

The gastric fundus is the most challenging site for endoscopic submucosal dissection (ESD) because accessing the fundus with the tip of the endoscope is difficult. Furthermore, the wall of the fundus is thin and the knife-edge is pointed towards the muscle layer. A combination of the previously reported effective methods, namely, a multibending endoscope 1 , multiloop traction 2 , and underwater technique 3 may offer safe treatment in the fundus. Herein, we report a successful ESD performed by a trainee using these three methods.
A 58-year-old woman presented with a 10-mm type 0-IIa gastric adenocarcinoma (fundic gland type) in the gastric fundus ( Fig. 1 ). ESD was performed using a multibending endoscope (GIF-2TQ260M; Olympus, Tokyo, Japan) and a DualKnife J (KD-655L; Olympus, Tokyo, Japan) by an endoscopist who was inexperienced in fundal surgery, under the supervision of an experienced surgeon ( Video 1 ).
Fig. 1.
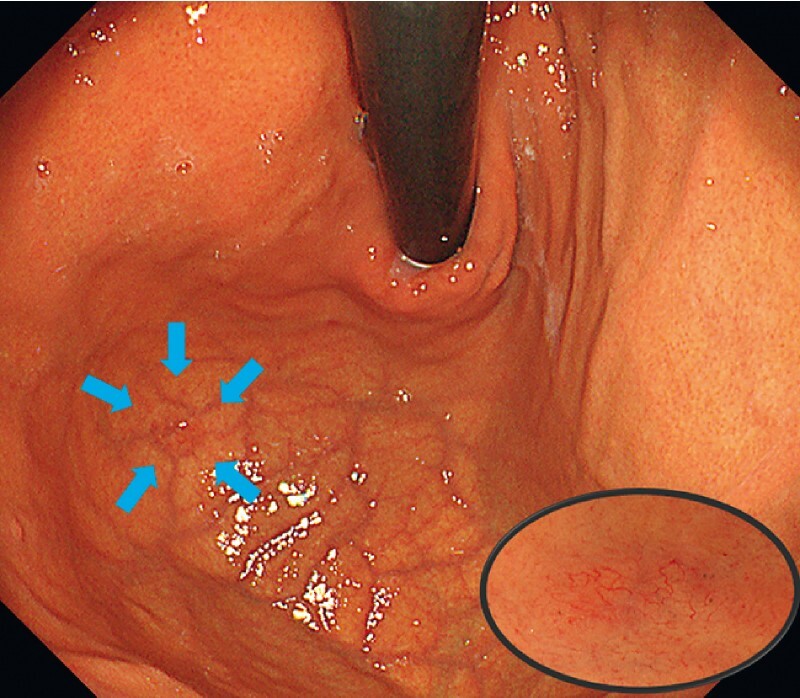
White-light endoscopic image of the lesion (blue arrows) showing a 10-mm type 0-IIa gastric cancer in the fundus of the stomach (inset, close-up image), which was revealed to be a gastric adenocarcinoma of the fundic gland type, pT1b (SM1), UL0, Ly0, V0, HM0, VM0.
Video 1 Endoscopic submucosal dissection of a lesion in the gastric fundus is safely performed by a nonexpert endoscopist using a combination of multibending endoscope, multiloop traction device, and the underwater method.
Although a conventional endoscope cannot reach the fundus, this area can be easily accessed with a multibending endoscope, so enabling an easy peripheral incision. Dissection of the submucosa was complicated because the stomach was tense with air and the knife-edge was facing the muscle layer. Once the stomach had been sufficiently degassed, the knife-edge was nearly parallel to the muscle layer; however, the resulting field of view for the procedure was unsatisfactory. Therefore, underwater ESD was performed, which enables safe dissection in the nondilated stomach, with the knife nearly parallel to the muscle layer, but with a good field of view ( Fig. 2 ). Furthermore, the respiratory movement was suppressed using this method. After the flap had been created, a multiloop traction device (Boston Scientific, Marlborough, Massachusetts, USA) was attached, and traction was applied in the opposite direction ( Fig. 3 ). The stomach was then dilated, providing better traction, and an uncomplicated en bloc dissection was performed by the trainee surgeon.
Fig. 2.
