

Abstract
OBJECTIVE
The objective of the study was to carry out validity and reliability of Type 1 Diabetes Stigma Assessment Scale (DSAS-1) in Turkish.
METHODS
The methodological study was conducted between December 2017 and May 2019, with 147 patients with Type 1 diabetes who applied to the Endocrinology, Internal Medicine policlinics of a Training and Research Hospital. The data were collected with the Introductory Information Form and DSAS-1. SPSS-22 and Mplus Version-7.4 were used for data analysis. Validity (group-back translation method, Polit and Beck technique, factor analysis, and known-group comparison and pilot study) and reliability (test-retest reliability, Cronbach’s alpha reliability coefficient, and item-total correlation) analyses were used.
RESULTS
It was found that 94.7% of the content validity index of the items of the DSAS-1 was 0.80 or above; the scale can factorable (Kaiser-Meyer-Olkin=0.86) and it was determined that the scale was able to separate known groups; the scale confirmed the 3-factor structure according to confirmatory factor analysis; the factor loads varied between 0.34 and 0.87 and their level was suitable according to fit index criteria (CFI=0.90, TLI=0.89, RMSEA=0.069, SRMR=0.065, Chi-square/df=1.706); the test-retest reliability value (r) was above 0.82; Cronbach’s alpha coefficient of Turkish DSAS-1 was 0.89; and Cronbach’s alpha coefficient of subscales was, respectively, to be 0.81, 0.80, and 0.81.
CONCLUSION
It was found that the DSAS-1 has validity and reliability in Turkish and is a suitable measurement tool to evaluate the stigma by the individuals with a diagnosis of Type 1 diabetes in Turkiye.
Keywords: Stigma, type 1 diabetes mellitus, validity
Highlight key points
Type 1 diabetes-related stigma is a common problem in our country as in many countries.
Type 1 diabetes-related stigma is a preventable psychosocial problem.
The first step in reducing type 1 diabetes-related stigma is to do research on the subject.
Turkish Type 1 Diabetes Stigma Assessment Scale is a valid and reliable measurement tool.
Type 1 diabetes is a chronic metabolic disease, occurs at any age [1], and poses a risk for many psychiatric and psychosocial problems. One of these problems and maybe one of the most important one of them are stigma and discrimination [2]. According to the study conducted in 17 countries (Turkiye, the United States, Canada, France, etc.), 10.4–31.0% of the individuals with diabetes were exposed to discrimination, although varied from country to another. Turkiye discrimination/stigma mean score among the countries where the study was conducted had the highest and the ratio of discrimination was determined to be approximately 28%. It was reported that individuals with Type 1 diabetes are exposed to more discrimination compared to individuals with Type 2 diabetes [3]. Diabetes-related stigma has rapidly gained attention around the world and is needed to research [4].
Stigma was defined by Goffman in 1960 as a social process consisting of labeling, stereotypical thoughts, discrimination, loss of status, and a social process of discrimination [5]. Stigma is seen in type 1 diabetes in three different ways. Self (internalized) stigma is stigmatizing yourself [5, 6]. In individuals experiencing this kind of stigma, denying the diagnosis of diabetes, hiding the diagnosis of diabetes from other for the fear of being blamed or discriminated or preventing intervention to their diet [7], injecting insulin only in public toilets or at home, and avoiding checking blood glucose in crowded places may be seen [8]. Social (interpersonal) stigma is defined as the stigmatization of individuals diagnosed with diabetes by other individuals in the community [5, 6]. Other people think that diabetes is the fault of individuals with diabetes [8, 9], they always sick and cannot do anything [10]. Other people believe that individuals with diabetes are deprived of many things and restricted in terms of food [10]. It can be seen as not inviting to places where there are unhealthy or sugary foods or restrictions [11], considering them as drug addicts and looking as strange at people who do insulin injection, supposing people who experience hypoglycemia as drunk [2, 9, 11], refraining from entering into emotional relations with them, thinking that diabetes affects family life and pregnancy and, therefore, not marrying with them, thinking that they should not conceive [10], and showing positive discrimination [9] (showing excessive tenderness, providing support to them even in what they can do by themselves). Structural stigma defined as the stigmatization of individuals diagnosed with diabetes by government, law, and organization [5, 6]. This type of stigma can be seen as rejecting their applications to shift works, dismissing them when it is found out that they have a diagnosis of diabetes, and giving them jobs that are much lighter compared to their capabilities [2] and changing employment prospects [12].
Type 1 diabetes-related stigma is known to be associated with poor glycemic control, elevated HbA1c, severe hypoglycemia, high diabetes distress, lower self-esteem, pronounced depressive symptoms, and less social support [13–15]. In summary, stigma in diabetes affected individuals physically, psychologically, emotionally, and socially in many ways. At this point, nurses (especially psychiatric consultation-liaison nursing and diabetes nurses) [16] and doctors (psychiatrists and internal medicine specialists) can play an active role in coping with the psychosocial problems experienced by individuals with chronic physical diseases such as diabetes, due to their professional and legal responsibilities.
