

Abstract
Balo's disease is an uncommon central nervous system disorder causing demyelination and is a form of multiple sclerosis. Concentric sclerosis, leukoencephalitis periaxialis concentrica, is also known as Balo's disease. Concentric sclerosis signalizes the bands of intact myelin and alternating rings of myelin loss present in several parts of the brainstem and brain. The present study aimed to assess and create awareness about Balo's disease among dental undergraduates. The study included an online survey about the knowledge and awareness of Balo's disease among dental students. A questionnaire was prepared, uploaded, and distributed in an online portal. The latest software version of SPSS was used to analyze the collected data. Descriptive statistical analysis and Chi-square test were done, and the P value was calculated. The survey showed that 54.55% of males and 45.45% of females participated in this survey. Most of the respondents (87.88%) knew about Balo's disease, whereas only 12.12% of participants were not aware of the disease. It was found that most of dental students are aware of Balo's disease. The study also showed that male respondents are more aware than the females.
Keywords: Balo's disease, concentric sclerosis, dental students, innovative technique, magnetic resonance imaging, novel method
INTRODUCTION
Balo's disease is an uncommon central nervous system disease causing demyelination and is an alternative form of multiple sclerosis. Concentric sclerosis, leukoencephalitis periaxialis concentrica, is also known as Balo's disease.[1] Concentric sclerosis signalizes the bands of intact myelin and alternating rings of myelin loss present in several parts of the brainstem and brain. The concentric pattern is observed on magnetic resonance imaging (MRI).[2] Balo's disease is normally found in adulthood, but it is also seen in childhood. The causes of multiple sclerosis and its alternative forms remain unrevealed. Moreover, certain studies suggested that autoimmune factors have a key role in Balo's disease.[3] Autoimmune disorders referred to as the body's natural defense mechanism start to attack healthy tissue. They are distinguished by the gradual appearance of symptoms that are found in the most common types of multiple sclerosis which include muscle spasms, headache, seizures, and paralysis. Further neurological manifestations develop mainly in brain areas that may cause physiological abnormalities.[4]
Symptoms of Balo's disease are unknown and it varies from individual to individual. It depends on the areas affected in the region of the brain. Duration of symptoms of Balo's disease may appear within a few weeks to years.[5] Males and females are most likely to be affected equally. Balo's disease is clinically indicated in clinical trials as that of multiple sclerosis. It shows that a few symptoms such as altered behavior and focal central nervous system may be seen along with the disease. The clinical trials reported that corticosteroids, which are anti-inflammatory, are effective against Balo's concentric sclerosis and its deficits.[6]
Injury can also occur in the brain stem, basal ganglion, pons cerebellum, and rarely in the spinal cord and most of them are seen in temporal and frontal lobes. The appearance of the lesions might be small or large which covers bigger sections of the cerebral hemisphere that is more than 2 cm in size when viewed under MRI, whereas histologically, it appears to be the rings of myelination which can be normal or partial that are related to areas of T2 intensity.[7]
The lesions related to multiple sclerosis resemble blotches or spots, while that in Balo's disease can be seen as bull’s-eye marks. Hence, Balo's disease is often referred to as Balo's concentric sclerosis, in which bull’s-eye-shaped scars are concentric rings. In many studies, it has reported that concentric ring appearance is not specific in patients with multifocal leukoencephalopathy and neuromyelitis.[8]
Balo's disease exists in three forms: acute and self-limiting, relapsing-remitting variant, and rapidly progressive primary disease. Diagnosis of the lesion under a lumbar puncture by cerebrospinal fluid (CSF) shows mild mononuclear inflammatory reaction and shows negative for CSF-restricted oligoclonal bands. Lesions in autopsy and biopsy show that inflammation increased lactate and anisotropy. MRI scan shows the alternating hypointense and hyperintense layers and myelin percentage of water content.[9]
The disease is more common in Asia and the Philippines than in India. Treatment is done only to relieve the inflammation by administering corticosteroids and there is no permanent cure for the disease which mostly leads to fatal.[10] Our team has deep knowledge and extensive research experience, which helped to produce several publications of high quality.[11,12,13,14,15,16,17,18,19,20,21,22,23,24] As Balo's disease is a rare disease, the study aimed to assess and create awareness among students about this disease.
MATERIALS AND METHODS
An online survey on the awareness and knowledge on Balo's disease was circulated among 100 dental undergraduates. The study was carried out during the period from January–March 2021. A set of 15 questions containing a questionnaire was prepared on symptoms, causes, diagnosis, and treatment modalities of Balo's disease. Then, through Google Forms, the questionnaire was uploaded that can facilitate the distribution of questionnaires through E-mail; using applications such as WhatsApp in smartphones and social media platforms, such as Instagram. Thus, the survey questionnaire reached the participants easily, and the results have been collected. The collected data were analyzed statistically using the latest version of SPSS (IBM, India). Chi-square test and Pearson correlation analysis were used, with P < 0.05 considered to be statistically significant.
RESULTS
The survey responses showed that 54.55% of the respondents were males and 45.45% were females [Figure 1]. About 87.88% of the respondents were aware of this disease, whereas 12.12% of respondents were not aware [Figure 2]. Figure 3 shows that 56.7% of respondents reported infections cause Balo's disease, 38.5% reported that Balo's disease is affected by medications, and 9.1% of respondents replied that the disease is related to cancers. The organs affected in Balo's disease are the brain, in which 46.2% reported it, whereas 47% of respondents reported skin is also affected [Figure 4]. From a total of 100 respondents, symptoms of Balo's disease are fever and headache (53.92%), muscle spasms (29.4%), and paralysis (10.78%) [Figure 5]. The disease is mostly seen in 48.4% of men and 42.4% of women [Figure 6]. Figure 7 shows that the majority of respondents say that it is an autoimmune disease of 84.8%. The most common age group affected is above 50 years of 45.4% and an equal percentage of 6.06% is seen in both 10–20 years and 20–50 years, respectively, as shown in Figure 8. Figure 9 shows 63.6% of respondents saying that Balo's disease is a genetic disease and 21.2% say that Balo's disease is caused by both genetic and inherited disease. The majority of respondents say that corticosteroids (66.6%) are used as medication, whereas only 33.3% say nonsteroidal anti-inflammatory drugs (NSAIDs) are used [Figure 10]. The duration of Balo's disease is 2–4 weeks of 48.4%, 6 months of 36.3%, and 12.1% is 2–3 years [Figure 11]. The respondents say that MRI (48.4%), blood (36.3%), and physical examination (9.09%) are shown in Figure 12. Figure 13 shows the treatment of Balo's disease is treated mainly by medications (48.4%), intravenous immunoglobulin (45.4%), and chemotherapy (3.03%).
Figure 1.

