

Abstract
Empirical evidence indicates a significant bidirectional association between mental disorders and physical diseases, but the prospective impact of mental disorders on clinical outcomes of physical diseases has not been comprehensively outlined. In this PRISMA‐ and COSMOS‐E‐compliant umbrella review, we searched PubMed, PsycINFO, Embase, and Joanna Briggs Institute Database of Systematic Reviews and Implementation Reports, up to March 15, 2022, to identify systematic reviews with meta‐analysis that examined the prospective association between any mental disorder and clinical outcomes of physical diseases. Primary outcomes were disease‐specific mortality and all‐cause mortality. Secondary outcomes were disease‐specific incidence, functioning and/or disability, symptom severity, quality of life, recurrence or progression, major cardiac events, and treatment‐related outcomes. Additional inclusion criteria were further applied to primary studies. Random effect models were employed, along with I2 statistic, 95% prediction intervals, small‐study effects test, excess significance bias test, and risk of bias (ROBIS) assessment. Associations were classified into five credibility classes of evidence (I to IV and non‐significant) according to established criteria, complemented by sensitivity and subgroup analyses to examine the robustness of the main analysis. Statistical analysis was performed using a new package for conducting umbrella reviews (https://metaumbrella.org). Population attributable fraction (PAF) and generalized impact fraction (GIF) were then calculated for class I‐III associations. Forty‐seven systematic reviews with meta‐analysis, encompassing 251 non‐overlapping primary studies and reporting 74 associations, were included (68% were at low risk of bias at the ROBIS assessment). Altogether, 43 primary outcomes (disease‐specific mortality: n=17; all‐cause mortality: n=26) and 31 secondary outcomes were investigated. Although 72% of associations were statistically significant (p<0.05), only two showed convincing (class I) evidence: that between depressive disorders and all‐cause mortality in patients with heart failure (hazard ratio, HR=1.44, 95% CI: 1.26‐1.65), and that between schizophrenia and cardiovascular mortality in patients with cardiovascular diseases (risk ratio, RR=1.54, 95% CI: 1.36‐1.75). Six associations showed highly suggestive (class II) evidence: those between depressive disorders and all‐cause mortality in patients with diabetes mellitus (HR=2.84, 95% CI: 2.00‐4.03) and with kidney failure (HR=1.41, 95% CI: 1.31‐1.51); that between depressive disorders and major cardiac events in patients with myocardial infarction (odds ratio, OR=1.52, 95% CI: 1.36‐1.70); that between depressive disorders and dementia in patients with diabetes mellitus (HR=2.11, 95% CI: 1.77‐2.52); that between alcohol use disorder and decompensated liver cirrhosis in patients with hepatitis C (RR=3.15, 95% CI: 2.87‐3.46); and that between schizophrenia and cancer mortality in patients with cancer (standardized mean ratio, SMR=1.74, 95% CI: 1.41‐2.15). Sensitivity/subgroup analyses confirmed these results. The largest PAFs were 30.56% (95% CI: 27.67‐33.49) for alcohol use disorder and decompensated liver cirrhosis in patients with hepatitis C, 26.81% (95% CI: 16.61‐37.67) for depressive disorders and all‐cause mortality in patients with diabetes mellitus, 13.68% (95% CI: 9.87‐17.58) for depressive disorders and major cardiac events in patients with myocardial infarction, 11.99% (95% CI: 8.29‐15.84) for schizophrenia and cardiovascular mortality in patients with cardiovascular diseases, and 11.59% (95% CI: 9.09‐14.14) for depressive disorders and all‐cause mortality in patients with kidney failure. The GIFs confirmed the preventive capacity of these associations. This umbrella review demonstrates that mental disorders increase the risk of a poor clinical outcome in several physical diseases. Prevention targeting mental disorders – particularly alcohol use disorders, depressive disorders, and schizophrenia – can reduce the incidence of adverse clinical outcomes in people with physical diseases. These findings can inform clinical practice and trans‐speciality preventive approaches cutting across psychiatric and somatic medicine.
Keywords: Mental disorders, physical diseases, outcomes, disease‐specific mortality, all‐cause mortality, trans‐speciality prevention
Both physical diseases and mental disorders contribute significantly to the increasing burden on health care systems worldwide1, 2. Cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes are accountable for more than 50% of global deaths 1 , while mental disorders are the third leading cause of disease burden, with depressive disorders accounting for 37% of all years of life lost to disability, followed by anxiety disorders (23%) and schizophrenia (12%) 2 .
