

Abstract
BACKGROUND:
Persecutory delusions are among the most common delusions in schizophrenia and represent the extreme end of the paranoia continuum. Paranoia is accompanied by significant worry and distress. Identifying cognitive mechanisms underlying paranoia is critical for advancing treatment. We hypothesized that aberrant belief updating, which is related to paranoia in human and animal models, would also contribute to persecutory beliefs in individuals with schizophrenia.
METHODS:
Belief updating was assessed in 42 participants with schizophrenia and 44 healthy control participants using a 3-option probabilistic reversal learning task. Hierarchical Gaussian Filter was used to estimate computational parameters of belief updating. Paranoia was measured using the Positive and Negative Syndrome Scale and the revised Green et al. Paranoid Thoughts Scale. Unusual thought content was measured with the Psychosis Symptom Rating Scale and the Peters et al. Delusions Inventory. Worry was measured using the Dunn Worry Questionnaire.
RESULTS:
Paranoia was significantly associated with elevated win-switch rate and prior beliefs about volatility both in schizophrenia and across the whole sample. These relationships were specific to paranoia and did not extend to unusual thought content or measures of anxiety. We observed a significant indirect effect of paranoia on the relationship between prior beliefs about volatility and worry.
CONCLUSIONS:
This work provides evidence that relationships between belief updating parameters and paranoia extend to schizophrenia, may be specific to persecutory beliefs, and contribute to theoretical models implicating worry in the maintenance of persecutory delusions.
Persecutory delusions—beliefs that others intend you harm—are among the most common delusions in schizophrenia (1,2). They exist on the extreme end of a paranoia continuum, which represents the degree of mistrust one has toward others, and includes the mild suspiciousness often observed in the general nonclinical population (3). Paranoia is related to reduced well-being, violence toward self and others (4–6), conspiracy theorizing (7), and less adherence to public health measures (8). Identifying the underlying mechanisms of paranoia will have clinical and broader societal impact.
Worry and negative self-beliefs contribute to paranoia and persecutory beliefs (9). These can be targeted with psychotherapy, with a large and specific impact on persecution (10). However, a deeper appreciation of the underlying mechanisms of paranoia is necessary. Belief updating is one candidate (11). The challenge of updating one’s beliefs is to remain robust to real-world variability (e.g., sometimes there is unexpectedly bad traffic) while simultaneously flexible in the face of true change (e.g., there is now a new traffic pattern and I need to find a different daily route home). Anecdotally, expecting a volatile (i.e., changing and unstable) world licenses worry and paranoia (12). We sought to test this hypothesis experimentally.
Recent work has linked belief updating parameters to paranoia in largely nonclinical samples. Specifically, parameters reflecting prior beliefs about volatility (i.e., beliefs held before new evidence is encountered), as well as sensitivity to volatility, were greater in individuals with elevated paranoia (8,13). Belief updating parameters were also increased in rats administered methamphetamine, an animal model of paranoia based on how escalating doses of methamphetamine increase paranoia in humans (14) and affect reversal learning in rats (13,15). How beliefs about, and sensitivity to, volatility each contribute to persecutory beliefs in schizophrenia has not yet been established.
Furthermore, belief updating is relevant to and affected by anxiety. Both trait and state anxiety are related to compromised adjustment of learning rates in the context of environmental uncertainty (16,17). Worry in particular is strongly associated with paranoia (18,19). It keeps threat beliefs in mind, encouraging elaboration and actions (e.g., avoidance) that nourish the persecutory belief (20). Cognitive behavioral therapy for worry reduces persecutory delusion severity (21). Understanding the relationship between belief updating, paranoia, and worry may connect computational psychiatry and the precision it affords with the therapeutic opportunities of psychotherapy (22).
We examined 1) whether the relationship between belief updating parameters and paranoia extends to schizophrenia, 2) the specificity of this relationship as compared with overall unusual thought content and anxiety, and 3) the indirect effect of paranoia on volatility and worry, hypothesizing that a greater expectation of volatility (“the world is frequently changing”) is associated with paranoid thinking (“I will be harmed”), which itself relates to worry.
METHODS AND MATERIALS
Participants
A total of 45 individuals with a schizophrenia spectrum disorder and 46 healthy control participants with no psychiatric history were recruited. Individuals ages 18 to 55 years were identified from the Vanderbilt University Medical Center Psychotic Disorders Program. Diagnoses were confirmed by a Structured Clinical Interview of the DSM-IV-TR or DSM-5 (23) completed by a trained rater and signed off in a consensus meeting. Diagnoses included 17 schizophrenia, 17 schizophreniform disorder, 7 schizoaffective disorder, and 1 psychotic disorder not otherwise specified. All participants were free of major physical or neurologic illness, active substance use disorder, and significant head injury and had an estimated IQ of >79. Healthy control participants did not have a first-degree relative with a psychotic disorder or any current psychotropic medication use. Study protocol was approved by the Vanderbilt Institutional Review Board, and informed consent was provided by all research participants before study participation.
Participants were recruited between December 2020 and October 2021. Given limitations of in-person research participation during the COVID-19 pandemic, the majority of participants (91%) conducted the study at home on a personal laptop. A smaller proportion of participants (9%) who did not have access to a laptop completed the study in person.
Delusion Assessments
In the schizophrenia group, clinical interviews were used to assess paranoia and unusual thought content. Paranoia was measured using the Positive and Negative Syndrome Scale (24) Suspiciousness/Persecution scores, and overall delusion severity was assessed using the Psychosis Symptom Rating Scale (25), an interviewer-rated assessment of the conviction, preoccupation, distress, and functional impairment related to a specific delusional belief that the participant was either currently experiencing or, if not experiencing any current delusions, had experienced strongly in the past. Severity of that delusion was rated in the past week and included a variety of themes (e.g., grandiose, religious, guilt, and persecution).
Self-reported paranoia and unusual thought content were measured across all participants using the revised Green et al. Paranoid Thoughts Scale (R-GPTS) (26), which includes a 10-item scale measuring persecutory ideation (GPTS-b), and the Peters et al. Delusions Inventory (27), which assesses endorsement (yes/no), level of distress, conviction, and pre-occupation related to a variety of delusional beliefs.
Other Symptom Assessments
Anxiety was assessed using 1) the Beck Anxiety Inventory (28), 2) the Dunn Worry Questionnaire (18), which includes 10 items related to how worry interferes with daily life (general worry) and a 5-item assessment of persecutory worries, 3) the Perseverative Thinking Questionnaire (29), and 4) the Liebowitz Social Anxiety Scale (30). Depression was assessed using the Beck Depression Inventory (31).
