbar spine: technical note. Acta Neurochir Suppl. 2005;92:99–101. doi: 10.1007/3-211-27458-8_21. [DOI] [PubMed] [Google Scholar]
- 9.Katayama Y, Matsuyama Y, Yoshihara H, et al. Comparison of surgical outcomes between macro discectomy and micro discectomy for lumbar disc herniation: a prospective randomized study with surgery performed by the same spine surgeon. J Spinal Disord Tech. 2006;19:344–7. doi: 10.1097/01.bsd.0000211201.93125.1c. [DOI] [PubMed] [Google Scholar]
- 10.Abudurexiti T, Qi L, Muheremu A, Amudong A. Micro-endoscopic discectomy versus percutaneous endoscopic surgery for lumbar disk herniation. J Int Med Res. 2018;46:3910–7. doi: 10.1177/0300060518781694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zheng B, Xu S, Guo C, Jin L, Liu C, Liu H. Efficacy and safety of unilateral biportal endoscopy versus other spine surgery: a systematic review and meta-analysis. Front Surg. 2022;9:911914. doi: 10.3389/fsurg.2022.911914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hong SH, Suh SP, Yeom J, Kim JY, Lee SG, Han JW. Minimally invasive spine surgery versus open posterior instrumentation surgery for unstable thoracolumbar burst fracture. Asian Spine J. 2021;15:761–8. doi: 10.31616/asj.2020.0572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alhashash M, Shousha M. Minimally invasive short-segment anteroposterior surgery for thoracolumbar osteoporotic fractures with canal compromise: a prospective study with a minimum 2-year follow-up. Asian Spine J. 2022;16:28–37. doi: 10.31616/asj.2020.0573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hinojosa-Gonzalez DE, Roblesgil-Medrano A, Villarreal-Espinosa JB, et al. Minimally invasive versus open surgery for spinal metastasis: a systematic review and meta-analysis. Asian Spine J. 2022;16:583–97. doi: 10.31616/asj.2020.0637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Park J, Park HJ, Park SM, Choi JY, Kim HJ, Yeom JS. Learning curve for microscopic unilateral laminectomy for bilateral decompression surgery using the cumulative summation test for learning curve. Medicine (Baltimore) 2022;101:e31069. doi: 10.1097/MD.0000000000031069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Patel JY, Kundnani VG, Merchant ZI, Jain S, Kire N. Superior facet joint violations in single level minimally invasive and open transforaminal lumbar interbody fusion: a comparative study. Asian Spine J. 2020;14:25–32. doi: 10.31616/asj.2019.0065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Park JH, Jung JT, Lee SJ. How I do it: L5/S1 foraminal stenosis and far-lateral lumbar disc herniation with unilateral bi-portal endoscopy. Acta Neurochir (Wien) 2018;160:1899–903. doi: 10.1007/s00701-018-3630-9. [DOI] [PubMed] [Google Scholar]
- 18.Ali U, Tariq MA. Letter to the editor: minimally invasive versus open surgery for spinal metastasis: a systematic review and meta-analysis. Asian Spine J. 2021;15:708–9. doi: 10.31616/asj.2021.0395.r1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ishii K, Isogai N, Shiono Y, et al. Contraindication of minimally invasive lateral interbody fusion for percutaneous reduction of degenerative spondylolisthesis: a new radiographic indicator of bony lateral recess stenosis using I line. Asian Spine J. 2021;15:455–63. doi: 10.31616/asj.2020.0083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Middleton SD, Wagner R, Gibson JNA. Multi-level spine endoscopy: a review of available evidence and case report. EFORT Open Rev. 2017;2:317–23. doi: 10.1302/2058-5241.2.160087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yingsakmongkol W, Jitpakdee K, Varakornpipat P, et al. Clinical and radiographic comparisons among minimally invasive lumbar interbody fusion: a comparison with three-way matching. Asian Spine J. 2022;16:712–22. doi: 10.31616/asj.2021.0264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jin-Tao Q, Yu T, Mei W, et al. Comparison of MIS vs. open PLIF/TLIF with regard to clinical improvement, fusion rate, and incidence of major complication: a meta-analysis. Eur Spine J. 2015;24:1058–65. doi: 10.1007/s00586-015-3890-5. [DOI] [PubMed] [Google Scholar]