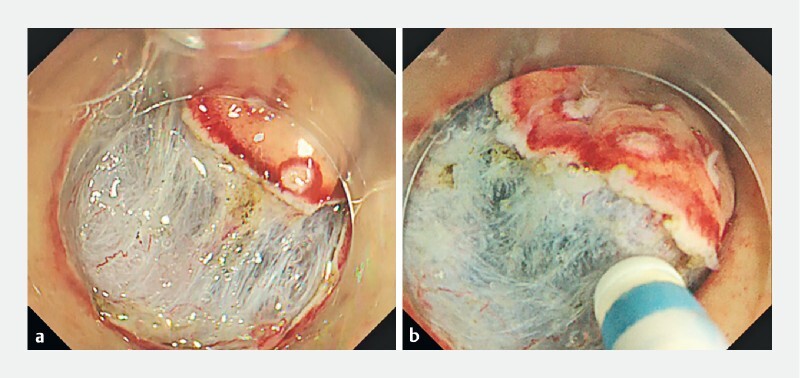
Endoscopic images of the lesion during endoscopic submucosal dissection (ESD) with: a conventional ESD, where the knife-edge is pointed towards the muscle layer when the stomach is filled with air; b underwater ESD, where a nearly parallel angle is obtained between the knife-edge and the muscle layer.
Fig. 3.
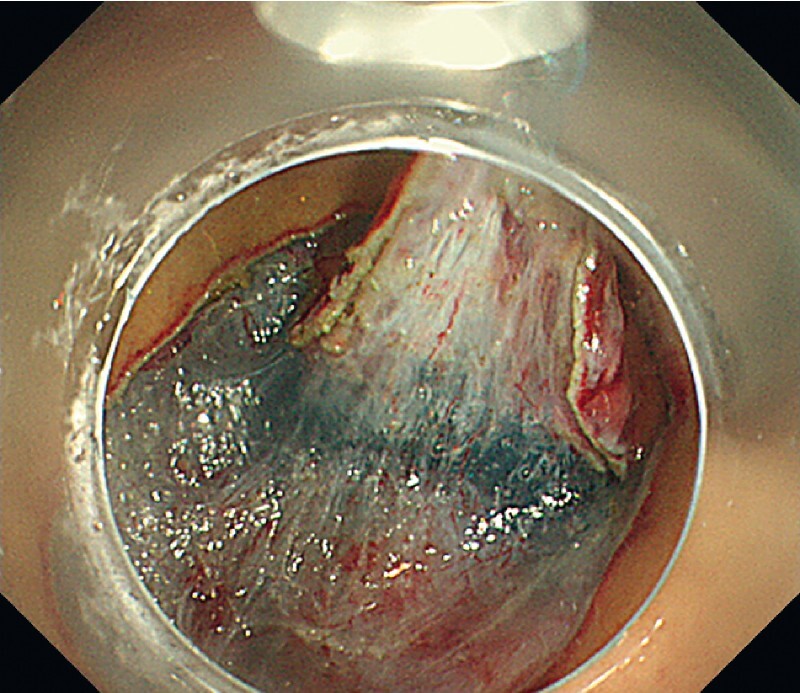
Endoscopic image showing the good view of the submucosa obtained by applying traction using a multiloop traction device.
We have demonstrated that even nonexperts can safely perform ESD in the fundus using these techniques.
Endoscopy_UCTN_Code_TTT_1AO_2AG
Acknowledgments
We thank Editage ( www.editage.com ) for English language editing and publication support.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Hamada K, Horikawa Y, Shiwa Y et al. Clinical benefit of the multibending endoscope for gastric endoscopic submucosal dissection: a randomized controlled trial. Endoscopy. 2021;53:683–690. doi: 10.1055/a-1288-0570. [DOI] [PubMed] [Google Scholar]
- 2.Matsui H, Tamai N, Futakuchi T et al. Multi-loop traction device facilitates gastric endoscopic submucosal dissection: ex vivo pilot study and an inaugural clinical experience. BMC Gastroenterol. 2022;22:10. doi: 10.1186/s12876-021-02085-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maida M, Sferrazza S, Murino A et al. Effectiveness and safety of underwater techniques in gastrointestinal endoscopy: a comprehensive review of the literature. Surg Endosc. 2021;35:37–51. doi: 10.1007/s00464-020-07907-8. [DOI] [PubMed] [Google Scholar]