According to Advocacy guide to the IDF Diabetes Atlas 2019, discrimination against people with diabetes is being problem that requires urgent action [17]. For this, it is first recommended that national surveys studies are recommended to understand extent and impact of stigma using questionnaires such as the validated Type 1 Diabetes Stigma Assessment Scale (DSAS-1) [18]. Although there are studies and scales related to stigma in diseases such as HIV, psoriasis, or tuberculosis in our country, it is seen that there are not enough studies related to stigma in diabetes. Perhaps, maybe the most important reason for this is that there is no standardized measuring tool. Turkish scales related to stigma are not intended for diabetes. Disease-specific stigma measurement tools provide more reliable measurement. Therefore, need a standard and specific measurement tool that can be easily used and evaluated in practice. Based on this essence, the purpose of this study is to examine the validity and reliability of the DSAS-1, which is developed to evaluate stigma in patients diagnosed with Type 1 diabetes. Two hypotheses were evaluated for the purpose of this study.
“The DSAS-1” adapted in Turkish is a valid scale.
“The DSAS-1” adapted in Turkish is a reliable scale.
Thanks to research that the validity and reliability of DSAS-1, the first standard measurement tool to evaluate stigma in Type 1 diabetes will be introduced to the national literature for use in studies and clinics. As this scale is a step for studies related to stigma in Type 1 diabetes, it is thought that it will contribute to preventing stigma and reducing existing stigma in Type 1 diabetes, improving individuals’ coping skills, increasing adaptation to the disease, and improving the quality of life.
MATERIALS AND METHODS
The study is a methodological study conducted to assess the validity and reliability of the DSAS-1.
Sample of the Study
The study was conducted between December 2017 and May 2019. The data were collected in the Endocrinology and Internal Medicine Polyclinics of a Training and Research Hospital. To make validity and reliability assessments of the scale, 3–10 times higher number of individuals should be reached for each scale item in sample determination [19]. In the light of the literature, 147 patients (7.7 times higher number of items) were included in the study. The reliability assessment of the study was conducted with 30 patients included in the sample, who agreed to participate in the retest 2–4 weeks after the test.
Inclusion and Exclusion Criteria of the Study
Patients who were admitted to the Training and Research Hospital Endocrinology and Internal Medicine Polyclinics were diagnosed with Type 1 diabetes at least 6 months ago and between the ages of 18 and 75 (adults) are included in the study. Patients who were cannot speak and understand Turkish on a level that can provide communication, not agreed to participate in the study, and not completed the entire scale (100%) were not included in the study.
Ethical Approval
A permit was obtained from Browne et al. [20] for using the scale. In addition, the approval of the ethics committee approval (number: 279 date: November 29, 2017) was obtained from the Non-Interventional Research Ethics Committee of Izmir Katip Celebi University Hospital while the written permissions of the policlinic responsible for the study and the Provincial Health Directorate were also obtained. In addition, verbal and written informed consents were obtained from the patients. This study was carried out in accordance with the Declaration of Helsinki Principles. To prevent bias in sampling and data collection, for the test-retest analysis, the code consisting of the last 4 digits of the phone numbers was used for the patients who stated that they would come back to the polyclinics within 2–4 weeks. To prevent bias in data analysis, the scale was reapplied to the patients who applied to the polyclinics 2–4 weeks later and the codes were matched during data entry.
Data Collection Tools
Two forms were used in the study. These forms were Introductory Information Form and DSAS-1.
Introduction Information Form
It consists of 25 closed- and open-ended questions prepared by the researcher, including information about the sociodemographic characteristics of the participants, the diagnosis and treatment process, diabetes management, and stigma in diabetes.
DSAS-1
The scale developed by Browne et al. (2017) [20] was designed to evaluate stigma in adults with Type 1 diabetes. The scale has three subscales; “Treated differently,” “Blame and judgment,” and “Identity concerns.” (Treated differently 3, 6, 8, 12, 15, and 19 items; blame and judgment 1, 4, 9, 11, 14, and 17 items; and identity concerns 2, 5, 7, 10, 13, 16, and 18 items). Each item was designed as a 5-point Likert scale. The scores on the scale vary between 19 and 95. The Cronbach’s alpha reliability coefficients of the whole scale and its subscales were αTreated differently=0.89; αBlame and judgment=0.88; αIdentity concerns=0.89; and αTotal=0.93, respectively. DSAS-1 is a valid and reliable scale [20].
