

Abstract
The effectiveness of eccentric exercise interventions (EEI) has been extensively explored in different populations. The aim of our umbrella review was to combine all systematic reviews about the chronic efficiency of EEI and to summarize the literature on the chronic effects of different types of eccentric exercise protocols, with or without extra loads and devices (e.g., Flywheel device), compared to other therapeutic interventions, exercise interventions, or no intervention. We screened four major electronic scientific databases (PubMed, Scopus, Web of Science, and PEDro), using one combined string for all included databases (eccentric exercise OR flywheel OR isoinertial exercise OR eccentric training). Included reviews needed to be based on any human population, that executed EEI in comparison with any other type of intervention. The methodological quality of the included reviews was assessed using AMSTAR 2 tool. Considering the inclusion criteria, we included 35 reviews. EEI were found suitable for chronic or long-term pain reduction in patient populations. EEI largely improved muscle performance (muscle strength, and muscle power), muscle architecture (e.g., pennation angle, fascicle length, cross-sectional area, muscle thickness, and muscle mass), decreased risk of injury, incidence, and severity of the injury, and increased range of motion of the joints There is less evidence about the effects of EEI in older adult populations, compared to athletes and younger populations, however, eccentric exercise seems promising for these populations as well.
Key Words: Eccentric contraction, eccentric exercise, muscle strength, muscle architecture
Ethical Publication Statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Human movement is achieved by muscle contraction, which is roughly divided into three types based on the change of muscle-unit complex: isometric, concentric, and eccentric. Isometric contraction is characterized by unchanging muscle length, concentric contraction is characterized by a shortening of the muscle,1 and an eccentric contraction occurs when the muscle lengthens to maintain a certain load or because external load/resistance becomes greater than the force that is produced by the muscle.1,2 By eccentric contraction, the muscle can produce greater force than by concentric contraction.3 Specifically, with eccentric contraction, the muscle is capable of producing the force to resist the loads up to 130% of the maximal concentric force.3 For the same absolute force, fewer muscle fibers are activated during an eccentric contraction, which need lower oxygen consumption (VO2),4–6 lower minute ventilation, and lower carbon dioxide production.6 Therefore, eccentric exercise causes a lower metabolic load of the body.4 Moreover, greater muscle strength gains and muscular hypertrophy seem to be achieved with eccentric compared to concentric cycling training, at a given heart rate or VO2.7 That is why the use of eccentric or eccentric-emphasized exercise is attractive in populations in which high metabolic demand or high VO2 is not desirable.8 However, the execution of eccentric exercise causes muscle damage and associated delayed onset muscular soreness.9 Consequently, eccentric load needs to be cautiously determined to limit delayed onset muscular soreness and also maximize training compliance and exercise tolerance.9 Since a greater load on the muscle-tendon unit can be achieved during an eccentric contraction, compared to a concentric or an isometric contraction, the excessive eccentric load of the muscle and/or tendon is one of the most common mechanisms of musculotendinous injury, because muscle and/or tendon cannot resist without getting injured.10 So the most common muscle injuries in the athlete population are injuries of knee flexors, hip adductors, and knee extensors and are caused because of excessive eccentric loads.10 Knee flexors injuries often occur during running, most often at the end of the swing phase of the running cycle, when the knee flexors are contracted eccentrically under high loads to limit knee extension and hip flexion.11 On the other hand, the mechanism of injury of hip adductors is a combination of high eccentric loads with simultaneous rapid stretching of the muscle-tendon unit,12 whereas injury of knee extensor occurs because of sudden eccentric loading of knee extensors while kicking.13,14 When we eccentrically load an activated muscle, that is lengthened beyond its optimum length, the risk of injury increases.15 Therefore, it seems reasonable that prevention and rehabilitation programs should emphasize eccentric loading to condition the muscle for high-eccentric loads.16–18 Indeed, eccentric exercises have been showing great potential as a part of a rehabilitation or prevention program. Hooper thinks that eccentric training/exercise can be categorized into three different categories.19 The first is “plyometric exercises” which consist of movements like drop jumps with extremely short contraction (which lasts milliseconds) by which a large amount of force is created.19 The second category of eccentric training is “classic eccentric resistance exercises” which contains protocols of almost-maximal eccentric contractions that last no more than a few seconds and are used to lift and lower weights like deadlift exercise or squats with a flywheel device.19 The last category is called “continuous moderate load eccentric exercises” and is characterized by movements wherein an external load is greater than the force produced by the muscle which can be observed while executing Nordic hamstring exercise.19,20 In scientific databases, a large number of systematic reviews that are focusing on the chronic effects (≥ 4 weeks) of eccentric exercise interventions (EEI) in different populations can be found.17,21–23 That is why the aim of this umbrella review is to combine all systematic reviews about the chronic efficiency of EEI (on human muscle performance, functional performance, muscle architecture, etc.) and to find out the most common effects of eccentric interventions between different types of eccentric exercise protocols with or without extra loads and devices (e.g., Flywheel device) or compared to other therapeutic interventions, exercise interventions or also to no intervention at all.
Materials and Methods
Information sources and search strategy
The search was performed in October 2021. Four major electronic scientific databases (PubMed, Scopus, Web of Science, and the Physiotherapy Evidence Database – PEDro) were screened. The search included all studies written in the English language, regardless of the year of publication. The terms used in the electronic search were: eccentric exercise, flywheel, isoinertial exercise, and eccentric training. Where possible (all databases except PEDro), the terms were combined into one string: eccentric exercise OR flywheel OR isoinertial exercise OR eccentric training. The databases search was performed by two reviewers. The search strategy was carried out in three stages: 1) assessing the eligibility of the papers based on the title, 2) assessing the eligibility of the papers based on the abstract, and 3) assessing the eligibility of the papers based on the full-text. All three stages were carried out by two reviewers independently. Any disagreements were resolved by additional discussion and consultation with a third reviewer. None of the authors were contacted for additional data.
Eligibility criteria
The inclusion criteria are structured according to the PICOS tool:24
P (population): Human population, regardless of their age, sports activities, and presence/absence of pathology.
I (intervention): Different exercise interventions focusing on (or emphasizing) eccentric contraction. This includes flywheel overload training, heavy load eccentric training, eccentric cycling, eccentric overload training, and eccentric or concentric-eccentric exercises by an isokinetic dynamometer.
C (comparison): Traditional physiotherapy (cross-friction massage, ultrasound, TENS, Cyriax physiotherapy, and bioptron light), mobilization (splinting), adjuvant therapy (heat, ice, heat, bands, massage, and stretching), passive interventions, or other exercise programs included traditional training, resistance exercise or heavy slow resistance training emphasizing concentric or in some cases isometric contraction or operative treatment of the problem in one of the reviews.