The figure shows the gender of the participants. Blue denotes males (66.34%) and green denotes females (33.66%)
Figure 2.
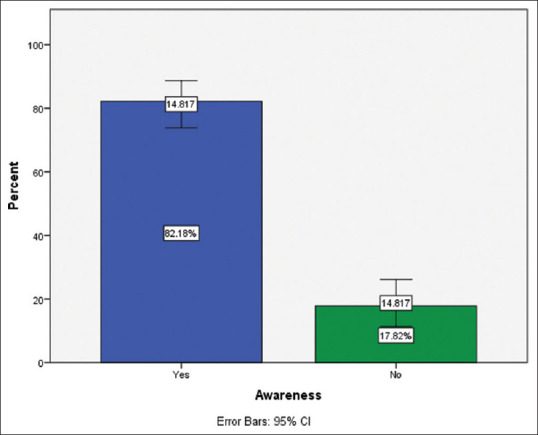
The bar graph represents the awareness of Balo's disease. Where blue denotes yes (82.1%) and green denotes no (17.82%)
Figure 3.

The figure shows the causes of Balo's disease
Figure 4.

The figure shows the distribution of areas affected in Balo's disease
Figure 5.

The figure shows the symptoms of Balo's disease
Figure 6.

The figure shows the percentage distribution of gender affected in Balo's disease
Figure 7.

The figure shows the percentage distribution awareness on Balo's disease as an autoimmune disease
Figure 8.

The figure shows the age group affected in Balo's disease
Figure 9.

The figure shows the distribution of whether Balo's disease is genetic or inherited
Figure 10.

The figure shows the awareness on the medications used in Balo's disease
Figure 11.

The figure shows the awareness on the durations of Balo's disease
Figure 12.

The figure shows the awareness on the diagnosis of Balo's disease
Figure 13.

