

Abstract
Objective
To examine services delivered during preventive care visits among reproductive‐age women with and without chronic conditions by physician specialty.
Data Sources
National Ambulatory Medical Care Surveys (2011–2018).
Study Design
We examined provision of specific services during preventive care visits by physician specialty among reproductive‐age female patients, overall and among women with five common chronic conditions (diabetes, hypertension, depression, hyperlipidemia, and asthma).
Data Collection/Extraction Methods
The sample included preventive visits to OB/GYNs or generalist physicians where the patient was female, age 18–44, and not pregnant.
Principal Findings
In OB/GYN preventive visits, reproductive health services were more likely to be provided, while non‐reproductive health services were less likely to be provided, both among reproductive‐age female patients overall and among those with chronic conditions. For example, pap tests were provided in 44.5% of OB/GYN preventive visits (95% CI: 40.6–48.4) and in 21.4% of generalist preventive visits (95% CI: 17.2–26.6). Lipid testing was provided in 2.8% of OB/GYN preventive visits (95% CI: 1.7–3.9) and in 30.3% of generalist preventive visits (95% CI: 26.1–34.6).
Conclusions
Understanding the full range of care received in preventive visits across settings could guide recommendations to optimize where reproductive‐age women with chronic conditions seek care.
Keywords: chronic conditions, physician specialty, preventive care, reproductive health, women's health
What is known on this topic
A substantial proportion of reproductive‐age women receive preventive care from obstetrician‐gynecologists
The prevalence of chronic conditions among US adults is high, including among reproductive‐age women
Provision of specific services in preventive visits may vary by physician specialty and patient chronic condition status
What this study adds
OB/GYN preventive care visits include more reproductive‐related services and fewer other services relative to generalist physicians, including for patients with chronic conditions
Preventive visits with OB/GYNs were shorter on average than preventive visits with generalist physicians
Better understanding the full range of care received in preventive visits across settings by reproductive‐age women with chronic conditions can help guide recommendations to optimize where this population seeks care
1. INTRODUCTION
Preventive care is important for optimal health, 1 and the Affordable Care Act required that insurance plans cover certain preventive services with no cost sharing starting in September 2010. 2 Primary care providers are often conceptualized as the key source of preventive care for patients. 3 , 4 However, for women of reproductive age, obstetrician‐gynecologists (OB/GYNs) play a central role in preventive care provision, as they provide both preventive and specialized care 5 , 6 ; thus, OB/GYNs may be providing most or all of a woman's preventive care.
An estimated 60% of adults in the US have at least one chronic condition, with hypertension, mood disorders, hyperlipidemia, and diabetes among the most common. 7 Chronic conditions are also common among reproductive‐age women. 8 , 9 , 10 People with chronic conditions often require regular disease‐specific monitoring that may be different than general preventive care recommendations for all adults. 11 , 12 Certain chronic conditions are risk factors for future disease, which may increase the number and intensity of recommended screenings.
Despite the importance of preventive care, it is unclear to what extent reproductive‐age women with chronic conditions receive recommended preventive services from OB/GYNs versus generalist physicians. Guidance from the American College of Obstetricians and Gynecologists (ACOG) notes that annual well‐woman visits should include healthy lifestyle counseling and recommendations for reducing health risks, including topics such as tobacco use, cardiovascular disease, and weight management. 13 Similarly, the United States Preventive Services Task Force (USPSTF) has a number of counseling, screening, and medication recommendations for reproductive‐age women, particularly for those with chronic conditions that place them at higher risk of adverse outcomes of cardiovascular disease. 14
Prior studies comparing aspects of preventive health services delivery by generalist physicians and OB/GYNs for female patients have found that reproductive health services were more common in OB/GYN visits, 15 and that visits for female patients with OB/GYNs were less likely to include certain cardiovascular disease preventive care services. 16 However, these studies used data from prior to the implementation of the preventive services coverage provisions of the ACA, and neither assessed care by chronic condition status.
We aimed to examine services delivered nationally in preventive care visits for reproductive‐age women by physician specialty, with a specific focus on women with common chronic conditions.
2. METHODS
2.1. Data and sample
Data are from the National Ambulatory Medical Care Survey (NAMCS) from 2011 to 2018 (2017 data have not been released). The NAMCS is a national survey of office‐based physicians, which gathers data about physician and practice characteristics; for each physician, information from approximately 50 patient visits during a randomly selected week is abstracted from clinical records.
The analytic sample included visits where the patient was female, age 18–44, and not pregnant, and the major reason for visit was preventive care. For 2011–2016, the sample was further limited to visits with OB/GYNs or generalist physicians (internal medicine, family medicine, or pediatrics). The definition of “preventive care” visits is general medical examinations and routine periodic examinations, including annual physicals, screening, and insurance examinations. For some analyses, we further restricted the analytic sample to patients with specific chronic conditions, as described below.