O (outcome): Outcomes describing muscle performance (muscle strength or power), functional performance (speed, jumping, change of direction, muscle shortening cycle, and change of direction), muscle architecture (fascicle length, cross-sectional area, pennation angle, muscle thickness, and muscle mass), risk of injury and its incidence and severity, pain reduction, range of motion, etc.
S (Study design): Systematic reviews (with or without meta-analyses). Narrative reviews were excluded.
Data extraction and analysis
The data extraction was performed by one reviewer, with additional help from the other reviewers, one of which supervised and re-reviewed extracted data. In case of dilemmas, these were resolved in consultation with other authors. From the included articles we extracted and analyzed: (a) the number of included studies in a systematic review and/or meta-analysis, (b) the main characteristics of participants (gender, age, sports activity, pathology, etc.), (c) intervention characteristics (target body area [upper, lower or whole-body]), (d) specialties about exercise programs (comparison between eccentric exercise and other interventions), (e) output variables (muscle performance, functional performance, muscle architecture, pain reduction, etc.), and (f) summary of key findings. The studies were qualitatively analyzed and compared. The results section describes the literature search and methodological assessment of the study, and briefly outlines the general findings, with studied separated by population of interest. In the discussion section, the findings are presented in more detail. Here, the included articles are again divided by population on the first level (patients, athletes, older adults and other/general population). We further divided the patient population based on the pathology/injury of interest. In athletes, a more logical step was to separately compare different types of eccentric exercise (Nordic hamstring exercise, flywheel exercise). We did not separate the reviews concerning older adults. The reviews concerning fundamental questions or general population were divided into those summarizing the effects of eccentric exercise on muscle structure or muscle/movement function
Fig 1.
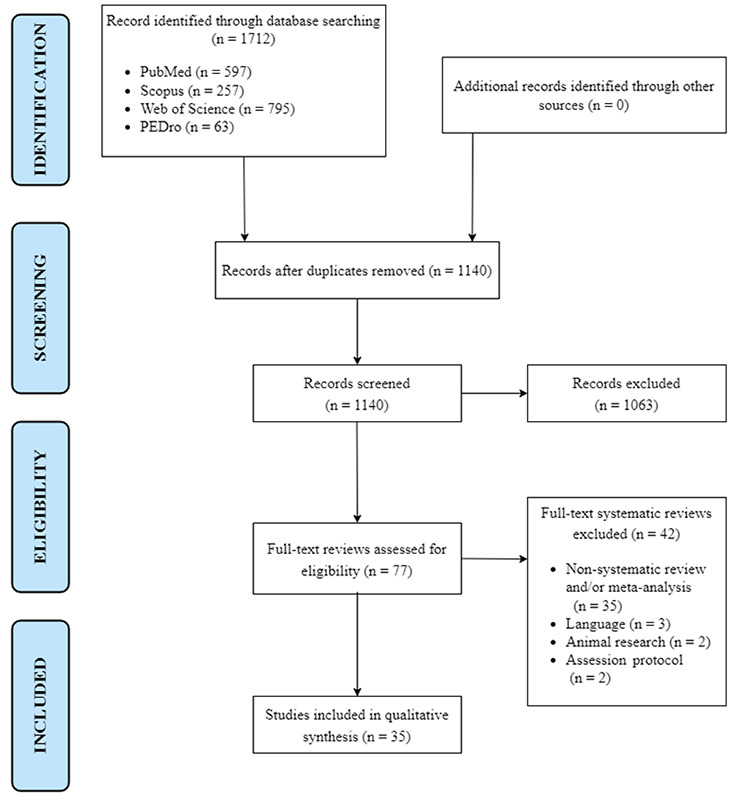
Flowchart of the selection of studies.
Methodological quality assessment
The methodological quality of the included systematic reviews and/or meta-analyses were assessed by one reviewer, using the Assessment of Multiple Systematic Reviews 2 tool (AMSTAR 2).25,26 It is a critical appraisal tool for systematic reviews which include randomized and/or non-randomized studies of healthcare interventions.26 In the assessment process, the AMSTAR 2 guidance document was used as an aid in interpreting the items. The AMSTAR 2 tool contains 16 items, of which 7 are critical domains, selected according to our field of research.26 We have decided that items 1, 3, 8, 9, 11, 14, and 15 are critical domains that are important for our field of research. The rating of overall confidence was categorized, depending on fulfilled criteria:26
High: no or one non-critical weakness;
Moderate: more than one non-critical weakness, multiple non-critical weaknesses may diminish confidence in the review, and it may be appropriate to move the overall appraisal down from moderate to low confidence;
Low: one critical flaw with or without non-critical weaknesses;
Critically Low: more than one critical flaw with or without non-critical weaknesses.
Results
Selection of studies
The data from PubMed (n = 597), Scopus (n = 257), Web of Science (n = 795), and PEDro (n = 63) was compilated, managed, and imported into Mendeley (version 1.19.8) (Mendeley, London, United Kingdom) to remove the duplicates, and exported into Microsoft Excel software (Microsoft, Redmond, Washington, USA) (n = 1140). Of these 1140 reviews and/or meta-analysis, 1063 were inappropriate and were excluded based on the title and/or abstract, leaving 77 potential reviews. Among the 77 reviews, 42 reviews were excluded due to not meeting the eligibility criteria. Thirty-seven studies of which were excluded because the reviews were not systematic reviews and/or meta-analysis, 3 were excluded due to not meeting language criteria (were in German or Spanish). Thus, a total of 35 systematic reviews and/or meta-analysis were included in the current umbrella review. The process of study selection is presented in Figure 1.
Methodological quality assessment of studies.
The results were presented as the rating of overall confidence in the range of critically low overall confidence and high overall confidence (See Supplementary Materials: Table 1.). Sixteen studies had a critically low rating of overall confidence,22,27–41 thirteen had a low rating of overall confidence,6,17,23,42–51 no studies had a moderate rating of overall confidence, and 6 had a high rating of overall confidence.21,52–56
Eleven out of 35 reviews were not limited to studies that included a control group to compare outcomes obtained between the experimental group (which implemented eccentric exercise) and the control group(/-s) (which implemented other types of therapies, other exercise interventions, or no intervention at all). Eight studies contained registered protocol, a meta-analysis/synthesis plan, a plan for investigating causes of heterogeneity, and justification for any deviations from the protocol. On the other hand, four studies did not include any of the aforementioned elements nor review question(s), a search strategy, inclusion/exclusion criteria, and/or a risk of bias assessment. Thirty-one studies had included only randomized controlled trials and/or non-randomized studies of the intervention. Eleven studies did not describe the included studies in adequate detail, because of a lack of comparators, while 11 studies described all assumptions in detail, and 13 studies partially described the study’s population, interventions, comparators, outcomes, and research design. The satisfactory technique for assessing the risk of bias was (at least) partially used in 24 out of 35 cases. Meta-analysis was included in eighteen studies of which 13 included appropriate methods for statistical combination of results. On the other hand, only 6 out of 18 studies, that included meta-analysis, carried out an adequate investigation of publication bias and discussed its likely impact on the results of the study. Any observed heterogeneity was explained and discussed in 23 studies, while 12 studies did not contain the mentioned content (See Supplementary Materials: Table 1).
