

Abstract
Duplication cysts are one of the rare congenital anomalies of the gastrointestinal tract. Although it can be seen at all levels throughout the gastrointestinal tract, it is most common in the ileum. One of the rarest of duplication cysts is cecal duplication cyst. Clinically, they become present in the form of vomiting, distention, abdominal pain and palpable mass. Rarely, it can cause acute abdomen such as perforation and obstruction. We present a case of cecal duplication cyst requiring urgent surgical treatment that causes obstruction in a 3-month-old baby.
Keywords: Duplication cyst, intestinal obstruction, ultrasonography
Duplication cysts are rare congenital anomalies that can be seen along the gastrointestinal tract. Its prevalence has been reported between 1/4500–1/10000. They can be in cystic and tubular form [1]. They are mostly seen in small bowel loops, most often in the ileum [2]. Colonic and rectal duplications are extremely rare. It usually gives signs in the first year of life. Its symptoms vary according to the size, type and location of the cyst. The most common symptoms are nausea-vomiting, abdominal pain, distension, and the palpable mass. Rarely, especially colonic duplication cysts cause perforation, intussusception, intestinal obstruction and volvulus [3].
In this case, the clinical, radiological and pathological findings of the cecal duplication cyst causing ileus were presented.
CASE REPORT
The 3-month-old baby boy was admitted to the emergency child service due to severe vomiting, abdominal distention and lack of gas gaita for 3–4 days. Except for the 35-week cesarean birth history, there was no pathology in his curriculum vitae. His physical examination revealed tenderness in the abdomen and a decrease in bowel sounds. Laboratory results have neutrophil leukocytosis. On the standing direct abdominal x-ray, air-fluid levels were present in the small bowel loops in the middle part of the abdomen (Fig. 1A). In the right lower quadrant, in the ileocecal region, 35x36 mm in size, lobulated contoured, dense cystic lesion and dilated bowel loops were present in ultrasonography examination (Fig. 1B). In contrast-enhanced abdominal computed tomography (CT) examination, a thick-walled cystic lesion that obstructed the lumen at the level of the cecum was observed. There was dilatation in the small bowel loops proximal to this level (Fig. 1C). As a first diagnosis, ileus secondary to the duplication cyst was considered. The patient was hospitalized for emergency surgery. A cystectomy procedure was applied to the lesion in the cecum (Fig. 2A). On the third postoperative day, the patient was discharged. The pathology result of the material removed during the operation was compatible with the cecal duplication cyst (Fig. 2B).
FIGURE 1.

(A) On standing abdominal X-ray, there is dilatation and air-fluid leveling in small bowel loops in the middle part of the abdomen. (B) In ultrasonography, a thick-walled cystic mass lesion with thick contents is observed. (C) In contrast-enhanced abdominal computed tomography, it is observed as a thick-walled cystic mass at the level of cecum.
FIGURE 2.
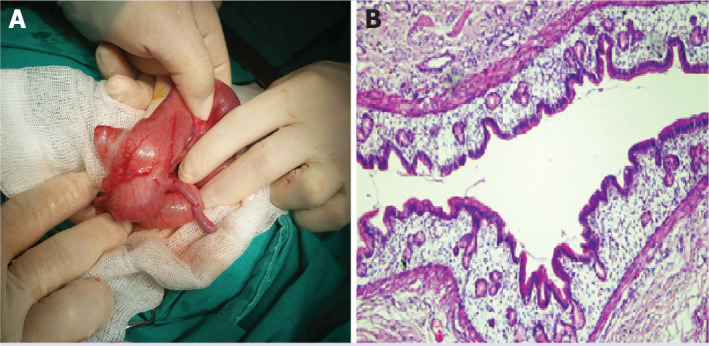
(A) Macroscopic view of the duplication cyst is observed. (B) Hematoxylin-eosin (HE) x 100: Cyst wall covered with gastric type columnar epithelium.
DISCUSSION
Intestinal duplications are rare congenital anomalies that can be seen in the entire gastrointestinal tract. Although its etiology is not fully known, many theories have been proposed. The most accepted theories are persistence of fetal intestinal diverticulum, defect in the recanalization of the primitive intestine, partial mating and notochord separation [1]. They are most common in small bowel loops [2]. Puligandla et al. [4] reported that duplication cysts were located in 31.5% ileum, 30.2% ileocecal valve, 9.6% duodenum, 8.2% stomach and 8.2% jejunum. In the presented study, only one of 73 patients had a duplication cyst in the cecum. Duplication cysts differ from other abdominal cystic lesions due to their intestinal mucosa and mucus content. They are usually located on the mesenteric side [5]. Often vertebral anomalies are accompanied. The pathology of our case was compatible with cecal duplication cyst. Vertebral anomaly was not detected.