2.2. Measures
Patients were coded as having one of five common chronic conditions (diabetes, hypertension, depression, hyperlipidemia, and asthma) if the condition was identified as present from medical records abstraction, regardless of relevance to the visit, or from International Classification of Diseases, Ninth Revision (ICD‐9) and ICD‐10 diagnosis codes (see Appendix 1).
Physician specialty (OB/GYN or generalist) was a key independent variable. This variable was not available in the 2018 data; the sample was limited to 2011–2016 data for analyses comparing visits by physician specialty.
Key outcome measures included services that may be provided as part of preventive care, including some universally recommended services, some recommended under certain circumstances only, and some commonly provided but not concordant with current guidelines. We created binary indicators for whether each service was provided, categorizing services as: (1) reproductive health related (Pap testing, pelvic exam, clinical breast exam, HPV testing, chlamydia testing, HIV testing, and contraceptive medication ordered or provided); (2) non‐reproductive health related (blood pressure measurement, depression screening, glucose testing, lipid testing, complete blood count, any medication ordered or provided, non‐contraceptive medication ordered or provided, and referral made during the visit); and (3) counseling topics (family planning, weight reduction, tobacco use/exposure, stress management, exercise, and diet/nutrition). Total time spent with the physician (in minutes, continuous) was also measured.
Covariates included patient characteristics (age category, race/ethnicity, and insurance type), physician characteristics (metropolitan statistical area practice location, census region, solo practice physician, and practice ownership), and visit characteristics (new or established patient visit, year of visit).
2.3. Analysis
We calculated descriptive statistics, then tabulated receipt of each service in preventive visits overall and by physician specialty. Finally, we estimated a multivariable regression model for each outcome by physician specialty, controlling for the covariates described above, as well as patient obesity. 17 Analyses were repeated for the overall sample and the sample limited to patients with chronic conditions.
As a sensitivity analysis, for certain services, we restricted the sample to visits with patients for whom the service was likely to be recommended and calculated the probability of services overall and by physician specialty. For tobacco use/exposure counseling, we limited to visits where the patient was a documented current tobacco user. For chlamydia screening (recommended for all sexually active women under age 25), 18 we limited the sample to patients under age 25. For weight reduction counseling, diet and nutrition counseling, and exercise counseling, we limited the sample to patients with documented obesity. 17
All analyses use visit weights constructed by the National Center for Health Statistics to make estimates representative of office‐based physician visits nationally; standard errors are adjusted for the complex survey design. Analyses were conducted in Stata version 17. This study was determined to not be human subjects research by the University of Massachusetts Amherst Institutional Review Board.
3. RESULTS
Table 1 shows characteristics of preventive care visits by reproductive‐age female patients (2011–2018). In the full sample (weighted N = 150,834,891 visits; unweighted n = 4445), 3.0% of visits were with patients who had diabetes, 6.1% hypertension, 7.6% depression, 3.5% hyperlipidemia, and 5.9% asthma. In 60.2% of visits, the patient was White, and in 75.1% of visits, the patient was privately insured. Among visits where the patient had at least one of the five chronic conditions (N = 31,384,151 visits, n = 876), 66.4% were for patients with private insurance.
TABLE 1.
Characteristics of preventive care visits by female patients age 18–44, National Ambulatory Medical Care Survey 2011–2016, 2018.
| Female patients age 18–44 (N = 150,834,891) a (%) | Female patients age 18–44 with diabetes, hypertension, depression, hyperlipidemia or asthma (N = 31,384,151) b (%) | |
|---|---|---|
| Chronic conditions | ||
| Diabetes | 3.0 | 14.6 |
| Hypertension | 6.1 | 29.4 |
| Depression | 7.6 | 36.3 |
| Hyperlipidemia | 3.5 | 16.7 |
| Asthma | 5.9 | 28.2 |
| Any chronic condition | 20.8 | 100.0 |
| Patient characteristics | ||
| Patient age | ||
| 18–24 | 21.7 | 14.4 |
| 25–29 | 17.4 | 16.6 |
| 30–34 | 26.2 | 26.1 |
| 35–39 | 14.4 | 17.0 |
| 40–44 | 20.2 | 26.0 |
| Patient race/ethnicity | ||
| Non‐Hispanic White | 60.2 | 58.1 |
| Non‐Hispanic Black | 14.5 | 20.7 |
| Hispanic | 16.9 | 12.0 |
| Non‐Hispanic Other | 8.3 | 9.2 |
| Insurance type | ||
| Private | 75.1 | 66.4 |
| Medicaid | 19.2 | 25.1 |
| Other | 5.6 | 8.5 |
| Physician characteristics | ||
| Located in metropolitan statistical area | 93.6 | 93.9 |
| Physician is in a solo practice | 34.3 | 32.9 |
| Practice ownership is physician or physician group | 80.2 | 78.6 |
| Visit characteristics | ||
| New (vs. established) patient | 17.2 | 17.6 |
Note: Data from 2017 are not available from the National Ambulatory Medical Care Survey. Visits are weighted to be representative of office‐based physician visits nationally.