Key findings
Patients population
This umbrella review consists of 14 systematic reviews and meta-analyses that focused on the effects of eccentric exercise in the patient populations (See Supplementary Materials: Table 2). It was found that eccentric exercise provides better results for treating tendinosis compared to adjuvant therapies (ultrasound, brace, stretching, ice, heat, or massage).50 Implementation of eccentric exercises in the individual’s training program can reduce tendinosis-related pain within 12 weeks.50 Eccentric exercise was found superior for decreasing pain levels for patients with shoulder tendinopathies,47 lateral epicondylitis,30,51,56 and patellar tendinopathy.34 It was found that pain reduction can be achieved even without any harmful effects resulting from eccentric exercise.34,47 Eccentric exercises were found more suitable for chronic or long-term pain reduction and improvement in knee function, while isometric exercises were found more appropriate for acute or short-term pain relief.35 The effects of regular eccentric exercise were found even at 6 months and 1-year follow-ups.47 Eccentric exercise (compared with adjuvant therapy) also greatly increased the grip muscle strength of patients with lateral epicondylitis compared to the same adjuvant therapies exclusive of eccentric exercise,30,51 or compared to concentric exercise combined with adjuvant therapy.51 The execution of eccentric resistance exercise increased cross-sectional area and strength of the muscle within 2-4 weeks for patients with rotator cuff tendinopathy.52 On the other hand, eccentric cycling was found to be an effective training protocol that significantly improved VO2,6,44 heart rate, and power output compared to baseline results for patients with cardio-respiratory and other chronic health conditions or ischemic heart disease, however, the effects were comparable to the effects of concentric exercise interventions.6,44
Athletes population
The umbrella review included 8 systematic reviews and meta-analyses relating to the athletes’ population (See Supplementary Materials: Table 3). Large-to-very large reduction in pennation angle,31 and increase in eccentric strength, and fascicle length were found and they can be achieved with high and also low volume prescriptions of exercise,28,31 but effect sizes generally favored the group that performed a higher training volume in minimal duration over 6 weeks.28 On the other hand, a training protocol using a flywheel device improved T-Test agility, Y-agility, change of direction, sprinting, and jumping performance.27 It was also found that flywheel training increased both eccentric27,39 and concentric strength when compared pre- to post-test results.27 Bautista et al.28 found out that after performing the Nordic hamstring exercise protocol sprint performance (on 5 m, 10 m, or 20 m distance) improved approximately by 0.04 s (0.01-0.08 s) compared to measurements taken before the start of the intervention. In the case of well-trained team sport athletes, body mass explained more than 90% of the variance in the effect size of eccentric strength of knee flexors.28 It was also found that the implementation of exercise in the warm-up protocol can reduce the probability of hamstring strain by 51 %.42
Older adult population
We included 2 systematic reviews and meta-analyses that focused on the older adult population (See Supplementary Materials: Table 4). It was found that eccentric intervention improved the balance, mobility, and endurance of older adults.21 But the difference between improvements after the eccentric and concentric intervention is minimal.21 Eccentric interventions also lower the incidence of falls to a greater extent than concentric interventions.21 The large effect size of muscle strength for the eccentric focused training in the pre-training versus post-training comparison was observed.55 It was also found that eccentric-focused training greatly increased muscle strength and cross-sectional area of the muscle compared to the combination of concentric and isometric training.55
Other reviews
This umbrella review included 11 systematic reviews and meta-analyses, which were not specific to any population (See Supplementary Materials: Table 5). The increase of the muscle volume and muscle strength after implementing eccentric exercise was found significantly higher compared with the concentric exercise.36 Greater forces that were produced by an eccentric contraction provided greater muscle damage resulting in greater muscle hypertrophy.32,36 Executing eccentric exercise was found to increase muscle cross-sectional, and distal muscle size, especially the fast-twitch muscle fibers to a greater range compared to concentric exercise.32,33,38,41 Nevertheless, authors23,32 pointed more solutions, how to achieve the greatest increase in cross-sectional area. Douglas et al.32 thought that the greatest increases of the cross-sectional area can be achieved by rising velocities of exercises and/or by following heavier eccentric training protocol. On the other hand, Roig et al.23 thought that the greatest increase in the cross-sectional area can be obtained especially at higher levels of intensity of the eccentric resistance training. Eccentric training also greatly increased fascicle length compared to baseline results,32,33 while greater increase of fascicle length was observed even when comparing the eccentric training results with a group that was executing concentric training.32 Emirzeoğlu et al.33 added that the increase inside of eccentric group was found independent of duration, frequency of intervention, and the number of repetitions. It was found that hamstring fascicle length increased greatly when Nordic hamstring exercise was implemented in the warm-up (before the training session), while muscle thickness and pennation angle increased greatly after implementing Nordic hamstring exercise after the training session.53 Other authors39 found out that eccentric exercise moderately improved isometric strength, largely improved the power of knee extensors, and very largely improved tendon stiffness, velocity, mobility, and balance in the older adults population.