The figure shows the awareness on the treatment for Balo's disease
The association graphs showed that males (42.4%) are more aware of Balo's disease than females (45.4%) [Figure 14]. The majority of males (36.3%) say Balo's disease is more contagious than females (45.4%) [Figure 15]. Figure 16 shows that 36.5% of females and 30.6% of males said that the brain is the most common affected area. The majority of females (27.2%) said 2–4 weeks, whereas 21.2% of males replied 2–4 weeks as the duration of the disease [Figure 17].
Figure 14.

The figure shows the association between gender and awareness of Balo's disease. X-axis indicates gender and Y-axis indicates the number of responses. Chi-square test value is 2.98, P = 0.39 (P > 0.05) hence it is not significant statistically
Figure 15.

The figure shows the association of gender with communicability of Balo's disease. X-axis indicates gender and Y-axis indicates number of responses. Chi-square test value is 0.31, P = 0.86 (P > 0.05) hence it is not significant statistically
Figure 16.

The figure shows the association of gender with areas affected in Balo's disease. X-axis represents gender and the Y-axis represents the number of responses. Chi-square test value is 0.11, P = 0.73 (P > 0.05) hence it is not significant statistically
Figure 17.

The figure shows the association of gender with the duration of Balo's disease. X-axis represents gender and the Y-axis represents the number of responses. Chi-square test value is 0.58, P = 0.44 (P > 0.05), hence it is not significant statistically
DISCUSSION
The current survey showed that 87.88% of students knew about Balo's disease, however, a similar study done by Pessini et al. reported that the majority of students does not know about the disease.[25]
The prime cause of Balo's disease is idiopathic, a study by Link and Tibbling says that Balo's is linked to infection based on symptoms such as fever and headache which are the earliest symptoms of the condition.[26] The majority of studies indicated that the cause of the disease is not yet known. In this study, respondents say that 56.7% of respondents reported infections cause Balo's disease, 38.5% reported that Balo's disease is due to medications, and 9.1% of respondents said that the disease is linked to cancers.
The majority of students responded that symptoms of Balo's disease include painful bumps on arms, neck, and legs (27.27%), erythematous (48.48%), and conjunctivitis (24.24%). A study by Reiber et al. suggests that in some cases, there is a gradual occurrence of symptoms which comprises paralysis and muscle spasms. Moreover, neurological symptoms can also develop based on the brain area affected and may have an intellectual impairment and/or physiological abnormalities, whereas in severe cases, shows the presence of infections starting with fever and headache.[27] In this study, the majority of the population says that the brain is the common area affected in Balo's disease. A study done also says that Balo's disease affected in various parts of the brain and brainstem.[28]
Another study says that autoimmune factors have a key role in the progression of Balo disease.[29] Several anatomical, physicochemical, and cytotoxic theories have been suggested, to elucidate the development of the typical lesions in Balo's disease, the latest one is the theory of tissue preconditioning, explained by Stadelmann et al.[2]
About 66.6% of the respondents said that the medication used for the disease is corticosteroids, while only 33.3% replied as NSAIDs. A previous study showed that corticosteroids help to treat multiple sclerosis to reduce swelling in the brain and tissues of the spinal cord. Corticosteroids through their anti-inflammatory action reduce the acute presentation severity. Childhood cases of Balo's disease have also been reported in Behrens et al.[30] The most common age group affected is above 50 years of 45.4% and an equal percentage of 6.06% is seen in both 10–20 years and 20–50 years, respectively. Lesions of Balo's disease under MRI are distinctive which shows the concentric shape, in the CSF test, patients with lesions show negative for CSF.[31] In this study, the respondents said that MRI (48.4%), blood (36.3%), and physical examination (9.09%) are the methods of diagnosis of this disease. Balo's disease is a very rare disease, it is a variant of multiple sclerosis, in which investigations are going on.
