

Abstract
In adolescence, teens manage close friendships while simultaneously evaluating their social position in the larger peer context. Conceptualizing distinct local and global network structures clarifies how social integration relates to mental wellbeing. Examining local cohesion and global embeddedness in the context of key factors related to mental health, such as gender and friends’ depression, can further distinguish when the structure and content of social integration relate to higher and lower depressive levels. Analyses using survey data from PROSPER (n = 27,091, grades 9–12) indicate global embeddedness is generally protective, but for girls, greater global embeddedness when friends are more depressive is associated with increased depressive symptoms. For girls, greater local cohesion reduces associations between more depressive friends and increased depressive levels, while for boys, both local cohesion and friends’ depression are largely irrelevant. Results indicate the importance of considering both local and global network integration in tandem with gender and friends’ depression to understand how social integration relates to mental health.
Keywords: depression, social integration, adolescence, social networks, mental health
Social integration is critical for mental wellbeing (Durkheim 2006 [1897]; Kawachi and Berkman 2001). Integration, or being embedded within cohesive structures of social ties, shapes behaviors, opportunities, and constraints that affect mental health (Moody and White 2003; Pescosolido 1992). Integration is particularly important in adolescence, a developmental period when peers take on heightened salience (Ragan, Osgood, and Feinberg 2014) and risks to mental health rise (Hankin 2006). About, 20–50 percent of teens report substantial depressive symptoms, with even minor depressive levels predicting subsequent suicidal behavior, depressive disorders, and impaired functioning (Allen et al. 2014; Hankin 2006). However, how social contexts shape depression early in the life course remains unclear, with greater connections in peer networks related to both lower (La Greca and Harrison 2005; Ueno 2005) and higher mental distress (Falci and McNeely 2009; Kornienko et al. 2013).
Teens occupy multidimensional positions at multiple network levels. These positions simultaneously include integration among immediate ties with close friends and embeddedness in the network overall. Individuals are thus structurally integrated within a network in two conceptually distinct ways: locally and globally. Being nested in one’s ego-network of direct ties and the overall network of a setting provide measures of local cohesion and global embeddedness that may impact mental health differently.
Moreover, how network structure relates to mental health depends on the content and context of social relationships (Pescosolido 2006). Gender socialization affects social relationships, mental health, and how relationships affect mental health (Rose and Rudolph 2006; Rosenfield and Mouzon 2013). The same network characteristics can relate differently to mental health for girls and boys (Copeland et al. 2019; Falci and McNeely 2009). Similarly, peers’ mental health may shape how relations affect individuals’ mental health, as relationships that are typically beneficial may become detrimental if friends are experiencing depressive symptoms (Schwartz-Mette et al. 2020). Consequently, any associations of local and global integration with mental health likely depend on gender and peer mental health.
This study advances research on social networks and mental health by examining gendered contexts of structural integration among close friends and the overall network, as local cohesion and global embeddedness. Using rich sociocentric data from the PROSPER survey, I examine whether within-person changes in local cohesion and global embeddedness predict changes in depressive symptoms in adolescence. I then test whether gender and friends’ depressive levels moderate these associations. In doing so, this study contributes to our understanding of social integration, the structure and content of network ties, and mental health.
I begin by reviewing the social networks perspective of social integration as potentially beneficial and detrimental in adolescence, then highlight two important levels of integration: local cohesion and global embeddedness. I then review the importance of considering key contextual features that shape how integration relates to mental health, specifically gender and friends’ mental health, before moving into the new empirical analyses of this study.
Background
Social Integration and Mental Health in Adolescence
The social networks perspective recognizes that social ties relate to outcomes in many domains, including health (Pescosolido 2015, 2006). Direct and indirect ties create webs of relational structure in which individuals are more or less embedded (Granovetter 1973; Hartwell and Benson 2007; Pescosolido et al. 2016). The structural arrangement of close and distant connections shapes access to resources, shared trust, social demands, norms, and behavior (Granovetter 1973; Pescosolido 1992). Consequently, the extent to which an individual is integrated within the network structure affects mental health (Abrutyn and Mueller 2016). Examining this structural integration is critical when considering mental health, as distress itself can skew self-perceptions of integration (Cillessen and Bellmore 1999).
In adolescence, same-age school peers guide norms, identity, psychological well-being, and behavior (Umberson, Crosnoe, and Reczek 2010). As a result, school peer networks provide multi-faceted contexts related to health, beyond effects of direct ties (Falci and McNeely 2009; Lee and Lee 2020; Suh, Shi, and Brashears 2017). Effects of peer social integration can also last into adulthood (Almquist 2011; Kamis and Copeland 2020). Adolescent networks thus provide a critical test case for networks and mental health, but the importance of social integration extends to other ages and contexts (Faris 2012).
Social integration typically benefits mental health (Kawachi and Berkman 2001). Integration in a network provides foundational structures for social support, shared identity, and other psychosocial benefits that support mental wellbeing (Hartwell and Benson 2007; Pescosolido et al. 2016; Ueno 2005). Lacking integration also predicts higher mental distress (Kornienko et al. 2013). For teens, popularity among school peers (as in-degree categories), one’s number of friends (total degree), and belonging to a high-status peer group all predict lower depressive levels (La Greca and Harrison 2005; Ueno 2005).
Yet integration is not exclusively beneficial. While research on integration and mental health typically highlights benefits of integration, integration can also harm wellbeing (Abrutyn and Mueller 2016). Integration can increase social regulation, sanctions for violating norms, and demands for support (McGloin, Sullivan, and Thomas 2014; Pescosolido et al. 2016). In adolescence, popularity and greater prestige among depressive friends (Reynolds and Crea 2015), and very high levels of popularity (Falci and McNeely 2009) predict higher depressive levels. Understanding when integration relates to better or worse mental health may benefit from examining distinct dimensions of integration.
Local Cohesion and Global Embeddedness
Understanding how integration relates to mental health can benefit from applying a multilevel network perspective (Brailly et al. 2016; Haas, Schaefer, and Kornienko 2010; Lee and Lee 2020). Structural integration occurs at two simultaneous levels of the network, here termed local cohesion and global embeddedness (Granovetter 1992).1 Some multilevel network approaches distinguish individual positions versus characteristics of the overall network (for examples using ego-network and global network-level characteristics, see Guan and Kamo 2016; Ueno 2005). However, an individual’s position is also integrated at multiple network levels. Individuals are more or less integrated in close relationships that are simultaneously nested within the larger web of connections in the overall network. That is, social integration is a combination of integration among both proximal, close ties and the more distal structure of the entire network. A multilevel network perspective conceptualizes these network levels as related and nested, but also distinct, with different structures and effects at each level (Brailly et al. 2016; Pescosolido et al. 2016). Examining these distinct levels of social integration can clarify how individuals’ connections present risks and benefits to health (Pescosolido 2015).
First, individuals’ can be more or less integrated in their ego-network. Ego-networks are a teen’s named friends, representing a group of close ties (with “close” meaning direct ties as opposed to indirectly connected acquaintances, rather than the strength or content of a relationship). Integration at this local level relates to mental health beyond simply the count of one’s ties (Falci and McNeely 2009). One aspect of integration among close ties is local cohesion, meaning the interconnectedness or density of ties in one’s ego-network. For example, an individual could have many ties to others, or alters, who are not connected to each other. This creates a non-integrative, non-cohesive group that is easily disconnected. The same number of ties among alters who are interconnected creates a cohesive group that is harder to disrupt. This local cohesion has implications for the benefits or constraints that an individual experiences, distinct from other network measures (Falci and McNeely 2009; Granovetter 1992). The cohesive structure of close ties indicates the extent and intensity of group interactions, shared identity, and trust (Haynie 2001; McGloin, Sullivan, and Thomas 2014). Greater local cohesion can strengthen group norms and social support, but it can also lead to over-regulation of behavior, sanctions for violating norms, and the proliferation of stress across ties (Falci and McNeely 2009; Kornienko et al. 2013; McGloin, Sullivan, and Thomas 2014).