The Cartesian dichotomy of mental disorder‐physical disease is challenged by empirical evidence from primary studies 3 , meta‐analyses3, 4, 5, 6, 7, and umbrella reviews8, 9 showing significant prospective associations between the two realms. For instance, individuals with schizophrenia, compared to the general population, have a higher incidence of metabolic and cardiovascular diseases and of cancer10, 11, 12, 13; those with mood disorders are at higher risk of developing cancer and diabetes mellitus7, 14; and those with borderline personality disorder have a higher risk to develop a gastrointestinal disease, arthritis and chronic pain. Moreover, mental disorders have been found to increase the burden of physical diseases10, 15, 16.
Neurobiologically, the core mechanisms that are likely to drive the neuroprogression of mental disorders – such as inflammation, oxidative stress, apoptosis, and mitochondrial dysfunction – overlap with the mechanisms driving somatoprogression 17 . Moreover, mental disorders interfere with adherence to healthy behaviors and treatment 18 . Consequently, the occurrence of mental disorders often worsens the prognosis of physical diseases. For example, depressive and anxiety disorders are associated with a higher mortality risk in people with cancer19, 20, cardiovascular diseases21, 22, chronic obstructive pulmonary disease 23 , and diabetes mellitus24, 25. The recent COVID‐19 pandemic has also indicated that mental disorders are associated with higher disease severity and mortality26, 27, 28.
Despite this accumulating evidence, studies concerning the impact of mental disorders on clinical outcomes of physical diseases are often restricted to small sets of associations, sometimes with conflicting results, and therefore hold limited clinical relevance 9 . Relevant confounders, such as differences in diagnostic methods, the timing of the diagnosis of mental disorders 9 and the effect of psychiatric medications 12 , have not been systematically controlled for. Furthermore, the observed associations have generally not been appraised using established classification criteria to grade the credibility of the evidence and control for several types of biases.
Another limitation is that the reported associations are not directly informative for clinical practice. For example, it is unclear to what extent preventive approaches for mental disorders could reduce the incidence of clinical outcomes of physical diseases. To address this question, it is essential to quantify the proportional reduction of disease that would occur if a given risk factor is eliminated (population attributable fraction, PAF) 29 , or partially reduced (generalized impact fraction, GIF)30, 31, 32, in a specific population. To our knowledge, no study has estimated the meta‐analytic PAF or GIF of the most robust associations between mental disorders and clinical outcomes in patients with physical diseases.
This is the first umbrella review comprehensively summarizing the evidence concerning the prospective impact of mental disorders on clinical outcomes of physical diseases using established classification criteria of evidence that address multiple biases33, 34, 35, controlling for relevant confounders, and estimating the related meta‐analytic PAF and GIF. Providing a solid and rigorous synthesis of this evidence is crucial to promote sound etiopathological research and to implement effective preventive strategies cutting across psychiatry and somatic medicine 36 .
METHODS
We followed the Preferred Reporting Items for Systematic Reviews and Meta‐analyses (PRISMA) 2020 statement 37 and the Conducting Systematic Reviews and Meta‐Analyses of Observational Studies of Etiology (COSMOS‐E) guidelines 38 . The study protocol is available at the Center for Open Science (https://osf.io/dt4fu).
Search strategy and selection criteria
We systematically searched PubMed, PsycINFO, Embase, and Joanna Briggs Institute Database of Systematic Reviews and Implementation Reports from inception to March 15, 2022, to identify systematic reviews with meta‐analysis that examined the prospective association between any mental disorder and clinical outcomes of physical diseases. Primary outcomes were disease‐specific and all‐cause mortality. Secondary outcomes were disease‐specific incidence, functioning and/or disability, symptom severity, quality of life, recurrence and progression, major cardiac events, and treatment‐related outcomes.
Categories of mental disorders were stratified according to the corresponding ICD‐10 diagnostic blocks, in line with previous studies39, 40, and defined by standard diagnostic criteria or requirements (i.e., any version of the ICD or the DSM), or established diagnostic research criteria (e.g., Research Diagnostic Criteria 41 ), or validated assessment instruments with cut‐offs that map onto discrete ICD/DSM diagnoses (e.g., Patient Health Questionnaire 42 ).