Unweighted n = 4,445.
Unweighted n = 876.
Among preventive care visits for reproductive‐age female patients in 2011–2016, (N = 127,076,191; n = 4229), 39.1% of visits were to generalist physicians, while 60.9% were to OB/GYNs (not shown). Among preventive care visits where the patient had a chronic condition (N = 26,615,140 visits; n = 839), 56.1% were to generalist physicians, while 43.9% were to OB/GYNs.
Appendix 2 shows descriptive statistics for services provided at preventive care visits (2011–2016) by physician specialty. Service frequency varied widely by specific service. For example, blood pressure screening occurred at over 90% of preventive care visits, while stress management counseling and HIV testing occurred in less than 5% of preventive care visits.
There were substantial differences in the services provided by physician specialty in regression‐adjusted results (Figures 1 and 2). In the overall sample (2011–2016), reproductive health services including Pap testing, clinical breast exam, chlamydia testing, HPV testing, pelvic exam, and ordering or prescribing contraceptive medication were more likely in OB/GYN visits, as was family planning counseling (Figure 1, Panel A). Non‐reproductive health services including glucose testing, lipid testing, complete blood count, and ordering or prescribing non‐contraceptive medication were less likely in OB/GYN visits (Figure 1, Panel B), as were counseling on weight reduction, diet and nutrition counseling, and tobacco use/exposure (Figure 1, Panel C). OB/GYN visits were less likely to result in a referral, and time with physician was significantly shorter (difference of 2.3 min, 95% CI: −3.82, −0.76 for the overall sample).
FIGURE 1.
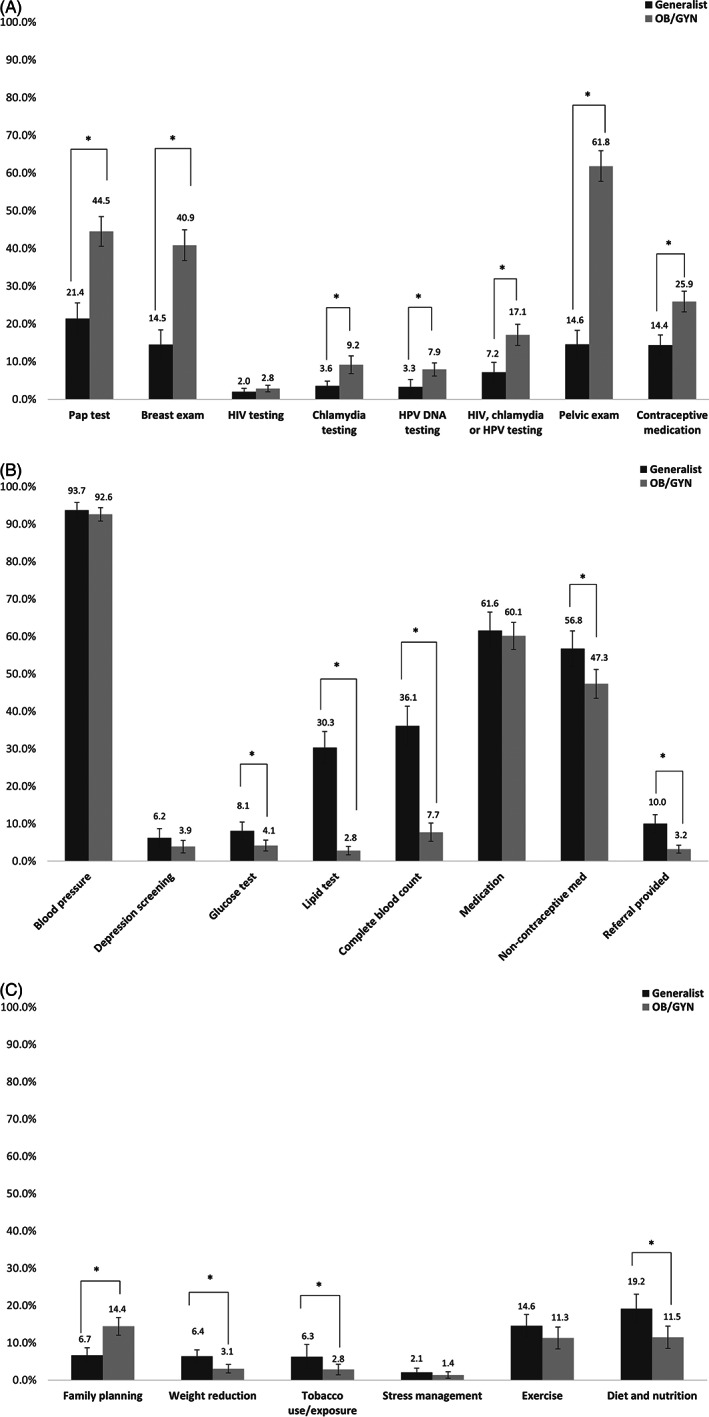
Adjusted probability of services provided in preventive care visits with OB/GYNs and generalist physicians by female patients age 18–44 (2011–2016). Panel A‐Reproductive health related services. Panel B‐Non‐reproductive health services. Panel C‐Counseling services. * indicates difference between generalist and obstetrician‐gynecologist (OB/GYN) estimates is statistically significant with p < 0.05. 95% confidence intervals are shown with vertical bars. Standard errors correct for the complex survey design. Sample size is 127,076,191 visits (n = 4229 unweighted). Reported estimates are predicted probability of service derived from regression models. Models adjust for diabetes, hypertension, depression, hyperlipidemia, asthma, patient age, patient race/ethnicity, insurance type, obesity, physician practice location in metropolitan statistical area, census region, solo practice, practice ownership, new or established patient, and visit year.
