

Abstract
Using national data on county-level mortality, coal mining, and shale development, we examine the effects of resource booms and busts on mortality in the United States. We find evidence that decreases in operating coal mines increased total all-cause mortality, non-drug mortality, and opioid overdose mortality, especially for counties with greater than 10 operating coal mines in 2000. Our model results for drug overdose mortality and opioid overdose mortality are sensitive to the panel’s start year. For shale development, the shale boom is associated with increases in non-drug suicides but otherwise had little impact on mortality. Our findings suggest a potential role for job-training programs and the cultivation of local healthcare resources in regions suffering coal busts and suicide prevention in areas with shale development.
Keywords: Opioid epidemic, shale boom, coal bust, economic shocks, mortality, I10 (Health Economics: General), Q00 (Environmental Economics), I15 (Health and Economic Development), Q33 (Resource Booms)
1. Introduction
An extensive literature has debated the relationship between business cycles and economic conditions on mortality. Some studies, especially in the U.S., have found evidence that economic growth improves health but may increase mortality contemporaneously and that recessions decrease or plateau mortality in the short run (Ruhm, 2000, 2015, 2016; Stevens et al., 2015). Economic conditions in early life have also been associated with lower later-life mortality (van den Berg, Lindeboom and Portrait, 2006; Almond and Currie, 2011; Lindo, 2015; Aizer et al., 2016; Cutler, Huang and Lleras-Muney, 2016; Hoynes, Schanzenbach and Almond, 2016; Noelke et al., 2019). Recent evidence suggests that some of the counter-intuitive findings are due to increased air pollution during economic boom periods and increased risky behaviors (e.g., alcohol consumption) (Cutler, Huang and Lleras-Muney, 2016; Heutel and Ruhm, 2016). Structural changes in the economy due to trade liberalization have reduced manufacturing, and these shocks have been linked to increased mortality, particularly increased opioid mortality (Charles, Hurst and Schwartz, 2018; Autor, Dorn and Hanson, 2019; Pierce and Schott, 2020). In this paper, we use plausibly exogenous shocks to local labor markets driven by the shale boom and coal bust to document a link between mortality and local economic conditions.
According to the Centers for Disease Control and Prevention, the U.S. age-adjusted fatal drug overdose rate grew from 6.1 to 21.7 per 100,000 people from 1999 to 2017; this increase was driven by the increased use of prescription and non-prescription opioids (Hedegaard, Minino and Warner, 2018). The causes of the epidemic are multifaceted: the increase in opioid prescriptions for pain management in the 1990s through the 2000s (Kuehn, 2007; Dart et al., 2015), the expanded promotion and marketing of pain relief drugs by pharmaceutical companies (Van Zee, 2009), and a regulatory environment increasingly focused on patient satisfaction (Kelly, Johnson and Harbison, 2016).
A growing line of research has also connected drug abuse with local demographic and socioeconomic factors, with evidence suggesting that declining economic conditions are associated with increased drug abuse (Martin Bassols and Vall Castelló 2016; Ayllón and Ferreira-Batista 2018; Carpenter, McClellan, and Rees 2017; Hollingsworth, Ruhm, and Simon 2017; Arkes 2007; Lee et al. 2015; Charles, Hurst, and Schwartz 2018; Betz and Jones 2018). The general argument in these studies is that local growth (decline) in economic opportunities may decrease (increase) substance abuse; this is commonly referred to as the “Deaths of Despair” hypothesis (Scutchfield and Keck, 2017; Stein et al., 2017; Dow et al., 2019; Ruhm, 2019).
In this paper, we examine how natural resource-fueled economic booms and busts impact local levels of non-drug mortality (i.e., all-cause mortality removing drug overdose mortality) and drug overdose mortality through the lens of prior evidence that economic conditions influence total mortality, as well as new evidence linking economic downturns to “Deaths of Despair.” We separately assess non-drug mortality as it may have a different causal relationship with local economic conditions from “Deaths of Despair”. We focus our attention on the recent shale oil and natural gas boom and the related and simultaneous bust in coal production. The shale oil and gas boom has been widespread across the U.S., leading to 52% and 39% increases in domestic oil and natural gas production, respectively, and a 79% increase in the level of electricity generation generated from natural gas between 2000 and 2016. This growth has been mainly at the expense of the coal industry; domestic coal production declined by 34% from a 21st-century high in 2008 to 2017 (estimates based on Mine Safety and Health Administration data). This decline has been driven by relative decreases in the price of natural gas to coal (Knittel, Metaxoglou and Trindade, 2015; Fell and Kaffine, 2018).
We argue that these energy-related developments can shed light on how economic and social dynamics impacted non-drug mortality trends and the scale of the drug overdose epidemic. Resource development has large effects on local employment (Agerton et al., 2017), wage and non-wage income (Black, McKinnish and Sanders, 2005; Brown, Fitzgerald and Weber, 2016; Feyrer, Mansur and Sacerdote, 2017), labor force participation (Hastings, Heller and Stephenson, 2017), the levels of disability and welfare-related payments (Black, Daniel and Sanders, 2002; Black, McKinnish and Sanders, 2003; Charles, Li and Stephens, 2017), and government revenue (Newell and Raimi, 2018; Morris, Kaufman and Doshi, 2019). It can also have positive economic spillovers into other industries (Marchand, 2012; Fleming and Measham, 2014). Most resource development has occurred in rural America, where opioid misuse and related mortality are the highest (Paulozzi and Xi, 2008; Young, Havens and Leukefeld, 2012; Keyes et al., 2013; Monnat and Rigg, 2016; Villapiano et al., 2017).
We apply fixed effects regression models at the county level and rely on intensive measures of resource development: the number of operating coal mines and the number of spudded horizontal oil and gas wells in a county by year. Due to the opioid epidemic co-occurring with these economic changes, we start by assessing the impact on non-drug mortality. Our measure of opioid overdose mortality uses a novel correction method (Boslett, Denham and Hill, 2020); we correct our outcome variable because ~22% of all drug overdoses (out of 632,331) did not have a classified drug from 1999–2016. Our identification strategy exploits temporal and spatial variation in coal mine closures and horizontal oil and gas well drilling from 2000 to 2016. We include state-by-year fixed effects to control for policy changes and other unobserved factors within the state and year that could impact mortality. We also estimate heterogeneity models by population characteristics and intensity of resource extraction.
For total all-cause and non-drug mortality, we find consistent evidence that declining coal mining is associated with increases in mortality. We do not observe strong evidence of a similar relationship for unconventional oil and gas development (UOGD). However, we find some evidence that UOGD reduces non-drug mortality, drug overdose mortality, and opioid overdose mortality in nearby areas. These effects appear to be predominantly felt by working-appenedents for coal mining. For drug overdose mortality, we find consistent evidence that declines in coal mining are associated with increases in drug overdose mortality and opioid overdose mortality. This finding is robust across multiple specifications and subsets of the data. We find limited evidence that coal mining has spatial spillover effects on mortality outcomes. However, we find that this result is sensitive to when the panel begins: if we start the panel in 2000, we observe declining coal mining increases drug overdose mortality, however, if we start the panel in 2006, we observe declining coal mining reduces drug overdose mortality likely explained by differential trends occurring concurrently with the opioid overdose crisis. We find limited evidence that unconventional drilling has a statistically meaningful effect on drug overdose mortality during the shale boom. Only in long-difference models do we find evidence that unconventional drilling can reduce the studied mortality outcomes. For non-drug overdose suicides and alcohol poisoning (other “Deaths of Despair”), we find suicide rates rise with decreasing coal mining and with increasing UOGD. These general findings are not necessarily consistent with a “Deaths of Despair” hypothesis. Following our main results, we examine the potential mechanisms behind our contrasting findings and examine alternative explanations behind our results (e.g., migration, population compositional changes, differences in opioid prescribing, regional differences). We find that the population dynamics, regional differences in boom-and-bust cycles, and the exponential increase in opioid overdose mortality in areas with resource extraction lead us to conclude a causal relationship is challenging to identify for opioid overdose mortality.
We estimate our models across various subgroups by age and race/ethnicity to investigate whether the impacts affect populations uniformly. We find some evidence that declines in coal mining are most associated with increased non-drug mortality and opioid overdose mortality for those population subgroups most likely to be employed by the coal industry. However, we find evidence that declines in coal mining are associated with declining mortality for younger males, a population that is highly-represented in the mining workforce. We do not document any substantial heterogeneity by population subgroups for shale development. We also find that the most intensively mined counties primarily drive the impacts of coal mining on mortality and substantial heterogeneity comparing Appalachian States to Rocky Mountain States.
We test the robustness of our main results in several ways. We evaluate our models with alternative sets of the data; alternative specifications; and alternative modeling frameworks (i.e., long-difference models). Our findings are robust to these checks. Additionally, we compare our results to Metcalf and Wang (2019), a recent paper that estimated the positive effects of the employment share in coal mining on opioid overdose mortality rates. Our estimated relationship contrasts with that found in their paper, and we replicated their results to understand the source of the seeming contradiction. We find evidence that the difference in results is due to the length of the panel: our model results square with their model results, and vice versa, if the models are subject to the same respective study periods.
Our paper contributes to a large and growing literature on the impacts of local economic conditions on mortality and the importance of place on life expectancy (Deryugina et al., 2019; Finkelstein, Gentzkow and Williams, 2019; Deryugina and Molitor, 2020). Resource extraction industries cannot exist everywhere due to geological conditions. Our results suggest that places that rely on resource extraction face large health shocks from the boom-and-bust cycles inherent in these industries. Additionally, we contribute to the extensive literature on “Deaths of Despair” by working to understand how resource-driven economic shocks impact total and drug overdose mortality. Our results suggest an economic story behind the drug overdose epidemic, contrary to recent research that suggests the main cause was an evolving drug environment (Currie and Schnell, 2018; Currie, Jin and Schnell, 2018; Currie and Schwandt, 2020). Our paper and its findings do not contradict this recent research. Instead, they suggest that the story is more complicated and involves economic malaise. Finally, our paper contributes to a growing literature assessing the local economic impacts on mortality when migration may influence measured mortality (Cutler, Huang and Lleras-Muney, 2016; Arthi, Beach and Hanlon, 2019; Finkelstein, Gentzkow and Williams, 2019).
Our paper also contributes to a vast literature on the local impacts of resource booms and busts on communities. Most health-related research in this space, however, focuses on the impacts of resource booms and busts on health through a pollution mechanism (Currie, Greenstone and Meckel, 2017; Hill, 2018; Black et al., 2021). In this paper, we take an alternative approach and consider the health effects that stem from the economic mechanism associated with these events. Evidence of links between the coal bust and shale boom and local drug use has largely been anecdotal (Horwitt, 2014). We contribute new empirical evidence of relationships between resource development and mortality.1
2. Background
In this section, we provide background on the opioid epidemic, shale boom and coal bust.
2.1. Background on Opioid Epidemic
We provide a more detailed history of the opioid epidemic in the Appendix. In Figure 1, we highlight trends in the number of total drug overdoses annually from 1999 to 2016. We separate drug overdoses that had at least some opioid involvement from those that had no opioid involvement. The number of both opioid and non-opioid overdoses has increased since 1999, though the rate of increase is substantially higher for opioid overdoses. We also highlight the number of overdoses with no identified drug as having caused the overdose. Between 1999 and 2016, ~22% of all drug overdoses (out of 632,331) did not have a classified drug. As others have noted (Ruhm, 2017; Buchanich et al., 2018; Boslett et al., 2019; Boslett, Denham and Hill, 2020), this data limitation has led to a significant underestimate of the scale of the opioid overdose epidemic. Boslett, Denham, and Hill (2020) estimate that almost 100,000 of these overdoses were opioid-involved (28% more than the reported level).
Figure 1:
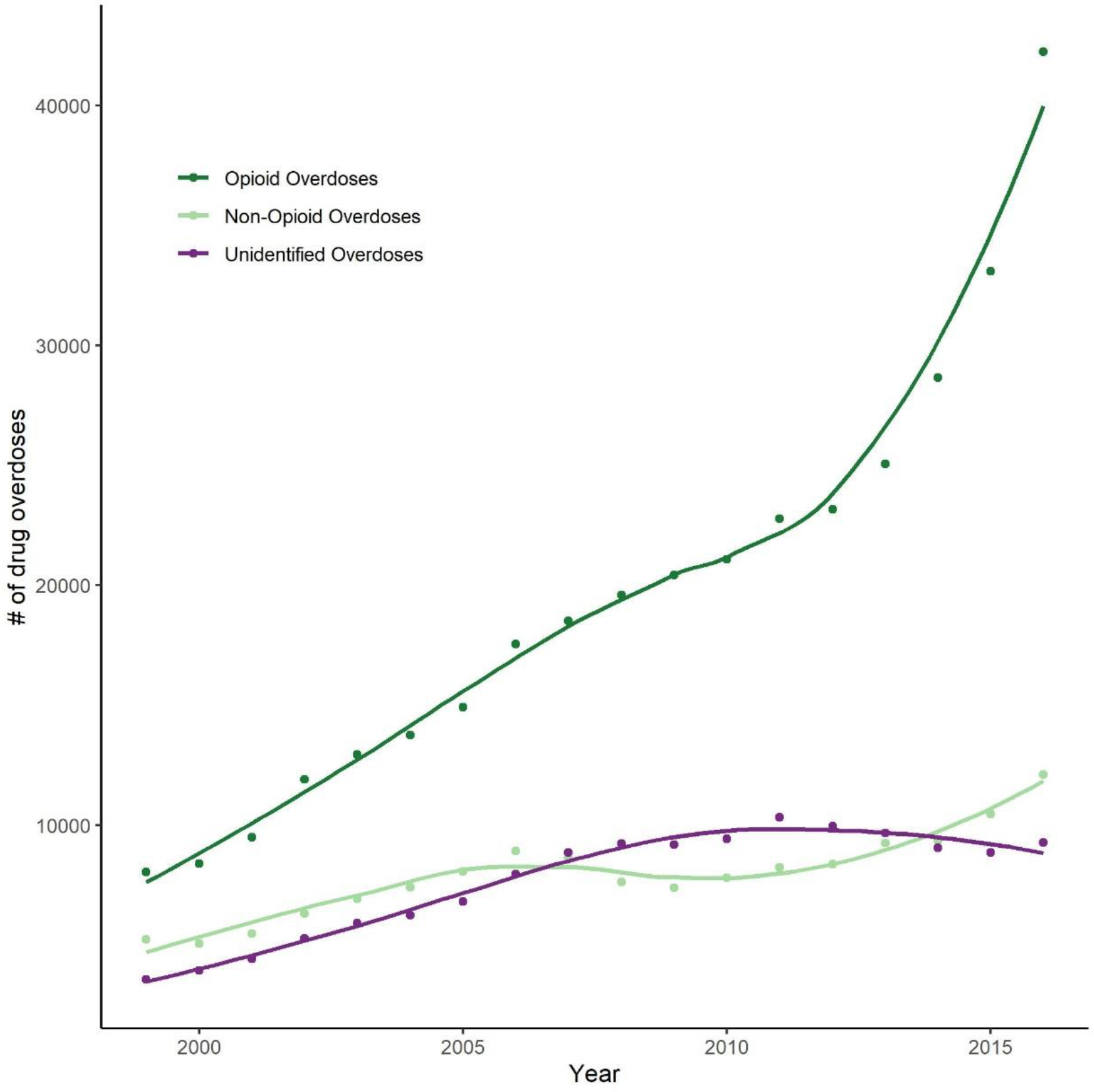
Number of drug overdoses from 1999 to 2016 in the United States
Notes: In this figure, we show the number of drug overdoses in the United States annually from 1999 to 2016 based on National Center for Health Statistics’ Multiple Cause of Death Data. We separate counts into mutually-exclusive bins: drug overdoses with a known opioid drug as having contributed to the overdose; drug overdoses with no specified opioid drug as having contributed to the overdose; and drug overdoses with no specific drug as having contributed to the overdose (i.e., only T50.9 is indicated in decedent’s list of contributing causes of death).