We focused on categories of physical diseases associated with the highest burden according to the 2019 Global Burden of Disease Study 1 and other recent studies 11 : cardiovascular diseases (e.g., coronary heart disease), chronic respiratory diseases (e.g., chronic obstructive pulmonary disease), neurological diseases (e.g., multiple sclerosis), nutritional and metabolic diseases (e.g., obesity), endocrine system diseases (e.g., diabetes mellitus), kidney diseases, neoplasms, digestive diseases (e.g., liver cirrhosis), infectious diseases (e.g., human immunodeficiency virus, HIV infection), and musculoskeletal diseases (e.g., low back pain).
As a search strategy, we combined key terms and Medical Subject Headings (MeSH) terms related to these categories of mental disorders and physical diseases with terms related to the clinical outcomes of interest and to systematic reviews or meta‐analyses (full details are described in supplementary information). The reference lists of the records identified during the screening process were also searched. Four independent investigators screened the records based on title and abstract reading. After excluding those that were not relevant, the full texts of the remaining records were further assessed for inclusion. Any discrepancy was solved through discussions with a fifth senior investigator.
We included: a) systematic reviews with meta‐analysis of observational studies with a prospective design, with meta‐analytic summary estimates derived from at least two primary studies; b) primarily investigating the association between mental disorders and clinical outcomes of physical diseases (defined as above); c) published in English.
We excluded: a) systematic reviews without meta‐analysis; b) systematic reviews with meta‐analysis of individual participant data or network meta‐analysis; c) systematic reviews with meta‐analysis of randomized controlled trials, interventions, study designs other than prospective (cross‐sectional and retrospective case‐control studies are subject to recall bias and reverse causality); d) meta‐analyses of data not identified via systematic reviews; e) meta‐analyses mixing mental disorders and physical diseases without providing distinguishable association measures; e) systematic reviews or meta‐analyses using unclear diagnostic criteria not operationalized as above; f) fully overlapping datasets.
When two systematic reviews or meta‐analyses presented overlapping data on the same association, only the one with the largest dataset in terms of number of primary studies was retained for the specific association (the two meta‐analyses could be non‐overlapping for other associations). In the case of similar datasets, we selected the meta‐analysis with the highest study quality. When two meta‐analyses presented minimally overlapping or not overlapping datasets, nevertheless still addressing the same association, both meta‐analyses were included.
Additional inclusion/exclusion criteria were applied to each of the primary studies included in the systematic reviews. Primary study‐level inclusion criteria were: a) prospective cohort or longitudinal study (if a meta‐analysis included multiple study designs such as randomized controlled trials and prospective studies, we only retained prospective studies); b) examining longitudinally the impact of a mental disorder on clinical outcomes of a physical disease (defined as above); c) distinguishing study participants with a mental disorder (exposed) or not (unexposed) who develop (cases) or not (controls) at least one clinical outcome of a physical disease.
Primary study‐level exclusion criteria were: a) studies investigating psychiatric symptoms only but not mental disorders; b) studies reporting on clinical outcomes only for mixed categories of mental or physical diseases (e.g., anxiety and depressive disorders, or diabetes and stroke), without distinguishable estimates per pair of disorders; c) studies using unclear diagnostic criteria not operationalized as above (e.g., continuous psychometric scales without established cut‐offs to estimate categorical diagnoses); d) studies reporting on outcomes other than those of interest.
Risk of bias
Four independent investigators assessed the risk of bias in the included systematic reviews by using the Risk of Bias in Systematic Reviews (ROBIS) tool 43 , which has shown good reliability and construct validity in systematic reviews 44 . Any discrepancy was solved through discussions with a fifth investigator.
The ROBIS tool is applied in three phases: 1) assess relevance (optional), 2) identify concerns with the review process, and 3) judge risk of bias in the review 43 . In this study, we employed phases 2 and 3. Phase 2 is divided into four domains. Domain 1 assesses concerns regarding the specification of study eligibility criteria; domain 2 evaluates any concerns regarding methods used to identify/select studies; domain 3 covers concerns regarding methods used to collect data and appraise studies; and domain 4 focuses on concerns regarding the synthesis of results. Phase 3 assesses the overall ROBIS risk of bias in the interpretation of review findings43, 45.
Data extraction
Data extraction was performed independently by three investigators and verified by a fourth investigator.
For each eligible systematic review, we extracted the standard identifier (PubMed identifier, PMID, or digital object identifier, DOI), the first author, the year and journal of publication, the number of prospective primary studies, and the specific populations evaluated. We also extracted the study‐specific association measures (odds ratio, OR; risk ratio, RR; hazard ratio, HR; and standardized mortality ratio, SMR), with their 95% confidence intervals (CIs), or the indirect information needed to estimate the association measure.
