

Abstract
Background
Racial and socioeconomic disparities have been associated with complications and poorer patient-reported outcomes after THA and TKA, but little is known regarding the variation of postacute care resource utilization based on socioeconomic difference in the communities in which patients reside. Hip and knee arthroplasty are among the most common elective orthopaedic procedures. Therefore, understanding social factors provides insight into patients at risk for readmission and the way in which these patients use other postoperative resources. This knowledge can help surgeons better understand which patients are at risk for complications or preventable readmissions and how to anticipate when additional surveillance or intervention might reduce this risk.
Questions/purposes
(1) Do patients from communities with a higher distress level experience higher rates of readmission after THA and TKA? (2) Do patients from distressed communities have increased postoperative resource utilization?
Methods
Demographics, ZIP code of residence, and Charlson comorbidity index (CCI) were recorded for each patient undergoing TKA or THA between 2016 and 2019 at two high-volume hospitals. Patients were classified according to the Distressed Communities Index (DCI) score of their ZIP code of residence. The DCI combines seven metrics of socioeconomic well-being (high school graduation, poverty rate, unemployment, housing vacancy, household income, change in employment, and change in establishment) to create a single score. ZIP codes are then classified by scores into five categories based on national quintiles (prosperous, comfortable, mid-tier, at-risk, and distressed). The DCI was chosen because it provides a single composite measure of multiple important socioeconomic factors. Multivariate analysis with logistic, negative binomial regression, or Poisson was used to investigate the association of DCI category with postoperative resource utilization while controlling forage, gender, BMI, and comorbidities. The primary outcome was 90-day readmissions. Secondary outcomes included postoperative medication prescriptions from the orthopaedic team, patient telephone calls to the surgeon’s office, physical therapy sessions attended, follow-up office visits, and emergency department visits. A total of 5077 patients who underwent TKA (mean age 66 ± 9 years, 59% [2983 of 5077] are women, and 69% [3519 of 5077] are White), and 5299 who underwent THA (mean age 63 ± 11 years, 50% [2654 of 5299] are women, and 74% [3903 of 5299] are White) were included.
Results
When adjusting for age, gender, race and CCI, readmission risk was higher in distressed communities compared with prosperous communities for patients undergoing TKA (odds ratio 1.6 [95% confidence interval 1.1 to 2.3]; p = 0.02) but not for THA. For secondary outcomes after TKA, at-risk communities had more postoperative prescriptions compared with prosperous communities, but no other differences were found. After THA, no major differences were found in the likelihood to utilize postoperative resources based on DCI category. Race was not associated with readmissions or resource utilization.
Conclusion
We found that socioeconomic distress was associated with readmission after TKA, but, after controlling for relevant confounding variables, race had no association. Patients from these communities do not demonstrate an increased or decreased use of other resources after post-TKA discharge. Increased awareness of these disparities may allow for closer monitoring and improved patient education and communication, with the goal of reducing the frequency of complications and preventable readmissions.
Level of Evidence
Level III, therapeutic study.
Introduction
There is a well-known association between socioeconomic deprivation and poor patient health outcomes [2, 12, 27, 30]. These disparities may result from upstream factors such as poverty, education level, and neighborhood safety, and downstream factors such as harmful coping behaviors or distress related to physical and mental health [5, 24]. The association of socioeconomic disparities on patient outcomes has received increased attention in orthopaedics [23]. Goodman et al. [9] found that White and Black patients had similar pain and function scores after TKA except in communities with high levels of poverty. Another study by Zhang et al. [32] found that patients who were Black, Hispanic, Asian, and Native American were less likely to undergo total joint arthroplasty (TJA) at hospitals performing a high volume of procedures. Lower education level and lack of support system has also been associated with worse pain scores after TKA [17]. However, a recent study by Chisari et al. [7] found neither poverty, education level, unemployment, nor vehicle possession to be independently associated with readmission or worse functional outcomes. Although none of these factors alone were associated with readmission, we are unaware of any studies that have effectively investigated them in combination.
Patients from minority groups, specifically Black and Hispanic patients, have been shown to be at an increased risk of medical and surgical complications after TJA in a large national sample [8]. Amen et al. [1] examined more than 8 million TJAs in the National Inpatient Survey database from 2006 to 2015 and found continuing or widening disparities between White and Black patients with regard to utilization, perioperative care, and discharge to rehabilitation facilities. Black patients had lower TJA use, longer lengths of stay, and increased perioperative complications—including mortality—than White patients. Patients with lower incomes and government-subsidized insurance also have less access to high-volume surgical centers and surgeons, which in turn often leads to higher costs of care [16]. Findings from these studies suggest a multifaceted etiology, as race alone is only one part of a much larger picture, and thus should not be interpreted in isolation. Factors such as race, income, and insurance type are often cited as factors associated with adverse outcomes; however, the true risk is likely due to a much more complex interaction of multiple socioeconomic determinants [14, 15].
