

Abstract
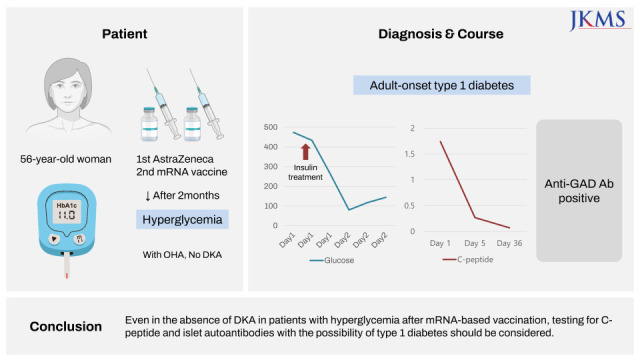
During the coronavirus disease 2019 (COVID-19) pandemic, COVID-19 vaccination-induced hyperglycemia and related complications have been reported. However, there have been few reports of type 1 diabetes triggered by COVID-19 vaccines in subjects without diabetes. Here, we report the case of a 56-year-old female patient who developed hyperglycemia after the second dose of COVID-19 mRNA-based vaccination without a prior history of diabetes. She visited our hospital with uncontrolled hyperglycemia despite administration of oral hyperglycemic agents. Her initial glycated hemoglobin level was high (11.0%), and fasting serum C-peptide level was normal. The fasting serum C-peptide level decreased to 0.269 ng/mL 5 days after admission, and the anti-glutamic acid decarboxylase antibody was positive. The patient was discharged in stable condition with insulin treatment. To our knowledge, this is the first case of the development of type 1 diabetes without diabetic ketoacidosis after mRNA-based COVID-19 vaccination, and is the oldest case of type 1 diabetes development under such circumstances.
Keywords: Type 1 Diabetes, COVID-19, Vaccination, mRNA Vaccines
Graphical Abstract
INTRODUCTION
Coronavirus disease 2019 (COVID-19) is caused by the beta coronavirus severe respiratory coronavirus syndrome coronavirus 2 (SARS-CoV-2). The pandemic of COVID-19 has a strong influence on the public health in the world. While diabetes might be a risk factor which contributes to the severity and mortality of COVID-19,1,2 new-onset diabetes and severe metabolic complications, including diabetic ketoacidosis (DKA) and hyperosmolarity have been observed in patients with COVID-19.3,4,5,6 Meanwhile, COVID-19 vaccines are the most effective strategy for prevention and reduction of severity in the event of COVID-19.6 However, there have been reports of adverse effects such as myocarditis, arrhythmia and transverse myelitis.7,8,9 COVID-19 vaccination-induced hyperglycemia and related complications were also reported.10,11 However, there have been scarce reports on type 1 diabetes triggered by COVID-19 vaccines in patients without diabetes. Here, we describe the case of adult-onset type 1 diabetes after COVID-19 mRNA vaccination without a prior history of diabetes.
CASE DESCRIPTION
A 56-year-old woman visited the outpatient department of our hospital for uncontrolled hyperglycemia in November 10, 2021. She was diagnosed with diabetes with hyperglycemia (fasting plasma glucose 371 mg/dL) in a local clinic a week before the first visit to our hospital. She had a 7-day history of thirst, polydipsia, polyuria, and weight loss, which occurred 7 days before the visit to a local clinic. Oral metformin 1,000 mg, glimepiride 8 mg, and gemigliptin 50 mg was initiated by the clinic following diagnosis. She had no history of diabetes, allergy, or autoimmune disease before the second dose of COVID-19 mRNA vaccination (Moderna®) two months prior. Her mother had a history of type 2 diabetes, but no one in her family had an autoimmune disease. She never drank alcohol nor did she smoke. She reported no evidence of diabetes in a medical checkup 6 months prior.
The patient was admitted to the hospital for insulin treatment to control hyperglycemia. Blood glucose management was initiated with subcutaneous multiple daily injections of insulin and intravenous fluid replacement. The initial glycated hemoglobin (HbA1c) level was high (11.0%) and fasting serum C-peptide level was normal (1.74 ng/mL; reference range 1.07–3.51 ng/mL) (Table 1).