Duplication cysts can be asymptomatic depending on the location, type and size, as well as cause an acute abdomen. They are often presented as vomiting, abdominal distention and palpable abdominal mass. They can rarely cause acute abdominal manifestations such as intussusception, perforation, obstruction and volvulus. Duplication cysts causing acute abdomen are mostly colonic located [3]. In our case, severe vomiting and abdominal distension were observed as a result of advanced obstruction due to duplication cyst.
In the diagnosis of duplication cyst, standing direct abdominal X-ray, ultrasonography, computed tomography and magnetic resonance imaging are used. Today, ultrasonography is used most frequently. Ultrasonography gives detailed information about the localization and origin of pediatric intraabdominal cysts. In ultrasonography, duplication cysts are identified by the presence of the echogenic inner mucosal layer and the hypoechoic muscular layer [6]. Nowadays, CT and MRI are used less frequently in terms of anatomical detail determination and complication research [7, 8]. In our case, air fluid levels in small bowel loops in the standing direct abdominal X-ray, and lobular contoured cystic lesion in the right lower quadrant on ultrasonography. On contrast-enhanced abdominal CT, there was a thick-walled cystic lesion causing obstruction at the cecum level. Dilatation was observed in small bowel loops proximal to this level.
Treatment of duplication cysts is surgical excision due to possible complications. Surgical treatment varies according to the type of cyst and location. Esophageal and gastric duplication cysts should be treated with cystectomy and other intestinal cysts with either cystectomy or resection anastomosis. In cases where cystectomy is impossible, cystotomy and mucosectomy is an option [8]. Our patient underwent cystectomy.
In conclusion, duplication cysts should be kept in mind in differential diagnosis in cases investigated for ileus in the pediatric population. Ultrasonography is a guide for surgeons in the exclusion of other acute abdominal pathologies and in the diagnosis of duplication cyst.
Footnotes
Cite this article as: Cullu N, Suzen A, Ozdemir MY, Celik SY. Cecal duplication cyst causing ileus: A rare pediatric case report. North Clin Istanb 2022;9(6):663–665.
Informed Consent
Written informed consent was obtained from the patient for the publication of the case report and the accompanying images.
Conflict of Interest
No conflict of interest was declared by the authors.
Financial Disclosure
The authors declared that this study has received no financial support.
Authorship Contributions
Concept – NC, AS, MYO, SYC; Design – NC, AS, MYO, SYC; Supervision – NC, AS, MYO, SYC; Fundings – NC, AS; Materials – SYC; Data collection and/or processing – NC, SYC; Analysis and/or interpretation – AS, MYO; Literature review – NC, MYO; Writing – NC, MYO; Critical review – NC, AS, SYC.
References
- 1.Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics. 1993;13:1063–80. doi: 10.1148/radiographics.13.5.8210590. [DOI] [PubMed] [Google Scholar]
- 2.Kumar K, Dhull VS, Karunanithi S, Chakraborty PS, Roy SG, Ghosh S, et al. Synchronous thoracic and abdominal enteric duplication cysts: Accurate detection with (99m)Tc-pertechnetate scintigraphy. Indian J Nucl Med. 2015;30:59–61. doi: 10.4103/0972-3919.147545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Erginel B, Soysal FG, Ozbey H, Keskin E, Celik A, Karadag A, et al. Enteric duplication cysts in children: a single-institution series with forty patients in twenty-six years. World J Surg. 2017;41:620–4. doi: 10.1007/s00268-016-3742-4. [DOI] [PubMed] [Google Scholar]
- 4.Puligandla PS, Nguyen LT, St-Vil D, Flageole H, Bensoussan AL, Nguyen VH, et al. Gastrointestinal duplications. J Pediatr Surg. 2003;38:740–4. doi: 10.1016/jpsu.2003.50197. [DOI] [PubMed] [Google Scholar]
- 5.Kuo HC, Lee HC, Shin CH, Sheu JC, Chang PY, Wang NL. Clinical spectrum of alimentary tract duplication in children. Acta Paediatr Taiwan. 2004;45:85–8. [PubMed] [Google Scholar]
- 6.Inoue Y, Nakamura H. Adenocarcinoma arising in colonic duplication cysts with calcification: CT findings of two cases. Abdom Imaging. 1998;23:135–7. doi: 10.1007/s002619900305. [DOI] [PubMed] [Google Scholar]
- 7.Lee NK, Kim S, Jeon TY, Kim HS, Kim DH, Seo HI, et al. Complications of congenital and developmental abnormalities of the gastrointestinal tract in adolescents and adults: evaluation with multimodality imaging. Radiographics. 2010;30:1489–507. doi: 10.1148/rg.306105504. [DOI] [PubMed] [Google Scholar]
- 8.Gupta P, Sharma R, Kumar S, Gadodia A, Roy KK, Malhotra N, et al. Role of MRI in fetal abdominal cystic masses detected on prenatal sonography. Arch Gynecol Obstet. 2010;281:519–26. doi: 10.1007/s00404-009-1190-1. [DOI] [PubMed] [Google Scholar]