Experimental Paradigm
Belief updating was measured using the 3-option probabilistic reversal learning task (Figure 1A). Participants were presented with 3 decks of cards on a computer screen and told that each deck includes both winning (+100 points) and losing (−50 points) cards, but that some decks win more often than others. They were instructed to find the best deck (i.e., the one with the highest probability for reward) and that the best deck might change, whereupon they should try and find the new best deck. Participants’ overarching goal was to win the most points they could. To enhance engagement and motivation, they were offered a $2 incentive for winning more points than 75% of other participants. There were 160 trials divided into 4 blocks, with an optional break in between each block. Before beginning the main task, participants completed 3 practice trials. Because the study was conducted remotely, participants were asked to share their screen with the researcher, who walked them through the instructions and practice trials and closely observed their behavior throughout the task.
Figure 1.
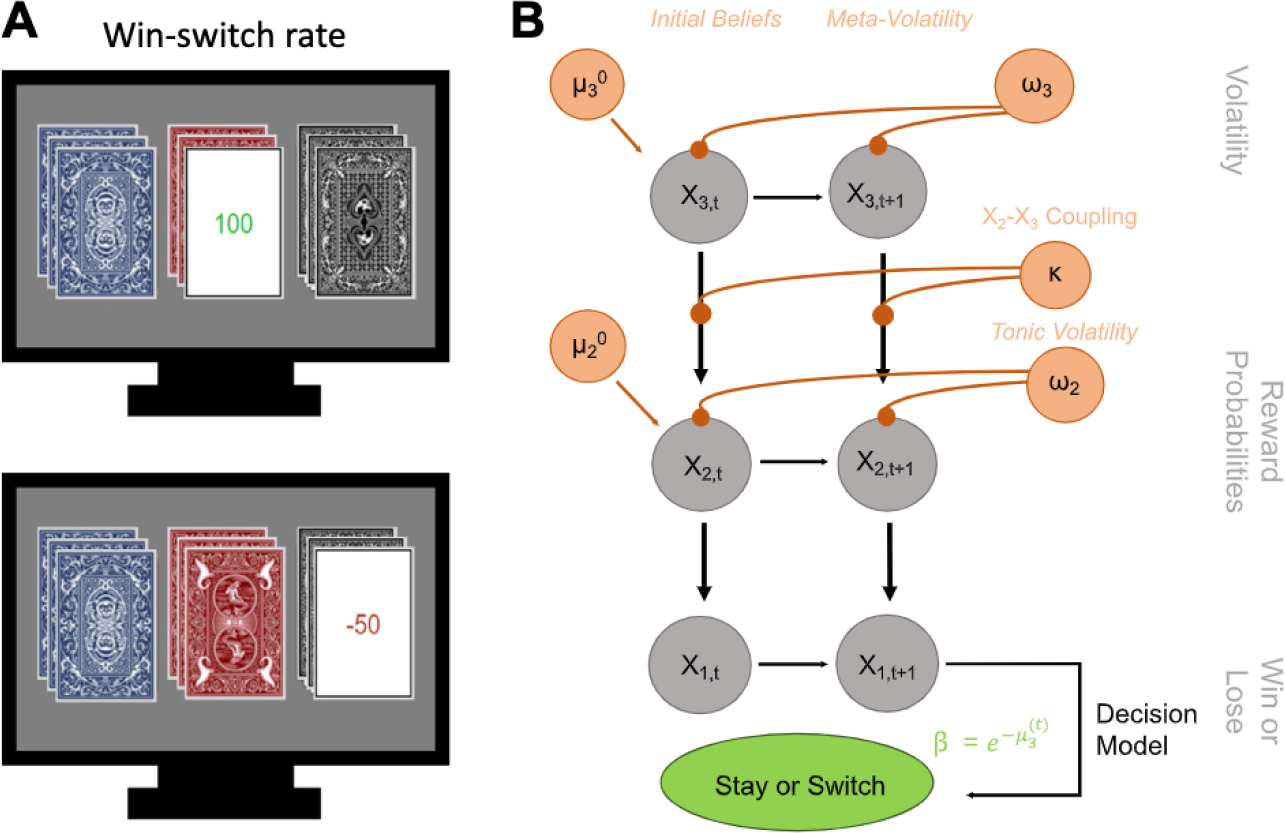
(A) Task image of 3-option probabilistic reversal learning. Participants are simultaneously shown 3 decks of cards and are asked to select a card from any of the decks using keys on the computer keyboard. Once a deck is selected, the card is flipped to reveal whether that card won (+100) or lost (−50) them points. At the start of the task, participants are instructed to earn as many points as possible. They are also told that, while all of the decks include both winning and losing cards, one of the decks is best and will win them the most points. Finally, they are told that the best deck may change during the task and, if they believe it has changed, they should find the new best deck. Reward contingencies begin at 90%/50%/10% to support development of strong beliefs about the task environment and then, unbeknownst to the participant, change to 80%/40%/20%. (B) Schematic of the 3-level Hierarchical Gaussian Filter model using a Softmax decision model. Level 1 (x1) represents trial-by-trial win or loss feedback. Level 2 (x2) is the stimulus-outcome association (reward probabilities of the decks). Level 3 (x3) is the perception of the overall reward contingency context (volatility). Initial beliefs about task volatility are captured by μ03, which reflects a participant’s expectation about instability and change in the task before new evidence is encountered. Readiness to learn about changes in the volatility of the task are captured by the meta-volatility rate (ω3), which indexes how stable the changes in underlying contingencies of the decks might be. Higher values imply a more rapid adjustment of their volatility belief. Sensitivity to that volatility (i.e., the impact of phasic volatility on stimulus-outcome associations) is captured by κ, whereas ω2 reflects the tonic volatility of stimulus-outcome associations, with lower values indicating slower adjustment of beliefs about the value of each deck choice.
The task was designed to elicit the experience of volatility in several ways. First, the best deck changed when a participant selected it in 9 of 10 consecutive trials (reversal events). Second, the decks yielded 90%, 50%, and 10% reward for blocks 1 and 2 (80 trials) and then, unbeknownst to the participant, these contingencies changed at the start of block 3 to 80%, 40%, and 20% (contingency transition). The goal of this task structure was to make it more difficult for participants to discern whether a loss was due to probabilistic noise or due to the best deck changing. By beginning the task with a 90-50-10 probability structure, participants were expected to develop stronger beliefs about the task environment, making the contingency transition more confounding, thereby increasing the experience of volatility (13).
Behavioral Analysis
The primary behavioral measure of interest was win-switch rate. Win-switching occurs when an individual chooses an alternative deck even after receiving positive feedback (+100 points). Win-switch rates were calculated as the number of win-switch decisions divided by the number of trials in which they received positive feedback. We also investigated lose-stay decisions, which reflect a decision to persist with a chosen deck after receiving negative feedback (−50 points). Lose-stay rates were calculated as the number of lose-stay decisions divided by the number of trials with negative feedback.