Second, individuals can be more or less globally integrated, meaning how deeply nested an individual is within the entire network. As with local ego-networks, the structural cohesion of an entire network is determined by whether multiple network pathways connect individuals (Moody and White 2003). This cohesion represents the extent to which social relations hold the network together and are robust to disruption (Moody and White 2003). Structural cohesion at the individual level means that each individual’s position in the network is embedded within the overall web of social ties “like Russian dolls—with increasingly cohesive groups nested inside each other” (Moody and White 2003, p. 109), akin to being in the core or periphery of the entire network. Unlike whole network characteristics (e.g., size of the entire network), this global embeddedness captures cohesive structures among an individual’s indirect social relations that shape norms, behaviors, or the spread of resources across a network (Bastomski, Brazil, and Papachristos 2017; Moody and White 2003). Individuals’ global embeddedness has been shown to shape economic action (Granovetter 1985), criminal activity (Bastomski, Brazil, and Papachristos 2017), and school attachment (Moody and White 2003), but it has not yet been applied to mental health.
Local cohesion and global embeddedness are theoretically and empirically distinct (Moody and White 2003). For example, a cohesive, tight-knit group of close friends situated on the periphery of the overall network represents high local cohesion and low global embeddedness. Conversely, a teen may be deeply nested within the entire network but span non-cohesive friend groups, representing high global embeddedness and low local cohesion. However, these two simultaneous aspects of individuals’ integration in a network have not been examined together in association with mental health.
Mental Health Context and Integration
Another key element in disentangling how network integration relates to wellbeing is the mental health context of ties. How network structure relates to health depends in part on the content within that structure (Pescosolido 2006). Integration may relate differently to depression depending on peers’ mental health. While some network studies examine depression contagion (Schaefer, Kornienko, and Fox 2011), friends’ mental health can also shape how integration predicts depression beyond direct diffusion processes. Depressive friends can induce conflict, stress, or maladaptive processes that increase distress (Coyne 1976; Schwartz-Mette et al. 2020).
Peers’ mental health may affect both local and global network integration. For example, processes that lead peers to benefit mental health, such as social support, typically happen among close friends rather than distant acquaintances in the wider network (Cornwell 2003; Schwartz-Mette et al. 2020). However, these same close friend groups can also spur detrimental processes, such as excessive support-seeking or co-rumination (Schwartz-Mette et al. 2020). Thus, local cohesion may typically benefit teens, but be moderated by friends’ depressive levels.
Friends’ mental health can also interact with the broader features of a setting (Lee and Lee 2020). For example, both close friends’ and grademates’ depressive levels relate to teens’ depression, but in different ways (Lee and Lee 2020). The salience of a teen’s social position in the overall setting also shapes how social ties affect mental health (Abrutyn and Mueller 2016). In this way, both local cohesion and global embeddedness may interact with friends’ depressive symptoms to affect teens’ mental health.2
Gender and Integration
Any view of mental health and social integration benefits from examining gender. Gender is a major status characteristic organizing social life and interpersonal interactions (Ridgeway and Correll 2004). Gender patterns mental distress, social relationships, and how social relationships relate to health (McMillan, Felmlee, and Osgood 2018; Turner and Turner 1999; Umberson et al. 2010). Women typically exhibit higher depressive levels than men (Rosenfield and Mouzon 2013; Turner and Turner 1999). This difference first manifests in adolescence (Hankin 2006) and cannot be reduced to artifacts of scale creation or gender differences in emotional expressiveness (Simon 2020).
How social relationships relate to mental health also varies with gender. Teens perform gender in friendships, with gender shaping interactions, norms, and social pressures that contribute to how friendships affect behavior and health (McMillan, Felmlee, and Osgood 2018). Girls are socialized to prioritize others over the self, emphasize emotional disclosure and support, “tend and befriend” others in response to stress, and generally depend upon others (Abrutyn and Mueller 2016; Rose and Rudolph 2006; Rosenfield 2012). Relationships, as well as events, strains, and changes in social networks, play a large role in girls’ self-schemas, with resultant effects on mental health (Rosenfield 2012; Simon 2020). This importance of close friendships to girls suggests that local cohesion can substantially impact girls’ mental health.
Girls are also typically more aware of network structure overall, and network structure has greater mental health effects for girls (Abrutyn and Mueller 2016; Kornienko and Santos 2014). Positions in the overall network affect girls’ mental health (Kornienko and Santos 2014), and girls are highly attuned to peer approval and status (Rose and Rudolph 2006). Thus, global embeddedness likely also relates to girls’ mental health.
Gender differences also arise in relational content. Compared to boys, girls typically maintain fewer, closer relationships marked by greater self-disclosure, support, and co-rumination, processes that affect distress (Kornienko and Santos 2014; Schwartz-Mette et al. 2020). These features of girls’ friendships mean that friends’ depressive symptoms may affect girls’ own depressive levels.
In contrast, boys are typically socialized to enforce and adhere to masculine norms in friendships. Boys generally maintain larger friend groups with fewer emotional demands or disclosures, less support-seeking, and greater sanctions against expressing poor mental health (Cheadle and Goosby 2012; Kornienko and Santos 2014; Reigeluth and Addis 2015). These norms against disclosure and support-seeking can make boys less attuned to the local level of friendships and less subject to effects of friends’ depressive levels. Instead, boys are socialized to emphasize dominance in friendships, with preferences for highly popular or high-status friends (Rose and Rudolph 2006; Shin 2017). This attention to high status and dominance within the entire network suggests that boys may be attuned to global embeddedness rather than local cohesion. Together, these patterns suggest girls are more sensitive to effects of local cohesion and to friends’ depressive levels than boys, but global embeddedness likely relates to mental health regardless of gender.
The Current Study
This study considers how local and global integration are associated with depressive symptoms in adolescence and how any association varies with teens’ gender and friends’ depression. Though global embeddedness has not yet been examined in relation to adolescent mental health, prior literature suggests several relevant expectations. First, local cohesion and global embeddedness are expected to have generally beneficial associations with mental health that can become detrimental if friends are increasingly depressive (Hypothesis 1). Second, given girls’ socialized attunement to relationships, increased local cohesion and global embeddedness are expected to predict lower depressive levels for girls, but greater integration among more depressive friends is expected to increase girls’ depressive levels (Hypothesis 2). As boys emphasize dominance and sanction emotional disclosure in friendships, local cohesion and friends’ depressive levels are likely less salient, so that only increased global embeddedness predicts lower depressive levels for boys (Hypothesis 3).
Data and Methods
The data used here were collected as part of the PROSPER (PROmoting School-community-university Partnerships to Enhance Resilience) Project. PROSPER was a randomized controlled trial evaluating a partnership-based delivery system for evidence-based preventive intervention (Spoth et al. 2004, 2013). This study uses data from the in-school survey within the larger PROSPER Project. Pencil-and-paper surveys were administered to students during school starting in the Fall of sixth grade for two cohorts. These cohorts were in successive calendar years starting in 2002 and 2003. Subsequent surveys were administered every spring from grades 6 to 12. Surveyed school districts (n = 27 participating in the social network survey) were in semi-rural and rural Pennsylvania and Iowa. Sampled districts had enrollments ranging from 1,500 to 5,200, and at least 15 percent of students in each district came from low-income families. This study includes respondents from both the control and treatment groups in the larger PROSPER Project randomized controlled trial targeting attitudes toward substance use. As noted in the robustness section, results here do not differ by treatment condition.
Mental health data were surveyed in the last four waves of high school, when students were in grades 9–12, with an average response rate of 81 percent. Social network measures came from a friend nomination question administered at each wave, where respondents listed the names of up to seven best or close friends in their grade and school. These nominations were then matched so that survey responses from students nominated as friends are linked, meaning that network ties indicate sent or received friendship nominations.
This design provides sociocentric (rather than only egocentric) network measures that indicate the entire peer network in that grade. This design also provides self-report data from peers rather than focal adolescents’ perceptions of peer behavior, eliminating concerns of false consensus bias where teens over-estimate how similar peers are to themselves (Prinstein and Wang 2005). While these data are not nationally representative, they provide unusually rich sociocentric network data, are comparable to nationally representative samples for a variety of adolescent outcomes, and are well-established in the adolescent networks literature (Copeland et al. 2019; Ragan et al. 2019, 2014; Siennick and Picon 2019, among others).
Dependent Variable
The outcome of depressive symptoms is measured with the average of five items from a popular and well-validated psychological scale. Items assess experiencing symptoms of depression, such as depressed mood and feelings of worthlessness, consistent with American Psychiatric Association guidelines (American Psychiatric Association 2000). Individuals’ scores are averaged within-wave to create a continuous measure of depressive symptoms at each wave ranging from 0 to 2 (α = .83), consistent with prior work (Siennick and Picon 2019).