Limitations
Reduced size of the sample and unwillingness of many of the respondents and inaccurate responses that might have an impact on the study.
Future scope
With a larger sample size and inclusion of different types of populations, the study can be used to expand awareness about the disease.
CONCLUSIONS
The study can be concluded that the majority of the dental students were aware of Balo's disease, in which male students are more aware than females.
Financial support and sponsorship
The present project is sponsored by:
Saveetha institute of medical and technical sciences
Saveetha Dental College and Hospitals, Saveetha University
Satyam G land developers.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank the Saveetha Institute, Department of Biochemistry and Management for providing a platform and kind cooperation throughout the study.
REFERENCES
- 1.Mowry EM, Woo JH, Ances BM. Baló's concentric sclerosis presenting as a stroke-like syndrome. Nat Clin Pract Neurol. 2007;3:349–54. doi: 10.1038/ncpneuro0522. [DOI] [PubMed] [Google Scholar]
- 2.Stadelmann C, Ludwin S, Tabira T, Guseo A, Lucchinetti CF, Leel-Ossy L, et al. Tissue preconditioning may explain concentric lesions in Baló's type of multiple sclerosis. Brain. 2005;128:979–87. doi: 10.1093/brain/awh457. [DOI] [PubMed] [Google Scholar]
- 3.Kreft KL, Mellema SJ, Hintzen RQ. Spinal cord involvement in Balo's concentric sclerosis. J Neurol Sci. 2009;279:114–7. doi: 10.1016/j.jns.2008.12.030. [DOI] [PubMed] [Google Scholar]
- 4.Xie P, Fan X, Tang H, Li Y. Balò′s concentric sclerosis presenting with benign clinical course and multiple sclerosis-like lesions on magnetic resonance images. Neurol India. 2009;57:66. doi: 10.4103/0028-3886.48815. [DOI] [PubMed] [Google Scholar]
- 5.Moore GR, Berry K, Oger JJ, Prout AJ, Graeb DA, Nugent RA. Baló's concentric sclerosis: Surviving normal myelin in a patient with a relapsing-remitting dinical course. Mult Scler. 2001;7:375–82. doi: 10.1177/135245850100700606. [DOI] [PubMed] [Google Scholar]
- 6.Dreha-Kulaczewski SF, Helms G, Dechent P, Hofer S, Gärtner J, Frahm J. Serial proton MR spectroscopy and diffusion tensor imaging in infantile Balo's concentric sclerosis. Neuroradiology. 2009;51:113–21. doi: 10.1007/s00234-008-0470-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rovira A. Tissue-specific MR imaging in multiple sclerosis. AJNR Am J Neuroradiol. 2009;30:1277–8. doi: 10.3174/ajnr.A1777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Iannucci G, Mascalchi M, Salvi F, Filippi M. Vanishing Balò-like lesions in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2000;69:399–400. doi: 10.1136/jnnp.69.3.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Singh S, Kuruvilla A, Alexander M, Korah IP. Balo's concentric sclerosis: Value of magnetic resonance imaging in diagnosis. Australas Radiol. 1999;43:400–4. doi: 10.1046/j.1440-1673.1999.433700.x. [DOI] [PubMed] [Google Scholar]
- 10.Yao DL, Webster HD, Hudson LD, Brenner M, Liu DS, Escobar AI, et al. Concentric sclerosis (Baló): Morphometric and in situ hybridization study of lesions in six patients. Ann Neurol. 1994;35:18–30. doi: 10.1002/ana.410350105. [DOI] [PubMed] [Google Scholar]
- 11.Jain RK, Kumar SP, Manjula WS. Comparison of intrusion effects on maxillary incisors among mini implant anchorage, j-hook headgear and utility arch. J Clin Diagn Res. 2014;8:ZC21–4. doi: 10.7860/JCDR/2014/8339.4554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Keerthana B, Thenmozhi MS. Occurrence of foramen of huschke and its clinical significance. Res J Pharm Technol. 2016;9:1835–6. [Google Scholar]
- 13.Thejeswar EP. Educational research-iPad system vs. textbook system. Res J Pharm Technol. 2015;8:1158–60. [Google Scholar]
- 14.Krishna RN, Nivesh Krishna R, Yuvaraj Babu K. Estimation of stature from physiognomic facial length and morphological facial length. Res J Pharm Technol. 2016;9:2071. [Google Scholar]
- 15.Muthukrishnan S, Krishnaswamy H, Thanikodi S, Sundaresan D, Venkatraman V. Support vector machine for modelling and simulation of heat exchangers. Thermal Sci. 2020;24:499–503. [Google Scholar]