Patients with decreased social resources and those without a strong social support system are the most impacted. Non-White patients and patients with lower incomes are also more likely to be discharged to a rehabilitation facility than to home after TJA [1, 22, 28, 29]. As these patients have increased postoperative needs, we theorized that they would have increased utilization of other resources, including physical therapy, phone calls, and office visits. Understanding the patterns of resource use by patients from underserved areas undergoing TJA can improve provider relationships with patients while working to avoid costly readmissions and complications. In addition, it can allow greater focus on adequate postoperative surveillance while meeting the needs of patients to avoid readmission for preventable reasons. Although previous work has looked at individual socioeconomic factors [7], the purpose of this study was to investigate postoperative utilization using a composite score combining numerous factors that contribute to socioeconomic distress. We stratified patients by the Distressed Communities Index (DCI) and adjusted for demographics and the comorbidities index.
We therefore asked: (1) Do patients from communities with a higher distress level experience higher rates of readmission after THA and TKA? (2) Do patients from distressed communities have increased postoperative resource utilization?
Patients and Methods
Study Design and Setting
This was a retrospective comparative study of patient undergoing surgery at one institution. Twenty-one high-volume arthroplasty surgeons performed the procedures at either an urban tertiary care hospital or a suburban orthopaedic specialty hospital within the same practice.
Participants
All patients who underwent primary TKA or THA between January 1, 2016, and December 31, 2019, at two high-volume surgical locations that were part of a tertiary healthcare network in a large metropolitan area were identified. We chose 2016 as the start point of our study because it was when our institution began using nurse navigators to ensure accurate follow-up within 90 days of surgery. We chose these two centers because both used nurse navigators.
Data Collection
Demographic data consisting of age, gender, self-reported race, BMI, and ZIP code of residence were recorded for each patient at the time of surgery. As most patients self-reported as White or Black, we decided to combine the race variable into White, Black, or other. Unreported or unknown race were kept as separate categories. Self-reporting of race by patients, although not without limitations, is the standard practice within our institution and was used for analysis. Hospitals collected information on patient comorbidities using the American Society of Anesthesiologists (ASA) physical status classification and the Charlson comorbidity index (CCI).
Distress Score
The DCI (Economic Innovation Group, 2018, https://eig.org/dci) was referenced to assign a distress score to all patients based on their ZIP code of residence at the time of surgery. All ZIP codes in the United States with at least 500 residents are included in the DCI. The DCI assigns each ZIP code an aggregate score from 0 (least distressed) to 100 (most distressed) based on seven metrics of economic well-being: percentage of the population with a high school diploma, poverty rate, unemployment rate, housing vacancy rate, median household income, change in employment, and change in establishments. We chose the DCI because it provides a single combined index that incorporates numerous factors that describe socioeconomic well-being, and it was available for most patients in our study population. Using a combined score helps to better understand the combined influences of a variety of factors rather than focusing on a single issue such as income or unemployment rate. Higher DCI scores have been associated with poor outcomes in multiple medical specialties, including higher mortality after coronary artery bypass grafting [6], lower long-term survival after bariatric surgery [19], and worse functional outcomes after mechanical thrombectomy for ischemic stroke [25]. The DCI divides scores into quintiles based on the national distribution of scores, defined as prosperous (first quintile, 0 to 20), comfortable (second quintile, 21 to 40), mid-tier (third quintile, 41 to 60), at risk (fourth quintile, 61 to 80), and distressed (fifth quintile, 81 to 100). DCI scores were available for 99% of patients included in the study. The remaining patients could not be matched to a score and thus were excluded from further analysis. We used the DCI categories defined based on national quintiles in our analysis.
Patients’ Descriptive Data
TKA
During the study, 5120 patients underwent TKA, of whom 99% (5077) had a DCI score assigned to their ZIP code of residence (Fig. 1). The mean age was 66 ± 9 years, with women encompassing 59% (2983 of 5077) of patients. White patients constituted 69% (3519 of 5077) of our population, and 14% (700 of 5077) of patients were Black. Seventeen percent (858 of 5077) reported other race, unknown race, or refused to report (Supplementary Table 1; http://links.lww.com/CORR/A771).
Fig. 1.
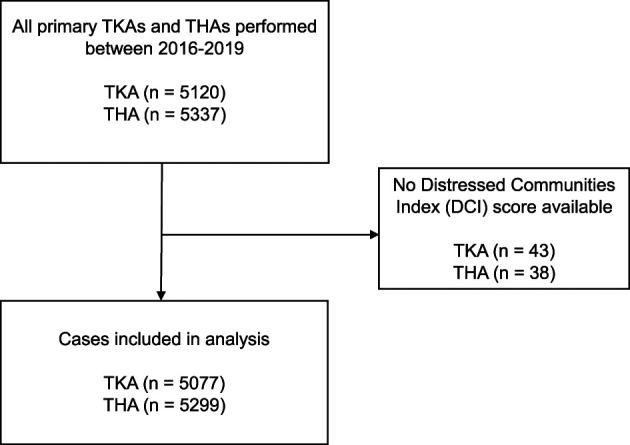
STROBE table outlining patient inclusion and exclusion.