Statistical Analysis
IBM SPSS Statistics-22 (Statistical Package for the Social Sciences version 22, IBM Corp., Armonk, NY) and Mplus Version 7.4 software (Los Angeles, CA) were used in the analysis of the data. Number and percentage were used for descriptive data analysis. In the validity of the scale; I-CVI and S-CVI were used with Polit and Beck technique for content validity. Kaiser-Meyer-Olkin (KMO) and Bartlett test were used for the factorizability of the sample; eigenvalues and explained variance were used for factor analysis. CFI, TLI, RMSEA, SRMR, and Chi-square/df were used for fit indices. T-test for independent groups was used for known-group comparison. In the reliability of the scale; reliability coefficient(r), arithmetic mean, and Pearson’s correlation coefficient were used for stability; Cronbach’s alpha reliability coefficient and item-total correlation analyses were performed for internal consistency. In all analyses, the level of statistical significance was accepted as p<0.05 within the 95% confidence interval [19].
RESULTS
About 63.9% of the participants are women, 61.2% are single, and their average age is 29.55±10.25. The duration of diagnosis of Type 1 diabetes is 159.12±109.91 and 70.7% of the participants use the insulin pen. About 45.6% of the participants stated that they did not work and 8.8% stated that they did not work because they could not manage their diabetes. About 33.3% of the participants stated that they experienced stigma/discrimination and 36.7% stated that they felt stigma/discrimination (Table 1).
TABLE 1.
Characteristics of the study sample
| Characteristics of the study sample | n | % |
|---|---|---|
| Age; | ||
| X=29.55±10.25 years | ||
| Gender | ||
| Women | 94 | 63.9 |
| Man | 53 | 36.1 |
| Marital status | ||
| Married | 57 | 38.8 |
| Single | 90 | 61.2 |
| Education status | ||
| Primary school | 8 | 5.4 |
| Middle school | 13 | 8.8 |
| High school | 48 | 32.7 |
| University | 71 | 48.3 |
| Master/doctorate | 7 | 4.8 |
| Job | ||
| Officer | 33 | 22.4 |
| Worker | 45 | 30.6 |
| Self-employment | 17 | 11.6 |
| ousewife | 17 | 11.6 |
| Student | 35 | 23.8 |
| Employment status | ||
| Not working | 39 | 26.5 |
| Working | 67 | 45.6 |
| Retired | 9 | 6.1 |
| Student | 32 | 21.8 |
| Reason for not working* | ||
| Business not accepted because diabetes | 5 | 3.4 |
| Looking for a job | 12 | 8.2 |
| Cannot manage diabetes | 13 | 8.8 |
| Does not want | 20 | 13.6 |
| Household income | ||
| Income >Expense | 27 | 18.4 |
| Income = Expense | 72 | 49.0 |
| Income <Expense | 48 | 32.7 |
| Type 1 diabetes duration | ||
| X=159.12±109.91 months | ||
| Primary insulin treatment | ||
| Insulin pen | 104 | 70.7 |
| Insulin pump | 43 | 29.3 |
| Blood glucose measurement environment | ||
| Only at home | 32 | 21.8 |
| In closed areas (like a toilet) | 19 | 12.2 |
| In open and public places | 97 | 66.0 |
| Thinking that individuals with diabetes | ||
| experience stigma/discrimination* | ||
| Not thinking | 72 | 49.0 |
| Thinking** | 75 | 51.0 |
| By the media | 10 | 6.8 |
| By health worker/health system | 23 | 15.6 |
| By family/friend/school/workplace | 63 | 42.9 |
| Feeling of stigma/discrimination | ||
| Feeling | 49 | 33.3 |
| Not feeling | 98 | 66.7 |
| Experience of stigma/discrimination | ||
| Experience | 54 | 36.7 |
| Not experience | 93 | 63.3 |
*: It was not answered by all participants; **: Some participants marked multiple options.
Validity Analysis
Language Validity
The language validity of the scale was carried out in three levels. In the first levels, it was translated to Turkish by seven professionals. In the second levels, the Turkish version of the scale was translated back from Turkish to English by one specialist who did not see the English version of the scale. In the third levels, the scale was retranslated into Turkish by six experts. The expert group consists of one internal medicine nurse, six psychiatric nurses, one PLC nurse, one internal medicine consultant, two consultant psychiatrists, two psychologists, and one social worker who were fluent in English, native speakers of Turkish. The final texts which had been translated into Turkish were evaluated by the researcher with an expert; the most suitable ones were selected and thus the language validity of the scale was ensured.
Content Validity
The Polit-Beck technique was used to ensure the content validity of the scale. For the content validity, a group of 15 experts from different disciplines was formed. The scale was translated into Turkish and then sent to 15 experts through e-mail. Three experts were excluded as they did not answer, and two experts whose S-CVI scores were lower than 0.80 were also excluded from the evaluation due to the Polit-Beck technique used. Thus, the I-CVI values were obtained for each item by combining the evaluations of the 10 experts who answered. Minor adjustments were made in the 8th item with a I-CVI value of 0.7; 4, 6, 15, and 16th items with I-CVI value of 0.8; and 3rd item with I-CVI value of 0.9; in line with the recommendations of the experts.