2.2. Background on the Shale Boom
The shale boom has led to a substantial increase in domestic oil and gas production. The boom was driven by a number of factors, including high resource prices, a series of policy initiatives that encouraged the development of “unconventional” oil and gas formations, and technological advancements in hydraulic fracturing and horizontal drilling (Wang and Krupnick, 2015). The shale boom has been a continental phenomenon, occurring in states across the country. Some of these regions have long histories of oil and natural gas production, including Colorado, Louisiana, and Texas. Others, including the Appalachian states of Ohio, Pennsylvania, and West Virginia, have comparatively short production histories. In Figure A1 in the Appendix, we show the extent of shale development in the continental U.S.
The impacts of the shale boom on local communities have been diverse. From an economic standpoint, the boom has led to increased employment and income (Agerton et al., 2017; Feyrer, Mansur and Sacerdote, 2017); royalty and lease signing bonus payments that annually number in the billions (Brown, Fitzgerald and Weber, 2016); reductions in disability insurance program payments (Charles, Li and Stephens, 2017); higher labor force participation rates (Hastings, Heller and Stephenson, 2017); and spillovers into other sectors in non-metro areas (Tsvetkova and Partridge, 2016). There is also evidence that the economic returns are greatest for those with lower human capital (Rickman, Wang and Winters, 2017); this population has experienced long-term declines in job opportunities (Autor, Levy and Murnane, 2003) and has been highly affected by drug abuse (Clarke et al., 2014; Case and Deaton, 2015). There are also concerns that the recent oil and gas boom has led to increases in crime (James and Smith, 2017; Gourley and Madonia, 2018; Komarek, 2018), prostitution (Ruddell, 2017), and sexually-transmitted disease rates (Komarek and Cseh, 2017; Beleche and Cintina, 2018). There are a number of concerns regarding environmental impacts, especially air (Litovitz et al., 2013) and water pollution (Osborn et al., 2011; Olmstead et al., 2013; Hill and Ma, 2017), and related public health effects (Currie, Greenstone and Meckel, 2017; McKenzie et al., 2017; Hill, 2018; Peng, Meyerhoefer and Chou, 2018). See a new review on the health, environmental and economic impacts of unconventional oil and gas development for more details (Black et al., 2020).
2.3. Background on the Coal Bust
Concurrent with the rise of shale development, nationwide coal production declined by more than 30% from 2000 to 2017. What production has remained is at far fewer operating mines, which have declined in number from 1,329 in 2000 to 639 in 2016 (calculations based on U.S. Mine Safety and Health Administration (MSHA) data).2 These declines have been most substantial for the Appalachian region of the United States, which have also suffered from declining employment at those mines that remain in operation. This is evident in Figure 2, which highlights the decline in operating coal mines in Appalachia between 2000 and 2016.3 Appalachian coal production and reserves are bituminous in rank, which is higher in sulfur compared to sub-bituminous coal basins in the western United States. This has left Appalachian coal production exposed to environmental regulations that have limited sulfur emissions from coal-fired power plants (U.S. Energy Information Administration, 1997; Hower, Robl and Thomas, 1999). Bituminous coal does have a higher energy content (11,000–15,000 Btu/pound) than sub-bituminous coal (8,500–13,000 Btu/pound), though bituminous coal is more difficult and expensive to extract; average production per employee is ~83% lower in Appalachia than it is in the western states.4 This is partly driven by the higher proportion of western U.S. coal production that occurs at surface mines, which have lower production costs (Ellerman et al., 2000).
Figure 2:
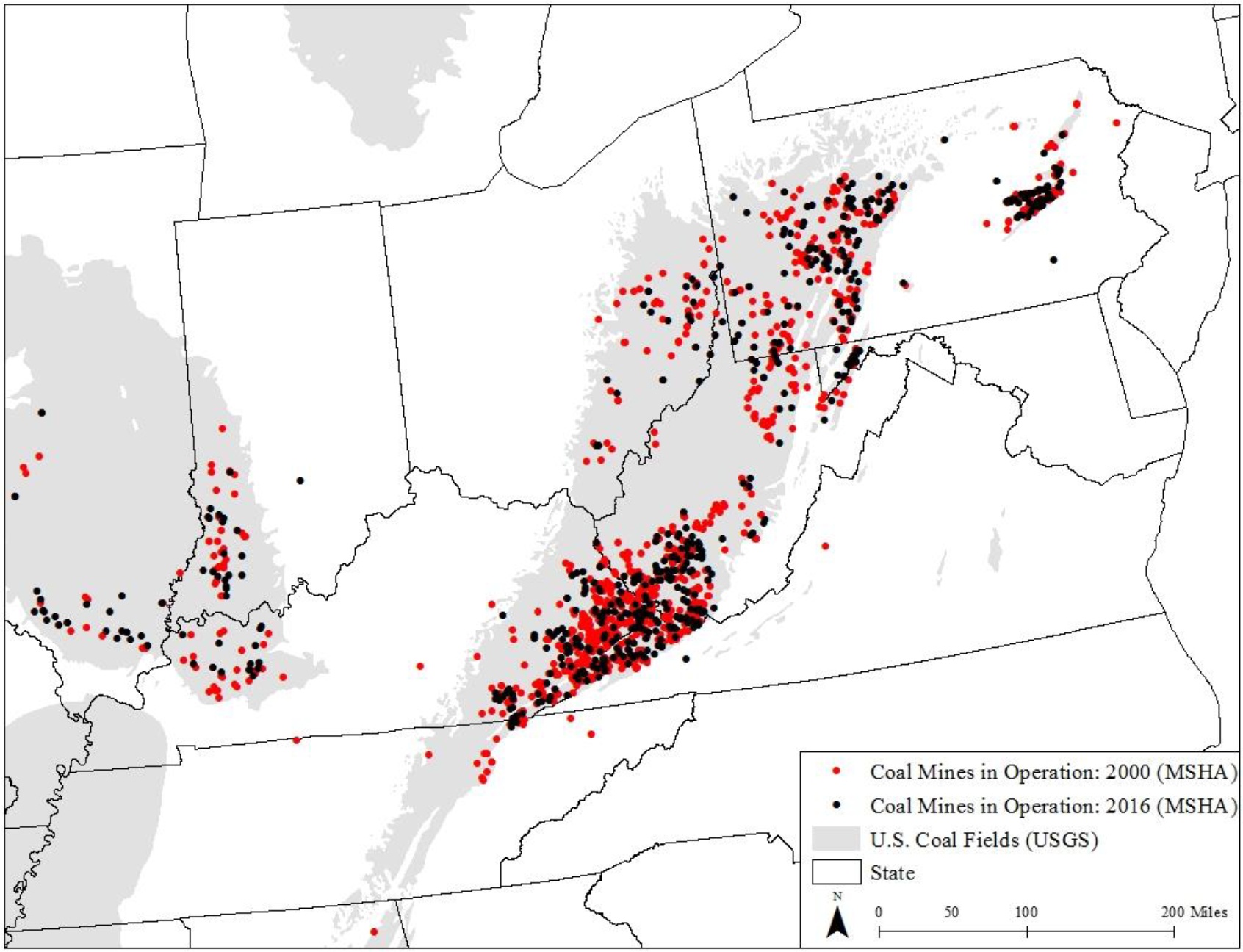
Coal mines in operation in 2000 and 2016 in Appalachia
Notes: In this figure, we show the locations of operating coal mines in the Appalachian region of the United States in 2000 and 2016. Mine location and production data are from the U.S. Mine Safety and Health Administration. Coal field boundaries are from the U.S. Geological Survey.
There is a rich literature describing recent trends in socio-economic dynamics related to the shale oil and gas boom, but there are relatively few studies on the same dynamics for the recent coal bust (Betz et al., 2015). Using data from 2010–2016, Weber (2019) estimates that each lost coal mining job is associated with a decline in county income by almost $100,000, and that a third of those who lost employment stayed in the county and remained unemployed. Historical coal busts have been associated with greater participation in disability programs (Black, Daniel and Sanders, 2002), welfare programs (Black, McKinnish and Sanders, 2003), and declines in earnings and employment in both the mining and non-mining sector (Black, McKinnish and Sanders, 2005).
2.4. Related Studies
There is a concurrent study focusing on the impact of the coal bust on opioid mortality. Metcalf and Wang (2019) find a positive relationship between the share of coal miners in the local labor force and county-level opioid overdose rates. See our discussion section for a detailed comparison of our findings with theirs.
Another related research area focuses on the impacts of shale development on various aspects of risky behavior (Komarek and Cseh, 2017; Beleche and Cintina, 2018; Cunningham, DeAngelo and Smith, 2020; Johnson et al., 2020). Most of this literature has focused on the rise in sexually-transmitted diseases in areas with shale development. If choices regarding whether to partake in risky sexual behavior co-occur with those associated with selection into drug abuse, then it is possible that shale development may lead to increases in drug abuse (and later mortality).
3. Conceptual Framework
In this study, we examine whether the coal bust and shale boom are associated with changes in non-drug mortality and opioid overdose mortality. This section briefly describes our conceptual frameworks that explain why local economic conditions are likely to impact mortality by these causes. We argue that the relationships are functions of the direction and strength of multiple mechanisms.
3.1. Non-drug mortality
Our conceptual framework for non-drug mortality is described in detail in prior literature (Cutler, Huang and Lleras-Muney, 2016; Lleras-Muney and Moreau, 2020). Short-term effects of economic conditions on mortality are ambiguous and suggest that this is inherently an empirical question. Long-term effects are also ambiguous in sign due to previous economic conditions impacting prior health investments as well as current investments, and these impacts depend on critical windows of development. Mortality in previous periods can result in selection effects that are also ambiguous in sign (Cutler, Huang and Lleras-Muney, 2016). These selection effects determine which individuals are at the threshold of surviving and are at risk for mortality. A negative investment, therefore, results in fewer individuals around the threshold of surviving, which lowers mortality in the next period. Negative investments, however, decrease the health stock of the entire population, which may increase the number of individuals at the threshold in the next period. In our study, we might expect regions with coal mining to have experienced investments during the coal boom such that the health stock is improved at the beginning of the coal bust, potentially protecting them from the loss.
Recent literature has found large migration responses to shale gas development, particularly in North Dakota and to a lesser extent Pennsylvania (Wilson, 2020). Those most likely to move into and out of fracking areas are male, younger workers, unmarried, and either be a high school dropout or college graduate. The author concludes that this migration is due to increased churn that is short-term with limited evidence that certain demographic groups are systematically sorting away or towards fracking areas (Wilson, 2020). The net migration effect, however, is positive, which may influence our estimates. Furthermore, younger individuals tend to be healthier and are less susceptible to mortality.
3.2. Opioid Overdose Mortality
The shale boom and coal bust have had impacts on local economic conditions. Economic upturns and downtowns can influence opioid abuse through the following demand-side mechanisms. First, the opportunity cost of one’s time increases during economic upturns (Ruhm, 2000). Time availability for recreational pursuits decreases when one is working more hours and it increases during economic downturns, when layoffs and cuts in available working hours provide past employees with more time to pursue non-work activities. Second, one’s personal fulfillment and happiness may improve when one believes he or she is contributing to a broader purpose through work. After a job loss, one may feel depressed about their declining work-based contribution to society (Clark and Oswald, 1994) and this lack of fulfillment may, in turn, lead to drug abuse (Nagelhout et al., 2017). Third, exposure to stress – whether it’s from a job loss or overwhelming job demands – may encourage people to abuse drugs, including opioids (Sinha, 2008). The direction of this mechanism on opioid abuse is unclear a priori. Fourth, opioid-based medications have been increasingly supplied for pain management. If pain-causing workplace injuries increase with an improving economy (Catalano, 1979), then opioid prescriptions (and potential subsequent abuse) may be countercyclical. This mechanism is especially likely to be relevant in resource-fueled economies where workers may face high levels of occupational injuries and fatalities (Reardon, 1993; Guo et al., 1999; Witter et al., 2014). Fifth, economic downturns may lead to improved social behavior (e.g., declines in opioid abuse) if people are more concerned about keeping or obtaining a job (Catalano, Novaco and McConnell, 2002). Lastly, economic upturns may lead to lower drug use if employment is conditional on drug testing.
Resource-driven economic upturns and downturns can also influence opioid abuse through the following supply-side mechanisms. First, in times of economic stress, more people may be inclined to join the illicit drug market and become drug dealers to sell their own or an acquaintance’s prescribed opioids (Carpenter, McClellan and Rees, 2017). Local economic distress may also encourage less than scrupulous doctors and drug wholesalers to inject opioids into the community. Second, economic conditions may impact the level of local healthcare available. This can be measured in multiple ways. The level of health care infrastructure, such as the number of local hospitals and primary care facilities, may increase during times of economic growth. There is also growing evidence that the health insurance quality decreases during economic recessions, especially in the hardest-hit sectors (Koh, 2018). If improving infrastructure and insurance includes greater capacity to control or prevent local opioid abuse, then drug abuse and related mortality may be countercyclical. Lastly, economic upturns may lead to greater enforcement of drug abuse if tax revenue is diverted for prescription opioid sale deterrence (Carpenter, McClellan and Rees, 2017).
The shale boom and coal bust may have influenced drug abuse through their impacts on the local makeup of the population due to in- and out- migration (Wilson, 2020, 2021). This is potentially important, as there is evidence in the literature that certain subpopulations are more susceptible than others to drug abuse. During the recent opioid epidemic, white men and women have been particularly susceptible to opioid abuse, many of whom were introduced to opioids through medical care (Rosenblum et al., 2007; Cicero et al., 2014). There is growing evidence that minority groups are less susceptible to opioid abuse (Palamar et al., 2016), perhaps as a result of differential prescription rates for pain management (Pletcher et al., 2008).5 These changes in population are potentially a threat to our identification strategy. To circumvent this threat, we test for changes in population, run subgroup analyses, and control for population characteristics in our regression models.