Discussion
Reviews concerning patients’ population
Tendinopathy
Wasielewski and Kotsko found that eccentric exercise was more effective than other types of adjuvant therapy (splinting, friction massage, and non-thermal ultrasound) for treating tendinosis, but the comparisons with other exercise types were inconclusive.50 Reduction of tendinosis-related pain can be achieved within 12 weeks of the execution of eccentric exercise.50 It was also found that performing the 12-week eccentric exercise program stimulated collagen synthesis, but did not change the rate of collagen degradation.50 On the other hand, Ortega-Castillo and Medina-Porqueres established that the eccentric exercises were very much effective for the treatment of upper limb tendinopathies, but their superiority against other methods (different types of exercises with or without extra accessories, stretching, and different manual-therapeutic protocols) was again not clear.48
Shoulder tendinopathies
It was found that eccentric exercise did not provide a better effect on the function of the shoulder for patients diagnosed with subacromial impingement syndrome compared to other interventions (massage, mobilization, manipulation, TENS, and corticosteroid injections), but the influence of eccentric exercise on pain reduction was greater even 6 months or 1 year after the eccentric exercise program ended.47 The effectiveness of the pain-free eccentric exercise on pain reduction and muscle function was found as effective as eccentric exercise accompanied by pain (painful eccentric exercise), but higher intensities might yield a better outcome.47
Comparable outstanding results of the effectiveness of eccentric exercise (combination of external rotation in supine with shoulder 90° abduction and eccentric phase of abduction in the scapular plane until 90°) compared to the conventional exercise program (typical exercise program for rotator-cuff tendinopathy; e.g. shoulder shrugs, knee push-up, horizontal abduction in a prone position with external rotation…) were obtained in the other systematic review.52 The authors suggested that the patients need to concentrate on the appropriate amount of load, rather than the method of physical exercise.52 It was also found that an increase in cross-sectional area in skeletal muscle for patients with rotator cuff tendinopathy can be achieved with the 2-4 weeks of performing eccentric resistance exercise.52
Lateral epicondylitis
Yoon et al.51 found that the eccentric exercises showed the best effects on pain reduction compared to concentric or isotonic exercises, but there were no significant differences in function and muscle strength between the results of experimental (eccentric exercise protocol with or without adjuvant therapy) and control group (adjuvant therapy with or without concentric or isotonic exercise). In all other reviews, the authors found that eccentric exercise (combined or non-combined with adjunctive therapy, like stretching, massage, heat and ice, or ultrasound) both decreased pain as well as an increased grip or muscle strength and improved function of elbow and wrist for patients with lateral epicondylitis when comparing pre- to post-tests results even at 1-year follow-up.30,56 So it was found that eccentric exercise can produce a greater outcome of pain reduction for patients who had problems with lateral epicondylitis than any other exercise (concentric exercise, isotonic exercise, or stretching) or therapy program (e.g. massage, heat and ice, TENS, ultrasound, or forearm banding) without the use of eccentric exercise.30,51,56 Ramen et al.49 added that the eccentric exercise protocol needs to be supervised to produce the greatest decrease of pain, improvement of function, and increase of pain-free grip strength and that the evidence of the aforementioned variables was moderate. Moderate evidence also showed that return to activity was better after receiving the EEI program than the concentric exercise intervention program.56 It was also found that the duration of lateral epicondylitis symptoms does not affect the decrease of pain after executing eccentric exercise protocol, compared to pre- to post-test results, measured by the Visual Analog Scale.49
Patellar tendinopathy
EEI reduced pain associated with patellar tendinopathy from the baseline without any harmful effects.34 A 4-week eccentric exercise program (eccentric squat or eccentric quadriceps training on a 25° decline board) for the rehabilitation of patellar tendinopathy was found better in reducing pain than passive interventions (ultrasound or transverse friction).35 It was also found that isometric exercise provided better acute or short-term pain reduction, whereas eccentric exercise showed greater results in chronic or long-term pain reduction (up to 1 year).35 A limited level of evidence showed that pain reduction in patellar tendinopathy can be achieved by following a 12-week EEI program, which included eccentric quadriceps training on a decline board, compared to a concentric exercise intervention programs.56 Eccentric exercise groups showed similar or greater improvements in function compared with other interventions and group programs.35
Achilles tendinopathy
Greater effects for treating patients with Achilles tendinopathy (reducing pain, returning patients to normal life activity) can be achieved by the implementation of eccentric exercises compared to implementing concentric exercises and/or ultrasound.56 Frizziero et al.34 found out that Silbernagel combined protocol seems as effective as isolated eccentric muscle training for Achilles tendinopathy treatment, especially in satisfaction, and improvements in ankle range of motion. In mid-portion Achilles tendinopathy, the combination of eccentric exercise and extracorporeal shock wave therapy is more effective than eccentric exercise alone in function improvement, pain reduction, and satisfaction.34 On the other hand, in insertional tendinopathy combination of extracorporeal shock wave therapy with cold air and high-energy laser therapy led to a greater decrease of pain compared to eccentric exercise and stretching program at 2 and 6 months follow-up.34 Better results of function improvement at 16-week follow-up were observed with heavy eccentric calf training protocol, compared to natural history or traditional physiotherapy, however, the results are inconclusive, because of the lack of strong evidence which can be provided by more research-oriented articles with a greater test battery.22
Cardio-respiratory and other chronic health conditions, ischemic heart disease Restoring musculoskeletal function without stressing the cardiopulmonary system can be achievable with eccentric actions.40 It was found that the eccentric exercise program (which consisted out of 3 sessions per week for 5-8 weeks) significantly improved VO2, heart rate, and power output compared to the baseline results, but there were no significant differences between results following EEI and concentric exercise intervention.6 In another review, eccentric training intervention did not show any significant differences in the level of maximal oxygen consumption after training compared to the level of maximal oxygen consumption after the concentric training intervention.44 Eccentric exercise also showed moderate to weak evidence of the effectiveness for improvement of functional capacity for ischemic cardiac patients.44
Reviews concerning athlete population
Eccentric training is often used in the athletes’ population as part of prevention or rehabilitation programs. Implementing eccentric exercise in training protocols, can cause an improvement of muscle performance (strength and power), decrease the risk of injury, improve moving efficiency (jumping, sprinting, change of direction, T-Test agility, etc.), pain reduction, and muscle architecture. Large-to-very large reduction of pennationa angle,31 and increase of eccentric strength, and fascicle length were found and those outcomes can be achieved with high and also low volume prescriptions of Nordic hamstring exercise (32 repetitions per week),28,31 but effect sizes generally favored the individuals that performed a higher training volume over a minimum duration of 6 weeks.31 It was found that lowering training volume does not necessarily elicit smaller effects on muscles.31 The main idea is to gradually increase the intensity of eccentric training just like in traditional strength training, but training volume must be constant.31 On the other hand, eccentric training protocol (supramaximal eccentric training) did not improve lower-body concentric 1RM more effectively than traditional training methods, which were characterized by submaximal loads (85% ±15% of concentric 1RM) moved throughout the concentric and eccentric phases of repetition cycle.29 It was however found that the risk of a hamstring injury can be significantly decreased by 65% following eccentric hamstring strengthening protocol, but the evidence is insufficient because of decreased compliance of the intervention that was connected to effects of delayed onset muscular soreness.17 Eccentric interventions integrate different exercise devices, different exercise methods, or specific eccentric exercises in the training program. The most widespread devices are Flywheel devices and isokinetic dynamometers, while the different methods have been named eccentric overload training, eccentric inertial overload resistance training, heavy eccentric training, supramaximal eccentric training, and loaded eccentric jump training protocol. On the other hand, some of the most common and recognizable eccentric exercises in training protocol are Nordic hamstring exercise, Hamstrings curl, knee-flexion exercise, and hip-extension exercise.