Face Validity
For the face validity of the scale, the scale items were generally assessed by the researcher and the expert in terms of clarity and expression in accordance with the expert recommendations. On the other hand, a pilot study was conducted for surface validity. They were asked to evaluate the items of the scale by asking questions in terms of regularity and significance, legibility, clarity of terms, length of sentences, clarity, and clarity of meaning. According to the results of the pilot study, there was no need to make any changes in the scale.
Structural Validity
Factor Analysis
KMO was found as 0.86 to evaluate the suitability of the sample size for factor analysis. Chi-square value of Bartlett’s test of sphericity was determined as 1155.64 (degree of freedom=171) and this value was found to be statistically significant (p<0.001). The eigenvalues of the subscales were found as F1-eigenvalue=6.67, F2-eigenvalue=1.96, and F3-eigenvalue=1.28, respectively. The percentages of variance explained were 35.1%, 10.3%, and 6.7%, respectively. In the exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), it was observed that it explained a three-factor structure as in the original language. The factor loads of the items of the subscales of the DSAS-1 ranged from 0.34 to 0.87 (Table 2 and Fig. 1). The t values of all factor loads were statistically significant (p<0.01). The R2 (item reliability) values of all items in the scale ranged from 0.12 to 0.76 (Table 2). According to the confirmatory analyses, the CFI, TLI, RMSEA, SRMR, and Chi-square/df were found as 0.90, 0.89, 0.069, 0.065, and 1.706, respectively. They were statistically significant (p<0.01).
TABLE 2.
Exploratory-confirmatory factor analysis and reliability factors of Turkish Type 1 Diabetes Stigma Assessment Scale and items
| F1 (TD) | F2 (BJ) | F3 (IC) | R2 | t | ||||
|---|---|---|---|---|---|---|---|---|
| Items | EFA | CFA | EFA | CFA | EFA | CFA | ||
| I3 | 0.64 | 0.62 | 0.39 | 10.68* | ||||
| I6 | 0.53 | 0.62 | 0.39 | 10.78* | ||||
| I8 | 0.66 | 0.75 | 0.56 | 16.62* | ||||
| I12 | 0.74 | 0.71 | 0.51 | 14.92* | ||||
| I15 | 0.74 | 0.74 | 0.55 | 16.09* | ||||
| I19 | 0.37 | 0.46 | 0.21 | 6.51* | ||||
| I1 | 0.51 | 0.34 | 0.12 | 4.45* | ||||
| I4 | 0.53 | 0.38 | 0.15 | 5.14* | ||||
| I9 | 0.66 | 0.73 | 0.53 | 16.37* | ||||
| I11 | 0.79 | 0.87 | 0.76 | 29.53* | ||||
| I14 | 0.67 | 0.53 | 0.28 | 8.30* | ||||
| I17 | 0.75 | 0.85 | 0.73 | 27.35* | ||||
| I2 | 0.68 | 0.67 | 0.45 | 12.94* | ||||
| I5 | 0.66 | 0.69 | 0.48 | 13.72* | ||||
| I7 | 0.66 | 0.67 | 0.45 | 12.63* | ||||
| I10 | 0.74 | 0.77 | 0.59 | 18.22* | ||||
| I13 | 0.59 | 0.41 | 0.17 | 5.59* | ||||
| I16 | 0.37 | 0.38 | 0.14 | 4.92* | ||||
| I18 | 0.69 | 0.72 | 0.52 | 15.19* | ||||
TD: Treated differently; BJ: Blame and judgment; IC: Identity concerns; EFA: Exploratory factor analysis; CFA: Confirmatory factor analysis; *: P<0.01 statistically significant.
FIGURE 1.