Computational Modeling
Computational modeling was conducted on task data using the Hierarchical Gaussian Filter toolbox (32,33) in MATLAB (version 2020b; The MathWorks, Inc.) (Figure 1B). Belief updating parameters were calculated for the 90-50-10 reward contingencies (first and second blocks) and the 80-40-20 contingencies (third and fourth blocks). Participant data were entered as separate column vectors for each block, modeling deck choice (deck 1, 2, or 3) and outcome (win or loss), using an autoregressive 3-level Hierarchical Gaussian Filter multiarm bandit configuration for the perceptual model, paired with a decision model that contains μ03 (Softmax-μ03 decision model) to model an individual’s behavior, driven by their prior belief of how volatile the task environment is. Belief updating trajectories are represented as probability distributions that encode belief content and uncertainty and were specific to each participant, due to the probabilistic and performance-dependent nature of the task. Analyses were completed using scripts that have been previously reported and shared (8) (https://github.com/psuthaharan/covid19paranoia). Previous work has tested the propriety of the 3-level Hierarchical Gaussian Filter through simulations and comparison with alternative models (13). Simulation recovers group differences between elevated and low paranoia better than simpler models, suggesting its appropriateness for examining relationships with paranoia.
The primary computational parameter of interest was μ03. This parameter estimates the initial (prior) beliefs of the level 3 (overall) volatility. In other words, it infers the participant’s belief about how volatile (changing, unstable) the task environment is before new evidence being encountered. Higher μ03 values indicate a greater prior belief about volatility (i.e., a stronger expectation that the contingencies will shift erratically). We were also interested in κ, which captures sensitivity to perceived unexpected (phasic) task volatility (changes), with higher κ (sensitivity to volatility) also contributing to more rapid and extensive updating of beliefs. In addition, ω2 and ω3 were calculated. These parameters reflect the evolution rate of the task environment at the level of contingencies (ω2) and volatility (ω3), with higher levels implying more rapid change. Model fit was estimated using the Bayesian information criterion.
Data Analysis
Participant demographics were compared between groups (Table 1). Multivariate outliers were identified using Mahalanobis distance calculations for the R-GPTS total score and the win-switch rate. Four multivariate outliers were identified and excluded from further analysis (1 healthy control participant and 3 participants with schizophrenia), in addition to 1 healthy participant who was prescribed a psychotropic medication. The final sample size for all analyses was 42 participants with schizophrenia and 44 healthy control participants.
Table 1.
Participant Demographics
| Characteristics | Healthy Control Participants, n = 44 | Participants With Schizophrenia, n = 42 | Statistic |
|---|---|---|---|
| Age, Years, Mean (SD) | 30.1 (8.0) | 27.4 (10.2) | t84 = 1.83, p = .07 |
| Gender, F/M, n | 17/27 | 11/31 | χ21 = 1.5, p = .22 |
| Race, Black/Other/White, n | 9/5/30 | 12/3/27 | χ23 = 1.0, p = .59 |
| Personal Educationa, Years, Mean (SD) | 17.1 (2.3) | 14.6 (2.4) | t84 = 5.0, p < .001 |
| Parental Education, Years, Mean (SD) | 14.7 (2.3) | 14.6 (2.8) | t84 = 0.24, p = .81 |
| Premorbid IQa, Mean (SD) | 114 (7.7) | 105 (13.2) | t84 = 4.0, p < .001 |
| Green et al. Paranoid Thoughts Scale-b, Mean (SD) | 1.6 (2.7) | 1.7 (3.8) | t84 = −0.04, p = .97 |
| PANSS Positive, Mean (SD) | – | 13.1 (4.1) | – |
| PANSS Negative, Mean (SD) | – | 13.8 (6.2) | – |
| PANSS General, Mean (SD) | – | 25.5 (5.2) | – |
Premorbid IQ was measured using the Wechsler Test of Adult Reading.
F, female; M, male; PANSS, Positive and Negative Syndrome Scale.
p < .05.
Repeated-measures analysis of variance was also used to determine whether computational parameters differed based on reward contingencies (main effect of block) and whether there was a significant group by block interaction. In the absence of a group by block interaction, computational parameters averaged across the blocks were used for further analysis. Group differences in behavioral measures (win-switch and lose-stay) and computational parameters (μ03. κ, ω2, ω3) were tested in two separate multivariate analysis of variance models.
Relationships between belief updating measures and symptom assessments were analyzed in two-tailed bivariate correlations, using either Spearman’s ρ (relationships with paranoia, which was non-normally distributed in our sample), or Pearson’s r (relationships with anxiety/depression). Hypothesized relationships between paranoia, win-switch, μ03, and κ were examined first (significance deemed at p < .05). Exploratory analyses between paranoia and lose-stay, ω2, and ω3 were Bonferroni-corrected for the 3 parameters (pcritical = .02). Relationships with anxiety/depression were also Bonferroni-corrected based on the number of belief updating parameters tested (pcritical = .03). Presented statistics are uncorrected, but it is noted when they do not meet significance due to multiple comparisons correction.
Specificity of relationships with paranoia was tested using Meng’s Z test of correlated correlations (34).
Given similar demographics across groups, no covariates were included in our primary analyses; however, results with covariates (age, gender, race) are outlined in the Supplement.
Cross-sectional mediation analysis was conducted using the Process macro (version 4.0) in SPSS (version 28, model 4; IBM Corp.), which used 5000 bootstrap samples with 95% confidence intervals to determine statistical significance.
RESULTS
Group Differences in Behavioral Performance
Participants with schizophrenia displayed slightly slower reaction time (F1,84 = 3.77, p = .06, η2 = 0.04) and achieved fewer reversals (F1,84 = 3.35 p = .07, η2 = 0.04), although the differences were not significant. They exhibited significantly more win-switch (F1,84 = 9.21, p = .003, η2 = 0.10) and less lose-stay (F1,84 = 4.53, p = .04, η2 = 0.05) behavior than healthy control participants, although lose-stay differences did not survive correction. Participants with schizophrenia shifted to a new card deck after a win almost 3 times as often as healthy control participants (11 % vs. 4% of the time) (Figure 2A).
Figure 2.