Independent Variables
Local cohesion is measured by ego-network density (based on directed sent and received ties) at each wave. This measure indicates the proportion of existing ties divided by the total possible ties in an individual’s ego-network, defined by sent and received ties (Wasserman and Faust 1994). Density indicates the extent to which adolescents are embedded in cohesive, tight-knit friend groups where friends are friends with each other and ego. Youth with 0 friends (n = 1,620 observations in the analytic sample) or one friend (n = 1,060 observations in the analytic sample) have a density of 0, as they do not have friends who are friends with each other. Prior work supports using density to measure integration among close friends (Guan and Kamo 2016; Haynie 2001) and as a local corollary to global embeddedness (Moody and White 2003).
Global embeddedness is measured as individual structural embeddedness. This measure captures how deeply nested an individual is within the entire network (here, a grade in school). This measure assesses structural cohesion to identify an individual’s deepest cutset level based on undirected ties (Moody and White 2003). The cutset represents the set of nodes whose removal disconnects the network, so that identifying minimum cuts indicates the nodes that are most easily removed from the network (Moody and White 2003). For example, eliminating the first cutset removes isolates and “pendant” nodes connected to the network by one tie, then removing the next cutset removes nodes connected to the remaining network through two ties, and so on. An individual’s cutset level thus shows how difficult it would be to disconnect that individual from the network. This measure indicates which individuals are hardest to disconnect, and thus are the most deeply embedded in the network. Global embeddedness is assessed at each wave and ranges from 0 to 5, indicating least to most embedded.
Figure 1 shows one example of global embeddedness in one network in this dataset, with circles (nodes) representing individuals and lines (edges) representing friendships. The shade of nodes and concentric lines indicate successively nested sets representing global embeddedness levels.
Figure 1.
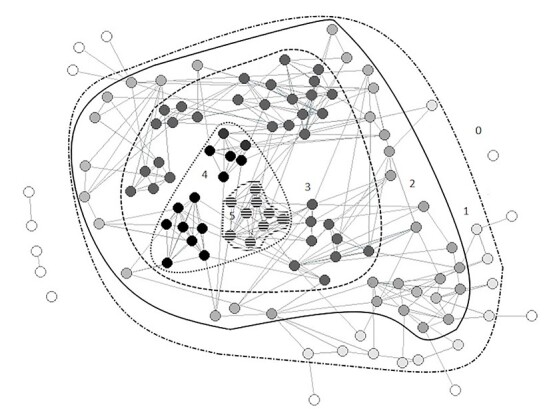
Global embeddedness in an example PROSPER network.
Correlations between variables are shown in table 1. While correlations of global embeddedness with control measures of popularity and gregariousness are high, removing these controls does not change the pattern of results. Tests for collinearity (variance inflation factor scores, shown in the supplemental appendix) have values well within acceptable ranges.
Table 1.
Correlation of Model Variables in PROSPER Sample
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Depressive symptoms | 1.00 | ||||||||||
| (2) Local cohesion | −.029*** | 1.00 | |||||||||
| (0.00) | |||||||||||
| (3) Global embeddedness | −.071*** | .361*** | 1.00 | ||||||||
| (0.00) | (0.00) | ||||||||||
| (4) Friend depression | .193*** | .044*** | .066*** | 1.00 | |||||||
| (0.00) | (0.00) | (0.00) | |||||||||
| (5) Popularity | −.033*** | .188*** | .661*** | .053*** | 1.00 | ||||||
| (0.00) | (0.00) | (0.00) | (0.00) | ||||||||
| (6) Gregariousness | −.073*** | .182*** | .723*** | .087*** | .456*** | 1.00 | |||||
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | |||||||
| (7) Low SES | .069*** | −.062*** | −.179*** | .065*** | −.146*** | −.134*** | 1.00 | ||||
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | ||||||
| (8) Biological parents | −.114*** | .067*** | .165*** | −.057*** | .131*** | .142*** | −.240*** | 1.00 | |||
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | |||||
| (9) School adjustment | −.243*** | .070*** | .179*** | −.009 | .119*** | .218*** | −.065*** | .138*** | 1.00 | ||
| (0.00) | (0.00) | (0.00) | (0.12) | (0.00) | (0.00) | (0.00) | (0.00) | ||||
| (10) Grade | −.056*** | −.007 | −.315*** | −.117*** | −.177*** | −.209*** | −.048*** | .005 | .026*** | 1.00 | |
| (0.00) | (0.23) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.37) | (0.00) | |||
| (11) Out-of-grade friends | .027*** | −.063*** | .023*** | .019** | −.030*** | .056*** | .031*** | −.028*** | −.025*** | −.095*** | 1.000 |
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) |
* p < .05.
** p < .01.
*** p < .001.
Moderating Variables
Models assess moderation by gender and friends’ mental health. Gender is a time-invariant variable measured dichotomously as male (male = 1, female = 0). Friend depression measures the depressive symptoms (with the same measure as the dependent variable) averaged for an individuals’ sent- and received-tie ego-network alters at each wave. Including this variable enables examining associations of integration and depressive symptoms net of friends’ depressive levels and testing the moderating effect of friends’ depression on these associations. Including this measure also adjusts for network autocorrelation, or the tendency of friends to have similar depressive levels. Individuals with 0 friends have a 0 for this measure (and results are consistent if these individuals are treated as missing).
Control Variables
Several variables adjust for known factors related to depressive symptoms and networks. Eligibility for free or reduced-price lunch, an indicator of a family income below 150 percent of the federal poverty level, is measured at each wave as a dichotomous approximation for low socioeconomic status (Low SES). Other time-varying control variables assessed at each wave include a dummy variable for biological parents indicating if respondents live with both biological parents, and school adjustment, which measures individuals’ feelings toward the school environment (items listed in the supplemental appendix). Because depressive symptoms and the importance of peers likely vary as adolescents age (Prinstein and Giletta 2014), a dummy variable is included for each grade (which, given survey design, is collinear with survey wave).
Other network measures were used as time-varying controls assessed at each wave to further isolate any association of global embeddedness and local cohesion with depressive symptoms. Popularity is measured by in-degree, the number of friendship nominations a respondent receives. Gregariousness is out-degree, the number of nominations a respondent sends. Including these measures means that any association of depressive symptoms with local cohesion and global embeddedness is measured net of individuals’ number of friendship ties. Out-of-grade friends is a count variable of the number of close friends respondents claim outside of their grade or school to adjust for adolescents spending social energy outside of the observed network. While some youth claim high numbers of out-of-grade friends, this is not unusual when friendships are elicited as a count rather than naming specific individuals that are then matched within a setting. As models assess within-person change, other time-invariant controls, such as race/ethnicity or intervention treatment condition, are already accounted for within the model and do not require separate control measures.
Analytic Plan
The final analytic sample excludes respondents who repeat a grade during observed years (n = 24), as they appear twice in the same wave. The total remaining sample is 34,888 person-waves. Given the lack of validated imputation methods for sociocentric network measures and the robustness of network measures to missingness (Smith, Moody, and Morgan 2017), analyses use listwise deletion. Less than 1 percent of cases are missing on the dependent variable, meaning listwise deletion mostly removes cases missing on predictor variables, a case in which analytic models are generally robust (Allison 2002). The final analytic sample after listwise deletion is 27,091 person-waves representing 11,418 individuals. This sample represents 5,969 girls and 5,449 boys across the four waves.
The analytic sample also does not look substantially different from deleted cases on key measures. Average depressive symptoms are .27 in both deleted and complete cases, not significantly different in two-tailed t-tests. Differences for both local cohesion and global embeddedness are significant (two-tailed t-test), but small in magnitude. Average local cohesion is .18 versus .21, and average global embeddedness 1.7 and 1.9 for deleted versus complete cases, respectively. These differences suggest that less integrated youth may be more likely to have greater missingness, perhaps from leaving surveys incomplete or school absence. However, differences are small in comparison to the standard deviation for each measure, and local cohesion and global embeddedness are not correlated with missingness on the dependent variable. Analyses reducing missingness by removing control variables with the highest missing values (Low SES, School Adjustment, Out-of-grade friends) also show the same pattern, suggesting listwise deletion does not drive results.