FIGURE 2.
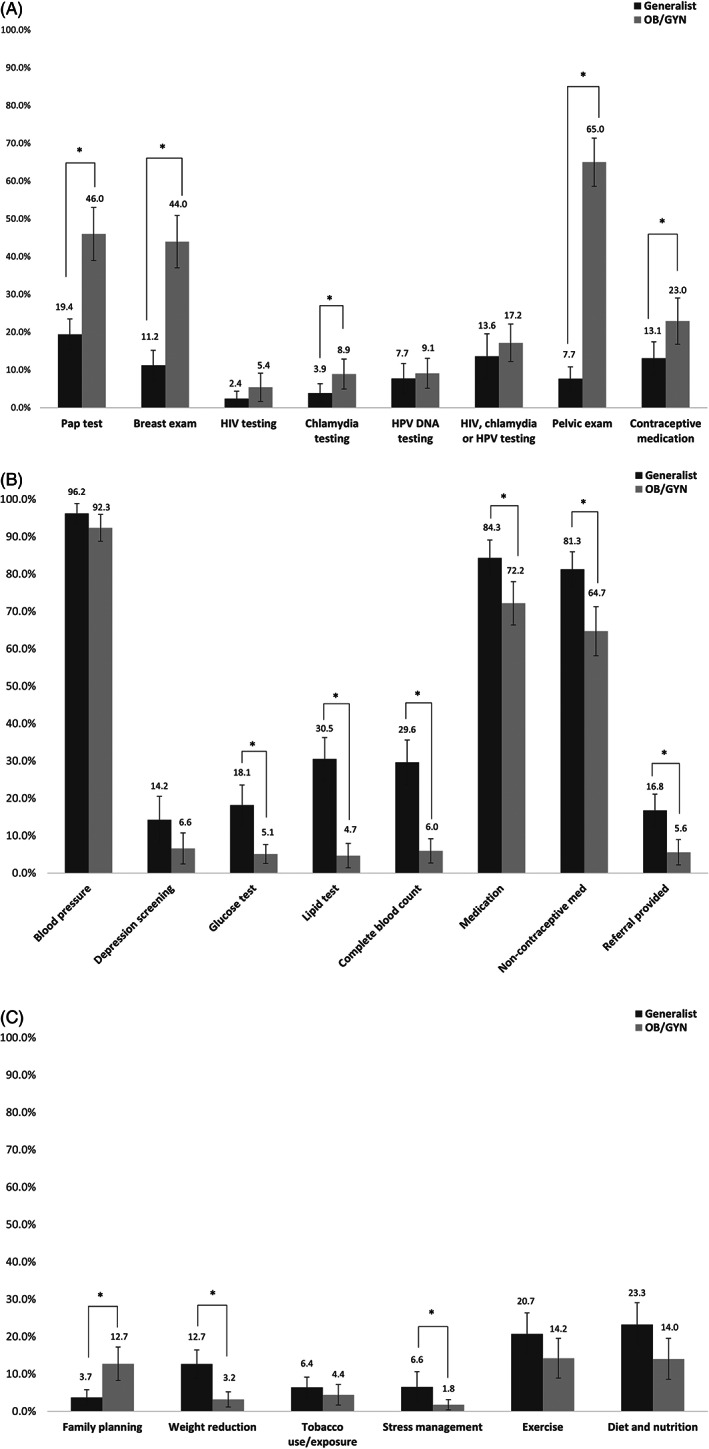
Adjusted probability of services provided in preventive care visits with OB/GYNs and generalist physicians by female patients age 18–44 with chronic conditions (2011–2016). Panel A‐Reproductive health related services. Panel B‐Non‐reproductive health services. Panel C‐Counseling services. * indicates difference between generalist and obstetrician‐gynecologist (OB/GYN) estimates is statistically significant with p < 0.05. Standard errors correct for the complex survey design. Sample size is 26,615,140 visits (n = 839 unweighted). Reported estimates are predicted probability of service derived from regression models. Models adjust for diabetes, hypertension, depression, hyperlipidemia, asthma, patient age, patient race/ethnicity, insurance type, obesity, physician practice location in metropolitan statistical area, census region, solo practice, practice ownership, new or established patient, and visit year.