THA
In this study, 5337 patients underwent THA, of whom 99% (5299) had a DCI score assigned to their ZIP code of residence (Fig. 1). The mean age was 63 ± 11 years, with women comprising 50% (2645 of 5299) of patients. White patients represented 74% of our population, and 10% were Black. Sixteen percent reported other race, unknown race, or refused to report (Supplementary Table 2; http://links.lww.com/CORR/A772).
Primary and Secondary Study Outcomes
The primary outcome was 90-day readmissions, which were tracked longitudinally via the nurse navigator program at our institution. We used multivariate logistic regression to compare the risk of readmission for DCI categories using prosperous communities as a reference. We adjusted for age, gender, BMI, self-reported race, and CCI.
We then queried our electronic medical record system to identify secondary outcomes, including postoperative medication prescriptions from a member of the joint arthroplasty team, physical therapy sessions attended, telephone calls between patients and their surgeon’s office, postoperative office visits, and visits to the emergency department after discharge. Separate regressions were conducted for each secondary outcome using prosperous communities as a reference and adjusting for age, gender, BMI, race, and CCI.
Ethical Approval
This study was reviewed by Thomas Jefferson University and was determined to be exempt from institutional review board approval (IRB number #21E.567).
Statistical Analysis
We used logistic and Poisson regression analyses to investigate the associations of individual DCI categories on the primary and secondary outcomes (prescriptions, physical therapy sessions, telephone calls, office visits, emergency department visits). Separate multivariate models were created for patients undergoing TKA and THA based on DCI category alone and DCI category adjusted for demographics (age, gender, BMI, and race) and comorbidities (CCI). Prosperous communities, women, and white race were used as reference groups in all models. Odds ratios were calculated with logistic regression for categorical data, and incidence rate ratios (IRR) were calculated with either negative binomial regressions or Poisson regressions for continuous count data, depending on variance. Parametric continuous data was presented as mean ± SD. Nonparametric continuous data was also presented as mean ± SD for easier interpretation. Categorical data is presented as cell count (%). An alpha of 0.05 was considered statistically significant. All statistical analyses were done using R studio (Version 3.6.3).
Results
Do Patients from Communities with a Higher Distress Level Experience Higher Rates of Readmission after THA and TKA?
After adjusting for demographic factors and CCI, patients in communities classified as distressed by the DCI were more likely to be readmitted after TKA compared with patients in communities classified as prosperous (odds ratio 1.6 [95% confidence interval 1.1 to 2.3]; p = 0.02). There was no difference compared with prosperous for communities classified as comfortable, mid-tier, or at risk (Fig. 2). Younger age and higher CCI were also associated with a slightly increased likelihood readmissions in our model (Table 1). Race was not associated with readmission.
Fig. 2.

ORs and 95% CIs for 90-day readmission by DCI category in patients undergoing TKA and THA after adjusting for demographics and CCI. Category 1 (prosperous) was used for reference.
Table 1.
Factors associated with 90-day readmissions after TKA and THA
| TKA | THA | |||
| OR (95% CI) | p value | OR (95% CI) | p value | |
| DCI category | ||||
| Comfortable | 1.1 (0.7-1.6) | 0.70 | 0.9 (0.6-1.4) | 0.63 |
| Mid-tier | 1.2 (0.8-1.8) | 0.34 | 0.8 (0.5-1.3) | 0.36 |
| At risk | 1.3 (0.8-2.1) | 0.31 | 1.5 (0.8-2.5) | 0.19 |
| Distressed | 1.6 (1.1-2.3) | 0.02 | 0.9 (0.5-1.5) | 0.60 |
| Age in years | 0.96 (0.93-0.98) | < 0.001 | 1.0 (1.0-1.0) | 0.50 |
| Men | 0.9 (0.7-1.2) | 0.68 | 0.92 (0.7-1.3) | 0.62 |
| BMI in kg/m2 | 1.0 (0.95-1.0) | 0.10 | 1.04 (1.01-1.08) | 0.01 |
| Race | ||||
| Black | 1.0 (0.7-1.4) | 0.92 | 1.0 (1.0-1.1) | 0.87 |
| Other | 1.0 (0.7-1.4) | 0.86 | 0.9 (0.5-1.4) | 0.57 |
| CCI | 1.4 (1.2-1.6) | < 0.001 | 1.3 (1.2-1.5) | < 0.001 |
Logistic regression for 90-day readmission versus no readmission for patients after TKA and THA; DCI category 1 (prosperous), women, and White race used for reference; ORs for continuous variables indicate change in risk per 1-year increase in age, 1-kg/m2 increase in BMI, and 1-point increase in CCI; DCI = Distressed Communities Index; CCI = Charlson comorbidity index.