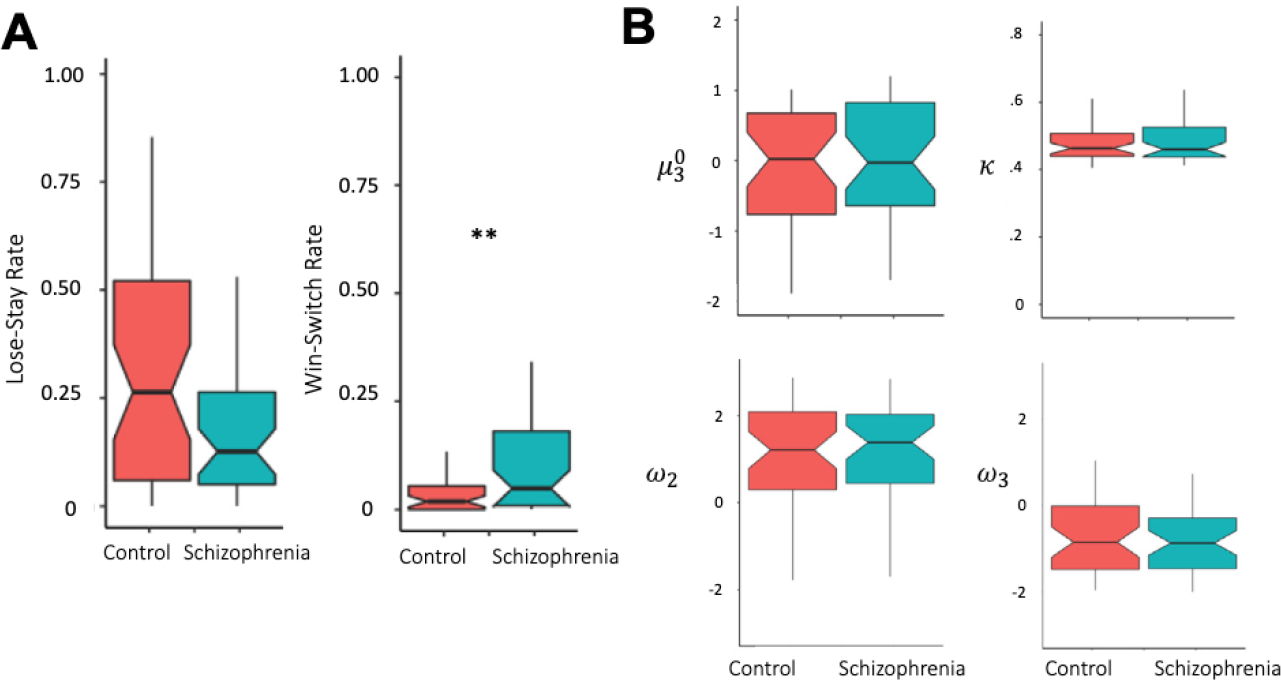
Group differences in belief updating behavior. (A) Participants with schizophrenia had significantly greater win-switch behavior but did not differ on lose-stay rate. (B) None of the computational parameters (μ03, κ, ω2, ω3) significantly differed between participants with schizophrenia and healthy control participants. **F1,84 = 9.21, p = .003, η2 = 0.10.
Behavioral Performance and Paranoia
In the schizophrenia group, interviewer-rated paranoia was significantly associated with win-switch (ρ42 = 0.34, p = .03) but not lose-stay (ρ42 = −0.19, p = .23) rate. Similarly, self-reported paranoia was significantly associated with win-switch rate across all participants (ρ86 = 0.27, p = .01) (Figure 3). Lose-stay was not significantly associated with self-reported paranoia (ρ86 = 0.03, p = .78).
Figure 3.
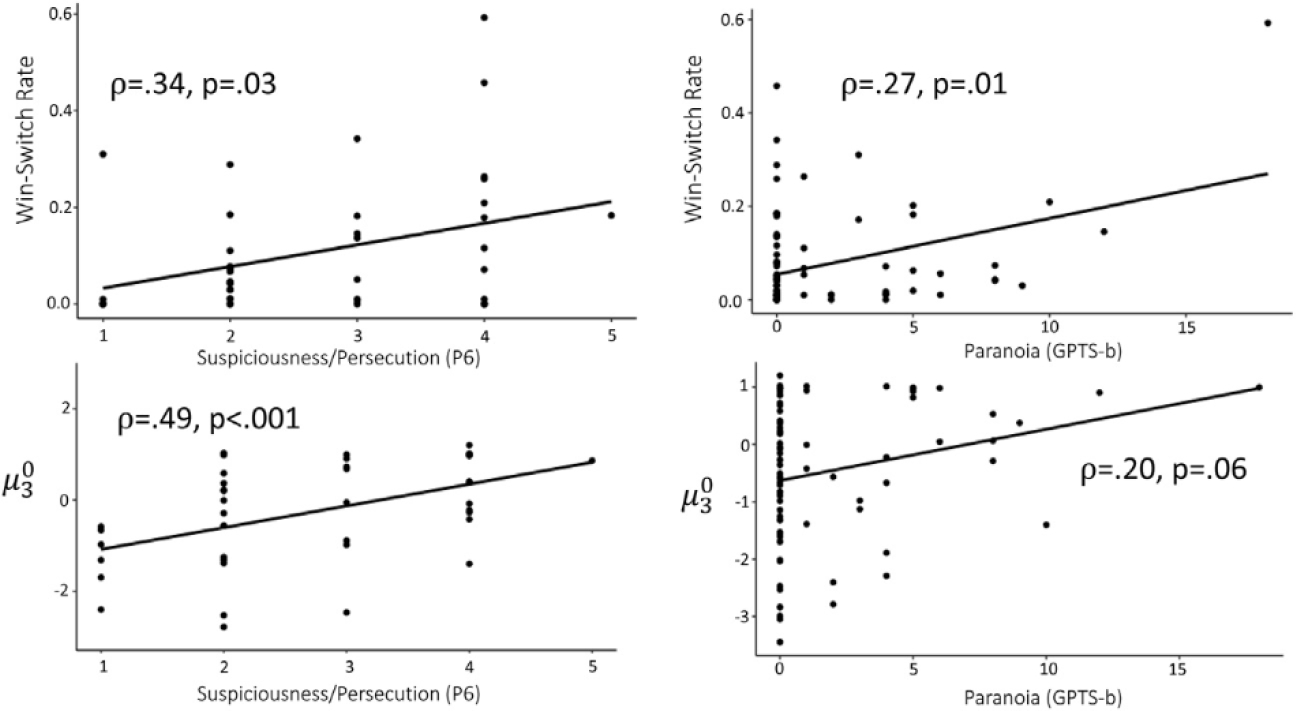
Both win-switch rate and μ03 were significantly associated with paranoia. This was true in the schizophrenia group alone using an interviewer rating of suspiciousness/persecution (Positive and Negative Syndrome Scale, item P6: Suspiciousness/Persecution). Across the entire sample using the revised Green et al. Paranoid Thoughts Scale-b (GPTS-b) self-report questionnaire, win-switch rate was also significantly associated with paranoia, but μ03 did not meet statistical significance (p = .06).
