

The standard treatment for rectal gastrointestinal stromal tumors (GISTs) without metastases is total surgical resection, but this strategy is controversial owing to the extremely low prevalence of GISTs. Minimally invasive transanal surgery can be performed as a surgical reduction technique via transanal local excision; however, this technique is not as selective as endoscopic resection and anastomotic leakage is a reported complication as a result of full-layer resection 1 . Although a number of endoscopic resections have been reported 2 3 , no established procedure is available.
A 36-year-old man was diagnosed with a GIST of approximately 1.5 cm in the lower rectum ( Fig. 1 ). Endoscopic ultrasound revealed a tumor that was predominantly located in the internal circular muscle, without invasion of the external longitudinal muscle ( Fig. 2 ). We considered selective resection to preserve the external longitudinal muscle and subsequently performed endoscopic intermuscular dissection 4 . We used a GIF-H290 T gastroscope (Olympus, Tokyo, Japan) with an ST hood short-type tip (DH-28GR; Fujifilm, Tokyo, Japan) and resected the tumor using a DualKnife J (Olympus, Tokyo, Japan) and injection of hyaluronic acid. We adopted the Endocut I mode (effect 2, duration 3, interval 3) of the VIO300-D electrosurgical system (Erbe Elektromedizin GmbH, Tübingen, Germany) during myotomy. Treatment was completed within 45 minutes without perforation ( Video 1 ; Fig. 3 ). Pathological findings demonstrated complete resection without tumor exposure and a very low risk GIST ( Fig. 4 ) 5 . The layer between the inner circular and external longitudinal muscles was accessed and injected with water-jet instrumentation to facilitate dissection and selective excision. The patient was discharged on the sixth postoperative day without complications.
Fig. 1.
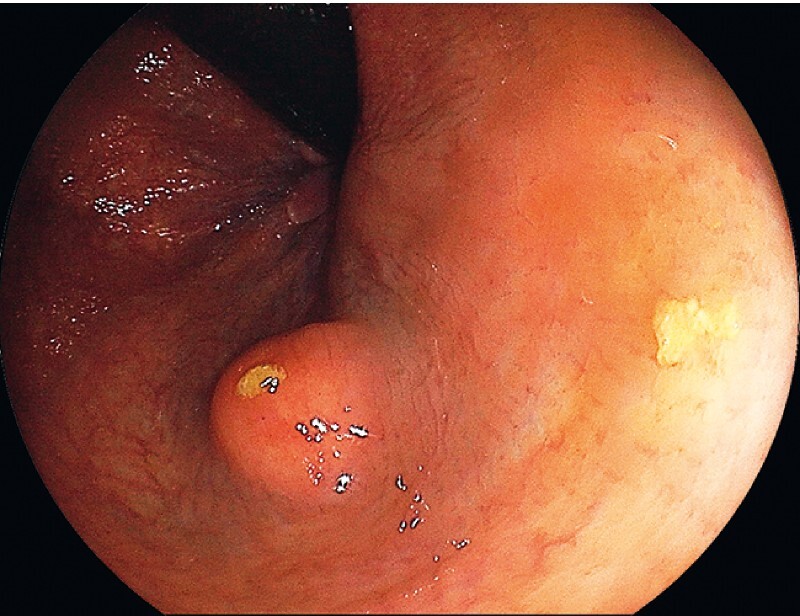
Endoscopic view showing a 1.5-cm submucosal tumor in the lower rectum, which was diagnosed on a boring biopsy to be a gastrointestinal stromal tumor.
Fig. 2.
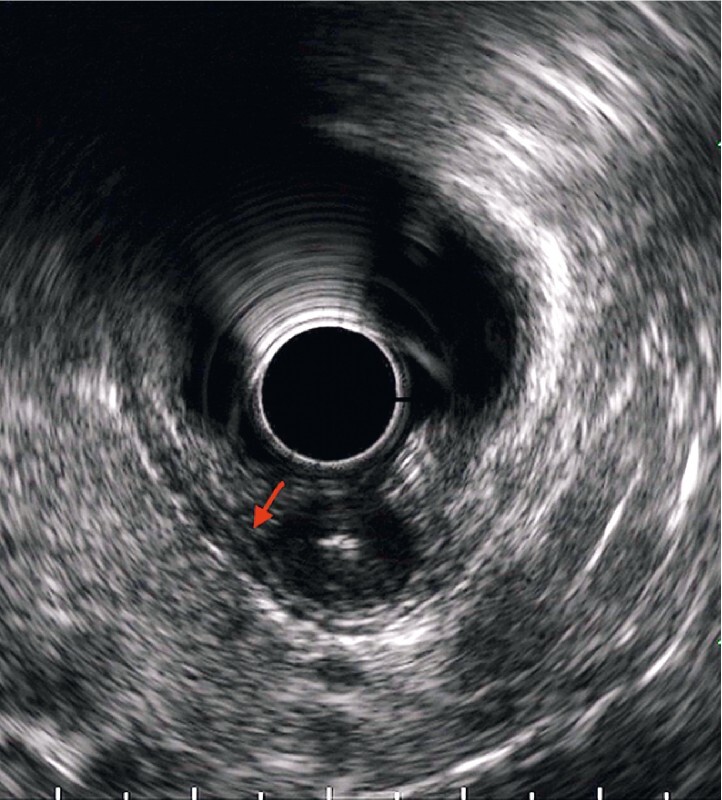
Endoscopic ultrasound image showing that the tumor was located primarily in the internal circular muscle, extending to the internal fourth layer (arrow), with no invasion of the external fourth layer.