Efficiency following training protocol using flywheel device
Following training protocol using flywheel devices has a lot of positive effects.27 It improves T-Test agility, Y-agility, change of direction, sprinting, and jumping performance, elicits hypertrophic adaptations, and caused higher electromyographic activity.27 It was found that flywheel resistance training interventions that took place 2-3 times per week improved jumping ability with moderate effect size (effect size = 0.65), while a change of directions improvements was also statistically significant compared to baseline results.46 Following training protocols using a flywheel device effectively increased both, concentric and eccentric isokinetic strength (of knee flexors).27 Flywheel training also increased muscle power and produced greater storage of elastic energy which provided greater force output during jumping and change of direction performance compared to plyometric training.27 Flywheel resistance training greatly increased muscle size and strength compared to traditional resistance training, which is why the individuals that executed flywheel resistance training achieved greater forces during the eccentric contraction of the muscle.46 All, jumping performance, sprinting time, and change of direction performance improved greater after achieving high velocities of the eccentric phase.46
Efficiency following the Nordic hamstring exercise protocol
Integrating Nordic hamstring exercise (alone or in conjunction with other eccentric exercises for knee flexors) in warm-up protocol decreases the probability of hamstring strain injury for football players by 51 % in a long term, compared with football players that did not execute the Nordic hamstring exercise integrated into the warm-up protocol.42 Nordic hamstring exercise also improved sprint performance on 5 m, 10 m, or 20 m distance (approximately by 0.04 s [0.01, 0.08]) and increased eccentric strength of knee flexors compared to measurements taken before the start of the intervention.28 A moderate relationship (Pearson’s r = 0.51), between 20 m sprint performance and eccentric strength of knee flexors, was also found.28 Nordic hamstring exercise beneficially affected especially individuals with greater body mass.28 Well-trained individuals’ increases, in eccentric strength of knee flexors, were less consistent compared to recreationally active individuals, although the effect sizes were similar.28 In the case of well-trained team sport athletes, body mass explained more than 90% of the variance in the effect size of eccentric strength of knee flexors.28 The incidence and subsequent recurrence of hamstring strains were reduced by following Nordic hamstring exercise protocols in combination with stretching or isokinetic eccentric, concentric, or combined eccentric and concentric protocol, but there was no reduction in the severity of the injuries after following eccentric exercise protocols, except in isokinetic eccentric intervention, within 1 year after intervention protocol ended.43 The combined effects of eccentric training and other interventions are not completely identified, especially in terms of the severity of hamstring strains.43
Reviews concerning older adult population
Both studies were focused on healthy participants or participants with the absence of any pathology that could interfere with the training effects of over 65 years old.21,55 Kulkarni et al.21 focused on the effects of EEI (including maximal eccentric contraction training, flywheel resistance exercise training, concentric-eccentric exercise, and eccentric resistance training without equipment) in comparison to specific concentric and other exercise interventions. It was found that eccentric-focused exercises elicited significant improvements in balance, mobility, and endurance in the healthy older adults’ population, but significant differences between eccentric and concentric interventions were just barely observed.21 The reduction in the incidence of falls was lower in response to eccentric exercise than to concentric exercise.21 We can observe the beneficial effects of eccentric exercise after a 6-12 week-long duration of the intervention.21 A large effect size for the eccentric focused training was appraised in the pre-training versus post-training comparison for muscle strength, while at the conventional strength group, 2 included studies in systematic review had a moderate effect size.55 It was also reported that different morphological adaptations were seen after the eccentric exercise-focused group and conventional groups (executing exercises that contained concentric and eccentric actions); specifically, a greater increase of cross-sectional area and addition of sarcomeres in parallel and series was observed in the eccentric training.55
Reviews concerning other populations
Muscle architecture
EEI is often used as a great protocol to improve muscle architecture (cross-sectional area, fascicle length, pennation angle, etc.). Because of great forces, the eccentric contraction provides greater exercise-induced muscle damage, which increases the production of muscle fiber proteins, and therefore, greatly increases muscle hypertrophy compared to concentric36 and isometric contractions.32 Schoenfeld et al.41 found out that eccentric-only muscle actions caused greater increases in the cross-sectional area compared to concentric-only actions, but the results were not statistically significant.41 On the other hand, Petré et al.38 and Emirzeoğlu et al.33 pointed that eccentric training significantly increased the cross-sectional area of the muscle and muscle volume/mass, while Petré et al.38 also pointed that they observed moderate effect sizes during 5-8 weeks of flywheel training for 2-3 times per week. The eccentric exercise was found to greatly increase distal muscle size of especially fast-twitch muscle fibers compared to concentric exercise, while concentric exercise caused greater mid-muscle hypertrophy compared to eccentric exercise.32,41 On the other hand, the cross-sectional area largely increased with higher velocities of eccentric training (e.g. heavy eccentric loads).32 Douglas et al.32 pointed out that particularly heavier eccentric training caused greater muscle hypertrophy and increased cross-sectional area, while Roig et al.23 emphasized that eccentric resistance training performed outstanding improvements in eccentric strength, muscle girth, and cross-sectional area compared to concentric training. Eccentric exercise in general greatly increased fascicle length too,32,33,37 but Emirzeoğlu et al.33 added that the increase was found independent of duration and frequency of intervention, and a number of repetitions. The other authors53 who were focused particularly on the effects of Nordic hamstring exercise agreed with Douglas et al.32 and Emirzeoğlu et al.,33 but added that they found out that in the case of implementing Nordic hamstring exercise in the training session, it provided great results (increased hamstring fascicle length) only when the exercise was performed before the training session (in warm-up). It was also found that executing of Nordic hamstring exercise significantly increased m. biceps femoris long head fascicle length (even in low-volume programs) and eccentric strength of knee flexors.45 On the other hand, increase of hamstring muscle thickness, and decrease of hamstring muscle pennation angle were observed only when the Nordic hamstring exercise was administered after field-training sessions.53 Eccentric exercise also effectively enhanced gains and lean mass compared to concentric exercise, but age has been found to have some negative effects on increasing muscle mass training processes.36
A large increase in lower limb muscle stiffness was also observed after executing eccentric training combined with fast concentric exercises intervention 3 times per week, for 10 weeks, especially when comparing with results, obtained after executing a combination of eccentric exercise with slow concentric exercises intervention (with the same amount of training sessions).32
Muscle performance and moving efficiency
Flywheel squat training moderately improved isometric strength (by 8 %) mobility, and balance (both by 13 %), largely improved the power of knee extensors (by 63 %), velocity (by 48 %), and very largely improved tendon stiffness (by 136 %), in the healthy older adults population over 6-12 weeks of flywheel squat training protocol.39
Authors noted greater increase in eccentric strength compared to concentric strength 32,36 and to a greater change of direction speed performance after receiving eccentric overload training protocol.54 It was also found that, before and after field training, eccentric strength training more effectively increased eccentric hamstring strength, and reduced hamstring strain injuries than concentric strength training.53 We have evidence that strength gains, were tended to be more velocity-dependent.40 Muscle contraction velocity, muscle and tendon strength, and muscle power (rate of force development) increased greater by fast compared to slow eccentric training.32 Fast eccentric training also improved stretch-shortening cycle performance to a greater extent than slow eccentric training.32 It was also found that flywheel overload training significantly increased hypertrophy in muscle cross-sectional area and muscle volume/mass with moderate effect sizes; power, and both, horizontal and vertical displacements (decreased times) with large effect size; and maximal strength with a very large effect size when comparing pre- to post-test results.38
Limitations
Some limitations of this review must be acknowledged. First, we included only systematic reviews and/or meta-analysis which were found in the aforementioned databases, while we did not search any other electronic or non-electronic databases.