After adjusting for demographics and CCI, there were no differences in readmission rates associated with any DCI category after THA. Increasing BMI and higher CCI were associated with slightly higher readmission rates (Table 1). Race was not associated with readmission.
Do Patients from Distressed Communities Have Increased Postoperative Resource Utilization?
TKA
After adjusting for demographics and CCI, patients from communities classified as comfortable, mid-tier, and distressed undergoing TKA had no difference in numbers of prescriptions, telephone calls, physical therapy visits, office visits, and ED visits compared with prosperous communities (Table 2).
Table 2.
Secondary outcomes after TKA
| Prescriptions | Telephone calls | Physical therapy | Office visits | ED visit | ||||||
| IRR (95% CI) | p value | IRR (95% CI) | p value | IRR (95% CI) | p value | IRR (95% CI) | p value | OR (95% CI) | p value | |
| DCI category | ||||||||||
| Comfortable | 0.90 (0.83-0.98) | 0.02 | 1.0 (0.9-1.1) | 0.94 | 1.0 (0.8-1.2) | 0.76 | 1.0 (0.9-1.1) | 0.84 | 0.9 (0.5-1.7) | 0.77 |
| Mid-tier | 1.0 (0.9-1.1) | 0.43 | 0.9 (0.9-1.0) | 0.08 | 1.0 (0.9-1.1) | 0.84 | 1.0 (0.9-1.1) | 0.51 | 0.9 (0.5-1.6) | 0.69 |
| At risk | 1.13 (1.02-1.26) | 0.03 | 1.1 (1.0-1.2) | 0.27 | 0.8 (0.7-1.0) | 0.08 | 1.1 (0.9-1.2) | 0.50 | 0.5 (0.1-1.2) | 0.14 |
| Distressed | 1.0 (0.9-1.1) | 0.63 | 1.0 (0.9-1.1) | 0.86 | 0.9 (0.8-1.1) | 0.26 | 1.0 (0.9-1.1) | 0.98 | 1.4 (0.8-2.5) | 0.24 |
| Age | 0.990 (0.985-0.995) | 0.001 | 0.993 (0.989-0.996) | 0.001 | 1.0 (1.0-1.0) | 0.28 | 1.0 (1.0-1.0) | 0.26 | 1.0 (1.0-1.0) | 0.52 |
| Men | 1.0 (0.9-1.0) | 0.12 | 1.0 (0.9-1.0) | 0.40 | 1.0 (0.9-1.1) | 0.40 | 1.0 (0.9-1.1) | 0.78 | 1.0 (0.7-1.6) | 0.84 |
| BMI | 1.0 (1.0-1.0) | 0.77 | 0.991 (0.986-0.996) | 0.001 | 1.0 (1.0-1.0) | 0.51 | 1.0 (1.0-1.0) | 0.92 | 1.0 (1.0-1.1) | 0.54 |
| Race | ||||||||||
| Black | 1.0 (0.9-1.1) | 0.37 | 0.9 (0.9-1.1) | 0.69 | 0.9 (0.8-1.0) | 0.11 | 1.1 (1.0-1.2) | 0.21 | 0.9 (0.6-1.6) | 0.68 |
| Other | 1.2 (1.1-1.3) | < 0.001 | 1.1 (1.0-1.1) | 0.15 | 1.0 (0.8-1.1) | 0.73 | 1.0 (0.9-1.2) | 0.47 | 0.7 (0.4-1.3) | 0.29 |
| CCI | 1.0 (0.9-1.0) | 0.08 | 1.0 (1.0-1.0) | 0.75 | 0.9 (0.9-1.0) | 0.07 | 1.0 (1.0-1.1) | 0.83 | 1.2 (0.9-1.4) | 0.12 |
Negative binomial regressions was used for the number of postoperative prescriptions, telephone calls, and physical therapy visits in patients after TKA; Poisson regression was used for the number of 90 day postop office visits; logistic regression was used for ED visits; DCI category 1 (prosperous), female, and white race were used for reference; ORs and IRRs for continuous variables indicate change in risk per 1-year increase in age and 1-kg/m2 increase in BMI; DCI = Distressed Communities Index; CCI = Charlson comorbidity index.
Patients from at-risk communities had more prescriptions written by the orthopaedic team (IRR 1.13 [95% CI 1.02 to 1.26]; p = 0.03) compared with prosperous communities after TKA. Telephone calls, physical therapy visits, office visits, and ED visits showed no difference.
THA
Patients from comfortable communities had fewer physical therapy visits (IRR 0.5 [95% CI 0.3 to 0.7]; p < 0.01) and ED visits (OR 0.5 [95% CI 0.3 to 0.9]; p = 0.02) compared with prosperous communities after THA. Prescriptions, telephone calls, and office visits showed no difference (Table 3).