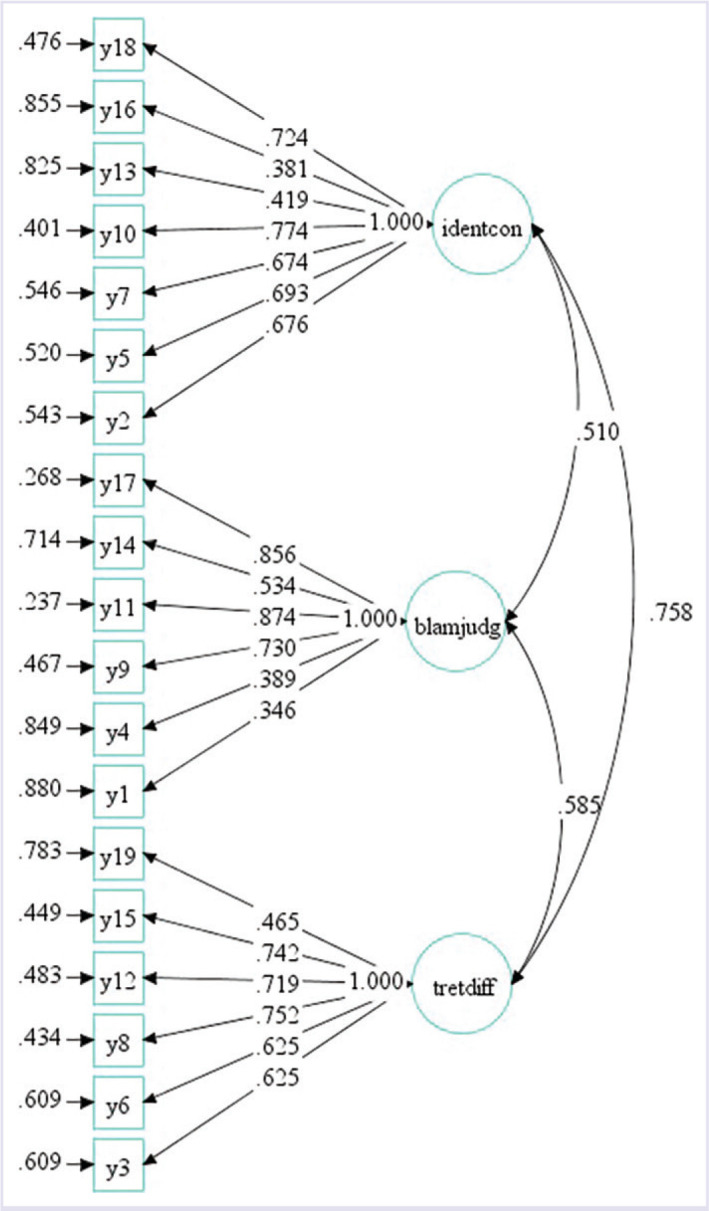
Path diagram of Type 1 Diabetes Stigma Assessment Scale.
Comparison of Known Groups
It was examined whether the scale scores differed according to whether individuals experienced and felt discrimination. The mean scores of the individuals with type 1 diabetes on the whole scale and its subscales were found to be statistically significantly different according to both whether they experienced discrimination (tTreated differently=5.07; p<0.01; tBlame and judgment=4.16; p<0.01; tIdentity concerns=3.51; p<0.01; and tTotal=5.17; p<0.01) and whether they felt discrimination (tTreated differently=5.94; p<0.01; tBlame and judgment=5.03; p<0.01; tIdentity concerns=5.24; p<0.01; and tTotal=6.76; p<0.01).
Reliability Analysis
Stability (Test-Retest) Reliability
The test-retest method was used to investigate the invariance of the DSAS-1 over time. The correlation coefficients of the whole scale and its subscales were found to be rTreated differently=0.86, rBlame and judgment=0.85, rIdentity Concerns=0.83, and rTotal=0.82.
Internal Consistency (Cronbach’s Alpha) Reliability
The reliability coefficients were αTreated differently=0.81, αBlame and Judgment=0.80, αIdentity Concerns=0.81, and αDSAS-1=0.89. The corrected item-total score correlation coefficients of all items of the DSAS-1 were found to be above 0.40 except 3 items. The corrected item-total score correlation coefficients of the 1st, 4th, and 13th items ranged between 0.25 and 0.40. When these 3 items excluded from the scale, Cronbach’s alpha coefficient did not significantly change the reliability of the test. The contribution of each item to the reliability of the test was found to be positive and similar (Table 3).
TABLE 3.
Item analysis results of Turkish Type 1 Diabetes Stigma Assessment Scale
| Turkish Type 1 Diabetes Stigma Assessment Scale | Item | Scale mean if item deleted | Scale variance if item deleted | Corrected item-total correlation | Alpha if item deleted |
|---|---|---|---|---|---|
| I1 | 44.1632 | 220.453 | 0.298 | 0.893 | |
| I2 | 45.2312 | 211.111 | 0.554 | 0.885 | |
| I3 | 44.9931 | 209.007 | 0.578 | 0.885 | |
| I4 | 44.1496 | 216.977 | 0.357 | 0.892 | |
| I5 | 45.2993 | 210.554 | 0.568 | 0.885 | |
| I6 | 45.2925 | 209.893 | 0.579 | 0.885 | |
| Alfa=0.89 | I7 | 45.5034 | 212.402 | 0.499 | 0.887 |
| Number of item=19 | I8 | 45.6394 | 212.575 | 0.606 | 0.884 |
| X=47.41±15.30 | I9 | 44.5510 | 206.783 | 0.539 | 0.886 |
| n=147 | I10 | 45.4217 | 210.903 | 0.568 | 0.885 |
| I11 | 44.6938 | 204.625 | 0.637 | 0.882 | |
| I12 | 45.3401 | 210.199 | 0.576 | 0.885 | |
| I13 | 44.2449 | 214.885 | 0.380 | 0.891 | |
| I14 | 43.7007 | 214.841 | 0.456 | 0.888 | |
| I15 | 45.4082 | 211.339 | 0.581 | 0.885 | |
| I16 | 45.1361 | 214.803 | 0.433 | 0.889 | |
| I17 | 44.6395 | 205.451 | 0.642 | 0.882 | |
| I18 | 45.1701 | 207.608 | 0.609 | 0.884 | |
| I19 | 44.8912 | 216.207 | 0.442 | 0.889 |
DISCUSSION
Validity Assessment
Language Validity
Language validity should be performed by experts with language proficiency and consisting of professionals from different fields [19]. In this context, seven professional experts who knew Turkish and English well and were suitable for the structure of the feature to be measured were asked to translate. Thus, the language validity of the scale was provided.