Lastly, there may be differences between the shale boom and coal bust in how these industries are employed and whether the employees come from the local community. This transience, most studied in the context of shale development, may influence the take-up of risky behaviors in a community. A few studies have found a relationship between the shale boom and sexually-transmitted disease prevalence as well as prostitution (Beleche and Cintina, 2018; Cunningham, DeAngelo and Smith, 2020; Johnson et al., 2020). These papers argue that “man-camps” housing workers in the oil and gas industry increase risk-taking activity in the community and change sex-ratios due to male workers migrating into an area to work in the industry. If opioid use is one of these many risky behaviors, we would expect to see higher levels of opioid misuse related to the shale boom. If coal mining, and especially the closure of coal mines, is less likely to influence risky behaviors or more likely to reduce risky behaviors due to the employees being members of their community in which they work and live, then we would not expect coal mining to be associated with risky behaviors.
4. Data
5.1. Multiple Cause of Death Data and other drug-related data sources
We received restricted access to the National Vital Statistics System (NVSS) Multiple Cause of Death Data from 1999 to 2016 for this study. This database contains data on the underlying causes of death (UCOD) and demographic information for the universe of deaths in the United States. The database is available on an annual basis and is maintained by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). We received protected versions of the data that contain decedent residence and place-of-death at the county level.
We identified all drug overdose deaths using UCOD codes X40–44 (unintentional poisoning), X60–64 (self-harm/suicide-related poisoning), X85 (assault/homicide-related poisoning), and Y10–14 (poisoning with unclear intent), following Center for Disease Control guidelines. To identify opioid-involved drug overdoses, we used ICD-10 UCOD codes T40.0 (opium), T40.1 (heroin), T40.2 (other opioids), T40.3 (methadone), T40.4 (other synthetic narcotics), and T40.6 (unspecified narcotics). In addition to studying drug overdose deaths, we report total all-cause mortality and non-drug mortality defined as all-cause mortality removing drug overdose deaths.
More than a fifth of all drug overdoses from 2000 to 2016 did not include a classified drug, but instead included the ICD-10 cause-of-death code T50.9 (i.e., Poisoning by, adverse effect of and underdosing of other and unspecified drugs, medicaments and biological substances). There is significant within and between-state variation in the level of underreporting (Warner et al., 2013; Ruhm, 2017; Boslett et al., 2019). There have been a number of approaches used to predict and impute opioid involvement in these unclassified overdoses (Ruhm, 2017; Buchanich et al., 2018; Boslett, Denham and Hill, 2020). Following Boslett, Denham, and Hill (2020), we estimate year-by-year logistic regression models of opioid involvement in unclassified overdoses using binary indicators of contributing causes of death, and then use model predictions to generate corrected county-level opioid overdose rates over time. We provide more information about this procedure in the Section B of the Appendix.
5.2. Other health-related data
We extracted annual, county-level historical data on the numbers of total hospitals and pharmacies from Area Health Resource Files from the U.S. Department of Health and Human Services’ Health Resources & Services Administration (HRSA). We obtained county-level opioid prescribing rates per 100 people from 2006 to 2016 from the CDC. Unfortunately, these data are not available prior to 2006. We obtained and cleaned annual Automated Reports and Consolidated Ordering System (ARCOS) data from the U.S. Department of Justice’s Drug Enforcement Administration (DEA). Available from 2000 to 2016, these databases provide estimates of the level of retail drug prescribing by weight in grams across a variety of different drug types. These data are available annually at the 3-digit zip code-level. We used a crosswalk between 3 and 5-digit zip codes to estimate the total weight of ARCOS-subjected drugs and opioid drugs in grams at the 5-digit zip code-level. We then aggregated these estimates to the county-level based on a population crosswalk between 5-digit zip codes and counties. We developed a database of different policies that may have an effect on local overdose rates by state and year, including a Good Samaritan Law, Naloxone Access Law, and civil and criminal immunity in the use of Naloxone (Rees et al., 2017). Given evidence that drug overdose rates are lower in states with triplicate prescription programs (Alpert et al., 2019), we generated a binary variable equal to 1 if the state passed a triplicate prescription program.
5.3. Resource Production and Geology Data
We obtained mine-level coal production data from the Mine Safety and Health Administration (MSHA). These databases include information on annual and quarterly production, employment, inspections, and violations at the mine-level. This database also includes information on the type of mine (e.g., surface versus underground) and its location. Using these data, we estimated annual production, employment, and the number of operating mines to the county-level.
Additionally, we received academic access to oil and gas drilling databases from Enverus/Drillinginfo, a data provider for the oil and gas industry. We estimated the number of horizontal oil and gas wells drilled annually from 2000 to 2016 at the county-level using each well’s coordinates and spud date, which is the date when a well is first drilled into the surface of the well pad.
We estimated county-level coverage of shale and coal resources using multiple databases. First, we calculated county-level shale play coverage using a shapefile of shale oil and gas play boundaries from the U.S. EIA (Tight Oil and Shale Gas Plays). Following, we estimated county-level coal coverage using coal field boundary data from the U.S. Geological Survey (Coal Fields of Conterminous United States ArcInfo files).
5.4. Socio-economic and demographic data
To understand dynamics in local economic conditions across time and space, we obtained median household income and poverty estimates at the county-level from 2000 to 2016 from the Small Area Income and Poverty Estimates (SAIPE) Program. We also obtained labor force participation and employment dynamics from the Quarterly Census of Employment and Wages. We obtained both overall employment and mining-specific (NAICS 2111) estimates of the number of employees in the county. We also estimated the total number of employees working at coal mines using MSHA databases, as described above.
For county-level demographic estimates, we obtained Survey of Epidemiology and End Results (SEER) U.S. county-population data from the National Bureau of Economic Research’s databases. We estimated total population, median age, and population in three race groups (i.e., White, Black, and Other Race) on an annual basis across time. We obtained U.S. Census Bureau county-level educational attainment data from the 2000 decennial census and the 2012–2016 5-year American Community Survey (from the U.S. Department of Agriculture’s Economic Research Service’s data products).
5. Empirical Methods
In this paper, we examine the impact of coal, oil, and natural gas extraction on local non-drug all-drug and opioid overdose mortality using two-way fixed effects models. Our baseline model is (1):
| (1) |
The dependent variable, MortalityRateit, is measured in multiple ways: total all-cause mortality, non-drug mortality, working age non-drug mortality, drug overdose mortality or opioid overdose mortality for county i in year t. All outcome variables are measured in rates per 100,000 people. We also estimate models for non-drug suicides and alcohol poisonings. Our explanatory variables of interest are Resourceit and NearbyResourceit, which are measures of coal mining or oil and natural gas drilling activity in county i in year t and in nearby counties of i within different distance bands, respectively. We primarily measure these variable in two ways: the number of operating coal mines (tens of mines) and the number of horizontal oil and gas wells spudded (hundreds of wells) in the given county-year. In both cases, β1 and β2 reflect the per-unit effects of coal, natural gas, or oil operations on local levels of non-drug and drug overdose mortality. We include county fixed effects, γ1, to control for unobserved, time-invariant heterogeneity across the country, and year fixed effects, τ1, to control for aggregate trends in drug overdose mortality across time. We also control for an interaction between the county’s initial mortality rate with a vector of year indicators (MortalityRatei,2000 · τt) to control for pre-coal bust and pre-shale boom differences in local mortality rates. Our preferred models are unconditioned beyond these factors. Many other potential explanatory variables, measured at the unit-level over time could be endogenous to resource development. Standard errors are clustered at the county-level. We also estimate models with these endogenous factors as outcomes to understand how they change with resource extraction (Pei, Pischke and Schwandt, 2019).
We extend this baseline model by adding state-by-year fixed effects. Given the fairly long period that we study, these state-by-year fixed effects control for unobserved factors that are changing at the state-level over time, in particular policies or state-specific shocks that may affect mortality in year t. We present models with and without state-by-year fixed effects but generally focus on models with these fixed effects included.
In robustness checks for total all-cause and non-drug mortality, we control for a vector of time-varying control variables, that are commonly included in models assessing the effects of economic conditions on total all-cause mortality (Ruhm, 2000, 2015, 2016; Heutel and Ruhm, 2016). These include the shares of the county population who are white, Hispanic, and working-aged (25–64 years old); total population; and the total number of hospitals and pharmacies in the county.
In robustness checks for drug overdose and opioid overdose mortality, we also control for a vector time-varying control variable, , including total population; shares of the county population who are white, Hispanic, and working-aged (25–64 years old); the total number of hospitals and pharmacies in the county; and the level of retail drug distribution of opioid drugs (in grams). We control for a series of binary variables indicating whether each county’s state government has passed either a Good Samaritan Law, Naloxone Access Program, or granted civil or criminal immunity in Naloxone administration.
We estimate our models nationally throughout the main paper and provide estimates for two regions in the Appendix (Appalachian region and northern Rocky Mountain states separately). For all, we focus on models of counties within 100 miles of both shale and coal basins. The literature has suggested that the economic benefits of UOGD may persist up to 40 miles (James and Smith, 2020).
6. Results
In this section, we describe the main results of our paper. We start with a description of summary statistics in our sample and then describe the results of first-stage models of resource development on economic outcomes. We then describe our main non-drug mortality and drug overdose mortality results.
6.1. Summary statistics
In Table 1, we provide summary statistics of drug overdose-related outcome variables for the restricted sample (within 100 miles of a coal basin or shale play). We highlight means of variables across mutually-exclusive groups defined by shale and coal resource availability: (1) counties with no shale or coal resources, and (2) counties that overlay both shale and coal basins. We chose these two types of groups because we restrict our sample in our preferred analyses to those within both a shale play and a coal basin or within a 100-mile buffer of both types of resources for a cleaner control and treatment group split. The make-up of these groups is time-invariant because they are based on geological availability and not resource production. We estimate means in 2000, which is prior to both the shale boom and the coal bust, and in 2016, which is post-coal bust and at a time of high production of both oil and gas. Drug overdose and non-drug mortality rates are generally higher in counties with shale and coal resources and these differences are evident before and after the boom and bust.
Table 1:
Summary statistics for unrestricted sample, 2000 and 2016
| No Coal/Shale | Both Coal/Shale | Coal Only | Shale Only | |||||
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| 2000 | 2016 | 2000 | 2016 | 2000 | 2016 | 2000 | 2016 | |
|
| ||||||||
| Total Mortality | 990.18 | 1042.43 | 1060.77 | 1114.96 | 1054.95 | 1113.04 | 944.97 | 1010.48 |
| Working-Aged Mortality | 395.51 | 471.89 | 428.91 | 523.17 | 446.58 | 547.73 | 386.12 | 464.25 |
| Senior Mortality | 5357.34 | 4356 | 5463.13 | 4528.27 | 5491.27 | 4532.52 | 5197.07 | 4307.02 |
| Total Drug Overdose | 4.64 | 20.14 | 4.89 | 20.63 | 4.1 | 14.18 | 4.54 | 17.96 |
| Known Opioid Overdose | 1.92 | 13.39 | 1.81 | 12.5 | 1.29 | 7.1 | 1.57 | 10.58 |
| Estimated Opioid | 2.79 | 15.85 | 2.78 | 15.47 | 2.08 | 9.65 | 2.34 | 13.23 |
| Alcohol Overdose | 0.16 | 0.72 | 0.11 | 0.75 | 0.14 | 1.09 | 0.08 | 0.57 |
| Suicide | 12.68 | 16.92 | 13.77 | 18.81 | 13.42 | 18.36 | 11.01 | 18.81 |
| # of coal mines | 0 | 0 | 2.45 | 1.14 | 0.13 | 0.08 | 0 | 0 |
| # of coal mines | X > 0 | 0 | 0 | 8.07 | 4.8 | 1.4 | 1.81 | 0 | 0 |
| # of horizontal wells | 0 | 0 | 0.4 | 6.67 | 0 | 0 | 0.63 | 14.58 |
| # of horizontal wells | X > 0 | 0 | 0 | 3.55 | 31.4 | 0 | 0 | 4.93 | 75.83 |
| # of observations | 736 | 513 | 489 | 194 | ||||
|
| ||||||||
| All counties in region <= 100 miles from shale/coal basins | X | X | X | X | X | X | X | X |
Notes: In this table, we display county means of mortality rates by whether the county is above no shale and coal resources; both types of resources; only coal resources; and only shale resources. All mortality rates are unadjusted for age and are measured per 100,000 people. County population values are from SEER population data.
6.2. Resource development and economic conditions
Our conceptual framework relies on an interpretation of resource booms and busts as economic phenomena. In Table 2, we estimate the relationship between resource development and economic conditions, as measured by county-level median household income, poverty rate, unemployment rate, and the level of disability payments made to workers. We include both forms of resource development in the same model. We show estimates of models with and without state-by-year fixed effects. We find support for our argument that coal mining and horizontal well development are associated with improved contemporaneous economic indicators. We observe that both forms of resource development are associated with higher income, lower poverty rates, and lower unemployment. These effects are statistically significant for both forms of resource development. We observe no evidence that either form of resource development has a significant effect on the amount of disability payments made to workers. Overall, our first-stage results support our conceptual framework of resource booms and busts as economic phenomena.
Table 2:
The relationship between resource development and economic conditions
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| Median Household Income | Poverty Rate | Unemployment Rate | Disability Payments to Workers | |||||
|
| ||||||||
| # of operating coal mines (in 10s) | 998.2*** (137.8) | 587.4*** (129.8) | −0.577*** (0.147) | −0.423***(0.130) | −1.040*** (0.145) | −0.944*** (0.133) | 151.4 (99.09) | 54.33 (109.9) |
| # of horizontal oil and gas wells (in 100s) | 17.65*** (4.223) | 13.53*** (3.101) | −0.00743*** (0.00168) | −0.00435*** (0.00105) | −0.00397*** (0.000995) | −0.00235*** (0.000592) | 0.102 (0.939) | 0.213 (0.772) |
| # of observations | 53,365 | 53,365 | 53,367 | 53,367 | 53,299 | 53,299 | 52,497 | 52,497 |
| R-squared | 0.958 | 0.971 | 0.939 | 0.954 | 0.842 | 0.923 | 0.925 | 0.936 |
|
| ||||||||
| State*Year FE | NO | YES | NO | YES | NO | YES | NO | YES |
| County FE | YES | YES | YES | YES | YES | YES | YES | YES |
| Year FE | YES | YES | YES | YES | YES | YES | YES | YES |
Notes: In this table, we highlight estimates of the effects of resource development on economic outcomes, including median household income and the poverty rate, both from Small Area Income and Poverty Estimation (U.S. Census Bureau); the unemployment rate from the Local Area Unemployment Statistics (Bureau of Labor Statistics); and disability payments made to workers in $1,000s (from the Social Security Administration). We include year fixed effects and county fixed effects. Statistical significance: 1% level, ***; l5% level, **; and 10% level, *.