Table 3.
Secondary outcomes after THA
| Prescriptions | Telephone Calls | Physical Therapy | Office Visits | ED Visit | ||||||
| IRR (95% CI) | p value | IRR (95% CI) | p value | IRR (95% CI) | p value | IRR (95% CI) | p value | OR (95% CI) | p value | |
| DCI category | ||||||||||
| Comfortable | 1.0 (0.9-1.1) | 0.65 | 1.0 (0.9-1.0) | 0.19 | 0.5 (0.3-0.7) | < 0.01 | 1.0 (0.9-1.1) | 0.54 | 0.5 (0.3-0.9) | 0.02 |
| Mid-tier | 0.9 (0.8-1.0) | 0.13 | 1.0 (0.9-1.0) | 0.29 | 1.3 (1.0-1.6) | 0.06 | 1.0 (0.9-1.2) | 0.66 | 0.6 (0.3-1.1) | 0.12 |
| At risk | 1.0 (0.9-1.2) | 0.90 | 1.0 (0.9-1.1) | 0.33 | 1.2 (0.8-1.8) | 0.34 | 1.0 (0.8-1.1) | 0.57 | 0.9 (0.4-1.7) | 0.70 |
| Distressed | 1.0 (0.9-1.1) | 0.93 | 1.0 (0.9-1.1) | 0.62 | 1.0 (0.7-1.3) | 0.89 | 1.0 (0.8-1.1) | 0.76 | 0.4 (0.2-1.0) | 0.05 |
| Age | 1.0 (1.0-1.0) | 0.11 | 0.995 (0.991-0.999) | 0.02 | 1.0 (1.0-1.0) | 0.63 | 1.0 (1.0-1.0) | 0.81 | 1.0 (1.0-1.1) | 0.34 |
| Men | 0.9 (0.9-1.0) | 0.05 | 0.93 (0.88-0.97) | 0.002 | 1.0 (0.8-1.3) | 0.73 | 1.0 (0.9-1.1) | 0.34 | 0.9 (0.6-1.3) | 0.56 |
| BMI | 1.0 (1.0-1.0) | 0.53 | 0.992 (0.987-0.997) | 0.001 | 1.0 (1.0-1.0) | 0.97 | 1.0 (1.0-1.0) | 0.28 | 1.0 (1.0-1.1) | 0.63 |
| Race | ||||||||||
| Black | 1.1 (1.0-1.2) | 0.05 | 1.0 (0.9-1.1) | 0.52 | 1.3 (1.0-1.8) | 0.08 | 1.0 (0.9-1.2) | 0.98 | 1.3 (0.6-2.4) | 0.46 |
| Other | 1.0 (0.9-1.1) | 0.42 | 1.0 (0.9-1.0) | 0.11 | 1.0 (0.7-1.3) | 0.76 | 1.0 (0.9-1.1) | 0.90 | 1.1 (0.6-1.9) | 0.76 |
| CCI | 1.0 (1.0-1.1) | 0.50 | 1.03 (1.01-1.06) | 0.01 | 1.1 (0.9-1.2) | 0.29 | 1.0 (1.0-1.1) | 0.88 | 1.0 (0.8-1.2) | 0.99 |
Negative binomial regressions was used for the number of postoperative prescriptions, telephone calls, and physical therapy visits in patients after THA; Poisson regression was used for the number of 90 day postop office visits; logistic regression was used for ED visits; DCI category 1 (prosperous), female, and white race were used for reference; ORs and IRRs for continuous variables indicate change in risk per 1 year increase in age, 1 kg/m2 increase in BMI, and 1 point increase in CCI; DCI = Distressed Communities Index; CCI = Charlson comorbidity index.
Patients from mid-tier, at risk, and distressed communities had no difference in numbers of prescriptions, telephone calls, physical therapy visits, office visits, and ED visits compared with prosperous communities.
Discussion
Socioeconomic status has been shown to be associated with differences in a variety of outcomes in many areas of medicine. Factors such as poverty, insurance status, and race have been associated with utilization, readmission rates and functional outcomes in TKA and THA; however, less is known about the combined associations of contributing upstream factors on postoperative readmission and utilization of other resources after discharge. In this study, we used the composite score of the DCI to examine readmissions, prescriptions, telephone calls, physical therapy visits, office visits, and ED visits after TKA and THA. We found that after TKA, patients from distressed communities were more likely to be readmitted compared with those from prosperous communities, but they did not have increased utilization of any other type of resource. This finding suggests that patients from distressed areas may have increased needs, but they are not receiving a higher level of surveillance or care until ultimately requiring readmission. No major differences were observed based on DCI category after THA. Despite previous studies reporting on the associations of race with readmissions, perioperative complications, and functional outcomes [1, 8, 28, 29], we did not observe race to be associated with higher readmission rates adjusting for age, gender, BMI, comorbidities, and DCI. This indicates that a combination of social factors—much deeper than just race—are associated with readmissions in patients from distressed communities.