Content Validity
Content validity provides evidence about the degree to which elements of an assessment instrument are representative of the targeted construct [19]. According to the Polit and Beck [21] technique, I-CVI and S-CVI should be at least 0.80. The 8th item with I-CVI value below 0.80 and the 4th, 6th, 15th, and 16th items with I-CVI values equal to 0.80 were adjusted in accordance with the recommendations of the experts. Although it’s I-CVI value was above 0.80, the 3rd item was corrected in accordance with the feedbacks received from the experts. After the corrections and adjustments, I-CVI, mean I-CVI, S-CVI, and mean S-CVI values were found to be over 0.80. It was showed that the scale represents the construct of stigma, that is, the scale has content validity.
Face Validity
Face validity refers to the degree to which a scale subjectively appears to measure the construct that it is supposed to measure. The scale’s items were assessed by the researchers and experts in terms of clarity and expression [19, 22]. The scale’s items were found to be suitable. As a result of the pilot study, it was determined that the scale was adequate and clear, that is, the scale has face validity.
Structural Validity
The structural validity is used to evaluate how accurately the measuring instrument can measure the desired structure [19]. To evaluate the construct validity of the DSAS-1, factor analysis method and known-group comparisons were made [23].
Factor Analysis
Factor analysis is used to study the dimensionality of variables. The KMO values above 0.8 indicate that the sample has good factorability [19]. According to the KMO value and Chi-square value of Bartlett’s test of sphericity, the DSAS-1 is a factorability matrix. EFA and CFA were performed to assess the model data fit of the DSAS-1. In the original form of the scale, it was found that it could have a non-forced three-factor structure or a forced single-factor structure. However, it was decided to have a three-factor structure [20]. It has been seen that there are similar findings about the Danish version [24]. When the factor loads obtained in this study were evaluated, it was determined that the scale could have a three- or a single-factor structure as in the original scale. Factor load should be at least between 0.30 and 0.40 and t values should be significant [19]. It was found that the factor loads of all items and subscales of the DSAS-1 ranged between 0.34 and 0.87 and the t values of all factor loads were statistically significant (p<0.01). In the Turkish version of the DSAS-1, both the three- and one-factor structure were acceptable. To cohere to the original, the Turkish version of the DSAS-1 was considered to be three factors. According to the CFA results, R2 (item reliability) values of each item ranged between 0.12 and 0.76. R2 values of all items were found to be high. According to Yaşlioğlu, the analyses were performed according to Byrne’s concordance index standards [25] and the evaluations on the original scale for determining the fit index of the DSAS-1 [20]. It was determined that the CFI, RMSEA, SRMR, TLI, and Chi-square/df values were in compliance with the index criteria as well as the original scale value. In other words, this finding shows reliable measures of stigma in Type 1 diabetes, with evidence of structural validity.
Known-Groups Comparison
Known-groups validity evaluates to the ability of the measure to discriminate between groups known to clinically different [19]. DSAS-1 and its subscales were compared according to their status for thinking and feeling of the experience of discrimination and it was seen that the differences between the mean scores on both the whole scale and its subscales were statistically significant (p<0.01). In other words, both the whole and sub-scales of the Turkish version of the DSAS-1 can distinguish the known groups which are experience and feel of stigma or not experience and feel of stigma.
Reliability Assessment
Stability (Test-Retest) Reliability
Stability is a measure of the repeatability of a test over time, so gives the same results whenever it is used [23]. Test-retest method was used for stability since there was no similar form in Turkish. In this study, the DSAS-1 was reapplied to 30 individuals with Type 1 diabetes in the sample group 2–4 weeks after the first application. The obtained r value of 0.70 and above shows that the scale has test-retest reliability [19]. In this study, all the r values found in the study were higher than 0.70, both the whole scale and its subscales had test-retest reliability, in other words, showed that stigma’s measurement does not vary over time and the scale is stable.