Among visits for patients with chronic conditions (2011–2016, Figure 2), patterns were similar, with reproductive health services more likely in visits with OB/GYNs and non‐reproductive health services less likely in visits with OB/GYNs. Notably, any medication ordered or prescribed was less likely in visits with OB/GYNs in this sample, and there was no significant difference in visit length by physician specialty.
In sensitivity analyses restricting the samples to patients for whom specific services were more likely to be recommended (Appendix 2), the rate of service provision was somewhat higher. For example, weight reduction counseling was provided in 13.0% of visits for patients with documented obesity (vs. 4.3% in the general sample), and tobacco use/exposure counseling was provided in 14.9% of visits for patients who were current tobacco users (vs. 3.8% in the general sample); however, differences in the provision of these services by physician specialty remained statistically significant.
4. DISCUSSION
We found OB/GYN preventive care visits were more likely to include reproductive health‐oriented services but were significantly less likely to include non‐reproductive health services that may be particularly important for patients with chronic conditions, such as lipid testing and counseling about weight reduction and diet. These findings are consistent with prior research 15 ; our analysis extends these findings to patients with chronic conditions after ACA implementation.
A number of recent policy efforts that have sought to improve health care quality, including those that impact this age range, have been oriented around primary care providers. 25 , 26 , 27 , 28 Primary care orientation of financing and delivery system reform may not adequately account for the role that OB/GYNs play for a large proportion of reproductive‐age women, including those with chronic conditions. Receiving recommended preventive care for reproductive‐age women with and without chronic conditions is important for short‐ and long‐term health. 19 , 20 For patients with chronic conditions, contact with any clinician for preventive care may also be an opportunity to ensure the receipt of condition‐specific care.
Since 2018, ACOG guidance on preventive services in well‐woman visits explicitly includes cardiovascular risk assessment and counseling. 13 A 2018 joint statement by ACOG and the American Heart Association emphasized the importance of OB/GYN care in addressing cardiovascular disease risk factors and screening for cardiovascular disease—the leading cause of death for US women 29 —among reproductive‐age women during well‐woman visits. 30 We found that lipid testing was very rare in OB/GYN visits; provision of counseling on relevant topics such as diet and nutrition counseling and weight reduction counseling was low across all visits, but less common in OB/GYN than in generalist visits. This may have significant implications for women with hypertension, for whom primary prevention of cardiovascular events includes medication and lifestyle changes. 21
ACOG recommendations for well‐woman visits include a large number of services 13 ; it is possible that services perceived as less central to the OB/GYN specialty may be less likely to be provided amidst time constraints, potentially explaining our findings that non‐reproductive health services are less frequent in preventive care visits with OB/GYNs, which were also shorter. This is concerning if OB/GYN visits substitute rather than complement generalist visits. Although OB/GYN training competencies include management of patients with common non‐reproductive health conditions, 31 , 32 OB/GYNs may vary in comfort level treating such conditions. 33 However, if OB/GYNs are less likely to provide non‐reproductive health‐related services because those services were received from a generalist, this could be positive, as it would avoid duplicative care.
It is also possible that reproductive‐related services are under‐provided in generalist physician visits. Recent studies have shown that only 50% of family medicine physicians and 20% of internal medicine physicians provide prescription contraceptives, with even smaller proportions providing long‐acting reversible contraceptives. 22 , 23 Additionally, many women are prescribed potentially teratogenic medications to manage chronic conditions without documented contraceptive management. 24 We were unable to observe the full set of services that reproductive‐age women received over time due to the visit‐level unit of analysis. However, in a prior study, nearly 80% of women with a past‐year physician visit had seen only one type of physician, 34 suggesting that a minority of women seek care from both an OB/GYN and a generalist annually.
Guidelines for preventive services change frequently, and many guidelines have been updated since the period of the data. Guidelines may also differ or be adopted at different times across professional organizations. Our results provide baseline information about the frequency of services in preventive visits; given the slow and uneven incorporation of new guidelines into clinical practice, 35 , 36 trends in service provision are likely to persist. We would not expect all services examined to be provided in all visits, as some services are only indicated for patients with specific risk factors, or are recommended at intervals that we cannot assess in this visit‐level sample; however, many services were quite rarely provided. Our analysis included services that may be underused, and those that have had guideline changes supporting expanded use. For example, universal depression screening was recommended by the USPSTF in 2016, 37 and was very low in both OB/GYN and generalist visits during the study period. We also examined services that may be overused, such as pelvic exams for asymptomatic women and clinical breast exams for younger women, which have harms that outweigh the benefits. 38 , 39 Future research should assess whether changes to clinical practice associated with recent guideline changes differ across OB/GYNs and generalists.