Analyses use ordinary least squares (OLS) regression with individual-level fixed effects. Robust standard errors are used to adjust for heteroscedasticity and provide more conservative estimates of significance. Analyses estimate the change in the dependent variable in response to the change in the independent variables within individuals. This means coefficients for integration measures indicate the change in depressive symptoms associated with increased integration. Essentially, values for each respondent are de-meaned from their personal mean over time on a given measure to adjust for effects of any unobserved time-invariant individual characteristics (Allison 2009). Because fixed-effects models adjust for all time-invariant individual characteristics, the association between integration and depressive symptoms is measured net of individual or contextual heterogeneity.
Adjusting for unobserved endogeneity in this way is particularly important when examining these research questions because many unobserved factors could affect both mental health and integration. Examining within-person change rather than between-person differences avoids wrongly attributing effects of unobserved individual heterogeneity to effects of integration. Analyses functionally adjust for individuals’ average depressive symptoms and average level of integration over time to net out between-person differences in mental health and integration. As such, fixed-effects provide a strict and conservative assessment of hypotheses. Results of the Hausman test support the use of fixed rather than random effects, and Wald tests support including the grade variable indicating time fixed effects (Allison 2009). Analyses were conducted in Stata 15 (StataCorp 2017).
Analyses do not used lagged variables because lagged models provide systematically biased estimates in conjunction with fixed-effects or when there is high serial correlation and endogeneity (Achen 2000; Vaisey and Miles 2017). Testing lagged models shows that they result in significant data loss (over 10,000 cases dropped) and have worse model fit than models shown here (indicated by an AIC and lower R2 for lagged independent variable analyses when compared in the same sample). Lagged models also show substantively the same results as current models. Similarly, stochastic actor-oriented models (SAOM’s) are not appropriate here. Global embeddedness as examined in this study is currently not implemented in an SAOM, and recent work also suggests that SAOM’s do not provide better assessments of network effects compared to well-specified regression models (Ragan et al. 2019), making the current modeling strategy best for this study.
Model 1 shows the association of depressive symptoms with local cohesion and global embeddedness, net of control measures. Model 2 interacts friends’ depressive symptoms with local and global measures to test for moderation by friends’ mental health. Model 3 tests for gender moderation of local cohesion and global embeddedness, then Model 4 interacts gender with friend depression. Separate analyses for girls and boys are then shown in Models 5 and 6.
Results
Descriptive statistics for the analytic sample are shown in table 2. Key measures show typical values for adolescents. Average local cohesion is .21, suggesting that roughly 20 percent of possible ego-network connections are observed. Average global embeddedness is just under 2 out of 5, indicating that most teens have a medium level of embeddedness in the overall network, but the range and standard deviation show some are deeply nested in the core of the network (at higher embeddedness levels) while others are on the network periphery (lower embeddedness). These statistics for local cohesion and global embeddedness align with values in nationally representative samples (Falci and McNeely 2009; Moody and White 2003). As expected, girls have significantly higher average depressive levels (.35 versus .18 for boys, two-sample t-test significant at p < .001) and higher average friends’ depressive levels compared to boys (.42 versus .25, two-sample t-test significant at p < .001). This prevalence of depressive symptoms falls within the typical range for adolescents (Hankin 2006).
Table 2.
Descriptive Statistics in PROSPER Sample
| Mean or Proportion | (SD) | Min. | Max. | |
|---|---|---|---|---|
| Local cohesion | .21 | (.22) | 0 | 1 |
| Global embeddedness | 1.9 | (1.11) | 0 | 5 |
| Depressive symptoms | .27 | (.43) | 0 | 2 |
| Female sub-sample | .35 | (.46) | ||
| Male sub-sample | .18 | (.37) | ||
| Friend depression | .34 | (.27) | 0 | 2 |
| Female sub-sample | .42 | (.27) | ||
| Male sub-sample | .25 | (.24) | ||
| Male | 46% | — | 0 | 1 |
| Low SES | 21% | — | 0 | 1 |
| Biological parents | 61% | — | 0 | 1 |
| School adjustment | 3.62 | (.70) | 1 | 5 |
| Popularity | 3.11 | (2.39) | 0 | 18 |
| Gregariousness | 3.21 | (2.14) | 0 | 7 |
| Out-of-grade friends | 10.45 | (6.36) | 0 | >20 |
| Total observations | 27,091 | |||
| Grade 9 | 7,772 | |||
| Grade 10 | 7,627 | |||
| Grade 11 | 6,013 | |||
| Grade 12 | 5,679 | |||
| Total Individuals | 11,418 |
Model 1 in table 3 shows associations of local cohesion and global embeddedness with depressive symptoms after adjusting for control measures and time-invariant individual characteristics controlled by the fixed-effects model (e.g., race or gender). Increases in friend depression, popularity, and the number of out-of-grade friends are associated with increased depressive symptoms. Living with both biological parents and increased school adjustment are associated with decreased depressive symptoms. Depressive symptoms decrease over time, with Grades 11 and 12 predicting significantly lower levels of depressive symptoms compared to Grade 9. In Model 1, local cohesion and global embeddedness do not significantly predict depressive symptoms.
Table 3.
Fixed-effect Regression Results for Depressive Symptoms on Social Integration in PROSPER Sample
| M1 | (SE) | M2 | (SE) | M3 | (SE) | M4 | (SE) | |
|---|---|---|---|---|---|---|---|---|
| Local cohesion | −0.006 | (0.01) | 0.035 | (0.02) | −0.037* | (0.02) | −0.006 | (0.01) |
| Global embeddedness | −0.003 | (0.00) | −0.024*** | (0.01) | 0.012* | (0.01) | −0.003 | (0.00) |
| Local cohesion × Friend depression | −0.106* | (0.05) | ||||||
| Global embeddedness × Friend depression | 0.061*** | (0.01) | ||||||
| Local cohesion × Male | 0.075** | (0.03) | ||||||
| Global embeddedness × Male | −0.032*** | (0.01) | ||||||
| Friend depression | 0.091*** | (0.01) | 0.027 | (0.02) | 0.089*** | (0.01) | 0.116*** | (0.02) |
| Friend depression × Male | −0.061* | (0.03) | ||||||
| Popularity | 0.003* | (0.00) | 0.004* | (0.00) | 0.003 | (0.00) | 0.003* | (0.00) |
| Gregariousness | −0.004 | (0.00) | −0.004 | (0.00) | −0.004* | (0.00) | −0.004 | (0.00) |
| Low SES | −0.004 | (0.01) | −0.005 | (0.01) | −0.004 | (0.01) | −0.005 | (0.01) |
| Biological parents | −0.054** | (0.02) | −0.052** | (0.02) | −0.053** | (0.02) | −0.054** | (0.02) |
| School adjustment | −0.119*** | (0.01) | −0.119*** | (0.01) | −0.119*** | (0.01) | −0.119*** | (0.01) |
| Grade (Grade 9 Baseline) | ||||||||
| Grade 10 | 0.000 | (0.01) | 0.001 | (0.01) | 0.001 | (0.01) | 0.001 | (0.01) |
| Grade 11 | −0.015* | (0.01) | −0.013* | (0.01) | −0.014* | (0.01) | −0.014* | (0.01) |
| Grade 12 | −0.038*** | (0.01) | −0.036*** | (0.01) | −0.036*** | (0.01) | −0.037*** | (0.01) |
| Out-of-grade friends | 0.002** | (0.00) | 0.002** | (0.00) | 0.001** | (0.00) | 0.002** | (0.00) |
| Intercept | 0.709*** | (0.03) | 0.723*** | (0.03) | 0.707*** | (0.03) | 0.708*** | (0.03) |
| R 2 (Overall) | 0.090 | 0.095 | 0.113 | 0.102 | ||||
| AIC | −4,133.6 | −4,197.5 | −4,190.2 | −4,144.8 | ||||
| BIC | −4,035.1 | −4,092.6 | −4,075.3 | −4,038.1 | ||||
| Observations | 27,091 | 27,091 | 27,091 | 27,091 | ||||
| Individuals | 11,418 | 11,418 | 11,418 | 11,418 | ||||
* p < .05.