Internal Consistency (Cronbach’s Alpha) Reliability
Internal consistency is consistency of results across items within content [23]. Sencan (2005) [19] stated that, according to George and Mallery (2003) [26], if the Cronbach’s alpha value determined for a measurement tool is >0.90, the scale reliability is excellent; if it varies between 0.80 and 0.90, the scale reliability is good; if it ranges between 0.70 and 0.80. In this study, it was observed that Cronbach’s alpha values ranged between 0.80 and 0.89 for the whole and sub-scales of the DSAS-1 while it ranges between 0.89 and 0.93 for original DSAS-1 and 0.75–0.89 for the Danish version [20, 24]. Accordingly, it can be said that the DSAS-1 shows a good reliability for the total of 19 items and its subscales. When the correlation coefficients between the whole DSAS-1 and its subscales were examined, the correlation coefficients between the mean scores on the whole scale and the subscales ranged between 0.458 and 0.856. It was determined that all p<0.01 were considered and thus there was a statistically significant relationship between the whole scale and the subscales. This finding shows that the items of the DSAS-1 are highly correlated with the whole scale and each item measures the feature to be measured in the same direction. It has been stated in the literature that the total item correlation should not be <0.30 or 0.50 [19, 23]. In this study, all items in the scale showed a high correlation with the scale as a whole. The Cronbach’s alpha values of the DSAS-1 were examined after the items were removed. The alpha coefficient did not dramatically increase the reliability of the test, if items after 1, 4, and 13 were excluded from the scale, with the corrected item-total score correlation coefficients ranged between 25.25 and 0.40. It was considered that each item contributed positively and similarly to the reliability of the test, and thus, these items were not removed from the scale to stick the original scale. These results showed that the scale items have high internal consistency and high reliability with each other.
Conclusion
As a result of the statistical analyses, the items of the Turkish version of Type 1 Diabetes Stigma Scale (DSAS-1) were found to represent the area which was aimed to be measured (content validity), to measure investigated structure (face validity), to consist of three subscale according to factor analysis, and to explain single structure. It was also found that it distinguishes known groups (construct validity), has a high internal consistency between its items (internal consistency reliability), and makes consistent measurements according to time (test-retest reliability). These results showed that DSAS-1 is a valid and reliable measurement tool to assess the stigma experienced and felt by individuals with Type 1 diabetes in Turkiye.
Access to the Turkish DSAS-1 Scale
The Turkish DSAS-1, as well as the original DSAS-1, is available free of charge to academic researchers, clinicians, and students for use in non-commercially funded research. Potential users are advised to email ecemutlu94@gmail.com, baysanarabaci@hotmail.com and info@acbrd.org.au to inquire about or access the latest version of the questionnaire (including instructions for administering the measure) and scoring guides.
Footnotes
Cite this article as: Mutlu Satil E, Baysan Arabaci L. Turkish validity and reliability of Type-1 Diabetes Stigma Assessment Scale. North Clin Istanb 2022;9(6):654–662.
Ethics Committee Approval
The Izmir Katip Celebi University Non-Interventional Research Ethics Committee granted approval for this study (date: 29.11.2017, number: 279).
Conflict of Interest
No conflict of interest was declared by the authors.
Financial Disclosure
The authors declared that this study has received no financial support.
Authorship Contributions
Concept – LBA, EMS; Design – LBA, EMS; Supervision – LBA; Fundings – LBA, EMS; Data collection and/or processing – EMS; Analysis and/or interpretation – LBA, EMS; Literature review – LBA, EMS; Writing – EMS; Critical review – LBA.
References
- 1.International Diabetes Federation . 9th Ed. Brussels, Belgium: 2019. IDF Diabetes Atlas. [PubMed] [Google Scholar]
- 2.Stuckey HL, Mullan-Jensen CB, Reach G, Kovacs Burns K, Piana N, Vallis M, et al. Personal accounts of the negative and adaptive psychosocial experiences of people with diabetes in the second Diabetes Attitudes, Wishes and Needs (DAWN2) study. Diabetes Care. 2014;37:2466–74. doi: 10.2337/dc13-2536. [DOI] [PubMed] [Google Scholar]
- 3.Nicolucci A, Kovacs Burns K, Holt RI, Comaschi M, Hermanns N, Ishii H, et al. DAWN2 Study Group Diabetes Attitudes, Wishes and Needs second study (DAWN2™): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet Med. 2013;30:767–77. doi: 10.1111/dme.12245. [DOI] [PubMed] [Google Scholar]