Fig. 3.

Endoscopic appearance after the tumor and the invaded internal circular muscle had been resected, leaving the external longitudinal muscle preserved and intact, with no evidence of perforation.
Fig. 4.
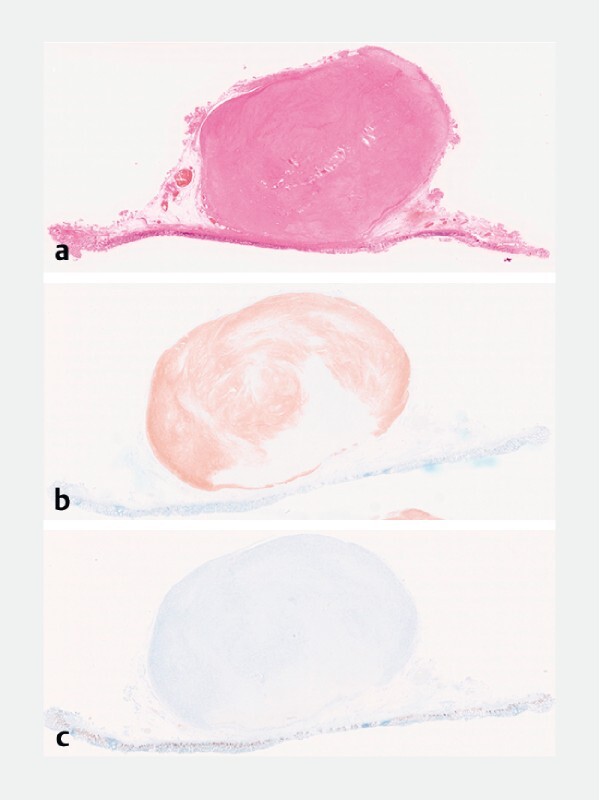
Histopathology of the resected submucosal tumor showing: a on hematoxylin and eosin staining, the tumor surface covered by the submucosal and muscular layer, with no tumor exposure observed; b positivity on c-Kit staining; c a Ki-67 index of < 5 %.
Endoscopic intermuscular dissection can be a treatment option for lower rectal GISTs without preoperative invasion of the external longitudinal muscle.
Video 1 Endoscopic intermuscular dissection is performed for a rectal gastrointestinal stromal tumor, allowing the preservation of the external longitudinal muscle.
Endoscopy_UCTN_Code_TTT_1AQ_2AD
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Albert M R, Atallah S B, deBeche-Adams T C et al. Transanal minimally invasive surgery (TAMIS) for local excision of benign neoplasms and early-stage rectal cancer: efficacy and outcomes in the first 50 patients. Dis Colon Rectum. 2013;56:301–307. doi: 10.1097/DCR.0b013e31827ca313. [DOI] [PubMed] [Google Scholar]
- 2.Wallenhorst T, Jacques J, Lièvre A et al. Endoscopic resection of a rectal gastrointestinal stromal tumor using the submucosal tunneling endoscopic resection (STER) technique. Endoscopy. 2022;54:E273–E274. doi: 10.1055/a-1508-5241. [DOI] [PubMed] [Google Scholar]
- 3.Kim S J, Jung Y, Hong R et al. Successful endoscopic resection of a rectal gastrointestinal stromal tumor larger than 5 cm. Korean J Gastroenterol. 2021;78:235–239. doi: 10.4166/kjg.2021.097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moons L MG, Bastiaansen B AJ, Richir M C et al. Endoscopic intermuscular dissection for deep submucosal invasive cancer in the rectum: a new endoscopic approach. Endoscopy. 2022;54:993–998. doi: 10.1055/a-1748-8573. [DOI] [PubMed] [Google Scholar]
- 5.Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum Pathol. 2008;39:1411–1419. doi: 10.1016/j.humpath.2008.06.025. [DOI] [PubMed] [Google Scholar]