6.3. The impact of resource development on mortality
In this section, we outline the main results of our paper: the estimated effects of coal mining and unconventional oil and gas development (UOGD) on non-drug mortality and drug overdose mortality. Despite the prior literature examining overall mortality using total all-cause mortality, we are limiting to non-drug mortality because there are exponential increases in drug overdose mortality during our study period. Our two main treatment variables are the number of operating coal mines (tens of mines) and the number of horizontal oil and gas wells spudded (hundreds of wells) in the given county-year. We additionally control for the number of coal mines and shale wells within a buffer from 0 < X ≤ 25 miles away from the county and a ring from 25 < X ≤ 50 miles away from the county to assess spatial spillovers.
In Table 3, we explore whether coal mining and UOGD influence overall non-drug mortality rates and drug overdose mortality rates in the U.S. (measured in rates per 100,000 people). In Columns 1–4, we focus on non-drug mortality results, including total non-drug mortality (Columns 1–2) and working-age (18–64 year olds) non-drug mortality (Columns 3–4). In Columns 5–8, we show results for drug overdose mortality (Columns 5–6) and opioid overdose mortality (Columns 7–8). Our observation set includes those counties within 100 miles of a shale or coal basin to reduce the potential for unobserved factors to influence our estimate. We estimate models with and without state-by-year fixed effects.
Table 3:
The relationship between resource development and non-drug mortality rates and drug overdose mortality rates
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| Non-drug Mortality | Working-Age Non-Drug Mortality | Drug Overdose Mortality | Opioid Overdose Mortality | |||||
|
| ||||||||
| # of operating coal mines (in 10s) | −29.87*** (6.886) | −18.36*** (6.746) | −25.82*** (7.091) | −22.12*** (7.200) | −3.078** (1.195) | −1.339 (0.918) | −2.856*** (1.067) | −1.177 (0.801) |
| # of horizontal O&G wells (in 100s) | −10.99 (6.781) | −7.326 (5.452) | −0.832 (1.848) | −1.139 (1.788) | 0.113 (0.236) | 0.360 (0.280) | −0.0146 (0.172) | 0.244 (0.198) |
| # of operating coal mines (in 10s), 0 < X ≤ 25 miles | −1.858 (2.800) | −5.434* (2.880) | −1.773 (2.051) | −4.487** (2.113) | 0.314 (0.403) | 0.281 (0.427) | 0.247 (0.365) | 0.289 (0.383) |
| # of operating coal mines (in 10s), 25 < X ≤ 50 miles | −2.869 (2.033) | −1.876 (2.063) | −2.047 (1.576) | −2.154 (1.623) | 0.155 (0.247) | 0.207 (0.269) | 0.114 (0.224) | 0.212 (0.238) |
| # of horizontal O&G wells (in 100s), 0 < X ≤ 25 miles | −0.919 (1.352) | −1.323 (1.230) | 2.003 (1.748) | 1.967 (1.720) | 0.141 (0.0916) | 0.144 (0.0909) | 0.0992 (0.0680) | 0.0975 (0.0662) |
| # of horizontal O&G wells (in 100s), 25 < X ≤ 50 miles | −3.668*** (0.971) | −1.499 (0.949) | −1.230 (0.815) | −0.624 (0.852) | −0.214*** (0.0587) | −0.192*** (0.0630) | −0.171*** (0.0456) | −0.120** (0.0488) |
|
| ||||||||
| # of observations | 32,752 | 32,684 | 32,752 | 32,684 | 32,844 | 32,776 | 32,844 | 32,776 |
| R-squared | 0.848 | 0.856 | 0.692 | 0.704 | 0.438 | 0.478 | 0.458 | 0.509 |
| State*Year FE | NO | YES | NO | YES | NO | YES | NO | YES |
| US counties <= 100 miles from shale/coal basins | YES | YES | YES | YES | YES | YES | YES | YES |
Notes: In this table, we highlight estimates of our baseline model (1) and model (2) including state-by-year FE. All outcomes are death rates per 100,000. In Columns 1–2, the death rate is for total mortality for all people, irrespective of age. In Column 3–4, the outcome variable is the mortality rate of individuals aged 25–65 years old. In Columns 5–6, our outcome variable is the drug overdose rate. In Columns 7–8, our outcome variable is the opioid overdose rate with corrections used based on models discussed in Boslett, Denham, and Hill (2019). All models include county fixed effects, year fixed effects, and interactions between a year vector and the initial mortality rate to control for pre-coal bust and pre-shale boom differences in mortality rates. Statistical significance: 1% level, ***; 5% level, **; and 10% level, *.
We observe strong evidence that declines in coal mining are associated with increases in total non-drug mortality rates, though we find no significant evidence of a relationship between UOGD and these outcomes. These results appear to be driven by working-age mortality. For coal mining, we observe some evidence of spillover effects within 25 miles, though these effects are limited to non-drug mortality and working-age mortality.. We observe evidence that UOGD in a 25 < X ≤ 50 miles ring of a county is associated with significant declines in total non-drug mortality, though we observe no evidence of a significant relationship in the interior buffer. Our results also suggest that declines in coal mining led to increases in drug overdose and opioid overdose mortality, though these results are attenuated and not statistically significant with state-by-year fixed effects. We again observe no statistically significant effect of UOGD on drug overdose and opioid overdose mortality, with meaningful effects only found in the spillover region of 25 < X ≤ 50 miles away from the county.
7. Robustness and Extensions
In this section, we evaluate the potential drivers of the results shown in Table 3 and provide robustness checks for our main results. In our conceptual framework, we hypothesized that the impacts of resource development on mortality rates through the economic mechanism would be similar across the two types of resource development. Yet, coal mining is associated with declines in drug overdose mortality on a consistent basis, while horizontal oil and gas well development generally has no effect on mortality. In this section, we evaluate several potential factors that could drive these findings such as population change, heterogeneity by demographics, regional differences, and resource extraction intensity. We also compare our results to the existing literature and discuss magnitudes of our findings.
7.1. Robustness checks
In this section, we describe a series of robustness checks undertaken to understand the robustness of the results shown in Table 3. We separate our robustness checks into two main categories. First, we evaluate the robustness of our results in Table 3 to alternative sets of observations in Table A1 of the Appendix. In Column 1, we evaluate our models on all observations in the U.S., dropping our restriction that all observations must be within 100 miles of a shale play and coal basin. In Column 2, we focus on all rural counties in the U.S., hypothesizing that these counties will be most affected by resource development. In Column 3, we focus on rural counties but maintain the 100-mile distance restriction applied in Table 3. In Column 4, we evaluate the robustness of our models without 2015–2016 data. In these years, there was a substantial decline in the level of UOGD in the U.S. (see Figure A4 in the Appendix). We drop these periods to see how robust our results are to the exclusion of these “shale bust” years. We generally observe the same overall results as those shown in Table 3 across these robustness checks. Declining coal mining is associated with increases in total non-drug mortality, working-age non-drug mortality, and overall and opioid-specific drug overdose mortality. We continue to observe no significant effects of UOGD on any of the considered mortality outcomes
In Table A2, we evaluate the robustness of our results with alternative specifications. In Column 1, we drop the interaction between the initial mortality rate in 2000 and year vector. In Columns 2 through 4, we add additional control variables. We start in Column 2 with the additional of population characteristics to control for the fact that populations are dynamic. We note that these variables are potential endogenous due to that fact that resource development may lead to in-migration and out-migration. We discuss this potential factor in the conceptual framework. In Column 3, we add the numbers of pharmacies and hospitals as control variables. In Column 4, we add state-level indicators of a number of drug overdose-related policies (e.g., a Naloxone access program). We only estimate this model specification using drug overdose and opioid overdose mortality rates as outcomes. Our results are robust to these alternative specifications (Table A2). We continue to find evidence that declining coal mining is associated with increases in non-drug mortality and drug overdose mortality. We also continue to find limited evidence that UOGD significantly impacts mortality.
We also test the robustness of our models in other ways. We test the robustness of our opioid overdose mortality results by using opioid overdose rates calculated based on only those opioid overdoses that were classified (i.e., known opioid overdoses) in the death record (Table A3). We find the same relationships as those found in Table 3 though the effects are attenuated. We highlight the importance of making corrections to the opioid overdose record to account for probable opioid overdoses that were explicitly classified in the death record (Boslett, Denham and Hill, 2020). In particular, the authors found that Pennsylvania was in the top-5 states with unclassified overdose rates, which is one of the states with the highest degree of both UOGD and coal mining in the country.
In a similar vein as Table A3, we estimate our models with all-cause mortality and working-age all-cause mortality rates in Table A4. These rates include both non-drug mortality and drug overdose mortality. These results support our main findings.
In recent work, Ruhm (2019) finds evidence that drug overdose rates are weakly affected by local economic conditions and strongly associated with evolving characteristics of the local drug environment. Given the fact that the drug overdose epidemic started in the 1990s, it is also possible that certain areas have higher drug abuse and overdose rates prior to either the shale boom or coal bust. In Appendix Table A5, we examine whether the results found so far are robust to dropping counties that are on the higher end of the distribution of pre-shale boom and coal bust opioid prescription levels and find consistent results to Table 3.
We also test the robustness of our results using alternative methodological approaches. In Appendix Tables A7–10, we evaluate our models using a long-difference approach:
| (2) |
6 In Model (2), we model the difference in mortality rates between two years, one in the pre-shale boom and coal bust period and one in a post-shale boom and coal bust period as a function of the change in resource development levels between the same years. We include state fixed effects, ϑs. We estimate these models using various sets of years. For the pre-shale boom and coal bust period, we use year increments from 2000 to 2006. For the post-shale boom and coal bust period, we use year increments from 2010 to 2016. We include both forms of resource development in the model, as we have done throughout the paper so far.
In Tables A7–10, we show our model results for both forms of resource development for each one of our main outcomes (non-drug mortality, working-age mortality, drug overdose mortality, and opioid overdose mortality, in order). In Panel A, we show the parameter estimates for the change in coal mining from the post-vs-pre period. In Panel B, we show the parameter estimates for the change in UOGD from the post-vs-pre period. Overall, we find statistically significant (strong) evidence that declining coal mining increases non-drug mortality and shale boom is associated with declining total non-drug mortality; strong evidence that declining coal mining is associated with increasing working-age non-drug mortality and moderate evidence that UOGD is associated with declining working-age non-drug mortality; strong evidence that declining coal mining is associated with increasing drug overdose mortality and opioid overdose mortality; and weak evidence that UOGD is associated with declining drug overdose mortality and opioid overdose mortality. Overall, results from this alternative model specification are supportive of our results shown in Table 3.
7.2. Are the non-drug overdose and drug overdose mortality effects of resource development heterogeneous across sub-populations?
If there is an economic mechanism behind resource development and mortality, we would expect that resource development would have the largest effects for those populations that are most directly involved in the industry. Coal mine employees are generally male (96%), white (96%), non-Hispanic (98%), and middle-aged (average age of 44 years) (McWilliams et al., 2012). According to data from the 2017 U.S. Energy and Jobs Report (U.S. Department of Energy, 2017), employees in the oil and natural gas production sector are highly male (75%), white (79%), non-Hispanic (85%), and younger than 55 years old (77%).7 These figures are similar but less extreme than those for employees in the coal mining industry.
In Table 4, we estimate the effects of coal mining and horizontal well development on mortality rates by sub-population. In Panel A, we focus on total non-drug mortality rates. In Panel B, we focus on opioid overdose mortality rates. We focus on sub-populations defined by race (white vs. non-white), and combinations of sex and age (18–39 and 40–65 years old). We hypothesize that resource development will most effect mortality rates for those sub-populations that are most often employed by the industry. We include state-by-year fixed effects in all models shown in Table 4.
Table 4:
Heterogeneity in the effects of resource development on mortality by population subgroups
| (1) | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
|
|
||||||
| Race | Aged: 18–39 | Age: 40–65 | ||||
|
|
||||||
| White | Non-White | Male | Female | Male | Female | |
|
| ||||||
| Panel A: Non-Drug Mortality | ||||||
|
| ||||||
| # of operating coal mines (in 10s) | −17.50*** (6.696) | 17.04 (25.03) | 9.646** (4.495) | −1.125 (2.774) | −29.66*** (9.880) | −33.80*** (12.26) |
| # of horizontal oil and gas wells (in 100s) | −14.68 (9.352) | 10.40 (11.88) | 1.083 −2.467 |
−0.424 (1.707) | 4.886 (3.891) | −3.668 (3.769) |
|
|
||||||
| # of observations | 32,601 | 32,123 | 32,546 | 32,546 | 32,546 | 32,546 |
| R-squared | 0.849 | 0.481 | 0.326 | 0.255 | 0.627 | 0.502 |
|
| ||||||
| Panel B: Opioid Overdose Mortality | ||||||
|
| ||||||
| # of operating coal mines (in 10s) | −1.153 (0.831) | 1.529 (2.404) | 7.177*** (2.455) | 2.129 (1.407) | −5.018** (2.149) | −3.117** (1.557) |
| # of horizontal oil and gas wells (in 100s) | 0.176 (0.191) | 0.452 (0.575) | 0.462 (0.587) | 0.479 (0.552) | −0.101 (0.320) | 0.123 (0.365) |
|
|
||||||
| # of observations | 32,776 | 32,725 | 32,776 | 32,776 | 32,776 | 32,776 |
| R-squared | 0.493 | 0.095 | 0.284 | 0.187 | 0.363 | 0.271 |
|
| ||||||
| All Region <= 100 miles from shale/coal basins | X | X | X | X | X | X |
Notes: In this table, we highlight estimates of the effects of resource development on opioid overdose rates across different populations. In Panel A, the outcome variable is the non-drug mortality rate (per 100,000 people). In Panel B, the outcome variable is the opioid overdose rate (per 100,000 people) with corrections used based on models discussed in Boslett, Denham, and Hill (2019) for the given population sub-group of interest. All models include county fixed effects, state-by-year fixed effects, and interactions between a year vector and the initial mortality rate in 2000 to control for pre-coal bust and pre-shale boom differences in mortality rates. Statistical significance: 1% level, ***; 5% level, **; and 10% level, *.
In Panel A of Table 4, we observe that declining coal mining is associated with increases in total non-drug mortality rates for the white population and decreasing mortality rates for the non-white population. The effect on the non-white population is not statistically significant. We observe that decreases in coal mining are associated with increases in non-drug mortality for males and females aged 40–65 years old. However, we see a statistically significant opposite effect for males aged 18–39 years old (Column 3). UOGD is associated with declining non-drug mortality for the white population and increasing non-drug mortality for the non-white population. Neither are statistically significant. We do not observe statistically significant effects of UOGD on non-drug mortality rates when we stratify by age and sex (columns 3–6).
In Panel B of Table 4, we find weak qualitative evidence that coal mining is also associated with declines in opioid overdose mortality for the white population but not the non-white populations. Neither estimate is statistically significant. Declining coal mining is also associated with increases in opioid overdose mortality for both middle-aged (40–65 years old) males and females, though we see decreasing relationship for men aged 18–39 years old. For UOGD, we find minimal evidence of heterogeneity by age or race/ethnicity.