Second, 11 reviews were not limited to studies that included a control group to compare outcomes obtained between the experimental group (which implemented eccentric exercise) and control group(/-s) (which implemented other types of therapy, other exercise interventions, or no intervention at all).
Third, if the included systematic review did not conduct a meta-analysis, we had to overlook 2 out of 7 critical domains (item 11 and item 15) when assessing the methodological quality of the included studies, which happened in the assessment of 17 out of 35 studies.
Fourth, among those 18 studies that have conducted meta-analysis, only 6 carried out an adequate investigation and discussion of the likelihood and magnitude of the impact of publication bias.
Fifth, because of the lack of similar research with the same outcome measures, due to different characteristics of the population (gender, age, sports activity, or different pathology, etc.) and different exercises or exercise protocols, we could not carry out the meta-analysis to find out the heterogeneity of the results, with which we would conclusively confirm the obtained data.
Sixth, 11 reviews did not assess the risk of bias for included studies, so the evidence of these reviews is of questionable quality.
Conclusion
It was found that eccentric exercise is being increasingly used within exercise protocols especially for injury rehabilitation and prevention, as well as improvement of athletic performance. Eccentric exercise programs can elicit large improvements in muscle performance, functional performance, muscle architecture, and reduce pain and the risk of injuries compared to other exercise modalities or therapy intervention programs. On the other hand, an implementation of an eccentric exercise can cause delayed onset muscular soreness or other kinds of muscle damage. By cautiously determining the eccentric exercise protocol we can limit delayed onset muscular soreness and also maximize training compliance and exercise tolerance. The quality of the evidence on the field is mixed, with the review quality rating scores ranging from critically low to high.
Supplementary Material
Acknowledgments
The authors thank the patients who volunteered for the study.
List of acronyms
- EEI
eccentric exercise interventions
- VO2
oxygen consumption
Funding Statement
Funding: We want to acknowledge the support of the European Regional Development Fund and Physiko- and Rheumatherapie Institute through the Centre of Active Ageing project in the Interreg Slovakia–Austria cross-border cooperation program (partners: Faculty for Physical Education and Sports, Comenius University in Bratislava: Institute for Physical Medicine and Rehabilitation, Physiko- and Rheumatherapie GmbH). NŠ and ŽK acknowledge the University of Primorska's suppirt through internal research program KINSPO (2990-1-2/2021). The funders had no role in conceptualization of the study, analysis of the data, manuscript preparation or any other activities leading to the creation of this article. There was no additional external funding received for this study.
Contributor Information
Luka Križaj, Email: 97210402@student.upr.si.
Žiga Kozinc, Email: ziga.kozinc@fvz.upr.si..
Stefan Löfler, Email: stefan.loefler@rehabilitation.lbg.ac.at.
References
- 1.Jeffrey L. Young, Joel M. The Physiologic Basis of Sports Rehabilitation. Physical Medicine and Rehabilitation Clinics of North America, Volume 5, Issue 1, 1994, 9-36. doi.org/10.1016/S1047-9651(18)30536-9. [Google Scholar]
- 2.Lindstedt SL, LaStayo PC, Reich TE. When active muscles lengthen: properties and consequences of eccentric contractions. News Physiol Sci. 2001. Dec;16:256-61. doi: 10.1152/physiologyonline.2001.16.6.256. [DOI] [PubMed] [Google Scholar]
- 3.Cowell JF, Cronin J, Brughelli M. Eccentric Muscle Actions and How the Strength and Conditioning Specialist Might Use Them for a Variety of Purposes. Strength Cond J. 2012;34(3):33–48. doi: 10.1519/SSC.0b013e 318253f578. [Google Scholar]
- 4.Perrey S, Betik A, Candau R, Rouillon JD, Hughson RL. Comparison of oxygen uptake kinetics during concentric and eccentric cycle exercise. J Appl Physiol (1985). 2001. Nov;91(5):2135-42. doi: 10.1152/jappl.2001.91.5.2135. [DOI] [PubMed] [Google Scholar]
- 5.Bigland-Ritchie B, Woods JJ. Integrated electromyogram and oxygen uptake during positive and negative work. J Physiol. 1976. Sep;260(2):267-77. doi: 10.1113/jphysiol.1976. sp011515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ellis R, Shields N, Lim K, Dodd KJ. Eccentric exercise in adults with cardiorespiratory disease: a systematic review. Clin Rehabil. 2015. Dec;29(12):1178-97. doi: 10.1177/02692155155 74783. Epub 2015 Mar 10. [DOI] [PubMed] [Google Scholar]
- 7.Clos P, Laroche D, Stapley PJ, Lepers R. Neuromuscular and Perceptual Responses to Sub-Maximal Eccentric Cycling. Front Physiol. 2019. Mar 28;10:354. doi: 10.3389/fphys.2019.00354. Erratum in: Front Physiol. 2020 Aug 12;11:934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lovering RM, Brooks SV. Eccentric exercise in aging and diseased skeletal muscle: good or bad? J Appl Physiol (1985). 2014. Jun 1;116(11):1439-45. doi: 10.1152/japplphysiol.00174.2013. Epub 2013 Mar 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Julian V, Thivel D, Costes F, Touron J, Boirie Y, Pereira B, Perrault H, Duclos M, Richard R. Eccentric Training Improves Body Composition by Inducing Mechanical and Metabolic Adaptations: A Promising Approach for Overweight and Obese Individuals. Front Physiol. 2018. Aug 7;9:1013. doi: 10.3389/fphys.2018. 01013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Garrett WE Jr. Muscle strain injuries. Am J Sports Med. 1996;24(6 Suppl):S2-8. [PubMed] [Google Scholar]
- 11.Malliaropoulos N, Mendiguchia J, Pehlivanidis H, Papadopoulou S, Valle X, Malliaras P, Maffulli N. Hamstring exercises for track and field athletes: injury and exercise biomechanics, and possible implications for exercise selection and primary prevention. Br J Sports Med. 2012. Sep;46(12):846-51. doi: 10.1136/bjsports-2011-09 0474. Epub 2012 Jun 9. [DOI] [PubMed] [Google Scholar]