Limitations
This study has several limitations. Socioeconomic status was determined at the ZIP code level, with information provided by the DCI. A patient’s socioeconomic status may be either above or below the average within his or her community, leading to variability at the level of each individual. This limitation must be understood in all studies using ZIP code, which provides a generalization of a community that may not reflect individual circumstances. However, when looking at the associations of disparities within communities, this method seemed most appropriate. Other tools also exist besides the DCI for categorizing socioeconomic distress within communities. Studies have used individual factors as predictive variables or a different combination of socioeconomic factors. We felt that the DCI offered a reliable combination of some of the most important factors contributing to economic well-being at the community level in a format that has been used in multiple other arenas.
We recognize that classification of race as White, Black, other, unknown, or unreported is also an oversimplification because true identities are often more complex, representing a combination. We used self-reported reported race, which is the standard practice within our institution, and we felt that this would adequately satisfy the purpose of using race in our analysis, which was to adjust when comparing the DCI categories. Our endpoint of postoperative prescriptions was not specific to certain classes of medications but was limited to those prescribed by the joint replacement team, with the assumption that most medications would be related to surgery (such as pain medications or antibiotics). Further, we only included patients receiving care at two high-volume centers in an urban/suburban area in the analysis; thus, our findings may not be generalizable to more rural or resource-limited settings nationwide. The findings of our study are most generalizable to high-volume arthroplasty practices within metropolitan areas consisting of wide variation in socioeconomic status. Lastly, the overall composition of our cohort was more than 50% White in all DCI categories, which may not represent the population receiving TJA in all practices. However, our institution provides orthopaedic care to a large metropolitan area with substantial economic variation.
Do Patients from Communities with a Higher Distress Level Experience Higher Rates of Readmission after THA and TKA?
After controlling for confounding variables, including age, gender, BMI, race, and comorbidities using CCI, we found that patients who lived in distressed communities (defined by the DCI using education, income, poverty rate, employment, housing vacancy, and economic trends) were more likely to be readmitted to the hospital within 90 days of TKA compared with patients in prosperous communities. This same finding was not observed after THA. Race was not independently associated with readmission in either model. These findings demonstrated that readmission was more closely linked to upstream socioeconomic factors measured in the DCI rather than race. Previous studies have reported higher rates of readmission and adverse perioperative events related to race [10, 11, 13, 21, 26]. Contrary to these studies, we did not identify race as an independent risk factor. As distressed communities had higher proportions of non-White patients, studying race as a covariate in isolation leads to confounding. The contributing factors to socioeconomic distress, as measured in the DCI, are likely much more related to patients from certain communities being at higher risk for complications.
Early identification of rare but important complications after discharge, such as wound infection or thromboembolic disease, may represent an increased challenge in in distressed populations, especially those for whom close follow-up is difficult [18]. Given that patients from distressed communities were found to have a higher prevalence of comorbidities, higher BMI, and greater proportion of women— which previous studies have associated with adverse outcomes including overall complication rates, thromboembolic events, and prosthetic joint infection after TKA—these factors may amplify the socioeconomic distress that drove readmissions within 90 days [3, 4]. However, these factors did not fully explain the differences found in our study. Prior research in arthroplasty has found a greater incidence of 90-day readmission in Black patients [10] and in patients with a higher number of diagnosed comorbidities [20]. In our model, we found that socioeconomic status was associated with readmission after TKA but race was not. Similarly, our results suggest that although higher ASA and CCI scores were found in patients with greater socioeconomic distress, controlling for comorbidities could not fully explain the variance in readmission. A previous study attempted to explain this relationship by exploring the association of poverty, unemployment, high school graduation, and vehicle possession rates independently and found that none were associated with readmission or revision [7]. Our study instead used a single combined index, which revealed that the sum of many factors that contribute to community distress may help explain increased readmissions in this population.
Do Patients from Distressed Communities Have Increased Postoperative Resource Utilization?
After controlling for confounding variables of age, gender, BMI, race, and CCI, we found that patients who lived in distressed communities (defined by the DCI) generally did not use more resources after discharge post-TKA or THA than patients whose communities were defined by greater levels of affluence. Secondary resources included prescriptions from the orthopaedic team, telephone calls to their surgeons’ office, physical therapy visits, office visits, and emergency department visits. Small differences were associated with at-risk communities after TKA and comfortable communities after THA, but no general trends were noted based on DCI category. Race was also not associated with different levels of resource utilization. These findings suggest that patients who are more likely to ultimately require readmission are not using postoperative resources at different levels than any other patients. Patients from distressed communities may have additional needs that are not being met earlier in their postoperative course via telephone calls, office visits, or other less costly and time-intensive points of contact. This suggests a role for closer monitoring and early intervention when necessary in certain patients who may require additional care to minimize adverse outcomes.