** p < .01.
*** p < .001.
Model 2 adds interactions between each type of integration and friend depression. Here, the conditional effect of global embeddedness is negatively associated with depressive symptoms. However, when friends report increased depressive symptoms, greater global embeddedness predicts increased depressive levels, consistent with Hypothesis 1. For local cohesion, the conditional effect is non-significant, but when friends’ depressive levels increase, greater local cohesion predicts decreased depressive symptoms. Local cohesion is moderated by increased friend depression, but not in the direction expected by Hypothesis 1.
Model 3 examines whether integration predicts depressive symptoms differently by gender. Gender differences are significant for both local cohesion and global embeddedness. Here, increased local cohesion predicts reduced depressive symptoms for girls and increased symptoms for boys, while greater global embeddedness predicts increased depressive levels for girls and reduced symptoms for boys. However, how the integration measures relate to depressive symptoms changes once moderation by friend depression is considered. Model 4 indicates that friend depression also differs by gender. An increase in average friend depression predicts increased depressive symptoms for girls, but significantly less so for boys.
Models 5 and 6 show separate models by gender (table 4). For girls (Model 5), results mirror those from Model 2: local cohesion reduces the extent to which increased friend depression increases individuals’ depressive levels, shown in figure 2. For girls with greater friend depression (set at one standard deviation greater than the mean), increased local cohesion essentially buffers the effects of friends’ depressive symptoms. Put differently, non-cohesive groups of more depressive friends predict increased depressive symptoms for girls. Although local cohesion is significantly moderated by friend depression, it is not in the expected direction of Hypothesis 2.
Table 4.
Fixed-effect Regression Results for Depressive Symptoms on Social Integration in PROSPER Sample, by Gender
| M5 Female | (SE) | M6 Male | (SE) | |
|---|---|---|---|---|
| Local cohesion | 0.034 | (0.03) | 0.020 | (0.03) |
| Global embeddedness | −0.023** | (0.01) | −0.016* | (0.01) |
| Local cohesion × Friend depression | −0.144* | (0.06) | 0.025 | (0.09) |
| Global embeddedness × Friend depression | 0.054*** | (0.01) | 0.038 | (0.02) |
| Friend depression | 0.057* | (0.03) | 0.011 | (0.04) |
| Popularity | 0.002 | (0.00) | 0.004 | (0.00) |
| Gregariousness | −0.000 | (0.00) | −0.007** | (0.00) |
| Low SES | −0.017 | (0.02) | 0.011 | (0.02) |
| Biological parents | −0.036 | (0.03) | −0.065* | (0.03) |
| School adjustment | −0.140*** | (0.01) | −0.095*** | (0.01) |
| Grade (Grade 9 Baseline) | ||||
| Grade 10 | −0.013 | (0.01) | 0.020* | (0.01) |
| Grade 11 | −0.038*** | (0.01) | 0.016 | (0.01) |
| Grade 12 | −0.072*** | (0.01) | 0.006 | (0.01) |
| Out-of-grade friends | 0.001 | (0.00) | 0.002* | (0.00) |
| Intercept | 0.895*** | (0.05) | 0.530*** | (0.05) |
| R 2 (Overall) | 0.129 | 0.070 | ||
| AIC | −965.3 | −3,499.0 | ||
| BIC | −859.0 | −3,395.1 | ||
| Observations | 14,709 | 12,382 | ||
| Individuals | 5,969 | 5,449 | ||
* p < .05.
** p < .01.
*** p < .001.
Figure 2.
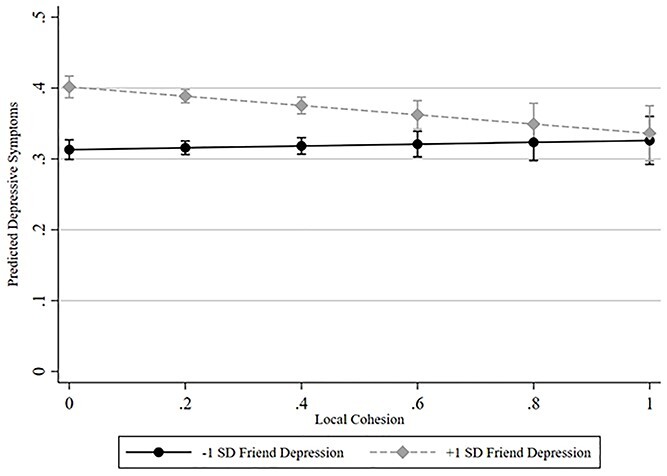
Predicted depressive symptoms by local cohesion and friend depression in PROSPER sample, girls only.
In contrast, greater global embeddedness predicts increased depressive levels when friend depression increases, and otherwise increased global embeddedness predicts decreased depressive levels. Figure 3 demonstrates this interaction for girls. Results for girls’ global embeddedness are consistent with Hypothesis 2. Thus, for girls with more depressive friends, the ideal integrative position is maximum local cohesion and minimum global embeddedness, meaning a cohesive friend group that is not deeply embedded in the overall network. While the magnitude of each association is modest, girls are simultaneously experiencing local cohesion, global embeddedness, and friend depression, so that effects may compound for more substantial associations with mental health. Similarly, effects across the range of friend depression and integration positions shows that girls with more extreme social experiences may face substantial risks or benefits of mental health.
Figure 3.
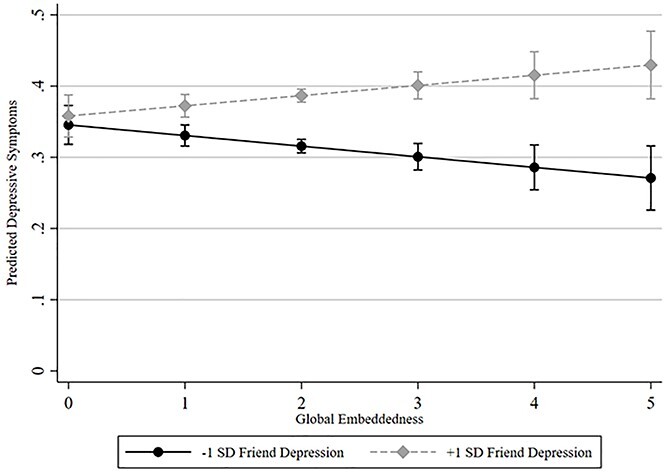
Predicted depressive symptoms by global embeddedness and friend depression in PROSPER sample, girls only.
For boys in Model 6 (comparable figures for boys shown in the appendix figure S2), increased friend depression and local cohesion do not predict boys’ own depressive levels. Although modest in magnitude, greater global embeddedness is associated with decreased depressive levels. This effect does not depend on friend depression for boys, consistent with Hypothesis 3.
Robustness
Results are robust to several other specifications. Modeling a log of depressive symptoms shows the same pattern of results. Results of Poisson models with a count dependent variable (shown in the appendix) have a few minor differences from models shown here: in Model 2, local cohesion and friend depression significantly predict depressive levels, but the overall association between local cohesion and friend depression with depressive levels remains the same. The interaction between male and friend depression is nonsignificant in Model 4, but friend depression continues to be significant for girls and nonsignificant for boys in separate gender models, and the interaction between global embeddedness and friend depression is also significant for boys in Model 6. Compared to Poisson models, those shown here provide the least sample loss and the most conservative results. Results after removing outliers or network isolates are consistent with those shown here, with one exception: after removing network isolates, global embeddedness no longer significantly predicts boys’ depressive symptoms, discussed further below. Being in the treatment or control condition of the larger PROSPER substance use intervention is nonsignificant and does not substantively change results.
Discussion
Social integration in networks can positively and negatively affect well-being (Falci and McNeely 2009; Granovetter 1985; Moody and White 2003). Individuals are simultaneously embedded in multiple levels of network structure, experiencing both local cohesion among close friends and global embeddedness in the overall network. Moreover, both network structure and context relate to health, so that characteristics such as gender and friends’ mental health may moderate any associations between integration and mental health. This study combines these key elements of teen peer networks to examine local and global integration predicting depressive symptoms, moderated by gender and friend depression. Results clarify the conditions under which integration relates to mental health. Results examining within-person change show that structural integration is indeed multi-dimensional, as local cohesion and global embeddedness relate differently to depressive symptoms in ways that vary with gender and friends’ depression.