In summary, we find some evidence that the sub-populations most often employed by the coal mining industry have the strongest relationship between coal mining activity and non-drug mortality and opioid overdose mortality, though the story is not complete. Based on the employment profile of coal mine workers, we observe evidence that coal mining affects non-drug mortality primarily for white people, women, and middle-aged men and women, while it affects opioid overdose mortality for middle-aged men and women. However, we observe that declining coal mining is associated with increases in non-drug mortality and opioid overdose mortality for males aged 20–39 years old. Assuming that this population would be highly-represented in the local mining workforce, we expected that declines in coal mining would lead to increases in mortality for this sub-population. Given the discrepancy, we hesitate to infer that the mortality effects of coal mining are largely felt by sub-populations most likely to be employed by the industry.
7.3. Does resource development impact other types of non-drug deaths of despair?
In this section, we now examine whether the same association exists between alternative “Deaths of Despair” that do not involve a drug overdose. It is possible that our results are driven by differences in the local drug environment that evolve with changing levels of resource development. For example, the local drug supply could change in response to declines in operating coal mines (Carpenter, McClellan and Rees, 2017). In Appendix Table A2 we evaluate our results while controlling for the total level of opioid prescriptions in the county (ARCOS) in our models, though it is possible that this variable is an imperfect proxy for variation in local drug supply. We now test whether our overall finding is unique to drug overdoses or if the finding holds for other forms of “Deaths of Despair.” If it is the latter, then our drug overdose-focused results are unlikely to be due to unobserved, varying levels of local drug supply.
In Table 6, we examine whether resource development influences other “Deaths of Despair”: non-drug overdose suicides and alcohol overdoses. The signs of our estimates are in line with those associated with drug overdoses: declines in coal mining is associated with increases in the rates of alcohol overdoses and non-drug overdose suicides, while horizontal oil and gas well development is associated with increases in the rates of these types of deaths. The effect of coal mining on non-drug overdose suicides is statistically significant at the 10% level for models with and without state-by-year fixed effects. The effect of horizontal drilling on non-drug overdose suicides is significant at the 10% level for models without, but not with, state-by-year fixed effects. The effects of both forms of resource development on alcohol overdoses are not statistically significant.
Table 6:
The relationship between resource development and non-drug overdose “Deaths of Despair”
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
|
|
||||
| Non-Drug Overdose Suicides | Alcohol Overdoses | |||
|
| ||||
| # of operating coal mines (in 10s) | −0.660* (0.392) | −0.664* (0.403) | −0.0751 (0.108) | −0.122 (0.102) |
| # of horizontal oil and gas wells (in 100s) | 0.439* (0.250) | 0.320 (0.236) | 0.00607 (0.0384) | 0.0348 (0.0381) |
| # of operating coal mines (in 10s), 0 < X ≤ 25 miles | 0.192 (0.221) | 0.311 (0.232) | 0.0159 (0.0478) | 0.0118 (0.0492) |
| # of operating coal mines (in 10s), 25 < X ≤ 50 miles | −0.142 (0.149) | −0.0862 (0.172) | −0.0107 (0.0290) | 0.000871 (0.0306) |
| # of horizontal O&G wells (in 100s), 0 < X ≤ 25 miles | −0.113 (0.0828) | −0.109 (0.0827) | −0.00130 (0.0159) | −0.000141 (0.0159) |
| # of horizontal O&G wells (in 100s), 25 < X ≤ 50 miles | 0.0823 (0.0573) | 0.0590 (0.0622) | 0.00826 (0.0126) | 0.00561 (0.0132) |
| # of observations | 27,384 | 27,384 | 32,844 | 32,844 |
| R-squared | 0.380 | 0.404 | 0.164 | 0.207 |
|
| ||||
| State * Year FE | X | X | X | X |
| All U.S. <= 100 miles from shale/coal basins | X | X | X | X |
Notes: In this table, we display results of models connecting resource development with mortality associated with non-drug overdose “Deaths of Despair” (rates measured per 100,000 people). In Column 1, our outcome variable is the county’s non-drug overdose suicide rate. In Column 2, our outcome variable is the county’s alcohol overdose rate. All models include county fixed effects, year fixed effects, and interactions between a year vector and the initial mortality rate to control for pre-coal bust and pre-shale boom differences in mortality rates. Statistical significance: 1% level, ***; 5% level, **; and 10% level, *.
These results lend some support for our argument that certain types of resource development can reduce the incidence of “Deaths of Despair”, including both drug overdoses and non-drug overdose suicides. However, we do not find strong support for a similar effect for UOGD, nor do we find any evidence of impacts on alcohol overdoses.
7.4. Does resource development impact mortality rates through migration?
In our conceptual framework, we argue that resource development may influence drug overdose rates through its impact on population makeup. As previous research has found, economic shocks can lead to migration, which could result in our outcome of interest being mismeasured by changing the denominator (and potentially the numerator). The concern is not just mechanical. If heterogeneous groups of people (e.g., young, healthy, educated) move into an area with a resource boom, then it will change not only the total population but also the composition. Additionally, this migration may contaminate our control group if individuals moving to the treatment area come from the control area. We address this “spillover” concern through the inclusion of indicators for rings outside of the treatment areas that may be most likely to migrate or experience economic spillovers, but that does not completely address changes in the control group if individuals are migrating from longer distances. Certain populations have different levels of susceptibility to non-drug mortality (Baltrus, 2019; Ferdows et al., 2020) or drug abuse (Rosenblum et al., 2007; Palamar et al., 2016), and we expect that resource development will lead to population-driven changes in drug overdose rates if these populations change in relative size due to resource development (e.g., migration).
As another robustness check, we control for the changing population make-up over time – i.e., the percentages of the population by race, ethnicity, and age by county-year – because our interest in this study is to understand the relationship between resource development and mortality. To assess how migration or compositional changes may be influencing our results, we first estimate how resource development affects population and sub-group population levels. In Appendix Table A12, we estimate the effects of resource development on total population and sub-group population levels, the latter measured in percentages. We find evidence that declining coal mining is associated with decreases in total population and the percentages of the population that are Hispanic and Asian. It is also associated with increasing the percentage of the population that is white. We find some evidence that declining coal mining is associated with decreases in the working-age population, though this result attenuates and switches sign with the inclusion of state-by-year fixed effects. Additionally, we find that UOGD is associated with increases in total population and the percentages of the working-age and white population and decreases in the percentage of the population that is Asian. It is possible that these population level and makeup dynamics are contributing to our estimated effects. For example, our models suggest that declining coal mining is associated with increases in the percentage of the population that is white, a group that has driven the rise in opioid overdose mortality in the 2000–2010 period (Alexander, Kiang and Barbieri, 2018). If the proportion of the population that is white increases with declining coal mining, we would expect that declines in coal mining would lead to increases in opioid overdose mortality, ceteris paribus.
These findings suggest that resource development may influence mortality rates through population-related mechanisms. In robustness checks, we control for contemporaneous population levels and makeup at the county-level, though we cannot be certain that this effect is unadulterated by changes in unobserved population-related variables. Furthermore, our annual measures of population and demographics are potentially mismeasured given they are not from Census years. However, we argue that our coal mining-related results are unlikely to be completely driven by changes in population make-up due to consistent findings using long-differences and one additional specification. Instead of using total population as the denominator, we estimate a regression with mortality per total employment which is better measured over time by the Bureau of Labor Statistics. In Table A12, we find qualitatively similar results.
7.5. Comparison with existing literature on coal mining and mortality
We now discuss one more possible robustness check: alternative measures of treatment. One possible alternative was put forth by Metcalf and Wang (2019) who find a positive relationship between the share of coal miners in the local labor force and county-level opioid overdose rates; they found a one percent increase in the share of coal miners resulted in a 0.192 percent increase in opioid mortality rates. Their results are counter to our conceptual framework and results. We attempted to replicate their approach for both coal and horizontal drilling but found many of the counties with the most horizontal drilling are “non-disclosure” at the county-level for employment data from the BLS (Pickenpaugh and Adder, 2018). Due to this, we only “replicate” coal mining and the national sample 2006–2016 (Table A13)8 and get similar findings. Using a different treatment variable to capture coal mining does not explain the discrepancy in results. Instead, the discrepancy comes from the start year of the data panel; the results are similar when we change our panel start year to be consistent with theirs (i.e., 2006) or change their panel start year to ours (i.e., 2000) (See Table A6 for our results in 2006 and Table A14 for theirs in 2000–2016).
We explore why our results are sensitive to start year by assessing heterogeneity by resource extraction intensity. First, we create intensity binaries of coal mining intensity (i.e., 1–2 mines, 2–5 mines, 5–10 mines, 10–20 mines and 20+ mines) due to us finding the strongest impacts for coal in Table 3 and our robustness checks. We allow these binaries to vary over time (i.e., are based upon the number of coal mines contemporaneously in each year) to understand whether the effect of mining is similar across coal mining intensity. We re-estimate model (2) replacing Resourceit with these intensity bins (these models do not have spillover controls but are restricted to within 100 miles of a coal basin or shale play). In Figure 3, we present the coefficients from this model and find that for non-drug mortality, the areas experiencing a protective effect are those with 20 or more mines. For opioid mortality, we find positive coefficients, but none are statistically precise. In the Appendix Figure A7, we present the same estimates for 2006–2016. The results for non-drug mortality remain negative for the most mined counties but suggest positive impacts for opioid mortality for all counties with more than 5 coal mines operating each year.
Figure 3.
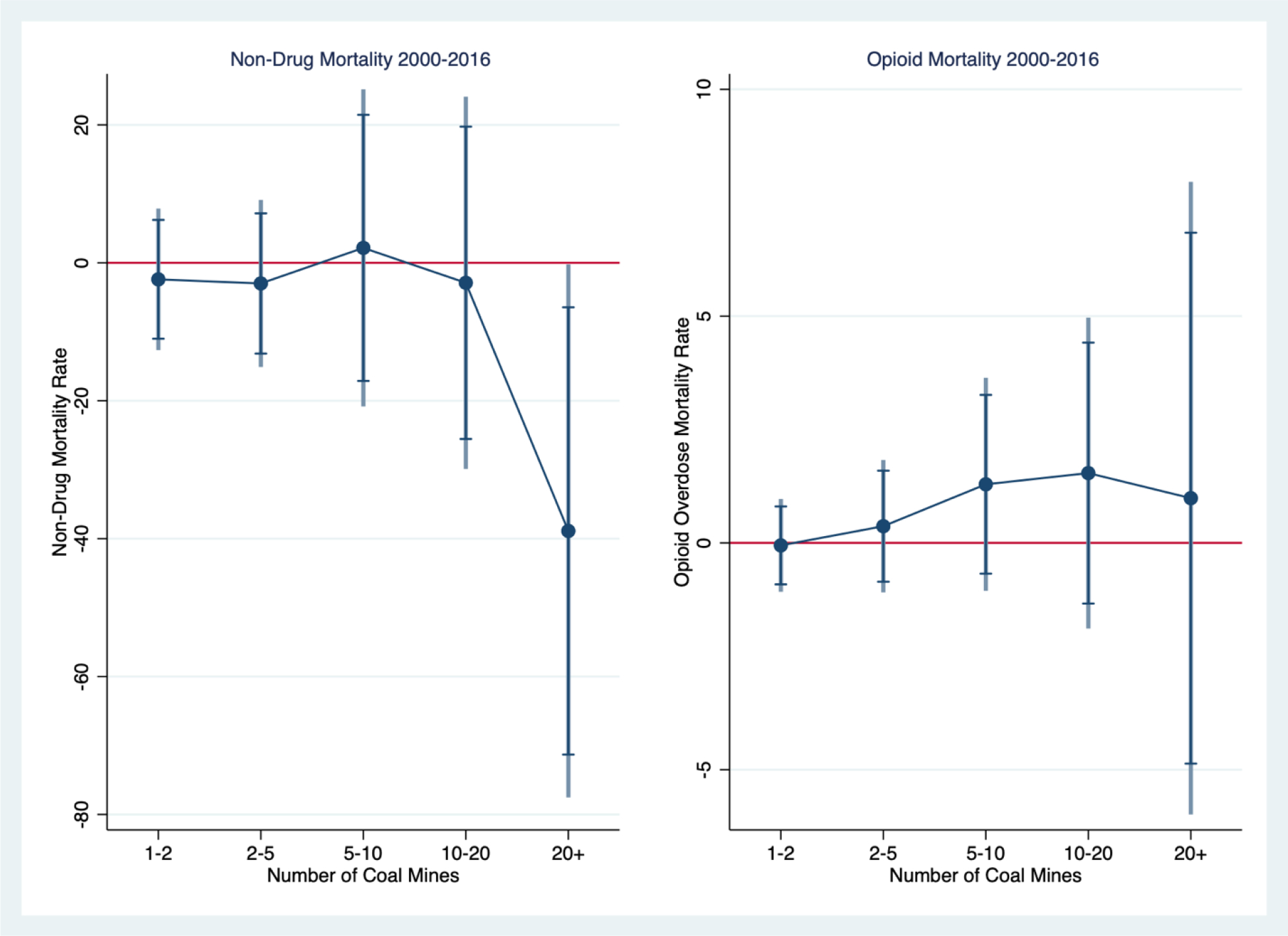
Impacts of Coal Mining Intensity by Number of Coal Mines, 2000–2016
Notes: Coefficient estimates from equation 1 where coal mining is modeled as dummies for number of coal mines in the county-year (1–2 mines, 2–5 mines, 5–10 mines, 10–20 mines and 20+ mines), county, year and state-by-year FE. Clustered standard errors at county. Sample is limited to within 100 miles of a coal basin or shale play.
One final explanation for why we find contrary results is that we find counties with the most coal mining in 2000 experienced an early bust during a relatively low period of opioid mortality that could drive a negative correlation, as shown in Figure A8. It is subtle, but from 2006 on there is a slight correlation between declining coal mines and the declining mortality gap and likely leads to the positive relationship measured in Metcalf and Wang (2019) and Figure A7. This leads us to conclude that estimating the causal impact of resource extraction on opioid mortality is challenging and difficult to achieve given these differential trends overlapping with the opioid overdose crisis.
We chose to continue with our treatment variable (i.e., # of operating mines) because we wish to understand the impact of resource booms and busts beyond individuals employed in the industry. Local economies in Appalachia, especially in rural areas, have been historically dependent on coal mining: there are many jobs in a county beyond the coal mine that are reliant on operating coal mines. For example, coal must be transported by barge or railway to end-consumers, and these jobs are likely to be lost with declining coal mining. This is supported by recent evidence in Weber (2019), which found declining numbers of employees at coal mines are associated with negative spillover effects into other local industries. Declines in the number of people employed at coal mines are likely to be met by declines in the number of people employed elsewhere in the community. As the local economy declines, people may move away reducing the total employed population in the county. We test this by estimating regression models with measures of total employment and share of employed in the coal industry as outcomes and our treatment variables as independent variables of interest in Table A15. We find that both the number of coal mines and number of horizontal wells increase total employment and that an additional 10 mines increase the share of coal employment by 0.03. Therefore, our measures are highly correlated, but also a reduction in coal employment is also likely to reduce total employment, such that the share may change or stay the same and not be a reliable measure of coal intensity.