5. LIMITATIONS
Our study had some important limitations. First, NAMCS only includes visits to office‐based physicians, and does not include visits to physicians in hospital outpatient departments or community health centers, or federally‐employed physicians. Visits to nurse practitioners or physician assistants are present in the sample in small numbers, but they are underrepresented relative to the amount of care provided by these clinicians. 40 , 41 Second, we were only able to include data through 2016 for analyses of differences in care provision by physician type. Descriptive statistics including 2018 data are very similar to those from prior years. Additional changes to the health policy landscape have occurred since 2016 and 2018, including additional states expanding Medicaid. However, we did not find differences in service provision by insurance status, somewhat limiting the implications of this change for our results. Third, as our unit of analysis is the preventive visit rather than the individual, we are unable to assess the full spectrum of care received across different sources over time; we are unable to determine whether a service not provided in an observed visit may have been provided in a different visit. However, as our sample consists of preventive visits only, the likelihood of more than one such visit per year is lower. While insurers are technically required to cover multiple preventive visits per year under the ACA without cost sharing, women and clinicians are often unaware of this, and women have reported experiencing cost sharing for preventive visits. 42 , 43
6. CONCLUSIONS
We find that services delivered in preventive visits by OB/GYNs to reproductive‐age women with and without chronic conditions primarily focus on reproductive health. This may mean women with non‐gynecological chronic conditions are not receiving recommended preventive care—particularly related to cardiovascular disease risk reduction—underscoring the importance of ensuring that women with chronic conditions receive care in the appropriate setting for their needs. Better understanding the full range of care received across settings by reproductive‐age women with chronic conditions could guide recommendations to optimize where this population seeks care.
Supporting information
Appendix Table 1. Coding of specific chronic health conditions using ICD‐9 and ICD‐10 codes.
Appendix 2. Services provided in preventive care visits with obstetrician‐gynecologists (OB/GYNs) and generalist physicians by female patients age 18–44.
ACKNOWLEDGMENTS
This work was supported by the National Heart, Lung, and Blood Institute (Grant Number R56HL151636). The funder had no role in study design, analysis, interpretation of data, or in the preparation, review or approval of the manuscript, or the decision to submit the manuscript for publication. The manuscript's contents are solely the responsibility of the authors and do not represent the official views of the National Heart, Lung, and Blood Institute.
Attanasio L, Ranchoff B, Jeung C, Goff S, Geissler K. Preventive care visits with OB/GYNs and generalist physicians among reproductive‐age women with chronic conditions. Health Serv Res. 2023;58(1):207‐215. doi: 10.1111/1475-6773.14100
[Correction added on 2 December 2022, after first online publication: in the article title, ‘reproductive‐ae’ has been changed to ‘reproductive‐age’.]
Funding information National Heart, Lung, and Blood Institute, Grant/Award Number: R56HL151636
REFERENCES
- 1. Maciosek MV, Coffield AB, Flottemesch TJ, Edwards NM, Solberg LI. Greater use of preventive services in U.S. health care could save lives at little or no cost. Health Aff. 2010;29(9):1656‐1660. doi: 10.1377/hlthaff.2008.0701 [DOI] [PubMed] [Google Scholar]
- 2. HealthCare.gov . Preventive health services. https://www.healthcare.gov/coverage/preventive-care-benefits/. Accessed May 19, 2022.
- 3. Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Quaterly. 2005;83(3):457‐502. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690145/pdf/milq0083-0457.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Starfield B. Primary care and equity in health: the importance to effectiveness and equity of responsiveness to Peoples' needs. Humanit Soc. 2009;33(1–2):56‐73. doi: 10.1177/016059760903300105 [DOI] [Google Scholar]
- 5. Henry J. Kaiser Family Foundation . Obamacare & you: if you are a woman…. Henry J Kaiser Fam Found. 2013:1. http://kff.org/health-reform/fact-sheet/obamacare-and-you-if-you-are-a-woman/ [Google Scholar]
- 6. MassHealth Comprehensive Quality Strategy ; 2018. https://www.mass.gov/doc/masshealth‐comprehensive‐quality‐strategy‐november‐2018‐0/download.
- 7. Buttorff C, Ruder T, Bauman M. Multiple Chronic Conditions in the United States ; 2017. doi: 10.7249/tl221 [DOI]
- 8. Azeez O, Kulkarni A, Kuklina EV, Kim SY, Cox S. Hypertension and diabetes in non‐pregnant women of reproductive age in the United States. Prev Chronic Dis. 2019;16(10):1‐9. doi: 10.5888/pcd16.190105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Guo N, Robakis T, Miller C, Butwick A. Prevalence of depression among women of reproductive age in the United States. Obstet Gynecol. 2018;131(4):671‐679. doi: 10.1097/AOG.0000000000002535 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hayes DK, Robbins CL, Ko JY. Trends in selected chronic conditions and related risk factors among women of reproductive age: behavioral risk factor surveillance system, 2011‐2017. J Women's Health. 2020;29(12):1576‐1585. doi: 10.1089/jwh.2019.8275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Centers for Disease Control and Prevention . Your Diabetes Care Schedule. https://www.cdc.gov/diabetes/managing/care-schedule.html. Accessed May 11, 2022.