Results for global embeddedness indicate that increased embeddedness in the network generally relates to decreased depressive levels, consistent with Hypothesis 1. This result is net of popularity (being named as a friend), gregariousness (naming more friends), and school adjustment. Teens’ structural embeddedness matters for mental health, separate from number of friends or feelings toward school. Global embeddedness may provide status, belongingness, or increased investment in the school context that reduces depressive levels. This result supports structural approaches to understanding social relations, adding global embeddedness to examinations of centrality, dyads, or perceptions of relations. This finding aligns with prior work emphasizing benefits of structural embeddedness (Moody and White 2003) and extends theories of embeddedness (Granovetter 1985) to teen mental health. This result also supports theories of the broader school peer context, beyond direct ties, as a key environment affecting teens’ well-being (Coleman 1961; Guan and Kamo 2016; Lee and Lee 2020).
These benefits of increased global embeddedness persist for boys in final models. Notably, robustness checks show that this benefit for boys is no longer statistically significant if isolated youth with zero ties are removed from the sample. This non-significance may suggest that the greatest risk for boys is isolation, or this pattern may stem from lower statistical power after removing cases, as future research should investigate.
For girls, however, effects of global embeddedness are contingent on friends’ mental health: greater embeddedness generally predicts lower depressive levels but when friend depression increases, deeper global embeddedness predicts increased depressive symptoms, consistent with Hypothesis 2. This finding aligns with prior studies finding that high peer status can harm girls’ mental health (Kamis and Copeland 2020; Kornienko and Santos 2014). For example, being more deeply nested in the network may increase scrutiny or pressure to maintain status, which may become stressful for girls with increasingly depressive friends. As girls are more attentive to wider peer perceptions, occupying a more visible position may become more stressful when friends are exhibiting stigmatized depressive symptoms. Alternatively, deeply embedded girls might be more invested in the social context in general so that their mental health is more sensitive to negative experiences of more depressive friends. This study does not test mechanisms and cannot adjudicate between such explanations. This result presents an interesting area for further inquiry across network levels, as the mental health status of ego-network friends moderates associations between mental health and girls’ embeddedness in the overall network. Future work should examine the exact mechanisms that link friends’ depression, global embeddedness, and girls’ depressive levels, and should consider if such patterns extend to boys, as interactions between global embeddedness and friends’ depression were significant for boys in sensitivity analyses using Poisson.
Results for local cohesion show a different pattern. In final models, local cohesion is unrelated to depressive symptoms for boys, as expected (Hypothesis 3). Girls’ local cohesion predicts depressive symptoms only when friends are experiencing more depressive symptoms. Increasingly depressive friends predict greater symptoms for girls, but less so when in cohesive friend groups. Put differently, local non-integration predicts worse mental health for girls with more depressive friends. This result for girls does not support Hypotheses 1 and 2, as local cohesion is only significant when friends are more depressive, and not in the expected direction. While unexpected, this pattern is not implausible: increasingly depressive friends may spur conflict, demands for support, or co-rumination in ways that are stressful among disconnected friends, but better managed in cohesive groups. This finding suggests that local cohesion can buffer greater peer depression for girls, aligning with prior work finding that friends’ distress (Rose and Rudolph 2006) and structures of local integration (Bearman and Moody 2004; Falci and McNeely 2009) affect girls’ mental health.
Results indicate gender differences in how networks and friends’ depression relate to teens’ mental health. Unlike global embeddedness, local cohesion and friend depression do not significantly affect boys’ depressive symptoms. These results are consistent with expectations of boys seeking dominant, high-status positions among peers (Shin 2017) and avoiding emotional disclosure or support-seeking in close friendships (Kornienko and Santos 2014). Girls’ mental health is affected by relational content (e.g., friend depression) and by structural patterns that can mitigate risks of depressive friends (e.g., greater local cohesion) or intensify them (e.g., greater global embeddedness). These results align with theories suggesting women are socialized to prioritize others, adopt “tend and befriend” approaches, and be attentive to their social standing among others (Rose and Rudolph 2006; Rosenfield, 2012).
While at first glance, the magnitude of effects of local cohesion and global embeddedness are modest, there are several reasons why patterns here may relate to substantial impacts on mental health. First, both types of integration and friends’ depression are experienced simultaneously in ways that may compound effects. Second, results here also provide insight into a snapshot of what is likely an unfolding process across adolescence so that effects may compound over time for more substantial effects on mental health. Third, the effects across the range of integration measures and friends’ depression indicate that potential effects can be substantial, especially for some young women with more depressive friends. Together, results provide theoretical and empirical insight into wider processes of how different levels of network integration and relational context may relate to teen mental health.
While this analysis examines teens, three main research implications apply beyond adolescence. First, treating integration as a monolithically beneficial concept overlooks important variation in how levels of network structure relate to health. Examining local and global structures jointly but separately clarifies how distinct, simultaneously experienced positions relate to well-being. For example, considering only close ties or overall network position fails to account for the interplay between close friends’ mental health and position in the wider network for girls. This study demonstrates the importance of conceptualizing multiple levels of networks in which individuals are embedded that can have different structural characteristics and distinct consequences for health (Brailly et al. 2016; Pescosolido 2015; Pescosolido et al. 2016).
Second, results here echo calls to recognize the importance of jointly examining integration and contextually salient characteristics (e.g., Pescosolido 2006). Examining both structural and contextual features of networks indicates the contingent importance of both for mental health. Here, gender and friends’ depression shape effects of network structure, and future work should consider how other characteristics may moderate social integration.
Third, researchers must also recognize gender differences in how network structures and mental health contexts relate to well-being. Associations may be misconstrued if separate patterns by gender are not considered. For example, in the full sample (Model 2), it appears that friend depression moderates integration for all youth, but after separating by gender, this pattern is largely irrelevant for boys. While further investigation is needed into exact mechanisms, especially those linking friends’ mental health and global network position, gendered processes clearly shape how integration affects well-being.
Some limitations in this study suggest areas for future research. This survey does not assess diagnoses or medications, and youth receiving treatment may not appear depressive. Future work should consider the impact of networks on depression diagnosis, treatment, or medication. Network measures are restricted to friendships within the in-grade network survey boundary and capture one annual snapshot of friendships. Youth who appear relatively unintegrated here may be more integrated in non-school social environments. Such a pattern makes results here conservative if youth that appear less integrated are really integrated elsewhere, where they also might encounter exposure to friends’ depression. The survey includes adolescents in Iowa and Pennsylvania, which may not generalize to all teens. Future research should consider more diverse, representative samples. Despite adjusting for unobserved endogeneity through fixed-effects, analyses do not fully establish causality or track depressive trajectories. Future research should examine mechanisms, particularly those that link contextual features of close friendships and overall network position. Another key area for research is how these processes unfold over time to distinguish causal, co-evolving effects of local cohesion, global embeddedness, and mental health.
Results suggest that practitioners might consider how social integration among school peers can relate to mental health for youth. Girls with more depressive friends who are deeply embedded in the overall school or in non-cohesive friend groups may appear more socially connected than the typical profile of at-risk youth, but still face significant risks to mental health from their social position. Practitioners should additionally consider how global embeddedness can provide a beneficial resource for mental health, particularly for boys.
This work disentangles how distinct levels of network structure, in conjunction with gender and friends’ mental health, relate to adolescent depressive symptoms. Results show the importance of peer relationships for teen mental health and the need to consider contextual features that shape how social networks relate to health. This study advances research on social networks, gender, and mental health to inform our understanding of social integration related to well-being.
Supplementary Material
Endnotes
Granovetter (1992) calls these levels “relational” and “structural”, but as these terms are now more often used to distinguish tie content from tie structure, I use the terms local and global.
Associations between integration and mental health could also indicate depressive levels affecting networks. Depressive symptoms may reduce induce withdrawal or avoidance (Schaefer, Kornienko, and Fox 2011), or stigma may reduce depressive teens’ integration (Siennick and Picon 2019). Examining associations of local and global dimensions of integration with depressive levels provides a next step in clarifying how integration relates to mental health, which can then be extended to consider how processes co-evolve.
About the Author
Molly Copeland is an Assistant Professor in the Department of Sociology at Michigan State University. Her research examines social networks and health across the life course, particularly adolescent peer networks and mental health. Her recent work has been published in the Journal of Health and Social Behavior, Archives of Suicide Research, Journal of Youth and Adolescence, and Network Science.