Metcalf and Wang (2019) argue that coal mining positively influences drug overdose rates because coal mine working conditions are difficult and even painful at times. To square our results with theirs, it is possible that coal mining is associated with higher drug overdose rates for active or recently-inactive coal miners at the same time it leads to reduced drug overdose rates for other individuals that do not work at coal mines but whose livelihoods are reliant on them. We are unable to observe the employment status and industry of decedents in the death record to test this hypothesis.
We do, however, separately estimate models for pain-related contributing causes of death. Resource development may lead to higher rates of drug abuse for pain relief and, subsequently, mortality because jobs in these industries require hard, physical work in dangerous environments. Fatality and injury rates in the coal and oil and gas industries have declined over time but are still substantially higher than other industries in the U.S. (Mason et al., 2015). Urine tests for coal miners have higher rates of detection of certain drugs, including opioids, after accidents (Price, 2012), which suggests that the mining work environment may lead to higher rates of pain-relieving drug use.
In Figure A9 in the Appendix, we visually examine how state-level drug overdose rates with pain-related contributing causes evolves over time in our study period. Appalachian states – highlighted by those with the highest levels of coal mining and horizontal well development in our study period – do not have noticeably higher or different trajectories in drug overdose rates with pain contributing causes of death versus those of non-Appalachian states. In Table A12, we examine the statistical relationship between levels of resource development and county-level drug overdose rates with pain-related contributing causes of death.9 We do not observe a strong, consistent relationship between coal mining and drug overdose rates with pain-related contributing causes of death. We observe some statistically significant evidence that horizontal well development leads to lower drug overdose rates with pain-related contributing causes of death. In total, we do not observe consistent evidence that either form of resource development influenced the level of drug overdoses with contributing causes related to chronic pain. This finding does not preclude some role in resource development positively influencing drug overdose rates due to a high degree of pain associated with work conditions, though these results would suggest the effect would be small.
7.6. Heterogeneity by Region
Our results do not perfectly square with the deaths of despair argument for shale gas development (not statistically significant). Before we conclude that there is something unique about the shale boom, we evaluate heterogeneity by region because the coal bust did not happen everywhere. In fact, in the Rocky Mountain States of Wyoming, Montana, North Dakota and Colorado, coal production stayed stable or slightly reduced relative to the bust that occurred in Appalachian States (See Appendix Figure A6). In this section we explore differences by these two regions to understand whether we see differences by boom-and-bust cycles, as opposed to the industry. Although UOGD using horizontal drilling and hydraulic fracturing occurred across the U.S. (Figure A1), most coal mining in the U.S. occurs in these two regions. We define our Appalachia sub-region based on those counties that are served by the Appalachia Regional Commission (ARC) (see Figure A5 in the Appendix for a map of the Appalachia region). We include counties in the states of Colorado, Montana, North Dakota, and Wyoming for the northern Rocky Mountain states. All four states have experienced UOGD and some degree of coal mining in the 21st century.
In Appendix Figure A10, we present trends in non-drug mortality and opioid overdose morality by two regions: Rocky Mountain States and Appalachian States. First, it’s important to note that counties in the Rocky Mountain states have fewer but more productive mines (there are no counties with more than 10 mines). The trends in Appalachia look similar to the national trends in Figure A8. We also present a version of Figure 3 in Appendix Figure A11 (2000–2016) by these two regions. For the counties with the most mines, we do see opposite impacts of mining intensity on mortality for these two regions. Given Rocky Mountain States do not experience a bust prior to 2010, we also present results from 2000–2010 to attempt to separate the industry from boom/bust interpretations (Appendix Figure A12). Non-drug mortality is similar as Figure A9, but for opioid overdose mortality both regions suggest a protective effect for the counties with the most mines.
In Appendix Table A16, we present the overall results stratified by region for 2000–2016 and 2000–2010. Overall, we observe that our main results only occur in Appalachia, with no evidence of significant effects of resource development on mortality in the northern Rocky Mountain states. For drug overdose and opioid overdose mortality we see opposite-signed relationships between the two regions, with the results for Rocky Mountain states not statistically significant. We argue that this is because of the unique nature of coal mining and UOGD in Appalachia. Coal mining in Appalachia has high labor intensity of coal mining relative to coal mining in the northern Rocky Mountain states. In 2016, the Appalachian states of Kentucky, Maryland, Ohio, Pennsylvania, and West Virginia, and Virginia made up more than 26% of total coal production in the U.S. yet employed almost 52% of the total coal workforce.10 Appalachian coal is also generally bituminous in rank; these counties have experienced large recent production declines, relative to areas of the country that house sub-bituminous coal, such as the northern Rocky Mountain States, whose production has increased over time. In Figure A6, we show coal production in 2000 and 2017 for the top-15 states in coal production in 2000. We observe that Appalachian states have experienced larger declines in coal production relative to those in the high production western states, where production has been largely stable or minimally declined (e.g., Wyoming; North Dakota). Overall, these comparisons do not suggest a consistent story for drug and opioid overdose mortality further supporting our conclusion that the combined dynamics of the overdose crisis and changing resource extraction in these communities leave an inconclusive picture.
7.7. Interpreting Magnitudes
To put our results in the context of existing studies of local economic shocks on both all-cause and opioid overdose mortality, our coefficient estimates imply that 10 fewer operating coal mines inreases non-drug mortality by 2% (p-value <0.001) and opioid overdose mortality by 7% (not significant) and an interquartile shift11 in exposure to coal mining is associated with a relative increase of 10.8 non-drug-related deaths per 100,000 and 0.702 increase in opioid overdose deaths per 100,000, or a 1% and 14% increase relative to the base mortality rates in 2000 (this is consistent with multiplying our log results by the interquartile range). We also calculate the change in the total number of deaths (excess deaths) associated with coal mining: our estimates imply the interquartile shift in less coal mining leads to 1,348 more non-drug deaths and 86 more opioid overdose deaths.12 We begin by comparing our results to studies of unemployment and county-level economic markers such as housing prices: Heutel and Ruhm (2016) found a 1 pp increase in unemployment decreased total mortality rate by 0.35%, Hollingsworth et al. (2017) found a 1 pp increase in unemployment increased the opioid mortality rate by 0.19 per 100,000 (3.6%) and Brown and Wehby (2019) found during the great recession drug overdose deaths significantly declined with higher house prices or by nearly 0.17 deaths per 100,000 (~4%) with a $10,000 increase in median house price. Arthi et al. (2019) found the cotton famine increased mortality by 2 deaths per 1,000, which is much larger in magnitude than our estimates for resource extraction. The magnitudes of our results are most similar to a study of trade liberalization which found an interquartile shift in counties’ exposure to trade liberalization policy is associated with a relative increase in mortality from overall deaths of despair of 2 to 3 per 100,000, or 10 to 15 percent of the average mortality rate the year of the policy change (Pierce and Schott, 2020). Finally, our results are comparable to two papers studying changes in manufacturing and opioid mortality: increased automation (each additional robot per 1,000 workers) led to just over 8 additional deaths per 100,000 males aged 45–54 (OBrien, Venkataramani and Bair, 2021) and five years after a manufacturing plant closure, mortality rates had increased by 8.6 opioid overdose deaths per 100 000 individuals in exposed counties compared with unexposed counties (85% higher relative increase) (Venkataramani et al., 2020). Our results fit within the magnitudes of the existing literature both in size and economic significance.
8. Conclusions
Our paper fills a gap in the literature by studying resource extraction booms and busts to estimate how local economic conditions impact mortality. We contribute to a growing economic literature on the causal effect of local economic conditions on mortality and specifically on drivers of the drug overdose epidemic. We find robust evidence that resource development can have measurable impacts on non-drug mortality rates in local areas. In particular, we find that the coal bust increased non-drug and working age non-drug mortality and the shale boom has provide some protection against non-drug mortality and working-age non-drug mortality. These results are driven by the most intensively-extracted counties. However, we find that some of this measured beneficial relationship could be explained by the influx of population through migration. We argue it is not completely explained by migration through several robustness checks (e.g., long difference, mortality-per-total employment). For drug overdose mortality and opioid mortality, our results are sensitive to start year and migration, although the long difference models suggest declines in coal mining increases opioid mortality. We believe the sensitivity of these results is driven by differential trends for the most intensively-extracted counties and that counties with the most coal mining in 2000 experienced an earlier bust during a time when there was less opioid mortality. The combination of migration, spillovers into control units, and heterogeneity leaves a complex picture for opioid mortality. We find no statistically precise relationship between UOGD and mortality, except for increased non-drug suicides.
We use resource booms and busts as exogenous economic shocks to understand how local economic conditions impact deaths of despair, such as drug overdose mortality. We find some suggestive evidence that the effects of coal mining on opioid overdose mortality are strongest for those likely employed by the industry (e.g., mid-life men; the white population). However, we see opposite effects for young males. For the shale boom, we observe limited evidence of heterogeneity. We find evidence that declines in operating coal mines are associated with increases in non-drug suicides and that UOGD may have increased non-drug suicides nationally. In terms of alternative mechanisms of our results, we observe that contemporaneous coal mining is associated with decreases in populations with high levels of drug overdose rates; thus, our estimates are unlikely to be biased upward due to population makeup changes due to coal mining.
Our paper discusses the challenges of studying how economic conditions impact mortality in the face of migration and spatial spillovers. Future work could use individual-level data with residential history and occupation/employment information to address the remaining questions around how resource extraction booms and busts impact opioid mortality. Future work could explore questions regarding non-labor income shocks from oil and gas leasing and its effects on health and mortality more broadly. These shocks were large (Brown, Fitzgerald and Weber, 2016; Fitzgerald and Rucker, 2016) and could have possibly had an effect on health expenditures and, potentially, a protective effect through pollution mitigation.
The decline of coal may be desirable for many reasons, not least of all health: air pollution from coal has been implicated in ~1 million or a 1/3rd of all deaths related to air pollution worldwide, coal mine work can be dangerous due to mine collapses and gas poisoning (Bennett and Passmore, 1984), long-term exposure to coal dust in and around mines can cause black lung (Hendryx and Ahern, 2008; Potera, 2019), and the transportation and storage of coal can cause downwind respiratory issues (Jha and Muller, 2017). Our research suggests that this decline may lead to local health costs through increased mortality. The number of deaths from coal-related air pollution on an annual basis worldwide swamps that of the number of drug overdoses in the U.S. over the 21st century. Thus, the overarching findings of a full cost-benefit analysis of coal mining are unlikely to change when one includes the effects of coal mine closures on local drug overdose mortality found in this research. However, our findings suggest a potential role for job-training programs and the cultivation of local healthcare resources in regions suffering from coal and other resource busts in the future.
Supplementary Material
Acknowledgements
Research reported in this publication was supported by the Office of the Director of the National Institutes of Health under award number DP5OD021338. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors thank Erin Campbell and Evan Volkin for research support.
Footnotes
Metcalf and Wang (2019) is one study in development that is similar to our work. Similarities and differences between our study and theirs are discussed in discussion section.
In Appendix Figure A2, we show the changing landscape of energy production and electricity generation in the United States from 2000 to 2016. Coal production from operating mines declines substantially over time, starting in earnest in around 2008.
In Appendix Figure A3, we show the decline in in operating coal mines on an annual basis by state in Appalachia.
This is based on calculations using the U.S. Energy Information Administration’s Table 21: Coal Productivity by State and Mine Type, 2017 and 2016.
Although this begins to shift after 2018, with Black and Latinx populations experiencing increased risk for drug overdose; this is even more pronounced during the COVID-19 Pandemic (Furr-Holden et al., 2021; Larochelle et al., 2021).
We drop the county fixed effect because it is subsumed in the difference.
The report provided statistics separated by industry, including natural gas production and oil extraction. We calculated means weighted by the number of employees in each industry.
We use replicate a bit loosely here. We do not employ their 3-lag model here due to the contemporaneous effect being similar in magnitude and statistical significance as their “cumulative effect”. This allows for a simpler comparison to our results as we do not present a lagged model.
To do so, we exploit the fact that each death in the death record has an underlying cause of death and a series of contributing causes of death. We used these data to impute opioid involvement in drug overdoses without an identified causal drug (Boslett, Denham and Hill, 2020). In that study, the authors found that general chronic pain (R52.2 and R52.9), Dorsalgia (M54.9), and fibromyalgia (M79.7) occurred at high rates in opioid overdoses. Using these and other long-term pain-related ICD-10 codes, we estimate that there were 7,903 drug overdoses with pain-related contributing causes of death (1.2% of all drug overdoses). We note that this is likely an underestimate given potential limitations in the ability of medical examiners and coroners in identifying long-term pain, post-death.
Author calculations using data from the Mine Safety and Health Administration (MSHA) Mine Data Retrieval System.
IQR is 0.6 coal mines. We multiply our coefficient by IQR and then divide by the average death rate in 2000.
However, if we calculate this for a base year of 2006, we find the interquartile shift reduced excess mortality by 753 non-drug related deaths and increased opioid overdose deaths by 130.
Conflict of Interest Statement
The authors declare no known interests related to their submitted manuscript.