Behavioral Performance and Unusual Thought Content
In the schizophrenia group, interviewer-rated measures of unusual thought content were not significantly associated with win-switch (ρ42 = 0.07, p = .64) or lose-stay (ρ42 = 0.16, p = .32) behavior. Similarly, self-reported delusional ideation was not significantly associated with win-switch (ρ86 = 0.13, p = .24) or lose-stay (ρ86 = 0.22, p = .05) behavior across the whole sample.
Group Differences in Computational Parameters
Model fit was similar across groups (F1,84 = 0.55, p = .46, η2 = 0.01). Repeated-measures analysis of variance did not reveal any significant group by block interactions for computational parameters (p values > .25). No significant group differences were observed for computational parameters between participants with schizophrenia and healthy control participants (Figure 2B).
Computational Parameters and Paranoia
In the schizophrenia group, interviewer-rated paranoia was significantly associated with μ03 (ρ42 = 0.49, p < .001) (Figure 3) but not κ (ρ42 = 0.27, p = .09), ω2 (ρ42 = −0.24, p = .13), or ω3 (ρ42 = −0.30, p = .06).
Across the whole sample, a similar pattern was observed, although the associations were less robust. For instance, greater μ03 was related to greater self-reported paranoia, but the relationship did not meet statistical significance (ρ86 = 0.20, p = .06). In addition, κ (ρ86 = 0.15, p = .17), ω2 (ρ86 = −0.12 , p = .27), and ω3 (ρ86 = −0.23, p = .04) were not significantly related after correcting for multiple comparisons.
Computational parameters were not significantly associated with either interview-rated delusion severity (all p values > .07) or self-reported delusional ideation across the whole sample (p values > .10).
Finally, participants were split into those with elevated and low paranoia based on their R-GPTS-b scores. Detailed in the Supplement (Figure S1), we observed significantly greater μ03 and κ in those with elevated paranoia.
Anxiety and Depression
Groups did not differ on self-reported anxiety or depression (p values > .15). Neither μ03 nor win-switch rate was significantly associated with measures of anxiety, including physiological anxiety, social anxiety, overall worry, or perseverative thinking (all p values > .15).
Persecutory worry was, however, significantly associated with win-switch behavior (r86 = 0.37, p < .001) and μ03 (r86 = 0.25, p = .02). General, nonpersecutory worry was not associated with win-switch behavior (r86 = 0.09, p = .42) or μ03 (r86 = 0.05, p = .63).
Indirect Effect Analysis
In the schizophrenia sample, paranoia demonstrated a significant indirect effect on the relationship between μ03 and overall worry (95% CI = 0.35–3.8) (Figure 4A) in the context of significant relationships between μ03 and paranoia (t40 = 3.43, p = .001) and between paranoia and worry (t39 = 2.65, p = .01). Similarly, in the whole sample, paranoia had a significant indirect effect on the relationship between μ03 and overall worry (95% CI = 0.07–1.4) (Figure 4B) in the context of significant relationships between μ03 and paranoia (t84 = 2.18, p = .03) and between paranoia and worry (t83 = 3.54, p < .001).
Figure 4.
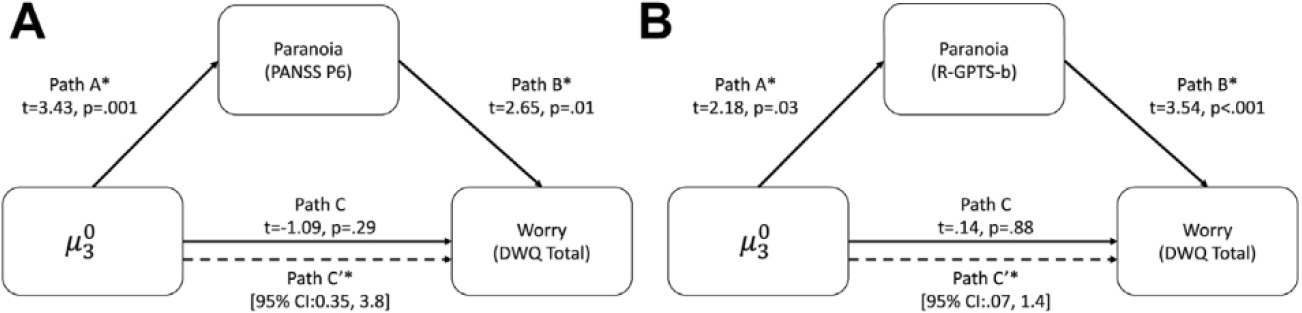
Indirect effect analysis. (A) In the schizophrenia sample, paranoia demonstrated an indirect effect between the prior belief about volatility μ03 and overall worry as measured by the total scores from the Dunn Worry Questionnaire (DWQ). (B) The same relationship was observed across the entire sample, using the revised Green et al. Paranoid Thoughts Scale-b (R-GPTS-b) self-report questionnaire. Path statistics were estimated using PROCESS model 4 SPSS. *p < .05. PANSS, Positive and Negative Syndrome Scale.
Additional Analyses
Specificity and covariate analyses are detailed in the Supplement. Briefly, μ03 was significantly more strongly correlated with paranoia than with anxiety, depression, or unusual thought content. Relationships between μ03 and paranoia were robust to the inclusion of age, gender, race, antipsychotic medication dose, and IQ. Inclusion of race and IQ did attenuate relationships between win-switch and paranoia.
DISCUSSION
This study replicates previous work connecting aberrant belief updating with paranoia and extends the relationship to individuals with schizophrenia. We replicate elevated win-switch rates in schizophrenia (35,36) and relationships between self-reported paranoia and belief updating (8,13). We then demonstrate that elevated win-switch behavior and prior belief about volatility are significantly associated with greater persecution beliefs in individuals with schizophrenia, suggesting that previous findings in a heterogenous sample do indeed extend along the persecutory delusion continuum. Belief updating parameters may also be specific to paranoid thinking, because they were significantly less associated with overall unusual thought content or measures of anxiety and depression. Further, we demonstrate a novel, significant indirect effect of paranoia on the relationship between volatility and worry.
Belief updating has been increasingly implicated in delusional thinking (37). It represents a key challenge that the brain faces, learning to predict the environment with sufficient confidence while remaining flexible enough when confronted with significant change (38). Our data and models implicate a prior expectation of change. This is often tethered to a prediction error, which may be reflected in mesocortical and mesostriatal dopamine signaling, as well as noradrenergic responses in the locus coeruleus, insula, and anterior cingulate cortex (39).