References
- Abrutyn, Seth and Anna S. Mueller 2016. “When Too Much Integration and Regulation Hurts: Reenvisioning Durkheim’s Altruistic Suicide.” Society and Mental Health 6(1):56–71. 10.1177/2156869315604346. [DOI] [Google Scholar]
- Achen, Christopher H. 2000. “Why Lagged Dependent Variables Can Suppress the Explanatory Power of Other Independent Variables.” In Annual Meeting of the Political Methodology Section of the American Political Science Association, 1–40.
- Allen, Joseph P., Joanna Chango, David Szwedo and Megan Schad 2014. “Long-Term Sequelae of Subclinical Depressive Symptoms in Early Adolescence.” Development and Psychopathology 26(1):171–80. 10.1017/S095457941300093X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allison, Paul D. 2002. Missing Data. Thousand Oaks, California: Sage Publications. doi: 10.4135/9781412985079. [DOI] [Google Scholar]
- Allison, Paul D. 2009. Fixed Effects Regression Models. Los Angeles: Sage Publications. [Google Scholar]
- Almquist, Ylva 2011. “Social Isolation in the Classroom and Adult Health: A Longitudinal Study of a 1953 Cohort.” Advances in Life Course Research 16(1):1–12. 10.1016/j.alcr.2010.11.001. [DOI] [Google Scholar]
- American Psychiatric Association 2000. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC. [Google Scholar]
- Bastomski, Sara, Noli Brazil and Andrew V. Papachristos 2017. “Neighborhood Co-Offending Networks, Structural Embeddedness, and Violent Crime in Chicago.” Social Networks 51:23–39. 10.1016/j.socnet.2016.12.003. [DOI] [Google Scholar]
- Bearman, Peter S. and James Moody 2004. “Suicide and Friendships among American Adolescents.” American Journal of Public Health 94(1):89–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brailly, Julien, Guillaume Favre, Josiane Chatellet and Emmanuel Lazega 2016. “Embeddedness as a Multilevel Problem: A Case Study in Economic Sociology.” Social Networks 44:319–33. 10.1016/j.socnet.2015.03.005. [DOI] [Google Scholar]
- Cheadle, Jacob E. and Bridget J. Goosby 2012. “The Small-School Friendship Dynamics of Adolescent Depressive Symptoms.” Society and Mental Health 2(2):99–119. 10.1177/2156869312445211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cillessen, Antonius H.N. and Amy D. Bellmore 1999. “Accuracy of Social Self-Perceptions and Peer Competence in Middle Childhood.” Merrill-Palmer Quarterly 45(4):650–76. [Google Scholar]
- Coleman, James S. 1961. The Adolescent Society: The Social Life of the Teenager and Its Impact on Education. Glencoe, IL: Free Press. [Google Scholar]
- Copeland, Molly, Sonja E. Siennick, Mark E. Feinberg, James Moody and Daniel T. Ragan 2019. “Social Ties Cut Both Ways: Self-Harm and Adolescent Peer Networks.” Journal of Youth and Adolescence 48(8):1506–18. 10.1007/s10964-019-01011-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornwell, Benjamin 2003. “The Dynamic Properties of Social Support: Decay, Growth, and Staticity, and Their Effects on Adolescent Depression.” Social Forces 81(3):953–78. 10.1353/sof.2003.0029. [DOI] [Google Scholar]
- Coyne, James C. 1976. “Toward an Interactional Description of Depression.” Psychiatry 39(1):28–40. 10.1080/00332747.1976.11023874. [DOI] [PubMed] [Google Scholar]
- Durkheim, Emile 2006. [1897]. On Suicide. London: Penguin. [Google Scholar]
- Falci, Christina and Clea McNeely 2009. “Too Many Friends: Social Integration, Network Cohesion and Adolescent Depressive Symptoms.” Social Forces 87(4):2031–61. 10.1353/sof.0.0189. [DOI] [Google Scholar]
- Faris, Robert 2012. “Aggression, Exclusivity, and Status Attainment in Interpersonal Networks.” Social Forces 90(4):1207–35. 10.1093/sf/sos074. [DOI] [Google Scholar]
- Granovetter, Mark S. 1973. “The Strength of Weak Ties.” The American Journal of Sociology 78(6):1360–80. 10.1086/225469. [DOI] [Google Scholar]
- Granovetter, Mark S. 1985. “Economic Action and Social Structure: The Problem of Embeddedness.” American Journal of Sociology 91(3):481–510. 10.1086/228311. [DOI] [Google Scholar]
- Granovetter, Mark S. 1992. “Problems of Explanation in Economic Sociology”. In Networks and Organizations: Structure, Form, and Action, edited by Nohria, N., Eccles, R.G., pp. 25–56. Boston, MA: Harvard Business School Press. [Google Scholar]
- La Greca, Annette M. and Hannah Moore Harrison 2005. “Adolescent Peer Relations, Friendships, and Romantic Relationships: Do They Predict Social Anxiety and Depression.” Journal of Clinical Child and Adolescent Psychology 34(1):49–61. 10.1207/s15374424jccp3401_5. [DOI] [PubMed] [Google Scholar]
- Guan, Win and Yoshinori Kamo 2016. “Contextualizing Depressive Contagion: A Multilevel Network Approach.” Society and Mental Health 6(2):129–45. 10.1177/2156869315619657. [DOI] [Google Scholar]
- Haas, Steven A., David R. Schaefer and Olga Kornienko 2010. “Health and the Structure of Adolescent Social Networks.” Journal of Health and Social Behavior 51(4):424–39. 10.1177/0022146510386791. [DOI] [PubMed] [Google Scholar]
- Hankin, Benjamin L. 2006. “Adolescent Depression: Description, Causes, and Interventions.” Epilepsy and Behavior 8(1):102–14. 10.1016/j.yebeh.2005.10.012. [DOI] [PubMed] [Google Scholar]
- Hartwell, Stephanie W. and Paul R. Benson 2007. “Social Integration: A Conceptual Overview and Two Case Studies”. In Mental Health, Social Mirror, pp. 329–53. New York, NY: Springer. [Google Scholar]
- Haynie, Dana L. 2001. “Delinquent Peers Revisited: Does Network Structure Matter?” American Journal of Sociology 106(4):1013–57. 10.1086/320298. [DOI] [Google Scholar]
- Kamis, Christina and Molly Copeland 2020. “The Long Arm of Social Integration: Gender, Adolescent Social Networks, and Adult Depressive Symptoms.” Journal of Health and Social Behavior 61(4):437–52. 10.1177/0022146520952769. [DOI] [PubMed] [Google Scholar]
- Kawachi, Ichiro and Lisa F. Berkman 2001. “Social Ties and Mental Health.” Journal of Urban Health: Bulletin of the New York Academy of Medicine 78(3):458–67. 10.1093/jurban/78.3.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kornienko, Olga, Katherine H. Clemans, Dorothée Out and Douglas A. Granger 2013. “Friendship Network Position and Salivary Cortisol Levels.” Social Neuroscience 8(4):385–96. 10.1080/17470919.2013.795500. [DOI] [PubMed] [Google Scholar]
- Kornienko, Olga and Carlos E. Santos 2014. “The Effects of Friendship Network Popularity on Depressive Symptoms During Early Adolescence: Moderation by Fear of Negative Evaluation and Gender.” Journal of Youth and Adolescence 43(4):541–53. 10.1007/s10964-013-9979-4. [DOI] [PubMed] [Google Scholar]
- Lee, Dohoon and Byungkyu Lee 2020. “The Role of Multilayered Peer Groups in Adolescent Depression: A Distributional Approach.” American Journal of Sociology 125(6):1513–58. 10.1086/709425. [DOI] [Google Scholar]
- McGloin, Jean Marie, Christopher J. Sullivan and Kyle J. Thomas 2014. “Peer Influence and Context: The Interdependence of Friendship Groups, Schoolmates and Network Density in Predicting Substance Use.” Journal of Youth and Adolescence 43(9):1436–52. 10.1007/s10964-014-0126-7. [DOI] [PubMed] [Google Scholar]
- McMillan, Cassie, Diane Felmlee and D.W. Osgood 2018. “Peer Influence, Friend Selection, and Gender: How Network Processes Shape Adolescent Smoking, Drinking, and Delinquency.” Social Networks 55:86–96. 10.1016/j.socnet.2018.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moody, James and Douglas R. White 2003. “Structural Cohesion and Embeddedness: A Hierarchical Concept of Social Groups.” American Sociological Review 68(1):103–27. 10.2307/3088904. [DOI] [Google Scholar]