REFERENCES
- Agerton M et al. (2017) ‘Employment impacts of upstream oil and gas investment in the United States’, Energy Economics, 62, pp. 171–180. doi: 10.1016/j.eneco.2016.12.012. [DOI] [Google Scholar]
- Aizer A et al. (2016) ‘The Long-Run Impact of Cash Transfers to Poor Families’, American Economic Review, 106(4), pp. 935–971. doi: 10.1257/aer.20140529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alexander MJ, Kiang MV and Barbieri M (2018) ‘Trends in Black and White Opioid Mortality in the United States, 1979–2015’, Epidemiology (Cambridge, Mass.), 29(5), pp. 707–715. doi: 10.1097/EDE.0000000000000858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Almond D and Currie J (2011) ‘Human Capital Development before Age Five’, Handbook of Labor Economics, 4, pp. 1315–1486. [Google Scholar]
- Alpert AE et al. (2019) Origins of the Opioid Crisis and Its Enduring Impacts. Working Paper 26500. National Bureau of Economic Research. doi: 10.3386/w26500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arkes J (2007) ‘Does the economy affect teenage substance use?’, Health Economics, 16(1), pp. 19–36. doi: 10.1002/hec.1132. [DOI] [PubMed] [Google Scholar]
- Arthi V, Beach B and Hanlon WW (2017) Estimating the Recession-Mortality Relationship when Migration Matters. w23507. Cambridge, MA: National Bureau of Economic Research, p. w23507. doi: 10.3386/w23507. [DOI] [Google Scholar]
- Arthi V, Beach B and Hanlon WW (2019) ‘Recessions, Mortality, and Migration Bias: Evidence from the Lancashire Cotton Famine’. [Google Scholar]
- Autor D, Dorn D and Hanson G (2019) ‘When Work Disappears: Manufacturing Decline and the Falling Marriage Market Value of Young Men’, American Economic Review: Insights, 1(2), pp. 161–178. doi: 10.1257/aeri.20180010. [DOI] [Google Scholar]
- Autor DH, Levy F and Murnane RJ (2003) ‘The Skill Content of Recent Technological Change: An Empirical Exploration’, The Quarterly Journal of Economics, 118(4), pp. 1279–1333. doi: 10.1162/003355303322552801. [DOI] [Google Scholar]
- Ayllón S and Ferreira-Batista NN (2018) ‘Unemployment, drugs and attitudes among European youth’, Journal of Health Economics, 57, pp. 236–248. doi: 10.1016/j.jhealeco.2017.08.005. [DOI] [PubMed] [Google Scholar]
- Baltrus P (2019) ‘Identifying County-Level All-Cause Mortality Rate Trajectories and Their Spatial Distribution Across the United States’, Preventing Chronic Disease, 16. doi: 10.5888/pcd16.180486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beleche T and Cintina I (2018) ‘Fracking and risky behaviors: Evidence from Pennsylvania’, Economics & Human Biology, 31, pp. 69–82. doi: 10.1016/j.ehb.2018.08.001. [DOI] [PubMed] [Google Scholar]
- Bennett JD and Passmore DL (1984) ‘Correlates of coal mine accidents and injuries: A literature review’, Accident Analysis & Prevention, 16(1), pp. 37–45. doi: 10.1016/0001-4575(84)90004-6. [DOI] [Google Scholar]
- van den Berg GJ, Lindeboom M and Portrait F (2006) ‘Economic Conditions Early in Life and Individual Mortality’, American Economic Review, 96(1), pp. 290–302. doi: 10.1257/000282806776157740. [DOI] [PubMed] [Google Scholar]
- Betz MR et al. (2015) ‘Coal mining, economic development, and the natural resources curse’, Energy Economics, 50, pp. 105–116. doi: 10.1016/j.eneco.2015.04.005. [DOI] [Google Scholar]
- Betz MR and Jones LE (2018) ‘Wage and Employment Growth in America’s Drug Epidemic: Is All Growth Created Equal?’, American Journal of Agricultural Economics, 100(5), pp. 1357–1374. doi: 10.1093/ajae/aay069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black D, Daniel K and Sanders S (2002) ‘The Impact of Economic Conditions on Participation in Disability Programs: Evidence from the Coal Boom and Bust’, American Economic Review, 92(1), pp. 27–50. doi: 10.1257/000282802760015595. [DOI] [PubMed] [Google Scholar]
- Black D, McKinnish T and Sanders S (2003) ‘Does the availability of high-wage jobs for low-skilled men affect welfare expenditures? Evidence from shocks to the steel and coal industries’, Journal of Public Economics, 87(9), pp. 1921–1942. doi: 10.1016/S0047-2727(02)00014-2. [DOI] [Google Scholar]
- Black D, McKinnish T and Sanders S (2005) ‘The Economic Impact Of The Coal Boom And Bust*’, The Economic Journal, 115(503), pp. 449–476. doi: 10.1111/j.1468-0297.2005.00996.x. [DOI] [Google Scholar]
- Black KJ et al. (2020) A Review of the Economic, Environmental, and Health Impacts of the Fracking Boom. SSRN Scholarly Paper ID 3780721. Rochester, NY: Social Science Research Network. Available at: https://papers.ssrn.com/abstract=3780721 (Accessed: 9 February 2021). [Google Scholar]
- Black KJ et al. (2021) ‘Economic, Environmental, and Health Impacts of the Fracking Boom’, Annual Review of Resource Economics, Forthcoming [Preprint]. [Google Scholar]
- Boslett A et al. (2019) ‘Unclassified drug overdose deaths in the opioid crisis: emerging patterns of inequity’, Journal of the American Medical Informatics Association [Preprint]. doi: 10.1093/jamia/ocz050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boslett A, Denham A and Hill E (2020) ‘Using contributing causes of death improves prediction of opioid involvement in unclassified drug overdoses in U.S. death records’, Addiction, Forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown E and Wehby GL (2019) ‘Economic Conditions and Drug and Opioid Overdose Deaths’, Medical Care Research and Review, 76(4), pp. 462–477. doi: 10.1177/1077558717722592. [DOI] [PubMed] [Google Scholar]
- Brown JP, Fitzgerald T and Weber JG (2016) ‘Capturing rents from natural resource abundance: Private royalties from U.S. onshore oil & gas production’, Resource and Energy Economics, 46, pp. 23–38. doi: 10.1016/j.reseneeco.2016.07.003. [DOI] [Google Scholar]
- Buchanich JM et al. (2018) ‘The Effect of Incomplete Death Certificates on Estimates of Unintentional Opioid-Related Overdose Deaths in the United States, 1999–2015, The Effect of Incomplete Death Certificates on Estimates of Unintentional Opioid-Related Overdose Deaths in the United States, 1999–2015’, Public Health Reports, 133(4), pp. 423–431. doi: 10.1177/0033354918774330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter CS, McClellan CB and Rees DI (2017) ‘Economic conditions, illicit drug use, and substance use disorders in the United States’, Journal of Health Economics, 52, pp. 63–73. doi: 10.1016/j.jhealeco.2016.12.009. [DOI] [PubMed] [Google Scholar]
- Case A and Deaton A (2015) ‘Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century’, Proceedings of the National Academy of Sciences, 112(49), p. 15078. doi: 10.1073/pnas.1518393112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catalano R (1979) ‘Health costs of economic expansion: the case of manufacturing accident injuries.’, American Journal of Public Health, 69(8), pp. 789–794. doi: 10.2105/AJPH.69.8.789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catalano R, Novaco RW and McConnell W (2002) ‘Layoffs and violence revisited’, Aggressive Behavior, 28(3), pp. 233–247. doi: 10.1002/ab.80003. [DOI] [Google Scholar]
- Charles KK, Hurst E and Schwartz M (2018) ‘The Transformation of Manufacturing and the Decline in U.S. Employment’, NBER Macroeconomics Annual 2018, volume 33 [Preprint]. Available at: https://www.nber.org/chapters/c14081 (Accessed: 25 February 2019). [Google Scholar]
- Charles KK, Li Y and Stephens M (2017) ‘Disability Benefit Take-Up and Local Labor Market Conditions’, The Review of Economics and Statistics, 100(3), pp. 416–423. doi: 10.1162/rest_a_00692. [DOI] [Google Scholar]
- Cicero TJ et al. (2014) ‘The Changing Face of Heroin Use in the United States: A Retrospective Analysis of the Past 50 Years’, JAMA Psychiatry, 71(7), pp. 821–826. doi: 10.1001/jamapsychiatry.2014.366. [DOI] [PubMed] [Google Scholar]
- Clark AE and Oswald AJ (1994) ‘Unhappiness and Unemployment’, The Economic Journal, 104(424), pp. 648–659. doi: 10.2307/2234639. [DOI] [Google Scholar]
- Clarke H et al. (2014) ‘Rates and risk factors for prolonged opioid use after major surgery: population based cohort study’, BMJ, 348, p. g1251. doi: 10.1136/bmj.g1251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cunningham S, DeAngelo G and Smith B (2020) ‘Fracking and Risky Sexual Activity’, Journal of Health Economics, p. 102322. [DOI] [PubMed] [Google Scholar]
- Currie J, Greenstone M and Meckel K (2017) ‘Hydraulic fracturing and infant health: New evidence from Pennsylvania’, Science Advances, 3(12), p. e1603021. doi: 10.1126/sciadv.1603021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Currie J, Jin J and Schnell M (2018) U.S. Employment and Opioids: Is There a Connection? w24440. Cambridge, MA: National Bureau of Economic Research. doi: 10.3386/w24440. [DOI] [Google Scholar]
- Currie J and Schnell M (2018) ‘A Closer Look at How the Opioid Epidemic Affects Employment’, Harvard Business Review, 20 August. Available at: https://hbr.org/2018/08/a-closer-look-at-how-the-opioid-epidemic-affects-employment (Accessed: 1 December 2018). [Google Scholar]
- Currie J and Schwandt H (2020) The Opioid Epidemic Was Not Caused by Economic Distress But by Factors that Could be More Rapidly Addressed. National Bureau of Economic Research. [Google Scholar]
- Cutler DM, Huang W and Lleras-Muney A (2016) Economic conditions and mortality: evidence from 200 years of data. National Bureau of Economic Research. [Google Scholar]
- Dart RC et al. (2015) ‘Trends in Opioid Analgesic Abuse and Mortality in the United States’, New England Journal of Medicine, 372(3), pp. 241–248. doi: 10.1056/NEJMsa1406143. [DOI] [PubMed] [Google Scholar]
- Deryugina T et al. (2019) ‘The mortality and medical costs of air pollution: Evidence from changes in wind direction’, American Economic Review, 109(12), pp. 4178–4219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deryugina T and Molitor D (2020) ‘Does When You Die Depend on Where You Live? Evidence from Hurricane Katrina’, American Economic Review, 110(11), pp. 3602–3633. doi: 10.1257/aer.20181026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dow WH et al. (2019) Can Economic Policies Reduce Deaths of Despair? Working Paper 25787. National Bureau of Economic Research. doi: 10.3386/w25787. [DOI] [Google Scholar]
- Ellerman AD et al. (2000) Markets for Clean Air: The U.S. Acid Rain Program. Cambridge University Press. [Google Scholar]
- Fell H and Kaffine DT (2018) ‘The Fall of Coal: Joint Impacts of Fuel Prices and Renewables on Generation and Emissions’, American Economic Journal: Economic Policy, 10(2), pp. 90–116. doi: 10.1257/pol.20150321. [DOI] [Google Scholar]
- Ferdows NB et al. (2020) ‘Assessment of Racial Disparities in Mortality Rates Among Older Adults Living in US Rural vs Urban Counties From 1968 to 2016’, JAMA Network Open, 3(8), p. e2012241. doi: 10.1001/jamanetworkopen.2020.12241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feyrer J, Mansur ET and Sacerdote B (2017) ‘Geographic Dispersion of Economic Shocks: Evidence from the Fracking Revolution’, American Economic Review, 107(4), pp. 1313–1334. doi: 10.1257/aer.20151326. [DOI] [Google Scholar]
- Finkelstein A, Gentzkow M and Williams HL (2019) Place-Based Drivers of Mortality: Evidence from Migration. w25975. National Bureau of Economic Research. doi: 10.3386/w25975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzgerald T and Rucker RR (2016) ‘US private oil and natural gas royalties: estimates and policy relevance’, OPEC Energy Review, 40(1), pp. 3–25. [Google Scholar]
- Fleming DA and Measham TG (2014) ‘Local job multipliers of mining’, Resources Policy, 41, pp. 9–15. doi: 10.1016/j.resourpol.2014.02.005. [DOI] [Google Scholar]
- Furr-Holden D et al. (2021) ‘African Americans now outpace whites in opioid-involved overdose deaths: a comparison of temporal trends from 1999 to 2018’, Addiction, 116(3), pp. 677–683. doi: 10.1111/add.15233. [DOI] [PubMed] [Google Scholar]
- Gourley P and Madonia G (2018) ‘Resource booms and crime: Evidence from oil and gas production in Colorado’, Resource and Energy Economics, 54, pp. 37–52. doi: 10.1016/j.reseneeco.2018.07.001. [DOI] [Google Scholar]
- Guo HR et al. (1999) ‘Back pain prevalence in US industry and estimates of lost workdays.’, American Journal of Public Health, 89(7), pp. 1029–1035. doi: 10.2105/AJPH.89.7.1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hastings K, Heller LR and Stephenson EF (2017) ‘Fracking and Labor Market Conditions: A Comparison of Pennsylvania and New York Border Counties’, Eastern Economic Journal, 43(4), pp. 649–659. doi: 10.1057/eej.2015.47. [DOI] [Google Scholar]
- Hedegaard H, Minino A and Warner M (2018) Drug Overdose Deaths in the United States, 1999–2017, NCHS Data Brief. No. 329. November 2018. Available at: https://www.cdc.gov/nchs/products/databriefs/db329.htm (Accessed: 29 July 2019).