- 4.Kato A, Yamauchi T, Kadowaki T. A closer inspection of diabetes-related stigma: why more research is needed. Diabetol Int. 2019;11:73–5. doi: 10.1007/s13340-019-00421-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goffman E. Englewood Cliffs, NJ: Prentice Hall; 1963. Stigma: Notes on the Management of Spoiled Identity. [Google Scholar]
- 6.Van Brakel WH. Measuring health-related stigma-a literature review. Psychol Health Med. 2006;11:307–34. doi: 10.1080/13548500600595160. [DOI] [PubMed] [Google Scholar]
- 7.Irani MD, Abdoli S, Parvizy S, Fatemi NS, Amini M. Breaking stigma within us: the role of people with type 1 diabetes in overcoming diabetes-related stigma. Int J Diabetes Dev Ctries. 2015;35:264–70. [Google Scholar]
- 8.Schabert J, Browne JL, Mosely K, Speight J. Social stigma in diabetes: a framework to understand a growing problem for an increasing epidemic. Patient. 2013;6:1–10. doi: 10.1007/s40271-012-0001-0. [DOI] [PubMed] [Google Scholar]
- 9.Abdoli S, Hardy LR, Hall J. The complexities of “struggling to live life”. Diabetes Educ. 2017;43:206–15. doi: 10.1177/0145721717697245. [DOI] [PubMed] [Google Scholar]
- 10.Abdoli S, Abazari P, Mardanian L. Exploring diabetes type 1-related stigma. Iran J Nurs Midwifery Res. 2013;18:65–70. [PMC free article] [PubMed] [Google Scholar]
- 11.Browne JL, Ventura A, Mosely K, Speight J. ‘I’m not a druggie, I’m just a diabetic’: a qualitative study of stigma from the perspective of adults with type 1 diabetes. BMJ Open. 2014;4:e005625. doi: 10.1136/bmjopen-2014-005625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee SM, Lim LC, Koh D. Stigma among workers attending a hospital specialist diabetes clinic. Occup Med (Lond) 2015;65:67–71. doi: 10.1093/occmed/kqu150. [DOI] [PubMed] [Google Scholar]
- 13.Hansen UM, Olesen K, Willaing I. Diabetes stigma and its association with diabetes outcomes: a cross-sectional study of adults with type 1 diabetes. Scand J Public Health. 2020;48:855–61. doi: 10.1177/1403494819862941. [DOI] [PubMed] [Google Scholar]
- 14.Brazeau AS, Nakhla M, Wright M, Henderson M, Panagiotopoulos C, Pacaud D, et al. Stigma and its association with glycemic control and hypoglycemia in adolescents and young adults with type 1 diabetes: cross-sectional study. J Med Internet Res. 2018;20:e151. doi: 10.2196/jmir.9432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gredig D, Bartelsen-Raemy A. Diabetes-related stigma affects the quality of life of people living with diabetes mellitus in Switzerland: implications for healthcare providers. Health Soc Care Community. 2017;25:1620–33. doi: 10.1111/hsc.12376. [DOI] [PubMed] [Google Scholar]
- 16.Resmi Gazete. 19 Nisan 2011 Tarihli 27910 Sayılı Hemşirelik Yönetmeliğinde Değişiklik Yapılmasına Dair Yönetmelik. Available at: http://www.resmigazete.gov.tr/eskiler/2011/04/20110419-5.htm Accessed Nov 1 2022.
- 17.International Diabetes Federation . 9th ed. 2019. Advocacy guide to the IDF Diabetes Atlas. [PubMed] [Google Scholar]
- 18.Wylie TAF, Shah C, Connor R, Farmer AJ, Ismail K, Millar B, et al. Transforming mental well-being for people with diabetes: research recommendations from Diabetes UK’s 2019 Diabetes and Mental Well-Being Workshop. Diabet Med. 2019;36:1532–8. doi: 10.1111/dme.14048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Şencan H. 1st ed. Ankara: Seçkin Yayıncılık Sanayi ve Ticaret AŞ; 2005. Sosyal ve davranışsal ölçümlerde güvenilirlik ve geçerlilik; pp. 499–559. [Google Scholar]
- 20.Browne JL, Ventura AD, Mosely K, Speight J. Measuring Type 1 diabetes stigma: development and validation of the Type 1 Diabetes Stigma Assessment Scale (DSAS-1) Diabet Med. 2017;34:1773–82. doi: 10.1111/dme.13507. [DOI] [PubMed] [Google Scholar]
- 21.Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29:489–97. doi: 10.1002/nur.20147. [DOI] [PubMed] [Google Scholar]
- 22.Çakmur H. Measurement-reliability-validity in research. TAF Preventive Medicine Bulletin. 2012;11:339–344. [Google Scholar]
- 23.Esin MN. Veri toplama yöntem ve araçları & veri toplama araçlarının güvenirlik ve geçerliği. In: Erdoğan S, Nahcivan N, Esin MN, editors. Hemşirelikte araştırma süreç uygulama ve kritik. 2nd ed. İstanbul: Nobel Tıp Kitabevileri; 2015. pp. 193–234. [Google Scholar]
- 24.Hansen UM, Willaing I, Ventura AD, Olesen K, Speight J, Browne JL. Stigma perceived and experienced by adults with type 1 diabetes: linguistic adaptation and psychometric validation of the Danish version of the Type 1 Diabetes Stigma Assessment Scale (DSAS-1 DK) Patient. 2018;11:403–12. doi: 10.1007/s40271-017-0289-x. [DOI] [PubMed] [Google Scholar]
- 25.Yaşlıoğlu MM. Factor analysis and validity in social sciences: application of exploratory and confirmatory factor analyses. İstanbul Üniversitesi İşletme Fakültesi Dergisi. 2017;46:74–85. [Google Scholar]
- 26.George D, Mallery P. 4th ed. Boston: Allyn & Bacon; 2003. SPSS for Windows step by step: A simpleguide and reference (11.0 update) [Google Scholar]