- Pescosolido, Bernice A. 2015. “Linking the Social Brain to the Social World through Network Connections”. In Social Neuroscience: Brain, Mind, and Society, edited by Schutt, Russel K., Seidman, Larry J., Keshavan, Matcheri S., pp. 247–79. Cambridge, MA: Harvard University Press. [Google Scholar]
- Pescosolido, Bernice A., Sigrun Olafsdottir, Olaf Sporns, Brea L. Perry, Eric M. Meslin, Tony H. Grubesic, Jack K. Martin et al. 2016. “The Social Symbiome Framework: Linking Genes-to-Global Cultures in Public Health Using Network Science”. In Handbook of Applied System Science, edited by Neal, Zachary P., pp. 25–48. New York, NY: Routledge. [Google Scholar]
- Pescosolido, Bernice A. 1992. “Beyond Rational Choice: The Social Dynamics of How People Seek Help.” American Journal of Sociology 97(4):1096–138. 10.1086/229863. [DOI] [Google Scholar]
- Pescosolido, Bernice A. 2006. “Of Pride and Prejudice: The Role of Sociology and Social Networks in Integrating the Health Sciences.” Journal of Health and Social Behavior 47(3):189–208. 10.1177/002214650604700301. [DOI] [PubMed] [Google Scholar]
- Prinstein, Mitchell J. and Matteo Giletta 2014. “Peer Relations and Developmental Psychopathology”. In Developemental Psychopathology, D. Cicchetti (Ed.). Vol. I, 3rd edn, pp. 527–79. 10.1002/9781119125556.devpsy112. [DOI] [Google Scholar]
- Prinstein, Mitchell J. and Shirley S. Wang 2005. “False Consensus and Adolescent Peer Contagion: Examining Discrepancies between Perceptions and Actual Reported Levels of Friends’ Deviant and Health Risk Behaviors.” Journal of Abnormal Child Psychology 33(3):293–306. 10.1007/s10802-005-3566-4. [DOI] [PubMed] [Google Scholar]
- Ragan, Daniel T., D. Wayne Osgood and Mark E. Feinberg 2014. “Friends as a Bridge to Parental Influence: Implications for Adolescent Alcohol Use.” Social Forces 92(3):1061–85. 10.1093/sf/sot117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ragan, Daniel T., D.W. Osgood, Nayan G. Ramirez, James Moody and Scott D. Gest 2019. “A Comparison of Peer Influence Estimates from SIENA Stochastic Actor–Based Models and from Conventional Regression Approaches.” Sociological Methods & Research 51(1):357–95. 10.1177/0049124119852369. [DOI] [Google Scholar]
- Reigeluth, Christopher S. and Michael E. Addis 2015. “Adolescent Boys’ Experiences With Policing of Masculinity: Forms, Functions, and Consequences.” Psychology of Men & Masculinity 17(1):74–83. 10.1037/a0039342. [DOI] [Google Scholar]
- Reynolds, Andrew D. and Thomas M. Crea 2015. “Peer Influence Processes for Youth Delinquency and Depression.” Journal of Adolescence 43(1):83–95. 10.1016/j.adolescence.2015.05.013. [DOI] [PubMed] [Google Scholar]
- Ridgeway, Cecilia L. and Shelley J. Correll 2004. “Unpacking the Gender System a Theoretical Perspective on Gender Beliefs and Social Relations.” Gender and Society 18(4):510–31. 10.1177/0891243204265269. [DOI] [Google Scholar]
- Rose, Amanda J. and Karen D. Rudolph 2006. “A Review of Sex Differences in Peer Relationship Processes: Potential Trade-Offs for the Emotional and Behavioral Development of Girls and Boys.” Psychological Bulletin 132(1):98–131. 10.1037/0033-2909.132.1.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenfield, Sarah 2012. “Triple Jeopardy? Mental Health at the Intersection of Gender, Race, and Class.” Social Science and Medicine 74(11):1791–801. 10.1186/s40608-016-0102-8. [DOI] [PubMed] [Google Scholar]
- Rosenfield, Sarah and Dawne Mouzon 2013. “Gender and Mental Health”. In Handbook of the Sociology of Mental Health, edited by Aneshensel, Carol S., Phelan, Jo C., Bierman, Alex, 2nd edn, pp. 277–96. New York: Springer. [Google Scholar]
- Schaefer, David R., Olga Kornienko and Andrew M. Fox 2011. “Misery Does Not Love Company: Network Selection Mechanisms and Depression Homophily.” American Sociological Review 76(5):764–85. 10.1177/0003122411420813. [DOI] [Google Scholar]
- Schwartz-Mette, Rebecca A., Jessica Shankman, Aubrey R. Dueweke, Sarah Borowski and Amanda J. Rose 2020. “Relations of Friendship Experiences with Depressive Symptoms and Loneliness in Childhood and Adolescence: A Meta-Analytic Review.” Psychological Bulletin 146(8):664–700. 10.1037/bul0000239. [DOI] [PubMed] [Google Scholar]
- Shin, Huiyoung 2017. “Friendship Dynamics of Adolescent Aggression, Prosocial Behavior, and Social Status: The Moderating Role of Gender.” Journal of Youth and Adolescence 46(11):2305–20. 10.1007/s10964-017-0702-8. [DOI] [PubMed] [Google Scholar]
- Siennick, Sonja E. and Mayra Picon 2019. “Adolescent Internalizing Symptoms and the ‘Tightknittedness’ of Friendship Groups.” Journal of Research on Adolescence 30 Suppl 2:391–402. 10.1111/jora.12484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simon, R.W. 2020. “Gender, Emotions, and Mental Health in the United States: Patterns, Explanations, and New Directions.” Society and Mental Health. 10(2):97–111. 10.1177/2156869320926236. [DOI] [Google Scholar]
- Smith, Jeffrey A., James Moody and Jonathan H. Morgan 2017. “Network Sampling Coverage II: The Effect of Non-Random Missing Data on Network Measurement.” Social Networks 48:78–99. 10.1016/j.socnet.2016.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth, R., C. Redmond, C. Shin, M. Greenberg, M. Feinberg and L. Schainker 2013. “PROSPER Community-University Partnership Delivery System Effects on Substance Misuse Through 6 1/2 Years Past Baseline From a Cluster Randomized Controlled Intervention Trial.” Preventive Medicine 56(3–4):190–6. 10.1016/j.ypmed.2012.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spoth, R., M. Greenberg, K. Bierman and C. Redmond 2004. “PROSPER Community-University Partnership Model for Public Education systems: Capacity-Building for Evidence-based, Competence-Building Prevention.” Prevention Science 5(1):31–9. 10.1023/B:PREV.0000013979.52796.8b. [DOI] [PubMed] [Google Scholar]
- StataCorp 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC. [Google Scholar]
- Suh, Chan S., Yongren Shi and Matthew E. Brashears 2017. “Negligible Connections? The Role of Familiar Others in the Diffusion of Smoking among Adolescents.” Social Forces 96(1):423–48. 10.1093/sf/sox046. [DOI] [Google Scholar]
- Turner, Heather A. and R. Jay Turner 1999. “Gender, Social Status, and Emotional Reliance.” Journal of Health and Social Behavior 40(4):360–73. 10.2307/2676331. [DOI] [PubMed] [Google Scholar]
- Ueno, Koji 2005. “The Effects of Friendship Networks on Adolescent Depressive Symptoms.” Social Science Research 34(3):484–510. 10.1016/j.ssresearch.2004.03.002. [DOI] [Google Scholar]
- Umberson, Debra, Robert Crosnoe and Corinne Reczek 2010. “Social Relationships and Health Behavior across Life Course.” Annual Review of Sociology 36(1):139–57. 10.1146/annurev-soc-070308-120011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaisey, Stephen and Andrew Miles 2017. “What You Can—and Can’t—Do With Three-Wave Panel Data.” Sociological Methods & Research 46(1):44–67. 10.1177/0049124114547769. [DOI] [Google Scholar]
- Wasserman, Stanley S. and Katherine Faust 1994. Social Network Analysis: Methods and Applications Vol. 8. Cambridge, UK: Cambridge University Press. [Google Scholar]
- Wooldridge, Jeffrey M. 2012. Introductory Econometrics: A Modern Approach, 5th edn. Mason, OH: South-Western, Cengage Learning. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.