In schizophrenia, we observed significant elevations in win-switch rate but not computational parameters. Elevated win-switch rate is frequently observed in schizophrenia (40,41). A recent neuroimaging study of a 2-option probabilistic reversal learning task in schizophrenia found elevated μ03 and κ in stable, medicated patients (35), in contrast to our findings. Elevated volatility priors in schizophrenia were related to activity in the dorsolateral prefrontal cortex, suggesting involvement of the dorsolateral prefrontal cortex in this experience of volatility during decision making. Although diagnostic groups did not differ, we replicated previous work showing that individuals with elevated paranoia have elevated μ03 and κ (14). While the groups were unbalanced and, therefore, this analysis was largely exploratory, this suggests that elevations in these belief updating parameters may be more related to paranoid beliefs than diagnosis.
A main goal of this study was determining whether individuals with schizophrenia exhibit the same continuous relationships between paranoia and belief updating as has been observed in the general population and further determining if these relationships extend to delusional ideation more broadly. We found that elevated prior belief about volatility μ03 was significantly associated with the suspiciousness/persecution rating on the Positive and Negative Syndrome Scale, a relationship that was robust to differences in IQ, age, gender, and race. Our participants with schizophrenia had an average score of 3, representing guardedness and a distrustful attitude but not a severe persecutory delusion in most participants. Paranoia exists on a continuum (42), and the similar levels of paranoia reported in our participants with schizophrenia and healthy control participants lends support to this model. While the relatively low level of delusion severity in this dataset limits our ability to detect relationships between volatility and paranoia on more extreme ends of the continuum, it also suggests that even when persecutory delusion severity is relatively low, the belief that the world is unpredictable and frequently changing contributes to a paranoid thinking style. Paranoia and beliefs about volatility may instead represent a more trait-like vulnerability that can be exacerbated in certain situations [e.g., under stress (8,43)]. Longitudinal assessment of individuals with schizophrenia will facilitate our understanding of how severity affects volatility beliefs.
Belief updating measures were not significantly associated with delusional ideation more broadly. The importance of delusional themes has been long debated in the clinical literature (44). On the one hand, understanding how an individual develops a false and incorrigible belief is broadly important; yet, conceptualizing the type of delusion may help guide specific treatment recommendations (45,46). The relationship between belief updating measures and paranoia, but not overall delusion severity, suggests importance of these volatility beliefs for the experience of threat and suspiciousness specifically. This is somewhat in line with recent findings in a large population-based dataset that found only marginal associations between psychotic-like experiences and distinct computational estimates of belief updating processes (decision noise), using a task with fewer dynamic shifts in contingencies (and therefore less volatility) (47). Broad measurements of delusions, particularly in populations with relatively low symptom severity, may not link as strongly to belief updating as specific measures of paranoia; however, this requires continued investigation.
An additional goal of the study was to examine relationships between belief updating, paranoia, and anxiety. Trait anxiety is associated with a deficit in adjusting learning rates when environmental volatility changes (16). State anxiety is related to underestimation of environmental uncertainty, contributing to reduced learning rates (17). Anxiety, particularly worry, contributes to paranoia and persecutory delusions (19,48). We found that physiological anxiety, social anxiety, and generalized worry were not significantly associated with belief updating parameters in this sample, including no significant relationships with learning rates (ω2). We did, however, observe a significant association between volatility and greater persecutory worry (e.g., “worries about someone trying to harm me have been really hard to control”) but not general worry (e.g., “In my mind I have been going over problems again and again”).
The relationship between worry, paranoia and volatility was further tested by measuring the indirect effect of paranoia on the relationship between volatility and worry, revealing that a stronger volatility belief was associated with paranoia, which was in turn associated with general worrying. Theoretical accounts of paranoia have suggested that worrying keeps threat beliefs in mind, elaborates on them, and drives behavior (49). A cognitive behavioral therapy intervention targeting worry significantly reduced persecutory delusion severity in individuals with schizophrenia, validating it as a contributory causal factor to maintenance of persecutory delusions (21). It remains unknown, however, what makes someone feel paranoid in the first place and what additional cognitive processes may be at play. These findings are the first to suggest that a prior belief that the world is volatile is associated with paranoid beliefs, which is itself associated with worry. While replication is needed, particularly in a longitudinal cohort and/or intervention study, this implies that volatility beliefs represent a future target for cognitive behavioral and other psychosocial interventions and that we might employ this computational marker as a metric of change with therapy or as a prospective harbinger of therapeutic success.
Related to the notion of psychosocial impact on volatility beliefs, individuals with elevated paranoia in our sample were significantly more likely to be African American. It is critical to note that this dataset is too small to draw conclusions about the influence of race or racial discrimination on paranoia and volatility; however, it opens up an interesting line of inquiry around how these volatility priors develop. Future research should examine whether discrimination, urbanicity, and poverty (known risk factors for the development of psychosis) (50) influence belief updating. Additionally, while the relationship between volatility and paranoia was robust to the inclusion of IQ, relationships with win-switch rate were more impacted. Both IQ and win-switch rate significantly differed between diagnostic groups, meaning that inclusion of IQ in these analyses (particularly group difference analysis) likely covaried for diagnostic effects. That said, previous work has identified associations between IQ and performance on reversal learning tasks in schizophrenia (51), which have been localized to the dorsolateral prefrontal cortex in a developmental cohort (52). These findings suggest that IQ may influence task performance but that computational markers of belief updating may be less sensitive to individual differences in IQ.
Limitations of this study include small sample size, relatively low symptom severity of our participants, and completion of the study virtually. Small sample size increases the risk of false positives (53); however, we note that the effect size of the group difference in win-switch rate and correlations between belief updating and paranoia are highly similar to those observed in previous studies (13), including a sample of several hundred individuals (8), increasing our confidence in these findings. Lower symptom ratings in participants with schizophrenia may have limited our ability to detect relationships with unusual thought content. Finally, due to lockdown conditions related to the COVID-19 pandemic, the majority of participants completed the study virtually. This may have introduced additional noise and slightly limited the ability of the interviewer to fully assess clinical symptom ratings. Reliability of the Positive and Negative Syndrome Scale over telehealth has not been specifically established, yet work from other fields (autism, dementia) suggests the validity of conducting clinical assessments virtually (54,55). Furthermore, previous work on paranoia and belief updating was replicated in the office and virtually (over MTurk) (13), again suggesting durability of these relationships regardless of location completed.
In summary, these findings provide additional evidence for a role of belief updating in paranoia (particularly elevated prior belief about volatility) and extend these relationships to individuals with schizophrenia. They further suggest specificity of these relationships to paranoia, as opposed to unusual thought content and anxiety. Finally, they suggest that a prior belief that the world is volatile relates to paranoid thoughts, which are themselves associated with worry. These findings implicate prior belief about volatility as a potential target for treatment of persecutory delusions.
Supplementary Material
ACKNOWLEDGMENTS AND DISCLOSURES
This work was supported by the Vanderbilt Department of Psychiatry and Behavioral Sciences (JMS) and Grant No. K23MH126313 (to JMS).