- Hendryx M and Ahern MM (2008) ‘Relations Between Health Indicators and Residential Proximity to Coal Mining in West Virginia’, American Journal of Public Health, 98(4), pp. 669–671. doi: 10.2105/AJPH.2007.113472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heutel G and Ruhm CJ (2016) ‘Air Pollution and Procyclical Mortality’, Journal of the Association of Environmental and Resource Economists [Preprint]. doi: 10.1086/686251. [DOI] [Google Scholar]
- Hill (2018) ‘Shale gas development and infant health: Evidence from Pennsylvania’, Journal of Health Economics, 61, pp. 134–150. doi: 10.1016/j.jhealeco.2018.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill L (2017) ‘Shale Gas Development and Drinking Water Quality’, American Economic Review, 107(5), pp. 522–525. doi: 10.1257/aer.p20171133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollingsworth A, Ruhm C and Simon K (2017) ‘Macroeconomic conditions and opioid abuse’, Journal of Health Economics, 56(C), pp. 222–233. [DOI] [PubMed] [Google Scholar]
- Hollingsworth A, Ruhm CJ and Simon K (2017) ‘Macroeconomic conditions and opioid abuse’, Journal of Health Economics, 56, pp. 222–233. doi: 10.1016/j.jhealeco.2017.07.009. [DOI] [PubMed] [Google Scholar]
- Horwitt D (2014) Up in Flames: U.S. Shale Oil Boom Comes at Expense of Wasted Natural Gas, Increased CO2. Washington, D.C.: Earthworks. [Google Scholar]
- Hower JC, Robl TL and Thomas GA (1999) ‘Changes in the quality of coal delivered to Kentucky power plants, 1978 to 1997: responses to Clean Air Act directives’, International Journal of Coal Geology, 41(1), pp. 125–155. doi: 10.1016/S0166-5162(99)00014-2. [DOI] [Google Scholar]
- Hoynes H, Schanzenbach DW and Almond D (2016) ‘Long-Run Impacts of Childhood Access to the Safety Net’, American Economic Review, 106(4), pp. 903–934. doi: 10.1257/aer.20130375. [DOI] [Google Scholar]
- James A and Smith B (2017) ‘There will be blood: Crime rates in shale-rich U.S. counties’, Journal of Environmental Economics and Management, 84, pp. 125–152. doi: 10.1016/j.jeem.2016.12.004. [DOI] [Google Scholar]
- James AG and Smith B (2020) ‘Geographic dispersion of economic shocks: Evidence from the fracking revolution: Comment’, American Economic Review, 110(6), pp. 1905–13. [Google Scholar]
- Jha A and Muller NZ (2017) ‘The Local Environmental Costs of Coal Procurement at U.S. Power Plants; ’, p. 64. [Google Scholar]
- Johnson NP et al. (2020) ‘A Multiregion Analysis of Shale Drilling Activity and Rates of Sexually Transmitted Infections in the United States’, Sexually Transmitted Diseases, 47(4), pp. 254–260. doi: 10.1097/OLQ.0000000000001127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly S, Johnson GT and Harbison RD (2016) ‘“Pressured to prescribe” The impact of economic and regulatory factors on South-Eastern ED physicians when managing the drug seeking patient’, Journal of Emergencies, Trauma, and Shock, 9(2), pp. 58–63. doi: 10.4103/0974-2700.179454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keyes KM et al. (2013) ‘Understanding the Rural–Urban Differences in Nonmedical Prescription Opioid Use and Abuse in the United States’, American Journal of Public Health, 104(2), pp. e52–e59. doi: 10.2105/AJPH.2013.301709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knittel CR, Metaxoglou K and Trindade A (2015) Natural Gas Prices and Coal Displacement: Evidence from Electricity Markets. Working Paper 21627. National Bureau of Economic Research. doi: 10.3386/w21627. [DOI] [Google Scholar]
- Koh K (2018) ‘The Great Recession and Workers’ Health Benefits’, Journal of Health Economics, 58, pp. 18–28. doi: 10.1016/j.jhealeco.2018.01.003. [DOI] [PubMed] [Google Scholar]
- Komarek T (2018) ‘Crime and natural resource booms: evidence from unconventional natural gas production’, The Annals of Regional Science, 61(1), pp. 113–137. doi: 10.1007/s00168-018-0861-x. [DOI] [Google Scholar]
- Komarek T and Cseh A (2017) ‘Fracking and public health: Evidence from gonorrhea incidence in the Marcellus Shale region’, Journal of Public Health Policy, pp. 1–18. doi: 10.1057/s41271-017-0089-5. [DOI] [PubMed] [Google Scholar]
- Kuehn BM (2007) ‘Opioid Prescriptions Soar’, JAMA, 297(3), pp. 249–251. doi: 10.1001/jama.297.3.249. [DOI] [PubMed] [Google Scholar]
- Larochelle MR et al. (2021) ‘Disparities in Opioid Overdose Death Trends by Race/Ethnicity, 2018–2019, From the HEALing Communities Study’, American Journal of Public Health, 111(10), pp. 1851–1854. doi: 10.2105/AJPH.2021.306431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee JO et al. (2015) ‘Unemployment and substance use problems among young adults: Does childhood low socioeconomic status exacerbate the effect?’, Social Science & Medicine, 143, pp. 36–44. doi: 10.1016/j.socscimed.2015.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindo JM (2015) ‘Aggregation and the estimated effects of economic conditions on health’, Journal of Health Economics, 40, pp. 83–96. doi: 10.1016/j.jhealeco.2014.11.009. [DOI] [PubMed] [Google Scholar]
- Litovitz A et al. (2013) ‘Estimation of regional air quality damages from Marcellus Shale natural gas extraction in Pennsylvania’, Environmental Research Letters, 8(1). [Google Scholar]
- Lleras-Muney A and Moreau FE (2020) A Unified Model of Cohort Mortality for Economic Analysis. w28193. National Bureau of Economic Research. doi: 10.3386/w28193. [DOI] [Google Scholar]
- Marchand J (2012) ‘Local labor market impacts of energy boom-bust-boom in Western Canada’, Journal of Urban Economics, 71(1), pp. 165–174. doi: 10.1016/j.jue.2011.06.001. [DOI] [Google Scholar]
- Martin Bassols N and Vall Castelló J (2016) ‘Effects of the great recession on drugs consumption in Spain’, Economics & Human Biology, 22, pp. 103–116. doi: 10.1016/j.ehb.2016.03.005. [DOI] [PubMed] [Google Scholar]
- Mason KL et al. (2015) ‘Occupational Fatalities During the Oil and Gas Boom — United States, 2003–2013’, MMWR. Morbidity and Mortality Weekly Report, 64(20), pp. 551–554. [PMC free article] [PubMed] [Google Scholar]
- McKenzie LM et al. (2017) ‘Childhood hematologic cancer and residential proximity to oil and gas development’, PLOS ONE, 12(2), p. e0170423. doi: 10.1371/journal.pone.0170423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McWilliams L et al. (2012) National Survey of the Mining Population, Part 1: Employees. IC 9527. Centers for Disease Control and Prevention, Department of Health and Human Services. [Google Scholar]
- Metcalf GE and Wang Q (2019) Abandoned by Coal, Swallowed by Opioids? Working Paper 26551. National Bureau of Economic Research. doi: 10.3386/w26551. [DOI] [Google Scholar]
- Monnat SM and Rigg KK (2016) ‘Examining Rural/Urban Differences in Prescription Opioid Misuse Among US Adolescents’, The Journal of Rural Health, 32(2), pp. 204–218. doi: 10.1111/jrh.12141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris A, Kaufman N and Doshi S (2019) The Risk of Fiscal Collapse in Coal-Reliant Communities. Center on Global Energy Policy, Columbia University. [Google Scholar]
- Nagelhout GE et al. (2017) ‘How economic recessions and unemployment affect illegal drug use: A systematic realist literature review’, International Journal of Drug Policy, 44, pp. 69–83. doi: 10.1016/j.drugpo.2017.03.013. [DOI] [PubMed] [Google Scholar]
- Newell RG and Raimi D (2018) ‘The fiscal impacts of increased U.S. oil and gas development on local governments’, Energy Policy, 117, pp. 14–24. doi: 10.1016/j.enpol.2018.02.042. [DOI] [Google Scholar]
- Noelke C et al. (2019) ‘Economic Downturns and Inequities in Birth Outcomes: Evidence From 149 Million US Births’, American Journal of Epidemiology, 188(6), pp. 1092–1100. doi: 10.1093/aje/kwz042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- OBrien R, Venkataramani A and Bair E (2021) ‘Death by Robots? Automation and Working-Age Mortality in the United States’. SocArXiv. doi: 10.31235/osf.io/8crze. [DOI] [PubMed] [Google Scholar]
- Olmstead SM et al. (2013) ‘Shale gas development impacts on surface water quality in Pennsylvania’, Proceedings of the National Academy of Sciences of the United States of America, 110(13), pp. 4962–4967. doi: 10.1073/pnas.1213871110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osborn SG et al. (2011) ‘Methane contamination of drinking water accompanying gas-well drilling and hydraulic fracturing’, Proceedings of the National Academy of Sciences, 108(20), pp. 8172–8176. doi: 10.1073/pnas.1100682108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palamar JJ et al. (2016) ‘Nonmedical opioid use and heroin use in a nationally representative sample of us high school seniors’, Drug and Alcohol Dependence, 158, pp. 132–138. doi: 10.1016/j.drugalcdep.2015.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paulozzi LJ and Xi Y (2008) ‘Recent changes in drug poisoning mortality in the United States by urban–rural status and by drug type’, Pharmacoepidemiology and Drug Safety, 17(10), pp. 997–1005. doi: 10.1002/pds.1626. [DOI] [PubMed] [Google Scholar]
- Pei Z, Pischke J-S and Schwandt H (2019) ‘Poorly Measured Confounders are More Useful on the Left than on the Right’, Journal of Business & Economic Statistics, 37(2), pp. 205–216. doi: 10.1080/07350015.2018.1462710. [DOI] [Google Scholar]
- Peng L, Meyerhoefer C and Chou S-Y (2018) ‘The health implications of unconventional natural gas development in Pennsylvania’, Health Economics [Preprint]. doi: 10.1002/hec.3649. [DOI] [PubMed] [Google Scholar]
- Pickenpaugh GC and Adder J (2018) Shale gas production and labor market trends in the U.S. Marcellus–Utica region over the last decade : Monthly Labor Review: U.S. Bureau of Labor Statistics, BLS.gov. Available at: https://www.bls.gov/opub/mlr/2018/article/shale-gas-production-and-labor-market-trends-in-the-us-marcellus-utica-region-over-the-last-decade.htm#_edn7 (Accessed: 18 December 2021). [Google Scholar]
- Pierce JR and Schott PK (2020) ‘Trade Liberalization and Mortality: Evidence from US Counties’, American Economic Review: Insights, 2(1), pp. 47–64. doi: 10.1257/aeri.20180396. [DOI] [Google Scholar]
- Pletcher MJ et al. (2008) ‘Trends in Opioid Prescribing by Race/Ethnicity for Patients Seeking Care in US Emergency Departments’, JAMA, 299(1), pp. 70–78. doi: 10.1001/jama.2007.64. [DOI] [PubMed] [Google Scholar]
- Potera C (2019) ‘Black Lung Disease Resurges in Appalachian Coal Miners’, AJN The American Journal of Nursing, 119(4), p. 14. doi: 10.1097/01.NAJ.0000554534.63115.c4. [DOI] [PubMed] [Google Scholar]
- Price JW (2012) ‘Comparison of Random and Postaccident Urine Drug Tests in Southern Indiana Coal Miners’, Journal of Addiction Medicine, 6(4), p. 253. doi: 10.1097/ADM.0b013e318266a8d5. [DOI] [PubMed] [Google Scholar]
- Reardon J (1993) ‘Injuries and illnesses among bituminous and lignite coal miners’, Monthly Labor Review, October 1993, pp. 49–55. [Google Scholar]
- Rees D et al. (2017) ‘With a Little Help from My Friends: The Effects of Naloxone Access and Good Samaritan Laws on Opioid-Related Deaths’, The National Bureau of Economic Research [Preprint]. Available at: https://www.nber.org/papers/w23171 (Accessed: 16 December 2019).
- Rickman DS, Wang H and Winters JV (2017) ‘Is shale development drilling holes in the human capital pipeline?’, Energy Economics, 62, pp. 283–290. doi: 10.1016/j.eneco.2016.12.013. [DOI] [Google Scholar]
- Rosenblum A et al. (2007) ‘Prescription opioid abuse among enrollees into methadone maintenance treatment’, Drug and Alcohol Dependence, 90(1), pp. 64–71. doi: 10.1016/j.drugalcdep.2007.02.012. [DOI] [PubMed] [Google Scholar]
- Ruddell R (2017) ‘Violence Toward Women: A Boom for Whom?’, in Ruddell R (ed.) Oil, Gas, and Crime: The Dark Side of the Boomtown. New York: Palgrave Macmillan US, pp. 69–91. doi: 10.1057/978-1-137-58714-5_4. [DOI] [Google Scholar]
- Ruhm CJ (2000) ‘Are Recessions Good for Your Health?’, The Quarterly Journal of Economics, 115(2), pp. 617–650. doi: 10.1162/003355300554872. [DOI] [Google Scholar]
- Ruhm CJ (2015) ‘Recessions, healthy no more?’, Journal of Health Economics, 42, pp. 17–28. doi: 10.1016/j.jhealeco.2015.03.004. [DOI] [PubMed] [Google Scholar]
- Ruhm CJ (2016) ‘Health effects of economic crises’, Health Economics, 25, pp. 6–24. [DOI] [PubMed] [Google Scholar]
- Ruhm CJ (2017) ‘Geographic Variation in Opioid and Heroin Involved Drug Poisoning Mortality Rates’, American Journal of Preventive Medicine, 53(6), pp. 745–753. doi: 10.1016/j.amepre.2017.06.009. [DOI] [PubMed] [Google Scholar]
- Ruhm CJ (2019) ‘Drivers of the fatal drug epidemic’, Journal of Health Economics, 64, pp. 25–42. doi: 10.1016/j.jhealeco.2019.01.001. [DOI] [PubMed] [Google Scholar]
- Scutchfield FD and Keck CW (2017) ‘Deaths of Despair: Why? What to Do?’, American Journal of Public Health, 107(10), pp. 1564–1565. doi: 10.2105/AJPH.2017.303992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sinha R (2008) ‘Chronic Stress, Drug Use, and Vulnerability to Addiction’, Annals of the New York Academy of Sciences, 1141(1), pp. 105–130. doi: 10.1196/annals.1441.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein EM et al. (2017) ‘The Epidemic of Despair Among White Americans: Trends in the Leading Causes of Premature Death, 1999–2015’, American Journal of Public Health, 107(10), pp. 1541–1547. doi: 10.2105/AJPH.2017.303941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens AH et al. (2015) ‘The Best of Times, the Worst of Times: Understanding Pro-cyclical Mortality’, American Economic Journal: Economic Policy, 7(4), pp. 279–311. doi: 10.1257/pol.20130057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsvetkova A and Partridge MD (2016) ‘Economics of modern energy boomtowns: Do oil and gas shocks differ from shocks in the rest of the economy?’, Energy Economics, 59, pp. 81–95. doi: 10.1016/j.eneco.2016.07.015. [DOI] [Google Scholar]
- U.S. Department of Energy (2017) U.S. Energy and Employment Report.
- U.S. Energy Information Administration (1997) The Effects of Title IV of the Clean Air Act Amendments of 1990 on Electric Utilities: An Update. Available at: https://www.eia.gov/electricity/pdfpages/titleivcaa/index.php (Accessed: 13 March 2019).
- Van Zee A (2009) ‘The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy’, American Journal of Public Health, 99(2), pp. 221–227. doi: 10.2105/AJPH.2007.131714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venkataramani AS et al. (2020) ‘Association Between Automotive Assembly Plant Closures and Opioid Overdose Mortality in the United States: A Difference-in-Differences Analysis’, JAMA Internal Medicine, 180(2), pp. 254–262. doi: 10.1001/jamainternmed.2019.5686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Villapiano NLG et al. (2017) ‘Rural and Urban Differences in Neonatal Abstinence Syndrome and Maternal Opioid Use, 2004 to 2013’, JAMA Pediatrics, 171(2), pp. 194–196. doi: 10.1001/jamapediatrics.2016.3750. [DOI] [PubMed] [Google Scholar]
- Wang Z and Krupnick A (2015) ‘A Retrospective Review of Shale Gas Development in the United States: What Led to the Boom?’, Economics of Energy & Environmental Policy, 4(1), pp. 5–18. [Google Scholar]
- Warner M et al. (2013) ‘State Variation in Certifying Manner of Death and Drugs Involved in Drug Intoxication Deaths’, Academic Forensic Pathology, 3(2), pp. 231–237. doi: 10.23907/2013.029. [DOI] [Google Scholar]
- Weber JG (2019) ‘How Should We Think about Environmental Policy and Jobs? An Analogy with Trade Policy and an Illustration from U.S. Coal Mining’, Review of Environmental Economics and Policy [Preprint]. doi: 10.1093/reep/rez016. [DOI] [Google Scholar]
- Wilson R (2020) ‘Moving to Economic Opportunity: The Migration Response to the Fracking Boom’, Journal of Human Resources, pp. 0817–8989R2. doi: 10.3368/jhr.57.3.0817-8989R2. [DOI] [Google Scholar]
- Wilson R (2021) ‘Moving to jobs: The role of information in migration decisions’, Journal of Labor Economics, 39(4), pp. 1083–1128. [Google Scholar]
- Witter RZ et al. (2014) ‘Occupational exposures in the oil and gas extraction industry: State of the science and research recommendations’, American Journal of Industrial Medicine, 57(7), pp. 847–856. doi: 10.1002/ajim.22316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young AM, Havens JR and Leukefeld CG (2012) ‘A Comparison of Rural and Urban Nonmedical Prescription Opioid Users’ Lifetime and Recent Drug Use’, The American Journal of Drug and Alcohol Abuse, 38(3), pp. 220–227. doi: 10.3109/00952990.2011.643971. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.