- 23.Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1:2–18. doi: 10.3978/j.issn.2414-469X.2015.10.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Xu DS, Walker CT, Godzik J, Turner JD, Smith W, Uribe JS. Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: a literature review. Ann Transl Med. 2018;6:104. doi: 10.21037/atm.2018.03.24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Koike Y, Kotani Y, Terao H, Iwasaki N. Comparison of outcomes of oblique lateral interbody fusion with percutaneous posterior fixation in lateral position and minimally invasive transforaminal lumbar interbody fusion for degenerative spondylolisthesis. Asian Spine J. 2021;15:97–106. doi: 10.31616/asj.2019.0342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Patel MR, Jacob KC, Zamanian C, et al. Single-level anterior lumbar interbody fusion versus minimally invasive transforaminal lumbar interbody fusion at L5/S1 for an obese population. Asian Spine J. 2022 Aug 23; doi: 10.31616/asj.2022.0071. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Park HY, Ha KY, Kim YH, et al. Minimally invasive lateral lumbar interbody fusion for adult spinal deformity: clinical and radiological efficacy with minimum two years follow-up. Spine (Phila Pa 1976) 2018;43:E813–21. doi: 10.1097/BRS.0000000000002507. [DOI] [PubMed] [Google Scholar]
- 28.Neradi D, Kumar V, Kumar S, Sodavarapu P, Goni V, Dhatt SS. Minimally invasive surgery versus open surgery for adolescent idiopathic scoliosis: a systematic review and meta-analysis. Asian Spine J. 2022;16:279–89. doi: 10.31616/asj.2020.0605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Leu H, Schreiber A. Endoscopy of the spine: minimally invasive therapy. Orthopade. 1992;21:267–72. [PubMed] [Google Scholar]
- 30.Chung AS, McKnight B, Wang JC. Scientific view on endoscopic spine surgery: can spinal endoscopy become a mainstream surgical tool? World Neurosurg. 2021;145:708–11. doi: 10.1016/j.wneu.2020.05.238. [DOI] [PubMed] [Google Scholar]
- 31.Park HJ, Park SM, Song KS, et al. Evaluation of the efficacy and safety of conventional and biportal endoscopic decompressive laminectomy in patients with lumbar spinal stenosis (ENDO-B trial): a protocol for a prospective, randomized, assessorblind, multicenter trial. BMC Musculoskelet Disord. 2021;22:1056. doi: 10.1186/s12891-021-04959-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Park SM, Song KS, Kim HJ, et al. Comparing the efficacy and safety of minimally invasive biportal endoscopic spine surgery versus conventional microscopic discectomy in single-level lumbar herniated intervertebral disc (ENDO-BH Trial): a multicenter, prospective, randomized controlled equivalence trial study protocol. Trials. 2022;23:172. doi: 10.1186/s13063-022-06094-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tieber F, Lewandrowski KU. Technology advancements in spinal endoscopy for staged management of painful spine conditions. J Spine Surg. 2020;6(Suppl 1):S19–28. doi: 10.21037/jss.2019.10.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Park SM, Lee HJ, Park HJ, et al. Biportal endoscopic versus microscopic discectomy for lumbar herniated disc: a randomized controlled trial. Spine J. 2022 Sep 23; doi: 10.1016/j.spinee.2022.09.003. [Epub]. [DOI] [PubMed] [Google Scholar]
- 35.Park SM, Park J, Jang HS, et al. Biportal endoscopic versus microscopic lumbar decompressive laminectomy in patients with spinal stenosis: a randomized controlled trial. Spine J. 2020;20:156–65. doi: 10.1016/j.spinee.2019.09.015. [DOI] [PubMed] [Google Scholar]
- 36.Kang MS, You KH, Han SY, Park SM, Choi JY, Park HJ. Percutaneous full-endoscopic versus biportal endoscopic posterior cervical foraminotomy for unilateral cervical foraminal disc disease. Clin Orthop Surg. 2022;14:539–47. doi: 10.4055/cios22050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Park SM, Kim GU, Kim HJ, et al. Is the use of a unilateral biportal endoscopic approach associated with rapid recovery after lumbar decompressive laminectomy?: a preliminary analysis of a prospective randomized controlled trial. World Neurosurg. 2019;128:e709–18. doi: 10.1016/j.wneu.2019.04.240. [DOI] [PubMed] [Google Scholar]
- 38.Park SM, Kim HJ, Kim GU, et al. Learning curve for lumbar decompressive laminectomy in biportal endoscopic spinal surgery using the cumulative summation test for learning curve. World Neurosurg. 2019;122:e1007–13. doi: 10.1016/j.wneu.2018.10.197. [DOI] [PubMed] [Google Scholar]