Table 1. Characteristics and laboratory test results of the patient.
| Variables | Initial (Day 1) | Day 5 | Day 36 | Unit | Reference range |
|---|---|---|---|---|---|
| Age | 56 | years | |||
| Weight | 46.7 | kg | |||
| BMI | 16.95 | kg/m2 | |||
| Glucose | 371 | 121 | mg/dL | 74–106 | |
| HbA1c | 11.0 | 9.6 | % | 3.9–6.1 | |
| GA | 28.3 | % | 11–16 | ||
| BUN | 13 | mg/dL | 7–20 | ||
| Creatinine | 0.83 | mg/dL | 0.51–0.95 | ||
| AST (SGOT) | 28 | U/L | 0–35 | ||
| ALT (SGPT) | 30 | U/L | 0–35 | ||
| CO2 total | 29 | mmol/L | 21–31 | ||
| Osmolality, serum | 295 | mOsm/kg | 289–302 | ||
| Total cholesterol | 150 | mg/dL | 0–200 | ||
| Triglyceride | 52 | mg/dL | |||
| HDL-C | 69 | mg/dL | |||
| LDL-C | 66 | mg/dL | 0–130 | ||
| Fasting serum C-peptide | 1.74 | 0.269 | 0.07 | ng/mL | 1.07–3.51 |
| Urinary C-peptide (24 hr) | 17.2 | ug/day | 17.2–181 | ||
| GAD antibody | Positive (87.24) | Positive (79.29) | u/mL | Negative < 1.00 |
BMI = body mass index, HbA1c = glycated hemoglobin, GA = glycoalbumin, BUN = blood urea nitrogen, AST = aspartate aminotransferase, SGOT = serum glutamic oxaloacetic transaminase, ALT = alanine aminotransferase, SGPT = serum glutamic pyruvic transaminase, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, GAD = glutamic acid decarboxylase.
She had no fever or other symptoms before admission. Biliary computed tomography (CT) was performed to identify other causes of hyperglycemia. No abnormal pancreatic findings were observed on biliary CT (data not shown).
Her blood glucose level was well controlled with multiple daily injections of insulin. However, the fasting serum C-peptide level decreased to 0.269 ng/mL 5 days after admission, suggesting the possibility of rapid progressive type 1 diabetes. In addition, the patient was positive for anti-glutamic acid decarboxylase (GAD) antibody (Table 1). She was discharged in stable condition with insulin treatment 6 days after admission. The fasting serum C-peptide level decreased to 0.07 ng/mL and anti-GAD antibody was consecutively positive 36 days after discharge.
Ethics statement
This study was approved by the Ethics Committee of Dong-A University School of Medicine in June 2022 (subject number: DAUHIRB-22-112). The ethics committee waived the requirement for written informed consent for this case report.
DISCUSSION
We reported a case of type 1 diabetes development following COVID-19 mRNA-based vaccination. The patient, a woman in her mid-50s, had no history of diabetes, but presented with hyperglycemia and was positive for anti-GAD antibody 2 months after the second dose of COVID-19 mRNA-based vaccines. Her history and laboratory results indicated a diagnosis of type 1 diabetes. In general, adult-onset type 1 diabetes exhibits unique features when compared to childhood or adolescent-onset type 1 diabetes including higher beta-cell function at the onset and slower rate of beta-cell deterioration.12 As there is a wide spectrum of fasting serum C-peptide values at the time of clinical diagnosis, fasting serum C-peptide values in those diagnosed with type 1 diabetes may be within the normal range at the time of diagnosis.13
Diabetes has been identified as a risk factor contributing to the severity and mortality of COVID-191,2 and COVID-19 may enhance complications in patients with diabetes.14 Severe metabolic complications, including DKA and hyperosmolarity have been observed in patients with diabetes infected with COVID-19.3,4,5 In addition, SARS-CoV-2 has been suggested to be a potential inducer of new-onset type 1 diabetes.15 Recently, a few new-onset diabetes cases have been reported following COVID-19 vaccination.10,16 A prior study described three cases of acute hyperglycemia 20–36 days after administration of the first dose of the COVID-19 vaccine (AstraZeneca®) in obese male patients (two of whom were already prediabetic).10 A case of fulminant type 1 diabetes following COVID-19 RNA-based vaccination has also been reported.16 This case report is characterized by no history of diabetes, rapid-onset DKA with a low HbA1c value, and negative islet-related autoantibodies 10 days after the first dose of COVID-19 vaccination.16 Another case report described new-onset type 1 diabetes in a 51-year-old woman with DKA after COVID-19 RNA vaccination.15 She had hyperglycemic symptoms, including polydipsia and weight loss after the second dose of vaccination, with a high HbA1c value and positive insulin autoantibody.17 In the two cases described above, type 1 diabetes was diagnosed with DKA. However, in our patient, diabetes was diagnosed without DKA or severe hyperglycemic symptoms, and endogenous insulin secretion was preserved on admission, unlike typical type 1 diabetes. For this reason, it is possible that the initial diagnosis was delayed due to a high HbA1c level on admission. Although it cannot be ruled out that the COVID-19 vaccination may have worsened the hidden diabetes, it is possible that hyperglycemia developed after she received the second dose of the vaccine, given that there was no evidence of diabetes in the medical checkup 6 months prior. In all three cases, including the two Japanese cases and our case, all diabetes cases occurred in East Asian women with unknown etiology. Among these cases, our patient was diagnosed with diabetes at the oldest age.