- 12. Centers for Disease Control and Prevention . Prevent and Manage High Blood Pressure. https://www.cdc.gov/bloodpressure/manage.htm. Accessed September 21, 2022.
- 13. Commitee on Gynecologic Practice . ACOG Committee opinion #755: well‐woman visit. Obstet Gynecol. 2018;132(4):e181‐e186. doi: 10.1097/00006250-200502000-00066 [DOI] [PubMed] [Google Scholar]
- 14. U.S. Preventive Services Task Force Recommendations. https://www.uspreventiveservicestaskforce.org/uspstf/topic_search_results?age_group%5B0%5D=10&gender%5B0%5D=13&topic_status=All&grades%5B0%5D=A&grades%5B1%5D=B&grades%5B2%5D=C&PAGE=2. Accessed May 23, 2022.
- 15. Stormo AR, Saraiya M, Hing E, Henderson JT, Sawaya GF. Women's clinical preventive services in the United States: who is doing what? JAMA Intern Med. 2014;174(9):1512‐1514. doi: 10.1001/jamainternmed.2014.3003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dean CA, Arnold LD, Hauptman PJ, Wang J, Elder K. Patient, physician, and practice characteristics associated with cardiovascular disease preventive Care for Women. J Women's Health. 2017;26(5):491‐499. doi: 10.1089/jwh.2015.5613 [DOI] [PubMed] [Google Scholar]
- 17. Claridy MD, Czepiel KS, Bajaj SS, Stanford FC. Treatment of obesity: pharmacotherapy trends of office‐based visits in the United States from 2011 to 2016. Mayo Clin Proc. 2021;96(12):2991‐3000. doi: 10.1016/j.mayocp.2021.07.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Davidson KW, Barry MJ, Mangione CM, et al. Screening for chlamydia and gonorrhea: US preventive services task force recommendation statement. J Am Med Assoc. 2021;326(10):949‐956. doi: 10.1001/jama.2021.14081 [DOI] [PubMed] [Google Scholar]
- 19. Dunlop AL, Jack BW, Bottalico JN, et al. The clinical content of preconception care: women with chronic medical conditions. Am J Obstet Gynecol. 2008;199(6 SUPPL. B):S310‐S327. doi: 10.1016/j.ajog.2008.08.031 [DOI] [PubMed] [Google Scholar]
- 20. Hammarberg K, Stocker R, Romero L, Fisher J. Pregnancy planning health information and service needs of women with chronic non‐communicable conditions: a systematic review and narrative synthesis. BMC Pregnancy Childbirth. 2022;22(1):1‐22. doi: 10.1186/s12884-022-04498-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Circ. 2019;140(11):e596‐e646. doi: 10.1161/CIR.0000000000000678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Casas RS, Prifti CA, Bachorik AE, et al. Contraceptive procedures in internal medicine clinics and resident education: a qualitative study of implementation methods, barriers, and facilitators. J Gen Intern Med. 2021;36(11):3346‐3352. doi: 10.1007/s11606-021-06832-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Chen C, Strasser J, Banawa R, et al. Who is providing contraception care in the United States? An observational study of the contraception workforce. Am J Obstet Gynecol. 2022;226(2):232.e1‐232.e11. doi: 10.1016/j.ajog.2021.08.015 [DOI] [PubMed] [Google Scholar]
- 24. Panchal BD, Cash R, Moreno C, et al. High‐risk medication prescriptions in primary care for women without documented contraception. J Am Board Fam Med. 2019;32(4):474‐480. doi: 10.3122/jabfm.2019.04.180281 [DOI] [PubMed] [Google Scholar]
- 25. Blue Cross Blue Shield Massachusetts ‐ Alternative Quality Contract. https://www.pcpcc.org/initiative/blue-cross-blue-shield-massachusetts-alternative-quality-contract. Accessed May 31, 2022.
- 26. Rutledge RI, Romaire MA, Hersey CL, Parish WJ, Kissam SM, Lloyd JT. Medicaid accountable care organizations in four states: implementation and early impacts. Milbank Q. 2019;97(2):583‐619. doi: 10.1111/1468-0009.12386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Center for Health Care Strategies . Medicaid Accountable Care Organizations: State Update ; 2018. https://www.chcs.org/resource/medicaid‐accountable‐care‐organizations‐state‐update/#:~:text=Thecollaborativeishelpingstates,riskandqualitytoproviders.