- 39.Dusad T, Kundnani V, Dutta S, Patel A, Mehta G, Singh M. Comparative prospective study reporting intraoperative parameters, pedicle screw perforation, and radiation exposure in navigation-guided versus non-navigated fluoroscopy-assisted minimal invasive transforaminal lumbar interbody fusion. Asian Spine J. 2018;12:309–16. doi: 10.4184/asj.2018.12.2.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kaliya-Perumal AK, Limthongkul W, Oh JY. Utilization of spinal navigation to facilitate hassle-free rod placement during minimally-invasive long-construct posterior instrumentation. Asian Spine J. 2019;13:511–4. doi: 10.31616/asj.2018.0233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ransom NA, Gollogly S, Lewandrowski KU, Yeung A. Navigating the learning curve of spinal endoscopy as an established traditionally trained spine surgeon. J Spine Surg. 2020;6(Suppl 1):S197–207. doi: 10.21037/jss.2019.10.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hanna G, Kim TT, Uddin SA, Ross L, Johnson JP. Video-assisted thoracoscopic image-guided spine surgery: evolution of 19 years of experience, from endoscopy to fully integrated 3D navigation. Neurosurg Focus. 2021;50:E8. doi: 10.3171/2020.10.FOCUS20792. [DOI] [PubMed] [Google Scholar]
- 43.Overley SC, Cho SK, Mehta AI, Arnold PM. Navigation and robotics in spinal surgery: where are we now? Neurosurgery. 2017;80:S86–99. doi: 10.1093/neuros/nyw077. [DOI] [PubMed] [Google Scholar]
- 44.Vo CD, Jiang B, Azad TD, Crawford NR, Bydon A, Theodore N. Robotic spine surgery: current state in minimally invasive surgery. Global Spine J. 2020;10(2 Suppl):34S–40S. doi: 10.1177/2192568219878131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sarkar M, Maalouly J, Ruparel S, Choi J. Sacroiliac joint fusion: fusion rates and clinical improvement using minimally invasive approach and intraoperative navigation and robotic guidance. Asian Spine J. 2022 Feb 22; doi: 10.31616/asj.2021.0058. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Judy BF, Pennington Z, Botros D, et al. Spine image guidance and robotics: exposure, education, training, and the learning curve. Int J Spine Surg. 2021;15:S28–37. doi: 10.14444/8138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.McKenzie DM, Westrup AM, O’Neal CM, et al. Robotics in spine surgery: a systematic review. J Clin Neurosci. 2021;89:1–7. doi: 10.1016/j.jocn.2021.04.005. [DOI] [PubMed] [Google Scholar]
- 48.Farber SH, Pacult MA, Godzik J, et al. Robotics in spine surgery: a technical overview and review of key concepts. Front Surg. 2021;8:578674. doi: 10.3389/fsurg.2021.578674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Park SM, Kim HJ, Lee SY, Chang BS, Lee CK, Yeom JS. Radiographic and clinical outcomes of robot-assisted posterior pedicle screw fixation: two-year results from a randomized controlled trial. Yonsei Med J. 2018;59:438–44. doi: 10.3349/ymj.2018.59.3.438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Sivaganesan A, Clark NJ, Alluri RK, Vaishnav AS, Qureshi SA. Robotics and spine surgery: lessons from the personal computer and industrial revolutions. Int J Spine Surg. 2021;15:S21–7. doi: 10.14444/8137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ariffin MH, Ibrahim K, Baharudin A, Tamil AM. Early experience, setup, learning curve, benefits, and complications associated with exoscope and three-dimensional 4k hybrid digital visualizations in minimally invasive spine surgery. Asian Spine J. 2020;14:59–65. doi: 10.31616/asj.2019.0075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Frisk H, Lindqvist E, Persson O, et al. Feasibility and accuracy of thoracolumbar pedicle screw placement using an augmented reality head mounted device. Sensors (Basel) 2022;22:522. doi: 10.3390/s22020522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Lohre R, Wang JC, Lewandrowski KU, Goel DP. Virtual reality in spinal endoscopy: a paradigm shift in education to support spine surgeons. J Spine Surg. 2020;6(Suppl 1):S208–23. doi: 10.21037/jss.2019.11.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ghaednia H, Fourman MS, Lans A, et al. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021;21:1617–25. doi: 10.1016/j.spinee.2021.03.018. [DOI] [PubMed] [Google Scholar]
- 55.Hersh A, Mahapatra S, Weber-Levine C, et al. Augmented reality in spine surgery: a narrative review. HSS J. 2021;17:351–8. doi: 10.1177/15563316211028595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Tatter C, Fletcher-Sandersjoo A, Persson O, Burstrom G, Edstrom E, Elmi-Terander A. Fluoroscopy-assisted C1-C2 posterior fixation for atlantoaxial instability: a single-center case series of 78 patients. Medicina (Kaunas) 2022;58:114. doi: 10.3390/medicina58010114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Park SM, Kim HJ, Yeom JS, Shin YG. Spine surgery using augmented reality. J Korean Soc Spine Surg. 2019;26:26–32. [Google Scholar]