In addition to type 1 diabetes, other new-onset autoimmune diseases after COVID-19 vaccination have been reported increasingly (e.g., Guillain-Barré syndrome, immune thrombotic thrombocytopenia, rheumatoid arthritis and Graves’ disease).18
The autoimmune/inflammatory syndrome induced by adjuvants, defines a disease entity including a broad spectrum of autoimmune/inflammatory conditions.18 Autoimmune type 1 diabetes have been reported to be caused by vaccines other than the COVID-19 vaccine, HBV (11 cases) and HPV vaccine (2 cases).18
The mechanisms of autoimmune activation triggered by COVID-19 vaccine is unclear. Vaccine adjuvants can increase both innate and adoptive immune responses.18 Molecular mimicry, the production of specific autoantibodies against pancreatic islet cells also seems to be a contributor to autoimmune phenomena.18
SARS-CoV-2 pathogenesis involves viral S protein utilization of the cellular angiotensin-converting enzyme 2 (ACE2) receptor.19 Despite uncertainty regarding the exact mechanism, ACE2 receptors, which are expressed in various metabolic tissues, such as pancreatic beta cells, have been implicated in impaired glucose homeostasis.3 Renin-angiotensin system (RAS) hyperactivity via ACE2 receptor downregulation following viral entry may impair insulin receptor signalling.20 In addition, RAS hyperactivity decreases perfusion of the pancreatic tissue, reduces insulin production, and increases oxidative stress resulting in fibrosis.21 It is possible that similar responses follow SARS-CoV-2 antigen presentation after vaccination.
Sakurai et al.16 suggested one possible explanation involving an association between melanoma differentiation-associated protein 5 (MDA5) and β-cell function. MDA5 is an innate pathogen recognition protein. If MDA5 recognizes RNA, type I interferons that impair insulin production, proinsulin conversion, and mitochondrial function in pancreatic β-cells are synthesized.22 It is plausible that MDA5 recognizes the RNA derived from COVID-19 RNA-based vaccines.
The association between acute rapid-onset type 1 diabetes and COVID-19 vaccine may be just coincidental, or the vaccines might be more likely to induce new onset type 1 diabetes than other vaccines. It is necessary to find out the possibility of causal relationship between them.
In summary, as far as we know, this is the first case of acute rapidly onset type 1 diabetes who did not develop DKA after mRNA-based vaccination in the mid-50’s. Our case report suggested that COVID-19 vaccination could provoke adult-onset type 1 diabetes in those who were vaccinated in subjects without history of diabetes. Even in the absence of DKA in patients with hyperglycemia after mRNA-based vaccination, testing for fasting serum C-peptide and islet autoantibodies with the possibility of type 1 diabetes should be considered.
ACKNOWLEDGMENTS
The authors thank Dong-A University, for funding for English language editing.
Footnotes
Funding: This case was supported by Dong-A University Research fund 2022.
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Moon H, Suh S, Park MK.
- Writing - original draft: Moon H.
- Writing - review & editing: Moon H, Suh S, Park MK.