We thank Kendall Beals, Lauren Hall, and Dr. Kristan Armstrong for the collection of this data.
Footnotes
The authors report no biomedical financial interests or potential conflicts of interest.
A previous version of this article was published as a preprint on PsyArXiv: https://psyarxiv.com/3gyde/.
Supplementary material cited in this article is available online at https://doi.org/10.1016/j.bpsc.2022.03.013.
Contributor Information
Julia M. Sheffield, Department of Psychiatry & Behavioral Sciences, Vanderbilt University Medical Center, Nashville, Tennessee
Praveen Suthaharan, Department of Psychiatry, Connecticut Mental Health Center, Yale University, New Haven, Connecticut.
Pantelis Leptourgos, Department of Psychiatry, Connecticut Mental Health Center, Yale University, New Haven, Connecticut.
Philip R. Corlett, Department of Psychiatry, Connecticut Mental Health Center, Yale University, New Haven, Connecticut
REFERENCES
- 1.Sartorius N, Jablensky A, Korten A, Ernberg G, Anker M, Cooper JE, Day R (1986): Early manifestations and first-contact incidence of schizophrenia in different cultures. A preliminary report on the initial evaluation phase of the WHO Collaborative Study on determinants of outcome of severe mental disorders. Psychol Med 16:909–928. [DOI] [PubMed] [Google Scholar]
- 2.Picardi A, Fonzi L, Pallagrosi M, Gigantesco A, Biondi M (2018): Delusional themes across affective and non-affective psychoses. Front Psychiatry 9:132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Freeman D (2007): Suspicious minds: The psychology of persecutory delusions. Clin Psychol Rev 27:425–457. [DOI] [PubMed] [Google Scholar]
- 4.Freeman D, Startup H, Dunn G, Wingham G, Černis E, Evans N, et al. (2014): Persecutory delusions and psychological well-being. Soc Psychiatry Psychiatr Epidemiol 49:1045–1050. [DOI] [PubMed] [Google Scholar]
- 5.Hor K, Taylor M (2010): Suicide and schizophrenia: A systematic review of rates and risk factors. J Psychopharmacol 24(suppl):81–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Coid JW, Ullrich S, Kallis C, Keers R, Barker D, Cowden F, Stamps R (2013): The relationship between delusions and violence: Findings from the East London first episode psychosis study. JAMA Psychiatry 70:465–471. [DOI] [PubMed] [Google Scholar]
- 7.Freeman D, Bentall RP (2017): The concomitants of conspiracy concerns. Soc Psychiatry Psychiatr Epidemiol 52:595–604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Suthaharan P, Reed EJ, Leptourgos P, Kenney JG, Uddenberg S, Mathys CD, et al. (2021): Paranoia and belief updating during the COVID-19 crisis. Nat Hum Behav 5:1190–1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Freeman D, Sheaves B, Goodwin GM, Yu LM, Nickless A, Harrison PJ, et al. (2017): The effects of improving sleep on mental health (OASIS): A randomised controlled trial with mediation analysis. Lancet Psychiatry 4:749–758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Freeman D, Emsley R, Diamond R, Collett N, Bold E, Chadwick E, et al. (2021): Comparison of a theoretically driven cognitive therapy (the Feeling Safe Programme) with befriending for the treatment of persistent persecutory delusions: A parallel, single-blind, randomised controlled trial. Lancet Psychiatry 8:696–707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Corlett PR, Frith CD, Fletcher PC (2009): From drugs to deprivation: A Bayesian framework for understanding models of psychosis. Psychopharmacology (Berl) 206:515–530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Feeney EJ, Groman SM, Taylor JR, Corlett PR (2017): Explaining delusions: Reducing uncertainty through basic and computational neuroscience. Schizophr Bull 43:263–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reed EJ, Uddenberg S, Suthaharan P, Mathys CD, Taylor JR, Groman SM, Corlett PR (2020): Paranoia as a deficit in non-social belief updating. Elife 9:e56345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Leamon MH, Flower K, Salo RE, Nordahl TE, Kranzler HR, Galloway GP (2010): Methamphetamine and paranoia: The methamphetamine experience questionnaire. Am J Addict 19:155–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Groman SM, Rich KM, Smith NJ, Lee D, Taylor JR (2018): Chronic exposure to methamphetamine disrupts reinforcement-based decision making in rats. Neuropsychopharmacology 43:770–780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Browning M, Behrens TE, Jocham G, O’Reilly JX, Bishop SJ (2015): Anxious individuals have difficulty learning the causal statistics of aversive environments. Nat Neurosci 18:590–596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hein TP, de Fockert J, Ruiz MH (2021): State anxiety biases estimates of uncertainty and impairs reward learning in volatile environments. Neuroimage 224:117424. [DOI] [PubMed] [Google Scholar]
- 18.Freeman D, Bird JC, Loe BS, Kingdon D, Startup H, Clark DM, et al. (2020): The Dunn Worry Questionnaire and the Paranoia Worries Questionnaire: New assessments of worry. Psychol Med 50:771–780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bebbington PE, McBride O, Steel C, Kuipers E, Radovanovic M, Brugha T, et al. (2013): The structure of paranoia in the general population. Br J Psychiatry 202:419–427. [DOI] [PubMed] [Google Scholar]
- 20.Startup H, Freeman D, Garety PA (2007): Persecutory delusions and catastrophic worry in psychosis: Developing the understanding of delusion distress and persistence. Behav Res Ther 45:523–537. [DOI] [PubMed] [Google Scholar]
- 21.Freeman D, Dunn G, Startup H, Pugh K, Cordwell J, Mander H, et al. (2015): Effects of cognitive behaviour therapy for worry on persecutory delusions in patients with psychosis (WIT): A parallel, single-blind, randomised controlled trial with a mediation analysis. Lancet Psychiatry 2:305–313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moutoussis M, Shahar N, Hauser TU, Dolan RJ (2018): Computation in psychotherapy, or how computational psychiatry can aid learning-based psychological therapies. Comput Psychiatr 2:50–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.First MB, Spitzer RL, Gibbon M, Williams JBW (2002): Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P). New York: Columbia University. [Google Scholar]
- 24.Kay SR, Fiszbein A, Opler LA (1987): The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull 13:261–276. [DOI] [PubMed] [Google Scholar]
- 25.Haddock G, McCarron J, Tarrier N, Faragher EB (1999): Scales to measure dimensions of hallucinations and delusions: The Psychotic Symptom Rating Scales (PSYRATS). Psychol Med 29:879–889. [DOI] [PubMed] [Google Scholar]