Conclusion
This study found that patients from distressed communities, as classified by the DCI composite score, were more likely to be readmitted after TKA, but they do not use postoperative resources (prescriptions, telephone calls, physical therapy, office visits) at a higher rate than patients from prosperous communities. Patients from these socioeconomic backgrounds may be challenged by structural barriers to accessing postoperative clinic-based care and physical therapy [31]. Given that readmissions were more common among patients from distressed communities, we ask: Were there missed opportunities to increase postoperative visits for these patients? We believe that the answer is almost certainly yes. Future studies should explore the potential of video-enabled telemedicine platforms, compared with telephone calls, to improve postoperative management and readmission containment. As we move into a new era of medicine better equipped to care for patients with resources such as telemedicine, this should be viewed as an opportunity to identify patients at risk for adverse outcomes based on socioeconomic factors and potentially intervene at earlier stages, for example patients with concerns about wound healing but who have difficulty with transportation to the office. Telemedicine represents a new tool, but care must be taken to ensure that all patients have the opportunity to use it appropriately because disparities and barriers to use may still exist [31].
Acknowledgments
We thank the Economic Innovation Group for providing data from the Distressed Communities Index for this study.
Footnotes
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
This study was reviewed by Thomas Jefferson University and was determined to be exempt from institutional review board approval (IRB number #21E.567).
This work was performed at the Rothman Orthopaedic Institute, Philadelphia, PA, USA.
The findings expressed in this publication are solely those of the authors and not necessarily those of The Economic Innovation Group.
Contributor Information
Justin A. Magnuson, Email: justin.magnuson@rothmanortho.com.
Sean A. Griffin, Email: griffins2020@health.fau.edu.
Nitya Venkat, Email: nxv035@students.jefferson.edu.
Peter A. Gold, Email: pgold12@gmail.com.
P. Maxwell Courtney, Email: paul.courtney@rothmanortho.com.
References
- 1.Amen TB, Varady NH, Rajaee S, Chen AF. Persistent racial disparities in utilization rates and perioperative metrics in total joint arthroplasty in the U.S.: a comprehensive analysis of trends from 2006 to 2015. J Bone Joint Surg Am. 2020;102:811-820. [DOI] [PubMed] [Google Scholar]
- 2.Anderson JKE, Jain P, Wade AJ, et al. Indicators of potential health-related social needs and the association with perceived health and well-being outcomes among community-dwelling medicare beneficiaries. Qual Life Res. 2020;29:1685-1696. [DOI] [PubMed] [Google Scholar]
- 3.Basques BA, Bell JA, Fillingham YA, Khan JM, Della Valle CJ. Gender differences for hip and knee arthroplasty: complications and healthcare utilization. J Arthroplasty. 2019;34:1593-1597. e1591. [DOI] [PubMed] [Google Scholar]
- 4.Blanco JF, Díaz A, Melchor FR, da Casa C, Pescador D. Risk factors for periprosthetic joint infection after total knee arthroplasty. Arch Orthop Trauma Surg. 2020;140:239-245. [DOI] [PubMed] [Google Scholar]
- 5.Braveman P, Gottlieb L. The social determinants of health: it's time to consider the causes of the causes. Public Health Rep. 2014;129:19-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Charles EJ, Mehaffey JH, Hawkins RB, et al. Socioeconomic distressed communities index predicts risk-adjusted mortality after cardiac surgery. Ann Thorac Surg. 2019;107:1706-1712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chisari E, Yayac M, Sherman M, Kozaily E, Courtney PM. Which socioeconomic factors affect outcomes following total hip and knee arthroplasty? J Arthroplasty. 2021;36:1873-1878. [DOI] [PubMed] [Google Scholar]
- 8.Ezomo OT, Sun D, Gronbeck C, Harrington MA, Halawi MJ. Where do we stand today on racial and ethnic health disparities? An analysis of primary total hip arthroplasty from a 2011–2017 national database. Arthroplast Today. 2020;6:872-876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goodman SM, Mandl LA, Parks ML, et al. Disparities in TKA outcomes: census tract data show interactions between race and poverty. Clin Orthop Relat Res. 2016;474:1986-1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hinman AD, Chan PH, Prentice HA, et al. The association of race/ethnicity and total knee arthroplasty outcomes in a universally insured population. J Arthroplasty. 2020;35:1474-1479. [DOI] [PubMed] [Google Scholar]