References
- 1.Gregory JM, Slaughter JC, Duffus SH, Smith TJ, LeStourgeon LM, Jaser SS, et al. COVID-19 severity is tripled in the diabetes community: a prospective analysis of the pandemic’s impact in type 1 and type 2 diabetes. Diabetes Care. 2021;44(2):526–532. doi: 10.2337/dc20-2260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.COVID-19 National Emergency Response Center, Epidemiology and Case Management Team, Korea Centers for Disease Control and Prevention. Coronavirus disease-19: the first 7,755 cases in the Republic of Korea. Osong Public Health Res Perspect. 2020;11(2):85–90. doi: 10.24171/j.phrp.2020.11.2.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rubino F, Amiel SA, Zimmet P, Alberti G, Bornstein S, Eckel RH, et al. New-onset diabetes in COVID-19. N Engl J Med. 2020;383(8):789–790. doi: 10.1056/NEJMc2018688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chung SM, Lee YY, Ha E, Yoon JS, Won KC, Lee HW, et al. The risk of diabetes on clinical outcomes in patients with coronavirus disease 2019: a retrospective cohort study. Diabetes Metab J. 2020;44(3):405–413. doi: 10.4093/dmj.2020.0105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim NY, Ha E, Moon JS, Lee YH, Choi EY. Acute hyperglycemic crises with coronavirus disease-19: case reports. Diabetes Metab J. 2020;44(2):349–353. doi: 10.4093/dmj.2020.0091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ku CR, Jung KY, Ahn CH, Moon JS, Lee JH, Kim EH, et al. COVID-19 vaccination for endocrine patients: a position statement from the Korean Endocrine Society. Endocrinol Metab. 2021;36(4):757–765. doi: 10.3803/EnM.2021.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kim IC, Kim H, Lee HJ, Kim JY, Kim JY. Cardiac imaging of acute myocarditis following COVID-19 mRNA vaccination. J Korean Med Sci. 2021;36(32):e229. doi: 10.3346/jkms.2021.36.e229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lim KH, Park JS. COVID-19 vaccination-induced ventricular fibrillation in an afebrile patient with Brugada syndrome. J Korean Med Sci. 2022;37(42):e306. doi: 10.3346/jkms.2022.37.e306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Finsterer J, Matovu D. Consider transverse myelitis as a complication of a SARS-CoV-2 vaccination. J Korean Med Sci. 2022;37(18):e150. doi: 10.3346/jkms.2022.37.e150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Edwards AE, Vathenen R, Henson SM, Finer S, Gunganah K. Acute hyperglycaemic crisis after vaccination against COVID-19: a case series. Diabet Med. 2021;38(11):e14631. doi: 10.1111/dme.14631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee HJ, Sajan A, Tomer Y. Hyperglycemic emergencies associated with COVID-19 vaccination: a case series and discussion. J Endocr Soc. 2021;5(11):bvab141. doi: 10.1210/jendso/bvab141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Karjalainen J, Salmela P, Ilonen J, Surcel HM, Knip M. A comparison of childhood and adult type I diabetes mellitus. N Engl J Med. 1989;320(14):881–886. doi: 10.1056/NEJM198904063201401. [DOI] [PubMed] [Google Scholar]
- 13.VanBuecken DE, Greenbaum CJ. Residual C-peptide in type 1 diabetes: what do we really know? Pediatr Diabetes. 2014;15(2):84–90. doi: 10.1111/pedi.12135. [DOI] [PubMed] [Google Scholar]
- 14.Cuschieri S, Grech S. COVID-19 and diabetes: the why, the what and the how. J Diabetes Complications. 2020;34(9):107637. doi: 10.1016/j.jdiacomp.2020.107637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Boddu SK, Aurangabadkar G, Kuchay MS. New onset diabetes, type 1 diabetes and COVID-19. Diabetes Metab Syndr. 2020;14(6):2211–2217. doi: 10.1016/j.dsx.2020.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sakurai K, Narita D, Saito N, Ueno T, Sato R, Niitsuma S, et al. Type 1 diabetes mellitus following COVID-19 RNA-based vaccine. J Diabetes Investig. 2022;13(7):1290–1292. doi: 10.1111/jdi.13781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yano M, Morioka T, Natsuki Y, Sasaki K, Kakutani Y, Ochi A, et al. New-onset type 1 diabetes after COVID-19 mRNA vaccination. Intern Med. 2022;61(8):1197–1200. doi: 10.2169/internalmedicine.9004-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Watad A, Bragazzi NL, McGonagle D, Adawi M, Bridgewood C, Damiani G, et al. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) demonstrates distinct autoimmune and autoinflammatory disease associations according to the adjuvant subtype: insights from an analysis of 500 cases. Clin Immunol. 2019;203:1–8. doi: 10.1016/j.clim.2019.03.007. [DOI] [PubMed] [Google Scholar]
- 19.Müller JA, Groß R, Conzelmann C, Krüger J, Merle U, Steinhart J, et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nat Metab. 2021;3(2):149–165. doi: 10.1038/s42255-021-00347-1. [DOI] [PubMed] [Google Scholar]
- 20.Sathish T, Tapp RJ, Cooper ME, Zimmet P. Potential metabolic and inflammatory pathways between COVID-19 and new-onset diabetes. Diabetes Metab. 2021;47(2):101204. doi: 10.1016/j.diabet.2020.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bindom SM, Lazartigues E. The sweeter side of ACE2: physiological evidence for a role in diabetes. Mol Cell Endocrinol. 2009;302(2):193–202. doi: 10.1016/j.mce.2008.09.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Blum SI, Tse HM. Innate viral sensor MDA5 and coxsackievirus interplay in type 1 diabetes development. Microorganisms. 2020;8(7):993. doi: 10.3390/microorganisms8070993. [DOI] [PMC free article] [PubMed] [Google Scholar]