- 28. Swietek KE, Domino ME, Beadles C, et al. Do medical homes improve quality of Care for Persons with multiple chronic conditions? Health Serv Res. 2018;53(6):4667‐4681. doi: 10.1111/1475-6773.13024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Centers for Disease Control and Prevention (CDC) . Leading Causes of Death – Females – All races and origins – United States, 2017. https://www.cdc.gov/women/lcod/2017/all-races-origins/index.htm. Accessed June 1, 2022.
- 30. Brown HL, Warner JJ, Gianos E, et al. Promoting risk identification and reduction of cardiovascular disease in women through collaboration with obstetricians and gynecologists: a presidential advisory from the American Heart Association and the American college of obstetricians and gynecologi. Circulation. 2018;137(24):e843‐e852. doi: 10.1161/CIR.0000000000000582 [DOI] [PubMed] [Google Scholar]
- 31. The Accreditation Council for Graduate Medical Education . The American Board of Obstetrics and Gynecology, The American College of Obstetrics and Gynecology Obstetrics. The Obstetrics and Gynecology Milestone Project Obstetrics and Gynecology Milestones: Joint Initiative of The Accreditation Council for Graduate Medical Education, The American Board of Obstetrics and Gynecology, and The American College of Obstetrics And. Accreditation Council for Graduate Medical Education; 2015. https://www.acgme.org/Portals/0/PDFs/Milestones/ObstetricsandGynecologyMilestones.pdf [Google Scholar]
- 32. Accreditation Council for Graduate Medical Education . ACGME Program Requirements for Graduate Medical Education in Obstetrics and Gynecology ; 2020.
- 33. Smith S, Seeholzer EL, Gullett H, et al. Primary care Residents' knowledge, attitudes, self‐efficacy, and perceived professional norms regarding obesity, nutrition, and physical activity counseling. J Grad Med Educ. 2015;7(3):388‐394. doi: 10.4300/JGME-D-14-00710.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Petterson SM, Bazemore AW, Phillips RL, Rayburn WF. Trends in office‐based care for reproductive‐aged women according to physician specialty: a ten‐year study. J Women's Health. 2014;23(12):1021‐1026. doi: 10.1089/jwh.2014.4765 [DOI] [PubMed] [Google Scholar]
- 35. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients' care. Lancet. 2003;362(9391):1225‐1230. doi: 10.1016/S0140-6736(03)14546-1 [DOI] [PubMed] [Google Scholar]
- 36. Westfall JM, Mold J, Fagnan L. Practice‐based research—“blue highways” on the NIH roadmap. JAMA. 2007;297(4):403‐406. [DOI] [PubMed] [Google Scholar]
- 37. Siu AL, Bibbins‐Domingo K, Grossman DC, et al. Screening for depression in adults: US preventive services task force recommendation statement. J Am Med Assoc. 2016;315(4):380‐387. doi: 10.1001/jama.2015.18392 [DOI] [PubMed] [Google Scholar]
- 38. Niven DJ, Mrklas KJ, Holodinsky JK, et al. Towards understanding the de‐adoption of low‐value clinical practices: a scoping review. BMC Med. 2015;13(1):255. doi: 10.1186/s12916-015-0488-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Colla CH, Mainor AJ, Hargreaves C, Sequist T, Morden N. Interventions aimed at reducing use of low‐value health services: a systematic. Review. 2017;74:507‐550. doi: 10.1177/1077558716656970 [DOI] [PubMed] [Google Scholar]
- 40. Nyweide DJ, Lee W, Colla CH. Accountable care organizations' increase in nonphysician practitioners may signal shift for health care workforce. Health Aff. 2020;39(6):1080‐1086. doi: 10.1377/hlthaff.2019.01144 [DOI] [PubMed] [Google Scholar]
- 41. Frost A, Hargraves J. HCCI Brief: Trends in Primary Care Visits; 2018. https://www.pcpcc.org/sites/default/files/resources/PCPBriefFinal.pdf
- 42. Fitzgerald T, Glynn A, Davenport K, Waxman J, Johnson PA. Well‐woman visits: guidance and monitoring are key in this turning point for women's health. Womens Health Issues. 2015;25(2):89‐90. doi: 10.1016/j.whi.2015.01.001 [DOI] [PubMed] [Google Scholar]
- 43. Salganicoff A, Ranji U, Beamesderfer A, Jurani N. Women and health care in the early years of the ACA: key findings from the 2013 Kaiser Women's health survey. Henry J Kaiser Fam Found. 2014;(May):Publication #8590, 45 pp. http://kff.org/womens‐health‐policy/report/women‐and‐health‐care‐in‐the‐early‐years‐of‐the‐aca‐key‐findings‐from‐the‐2013‐kaiser‐womens‐health‐survey/ [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix Table 1. Coding of specific chronic health conditions using ICD‐9 and ICD‐10 codes.
Appendix 2. Services provided in preventive care visits with obstetrician‐gynecologists (OB/GYNs) and generalist physicians by female patients age 18–44.