- 11.Inneh IA, Clair AJ, Slover JD, Iorio R. Disparities in discharge destination after lower extremity joint arthroplasty: analysis of 7924 patients in an urban setting. J Arthroplasty. 2016;31:2700-2704. [DOI] [PubMed] [Google Scholar]
- 12.Johnson KF, Brookover DL, Borden NS. General health and depression outcomes related to cumulative indicators of unmet social determinant of health needs for college students. J College Stud Psychother. Published online March 1, 2021. DOI: 10.1080/87568225.2021.1881752. [Google Scholar]
- 13.Lavernia CJ, Villa JM. Does race affect outcomes in total joint arthroplasty? Clin Orthop Relat Res. 2015;473:3535-3541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Leopold SS. Editorial: beware of studies claiming that social factors are “independently associated” with biological complications of surgery. Clin Orthop Relat Res. 2019;477:1967-1969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leopold SS, Beadling L, Calabro AM, et al. Editorial: the complexity of reporting race and ethnicity in orthopaedic research. Clin Orthop Relat Res. 2018;476:917-920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Li L, Bokshan SL, Mehta SR, Owens BD. Disparities in cost and access by caseload for arthroscopic rotator cuff repair: an analysis of 18,616 cases. Orthop J Sports Med. 2019;7:2325967119850503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lopez-Olivo MA, Landon GC, Siff SJ, et al. Psychosocial determinants of outcomes in knee replacement. Ann Rheum Dis. 2011;70:1775-1781. [DOI] [PubMed] [Google Scholar]
- 18.Lowe CJM, Barker KL, Murray DW, Sackley CM. Letter to the editor: complications of total knee arthroplasty: standardized list and definitions of The Knee Society. Clin Orthop Relat Res. 2013;471:3706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mehaffey JH, Hawkins RB, Charles EJ, et al. Socioeconomically distressed communities associated with long-term mortality after bariatric surgery. J Surg Res. 2019;243:8-13. [DOI] [PubMed] [Google Scholar]
- 20.Mesko NW, Bachmann KR, Kovacevic D, et al. Thirty-day readmission following total hip and knee arthroplasty–a preliminary single institution predictive model. J Arthroplasty. 2014;29:1532-1538. [DOI] [PubMed] [Google Scholar]
- 21.Nwachukwu BU, Kenny AD, Losina E, Chibnik LB, Katz JN. Complications for racial and ethnic minority groups after total hip and knee replacement: a review of the literature. J Bone Joint Surg Am. 2010;92:338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Owens JM, Bedard NA, Dowdle SB, Gao Y, Callaghan JJ. Venous thromboembolism following total knee arthroplasty: does race matter? J Arthroplasty. 2018;33:S239-S243. [DOI] [PubMed] [Google Scholar]
- 23.Pandya NK, Wustrack R, Metz L, Ward D. Current concepts in orthopaedic care disparities. J Am Acad Orthop Surg. 2018;26:823-832. [DOI] [PubMed] [Google Scholar]
- 24.Price JH, Khubchandani J, Webb FJ. Poverty and health disparities: what can public health professionals do? Health Promot Pract. 2018;19:170-174. [DOI] [PubMed] [Google Scholar]
- 25.Ramos CL, Bagley JH, Shahin MN, et al. The impact of the socioeconomic “Distressed Communities Index” on outcomes after mechanical thrombectomy for acute ischemic stroke. Neurosurgery. 2020;67:103. [Google Scholar]
- 26.Rasouli MR, Restrepo C, Maltenfort MG, Purtill JJ, Parvizi J. Risk factors for surgical site infection following total joint arthroplasty. J Bone Joint Surg Am. 2014;96:e158. [DOI] [PubMed] [Google Scholar]
- 27.Sandoval V, Saleeby E, Jackson A, Smith L, Schickedancz A. Unmet social needs in the prenatal period: effects on birth outcomes and child health [39O]. Obstet Gynecol. 2020;135:167S. [Google Scholar]
- 28.Shahid H, Singh JA. Racial/ethnic disparity in rates and outcomes of total joint arthroplasty. Curr Rheumatol Rep. 2016;18:1-13. [DOI] [PubMed] [Google Scholar]
- 29.Stone AH, MacDonald JH, Joshi MS, King PJ. Differences in perioperative outcomes and complications between African American and white patients after total joint arthroplasty. J Arthroplasty. 2019;34:656-662. [DOI] [PubMed] [Google Scholar]
- 30.Thompson JM, Park MK, Qureshi AA, Cho E. Race and alopecia areata amongst US women. J Investig Dermatol Symp Proc. 2018;19:S47-S50. [DOI] [PubMed] [Google Scholar]
- 31.Xiong G, Greene NE, Lightsey HMI, et al. Telemedicine use in orthopaedic surgery varies by race, ethnicity, primary language, and insurance status. Clin Orthop Relat Res. 2021;479:1417-1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zhang W, Lyman S, Boutin-Foster C, et al. Racial and ethnic disparities in utilization rate, hospital volume, and perioperative outcomes after total knee arthroplasty. J Bone Joint Surg Am. 2016;98:1243-1252. [DOI] [PubMed] [Google Scholar]