- 12.Serner A, Mosler AB, Tol JL, Bahr R, Weir A. Mechanisms of acute adductor longus injuries in male football players: a systematic visual video analysis. Br J Sports Med. 2019. Feb;53(3):158-164. doi: 10.1136/bjsports-2018-099246. Epub 2018 Jul 13. [DOI] [PubMed] [Google Scholar]
- 13.Kary JM. Diagnosis and management of quadriceps strains and contusions. Curr Rev Musculoskelet Med. 2010. Jul 30;3(1-4):26-31. doi: 10.1007/s12178-010-9064-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mendiguchia J, Alentorn-Geli E, Idoate F, Myer GD. Rectus femoris muscle injuries in football: a clinically relevant review of mechanisms of injury, risk factors and preventive strategies. Br J Sports Med. 2013. Apr;47(6):359-66. doi: 10.1136/ bjsports-2012-091250. Epub 2012 Aug 3. [DOI] [PubMed] [Google Scholar]
- 15.Brockett CL, Morgan DL, Proske U. Predicting hamstring strain injury in elite athletes. Med Sci Sports Exerc. 2004. Mar;36(3):379-87. doi: 10.1249/01.mss.0000117165.75832.05. [DOI] [PubMed] [Google Scholar]
- 16.Vogt M, Hoppeler HH. Eccentric exercise: mechanisms and effects when used as training regime or training adjunct. J Appl Physiol (1985). 2014. Jun 1;116(11):1446-54. doi: 10.1152/ japplphysiol.00146.2013. Epub 2014 Feb 6. [DOI] [PubMed] [Google Scholar]
- 17.Goode AP, Reiman MP, Harris L, DeLisa L, Kauffman A, Beltramo D, Poole C, Ledbetter L, Taylor AB. Eccentric training for prevention of hamstring injuries may depend on intervention compliance: a systematic review and meta-analysis. Br J Sports Med. 2015. Mar;49(6):349-56. doi:10.1136/bjsports-2014-093466. Epub 2014 Sep 16. [DOI] [PubMed] [Google Scholar]
- 18.LaStayo PC, Woolf JM, Lewek MD, Snyder-Mackler L, Reich T, Lindstedt SL. Eccentric muscle contractions: their contribution to injury, prevention, rehabilitation, and sport. J Orthop Sports Phys Ther. 2003. Oct;33(10):557-71. doi: 10.2519/jospt.2003.33.10.557. [DOI] [PubMed] [Google Scholar]
- 19.Hoppeler H. Moderate Load Eccentric Exercise; A Distinct Novel Training Modality. Front Physiol. 2016. Nov 16;7:483. doi: 10.3389/fphys.2016.00483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.LaStayo P, Marcus R, Dibble L, Wong B, Pepper G. Eccentric versus traditional resistance exercise for older adult fallers in the community: a randomized trial within a multi-component fall reduction program. BMC Geriatr. 2017. Jul 17;17(1):149. doi: 10.1186/s12877-017-0539-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kulkarni D, Gregory S, Evans M. Effectiveness of eccentric-biased exercise interventions in reducing the incidence of falls and improving functional performance in older adults: a systematic review. Eur Geriatr Med. 2022. Apr;13(2):367-380. doi: 10.1007/s41999-021-00571-8. Epub 2021 Oct 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Murphy MC, Travers MJ, Chivers P, Debenham JR, Docking SI, Rio EK, Gibson W. Efficacy of heavy eccentric calf training for treating mid-portion Achilles tendinopathy: a systematic review and meta-analysis. Br J Sports Med. 2019. Sep;53(17):1070-1077. doi: 10.1136/bjsports-2018-099934. Epub 2019 Jan 13. [DOI] [PubMed] [Google Scholar]
- 23.Roig M, O'Brien K, Kirk G, Murray R, McKinnon P, Shadgan B, Reid WD. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. Br J Sports Med. 2009. Aug;43(8):556-68. doi: 10.1136/bjsm.2008. 051417. Epub 2008 Nov 3. [DOI] [PubMed] [Google Scholar]
- 24.Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. 2014. Nov 21;14:579. doi: 10.1186/s12913-014-0579-0.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthc. 2015. Sep;13(3):132-40. doi: 10.1097/XEB.0000000000000055. [DOI] [PubMed] [Google Scholar]
- 26.Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, Henry DA. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017. Sep 21;358:j4008. doi: 10.1136/bmj.j4008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Allen WJC, De Keijzer KL, Raya-González J, Castillo D, Coratella G, Beato M. Chronic effects of flywheel training on physical capacities in soccer players: a systematic review. Res Sports Med. 2021. Jul 27:1-21. doi: 10.1080/15438627.2021.1958813. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 28.Bautista IJ, Vicente-Mampel J, Baraja-Vegas L, Segarra V, Martín F, Van Hooren B. The effects of the Nordic hamstring exercise on sprint performance and eccentric knee flexor strength: A systematic review and meta-analysis of intervention studies among team sport players. J Sci Med Sport. 2021. Sep;24(9):931-938. doi: 10.1016/j.jsams.2021.03.009. Epub 2021 Mar 22. [DOI] [PubMed] [Google Scholar]
- 29.Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin Rehabil. 2014. Jan;28(1):3-19. doi: 10.1177/0269215513 491974. Epub 2013 Jul 23. [DOI] [PubMed] [Google Scholar]
- 30.Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin Rehabil. 2014. Jan;28(1):3-19. doi: 10.1177/0269215513491974. Epub 2013 Jul 23. [DOI] [PubMed] [Google Scholar]
- 31.Cuthbert M, Ripley N, McMahon JJ, Evans M, Haff GG, Comfort P. The Effect of Nordic Hamstring Exercise Intervention Volume on Eccentric Strength and Muscle Architecture Adaptations: A Systematic Review and Meta-analyses. Sports Med. 2020. Jan;50(1):83-99. doi: 10.1007/s40279-019-01178-7. Erratum in: Sports Med. 2019 Nov 7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Douglas J, Pearson S, Ross A, McGuigan M. Chronic Adaptations to Eccentric Training: A Systematic Review. Sports Med. 2017. May;47(5):917-941. doi: 10.1007/s40279-016-0628-4. [DOI] [PubMed] [Google Scholar]
- 33.Emirzeoğlu M, Fırat T, Ülger Ö. The effects of eccentric training on hamstring muscle architecture: A systematic review. Language (Baltim). 2021;97(2):141–153. [Google Scholar]
- 34.Lim HY, Wong SH. Effects of isometric, eccentric, or heavy slow resistance exercises on pain and function in individuals with patellar tendinopathy: A systematic review. Physiother Res Int. 2018. Oct;23(4):e1721. doi: 10.1002/pri.1721. Epub 2018 Jul 4. [DOI] [PubMed] [Google Scholar]