- 16.Nandhini NT, Rajeshkumar S, Mythili S. The possible mechanism of eco-friendly synthesized nanoparticles on hazardous dyes degradation. Biocatal Agric Biotechnol. 2019;19:101138. [Google Scholar]
- 17.Ezhilarasan D. Oxidative stress is bane in chronic liver diseases: Clinical and experimental perspective. Arab J Gastroenterol. 2018;19:56–64. doi: 10.1016/j.ajg.2018.03.002. [DOI] [PubMed] [Google Scholar]
- 18.Rajagopal R, Padmanabhan S, Gnanamani J. A comparison of shear bond strength and debonding characteristics of conventional, moisture-insensitive, and self-etching primers in vitro. Angle Orthod. 2004;74:264–8. doi: 10.1043/0003-3219(2004)074<0264:ACOSBS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 19.Neelakantan P, Sharma S, Shemesh H, Wesselink PR. Influence of irrigation sequence on the adhesion of root canal sealers to dentin: A Fourier transform infrared spectroscopy and push-out bond strength analysis. J Endod. 2015;41:1108–11. doi: 10.1016/j.joen.2015.02.001. [DOI] [PubMed] [Google Scholar]
- 20.Sahu D, Kannan GM, Vijayaraghavan R. Carbon black particle exhibits size dependent toxicity in human monocytes. Int J Inflam 2014. 2014:827019. doi: 10.1155/2014/827019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jose J, Palanivelu A, Subbaiyan H. Different treatment modalities followed by dental practitioners for Ellis class 2 fracture –A Questionnaire-based Survey. Open Dent J. 2020;14:59–65. [Google Scholar]
- 22.Wu F, Zhu J, Li G, Wang J, Veeraraghavan VP, Krishna Mohan S, et al. Biologically synthesized green gold nanoparticles from Siberian ginseng induce growth-inhibitory effect on melanoma cells (B16) Artif Cells Nanomed Biotechnol. 2019;47:3297–305. doi: 10.1080/21691401.2019.1647224. [DOI] [PubMed] [Google Scholar]
- 23.Dua K, Wadhwa R, Singhvi G, Rapalli V, Shukla SD, Shastri MD, et al. The potential of siRNA based drug delivery in respiratory disorders: Recent advances and progress. Drug Dev Res. 2019;80:714–30. doi: 10.1002/ddr.21571. [DOI] [PubMed] [Google Scholar]
- 24.Patil SB, Durairaj D, Suresh Kumar G, Karthikeyan D, Pradeep D. Comparison of extended nasolabial flap versus buccal fat pad graft in the surgical management of oral submucous fibrosis: A prospective pilot study. J Maxillofac Oral Surg. 2017;16:312–21. doi: 10.1007/s12663-016-0975-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pessini LM, Kremer S, Auger C, Castilló J, Pottecher J, de Sèze J, et al. Tumefactive inflammatory leukoencephalopathy in cocaine users: Report of three cases. Mult Scler Relat Disord. 2020;38:101496. doi: 10.1016/j.msard.2019.101496. [DOI] [PubMed] [Google Scholar]
- 26.Link H, Tibbling G. Principles of albumin and IgG analyses in neurological disorders. III. Evaluation of IgG synthesis within the central nervous system in multiple sclerosis. Scand J Clin Lab Invest. 1977;37:397–401. doi: 10.1080/00365517709091498. [DOI] [PubMed] [Google Scholar]
- 27.Reiber H, Teut M, Pohl D, Rostasy KM, Hanefeld F. Paediatric and adult multiple sclerosis: Age-related differences and time course of the neuroimmunological response in cerebrospinal fluid. Mult Scler. 2009;15:1466–80. doi: 10.1177/1352458509348418. [DOI] [PubMed] [Google Scholar]
- 28.Jarius S, König FB, Metz I, Ruprecht K, Paul F, Brück W, et al. Pattern II and pattern III MS are entities distinct from pattern I MS: Evidence from cerebrospinal fluid analysis. J Neuroinflammation. 2017;14:171. doi: 10.1186/s12974-017-0929-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Grüter T, Metz I, Gahlen A, Kneiphof J, Stork L, Brück W, et al. Mitoxantrone treatment in a patient with multiple sclerosis and pattern III lesions. Clin Exp Neuroimmunol. 2018;9:169–72. [Google Scholar]
- 30.Behrens JR, Wanner J, Kuchling J, Ostendorf L, Harms L, Ruprecht K, et al. 7 Tesla MRI of Balo's concentric sclerosis versus multiple sclerosis lesions. Ann Clin Transl Neurol. 2018;5:900–12. doi: 10.1002/acn3.572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Jolliffe EA, Guo Y, Hardy TA, Pearse Morris P, Flanagan EP, Lucchinetti CF, et al. Clinical and radiologic features, pathology, and treatment of Balóconcentric sclerosis. Neurology. 2021;97:e414–22. doi: 10.1212/WNL.0000000000012230. [DOI] [PMC free article] [PubMed] [Google Scholar]