- 26.Freeman D, Loe BS, Kingdon D, Startup H, Molodynski A, Rosebrock L, et al. (2021): The revised Green et al., Paranoid Thoughts Scale (R-GPTS): Psychometric properties, severity ranges, and clinical cut-offs. Psychol Med 51:244–253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Peters E, Joseph S, Day S, Garety P (2004): Measuring delusional ideation: The 21 -Item Peters et al. Delusions Inventory (PDI). Schizophr Bull 30:1005–1022. [DOI] [PubMed] [Google Scholar]
- 28.Fydrich T, Dowdall D, Chambless DL (1992): Reliability and validity of the Beck Anxiety Inventory. J Anxiety Disord 6:55–61. [Google Scholar]
- 29.Ehring T, Zetsche U, Weidacker K, Wahl K, Schönfeld S, Ehlers A (2011): The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. J Behav Ther Exp Psychiatry 42:225–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Heimberg RG, Horner KJ, Juster HR, Safren SA, Brown EJ, Schneier FR, Liebowitz MR (1999): Psychometric properties of the Liebowitz Social Anxiety Scale. Psychol Med 29:199–212. [DOI] [PubMed] [Google Scholar]
- 31.Beck AT, Steer RA, Brown G (1996): Beck Depression Inventory-ll. Psychol Assess. [Google Scholar]
- 32.Mathys C, Daunizeau J, Friston KJ, Stephan KE (2011): A Bayesian foundation for individual learning under uncertainty. Front Hum Neurosci 5:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mathys CD, Lomakina El, Daunizeau J, Iglesias S, Brodersen KH, Friston KJ, Stephan KE (2014): Uncertainty in perception and the Hierarchical Gaussian Filter. Front Hum Neurosci 8:825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Meng XI, Rosenthal R, Rubin DB (1992): Comparing correlated correlation coefficients. Psychol Bull 111:172–175. [Google Scholar]
- 35.Deserno L, Boehme R, Mathys C, Katthagen T, Kaminski J, Stephan KE, et al. (2020): Volatility estimates increase choice switching and relate to prefrontal activity in schizophrenia. Biol Psychiatry Cogn Neurosci Neuroimaging 5:173–183. [DOI] [PubMed] [Google Scholar]
- 36.Waltz JA (2017): The neural underpinnings of cognitive flexibility and their disruption in psychotic illness. Neuroscience 345:203–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sterzer P, Adams RA, Fletcher P, Frith C, Lawrie SM, Muckli L, et al. (2018): The predictive coding account of psychosis. Biol Psychiatry 84:634–643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Heinz A, Murray GK, Schlagenhauf F, Sterzer P, Grace AA, Waltz JA (2019): Towards a unifying cognitive, neurophysiological, and computational neuroscience account of schizophrenia. Schizophr Bull 45:1092–1100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tervo DGR, Proskurin M, Manakov M, Kabra M, Vollmer A, Branson K, Karpova AY (2014): Behavioral variability through stochastic choice and its gating by anterior cingulate cortex. Cell 159:21–32. [DOI] [PubMed] [Google Scholar]
- 40.Reddy LF, Waltz JA, Green MF, Wynn JK, Horan WP (2016): Probabilistic reversal learning in schizophrenia: Stability of deficits and potential causal mechanisms. Schizophr Bull 42:942–951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pratt DN, Barch DM, Carter CS, Gold JM, Ragland JD, Silverstein SM, MacDonald AW (2021): Reliability and replicability of implicit and explicit reinforcement learning paradigms in people with psychotic disorders. Schizophr Bull 47:731–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Freeman D (2016): Persecutory delusions: A cognitive perspective on understanding and treatment. Lancet Psychiatry 3:685–692. [DOI] [PubMed] [Google Scholar]
- 43.Lincoln TM, Peter N, Schäfer M, Moritz S (2009): Impact of stress on paranoia: An experimental investigation of moderators and mediators. Psychol Med 39:1129–1139. [DOI] [PubMed] [Google Scholar]
- 44.Coltheart M (2013): On the distinction between monothematic and polythematic delusions. Mind Lang 28:103–112. [Google Scholar]
- 45.Isham L, Griffith L, Boylan AM, Hicks A, Wilson N, Byrne R, et al. (2021) : Understanding, treating, and renaming grandiose delusions: A qualitative study. Psychol Psychother 94:119–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kendler KS, Campbell J (2009): Interventionist causal models in psychiatry: Repositioning the mind-body problem. Psychol Med 39:881–887. [DOI] [PubMed] [Google Scholar]
- 47.Croft J, Teufel C, Heron J, Fletcher PC, David AS, Lewis G, et al. (2022): A computational analysis of abnormal belief updating processes and their association with psychotic experiences and childhood trauma in a UK birth cohort. Biol Psychiatry Cogn Neurosci Neuroimaging 7:725–734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Freeman D, Stahl D, McManus S, Meltzer H, Brugha T, Wiles N, Bebbington P (2012): Insomnia, worry, anxiety and depression as predictors of the occurrence and persistence of paranoid thinking. Soc Psychiatry Psychiatr Epidemiol 47:1195–1203. [DOI] [PubMed] [Google Scholar]
- 49.Startup H, Pugh K, Dunn G, Cordwell J, Mander H, Čemis E, et al. (2016): Worry processes in patients with persecutory delusions. Br J Clin Psychol 55:387–400. [DOI] [PubMed] [Google Scholar]
- 50.Anglin DM, Ereshefsky S, Klaunig MJ, Bridgwater MA, Niendam TA, Ellman LM, et al. (2021): From womb to neighborhood: A racial analysis of social determinants of psychosis in the United States. Am J Psychiatry 178:599–610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Leeson VC, Robbins TW, Matheson E, Hutton SB, Ron MA, Barnes TRE, Joyce EM (2009): Discrimination learning, reversal, and set-shifting in first-episode schizophrenia: Stability over six years and specific associations with medication type and disorganization syndrome. Biol Psychiatry 66:586–593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.van den Bos W, Cohen MX, Kahnt T, Crone EA (2012): Striatum-medial prefrontal cortex connectivity predicts developmental changes in reinforcement learning. Cereb Cortex 22:1247–1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kühberger A, Fritz A, Scherndl T (2014): Publication bias in psychology: A diagnosis based on the correlation between effect size and sample size. PLoS One 9:e105825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dahiya AV, DeLucia E, McDonnell CG, Scarpa A (2021): A systematic review of technological approaches for autism spectrum disorder assessment in children: Implications for the COVID-19 pandemic. Res Dev Disabil 109:103852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Watt JA, Lane NE, Veroniki AA, Vyas MV, Williams C, Ramkissoon N, et al. (2021): Diagnostic accuracy of virtual cognitive assessment and testing: Systematic review and meta-analysis. J Am Geriatr Soc 69:1429–1440. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.