- 35.Lim HY, Wong SH. Effects of isometric, eccentric, or heavy slow resistance exercises on pain and function in individuals with patellar tendinopathy: A systematic review. Physiother Res Int. 2018. Oct;23(4):e1721. doi: 10.1002/pri.1721. Epub 2018 Jul 4. [DOI] [PubMed] [Google Scholar]
- 36.Nuñez Sanchez FJ, Sáez de Villarreal E. Does Flywheel Paradigm Training Improve Muscle Volume and Force? A Meta-Analysis. J Strength Cond Res. 2017. Nov;31(11):3177-3186. doi: 10.1519/JSC.0000000000002095. [DOI] [PubMed] [Google Scholar]
- 37.O'Sullivan K, McAuliffe S, Deburca N. The effects of eccentric training on lower limb flexibility: a systematic review. Br J Sports Med. 2012. Sep;46(12):838-45. doi: 10.1136/bjsports-2011-090835. [DOI] [PubMed] [Google Scholar]
- 38.Petré H, Wernstål F, Mattsson CM. Effects of Flywheel Training on Strength-Related Variables: a Meta-analysis. Sports Med Open. 2018. Dec 13;4(1):55. doi: 10.1186/s40798-018-0169-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Raya-González J, de Keijzer KL, Bishop C, Beato M. Effects of flywheel training on strength-related variables in female populations. A systematic review. Res Sports Med. 2022. Jul-Aug;30(4):353-370. doi: 10.1080/15438627.2020.1870977. Epub 2021 Jan 5. [DOI] [PubMed] [Google Scholar]
- 40.Roig M, Shadgan B, Reid WD. Eccentric exercise in patients with chronic health conditions: a systematic review. Physiother Can. 2008. Spring;60(2):146-60. doi: 10.3138/physio.60.2. 146. Epub 2008 Oct 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Schoenfeld BJ, Ogborn DI, Vigotsky AD, Franchi MV, Krieger JW. Hypertrophic Effects of Concentric vs. Eccentric Muscle Actions: A Systematic Review and Meta-analysis. J Strength Cond Res. 2017. Sep;31(9):2599-2608. doi: 10.1519/JSC.0000000000001983. [DOI] [PubMed] [Google Scholar]
- 42.Al Attar WSA, Soomro N, Sinclair PJ, Pappas E, Sanders RH. Effect of Injury Prevention Programs that Include the Nordic Hamstring Exercise on Hamstring Injury Rates in Soccer Players: A Systematic Review and Meta-Analysis. Sports Med. 2017. May;47(5):907-916. doi: 10.1007/s 40279-016-0638-2. [DOI] [PubMed] [Google Scholar]
- 43.K Grant A, Beers A, Moizumi T. A systematic review of the effectiveness of eccentric strength training in the prevention of hamstring muscle strains in otherwise healthy individuals. N Am J Sports Phys Ther. 2008. May;3(2):67-81. [PMC free article] [PubMed] [Google Scholar]
- 44.Karagiannis C, Savva C, Mamais I, Efstathiou M, Monticone M, Xanthos T. Eccentric exercise in ischemic cardiac patients and functional capacity: A systematic review and meta-analysis of randomized controlled trials. Ann Phys Rehabil Med. 2017. Jan;60(1):58-64. doi: 10.1016/j.rehab.2016.10.007. Epub 2016 Dec 14. [DOI] [PubMed] [Google Scholar]
- 45.Medeiros DM, Marchiori C, Baroni BM. Effect of Nordic Hamstring Exercise Training on Knee Flexors Eccentric Strength and Fascicle Length: A Systematic Review and Meta-Analysis. J Sport Rehabil. 2020. Oct 12;30(3):482-491. doi: 10.1123/jsr.2019-0388. [DOI] [PubMed] [Google Scholar]
- 46.Raya-González J, Prat-Luri A, López-Valenciano A, Sabido R, Hernández-Davó JL. Effects of Flywheel Resistance Training on Sport Actions. A Systematic Review and Meta-Analysis. J Hum Kinet. 2021. Jan 30;77:191-204. doi: 10.2478/ hukin-2021-0020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Larsson R, Bernhardsson S, Nordeman L. Effects of eccentric exercise in patients with subacromial impingement syndrome: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019. Oct 14;20(1):446. doi: 10.1186/s12891-019-2796-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ortega-Castillo M, Medina-Porqueres I. Effectiveness of the eccentric exercise therapy in physically active adults with symptomatic shoulder impingement or lateral epicondylar tendinopathy: A systematic review. J Sci Med Sport. 2016. Jun;19(6):438-53. doi: 10.1016/j.jsams.2015.06. 007. Epub 2015 Jun 15. [DOI] [PubMed] [Google Scholar]
- 49.Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epicondylosis - A systematic review. J Hand Ther. United States: Hanley & Belfus; 2012;25(1):5–26. doi:10.1016/j.jht.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 50.Wasielewski NJ, Kotsko KM. Does eccentric exercise reduce pain and improve strength in physically active adults with symptomatic lower extremity tendinosis? A systematic review. J Athl Train. 2007. Jul-Sep;42(3):409-21. [PMC free article] [PubMed] [Google Scholar]
- 51.Yoon SY, Kim YW, Shin IS, Kang S, Moon HI, Lee SC. The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis. J Clin Med. 2021. Sep 1;10(17):3968. doi: 10.3390/jcm10173968.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dominguez-Romero JG, Jiménez-Rejano JJ, Ridao-Fernández C, Chamorro-Moriana G. Exercise-Based Muscle Development Programmes and Their Effectiveness in the Functional Recovery of Rotator Cuff Tendinopathy: A Systematic Review. Diagnostics (Basel). 2021. Mar 16;11(3):529. doi: 10.3390/diagnostics11030529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gérard R, Gojon L, Decleve P, Van Cant J. The effects of eccentric training on biceps femoris architecture and strength: A systematic review with meta-analysis. J Athl Train. 2020;55(5):501–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Liu R, Liu J, Clarke CV, An R. Effect of eccentric overload training on change of direction speed performance: A systematic review and meta-analysis. J Sports Sci. 2020. Nov;38(22):2579-2587. doi: 10.1080/02640414.2020.1794247. Epub 2020 Jul 17. [DOI] [PubMed] [Google Scholar]
- 55.Molinari T, Steffens T, Roncada C, Rodrigues R, Dias CP. Effects of Eccentric-Focused Versus Conventional Training on Lower Limb Muscular Strength in Older People: A Systematic Review With Meta-Analysis. J Aging Phys Act. 2019. Dec 1;27(4):823-830. doi: 10.1123/japa.2018-0294. [DOI] [PubMed] [Google Scholar]
- 56.Woodley BL, Newsham-West RJ, Baxter GD. Chronic tendinopathy: effectiveness of eccentric exercise. Br J Sports Med. 2007. Apr;41(4):188-98; discussion 199. doi: 10.1136/bjsm.2006.029769. Epub 2006 Oct 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.