For each primary study, we extracted the specific population, the number of cases (number of outcome events in participants with a mental disorder), the number of non‐cases (number of outcome events in participants without mental disorders), the sample size, the method used to diagnose physical diseases, and the confounders to be tested in subgroup analyses – i.e., the method used to diagnose mental disorders, the timing of mental disorder diagnosis (before or after the diagnosis of a physical disorder), the type of estimates (fully/partially adjusted or unadjusted), the age and sex of participants, and the exposure to psychiatric medications.
For primary studies, we extracted in decreasing order of preference the fully adjusted estimates (e.g., controlling for all available covariates), the partially adjusted estimates (e.g., controlling only for age and sex or some of the covariates reported in the study) and the unadjusted estimates. Whenever studies used multiple control groups, we only considered data from participants without a mental disorder (non‐exposed).
We also recorded the quality score of the primary studies and the scale used (when reported) to assess quality; otherwise, we rated the study with the Newcastle‐Ottawa scale (NOS) 46 .
Statistical analysis
The main effect size of interest was the prospective association between mental disorders and clinical outcomes of physical diseases, indexed by the meta‐analytic OR, RR, HR or SMR measures and eventually converted into equivalent odds ratios (eORs) 33 for comparative purposes. The direction of the effect sizes was harmonized 47 : an eOR greater than 1 indexed an increased likelihood of the outcome, while an eOR less than 1 indexed a decreased likelihood of the outcome.
Whenever studies provided effect sizes for independent subgroups (e.g., they presented effect sizes for males and females separately), we pooled them using the Borenstein method 48 . When multiple outcomes (e.g., all‐cause mortality and cardiovascular mortality) were assessed in the same primary study, we estimated a pooled effect size 10 , assuming a correlation of 0.8 between outcomes49, 50.
Random effects models with the restricted maximum likelihood (REML) variance estimator were employed 50 . The I2 statistic was computed to evaluate inconsistency (I2>50% indicated high inconsistency) 51 , together with the 95% prediction intervals to estimate the plausible range in which the effect sizes of future studies are expected to fall 52 . The presence of small‐study effects was tested with Egger's regression asymmetry test (p≤0.05 53 ).
The presence of excess significance bias was calculated by using the new Test for Excess Statistical Significance (TESS) and the Proportion of Statistical Significance Test (PSST) 54 . Both TESS and PSST have desirable statistical properties: adequate control of Type I errors and high statistical power, which takes inconsistency into account 54 . The presence of excess significance bias was assumed if either TESS or PSST was greater than the Z‐score of 1.645 54 .
Associations were classified into five levels of evidence according to established classification criteria9, 33, 34, 35, 55: convincing (class I: N>1,000 cases, p<10−6, no evidence of small‐study effects or excess significance bias, 95% prediction interval not including the null, and no large inconsistency); highly suggestive (class II: N>1,000 cases, p<10−6, largest study with a statistically significant effect, and class I criteria not met); suggestive (class III: N>1,000 cases, p<10−3, and class I and II criteria not met); weak (class IV: all other associations with p≤0.05); and non‐significant (NS: all associations with p>0.05).
A sensitivity analysis was performed by removing the criterion of N>1,000 cases to examine the robustness of the main analysis when smaller numbers of cases were included 56 . Subgroup analyses were also performed for associations supported by class I/II evidence to test confounders identified at the primary study level. We stratified the analyses by: a) diagnostic method (standard diagnostic criteria vs. research criteria vs. validated assessment instruments with cut‐offs that map onto discrete categories); b) timing of mental diagnosis (diagnosis of mental disorder confirmed before or after the diagnosis of physical disease); c) follow‐up duration (>5 vs. ≤5 years); d) type of estimates (adjusted vs. unadjusted); e) age of participants (<50 vs. ≥50 years old); f) exposure to psychiatric medications (yes/no); and g) sex (majority of males vs. majority of females).
The PAF analysis was conducted for each class I‐III association, following a method previously established 57 . Prevalence data (± 95% CIs) of mental disorders in physical diseases were extracted from the primary studies as the total number of those exposed and those in the total population of interest (e.g., the population of patients with cardiovascular diseases). The calculation of the PAF was based on Levin's formula 58 , which requires the RR estimate and the prevalence of the risk factor 59 . We converted all ORs to RRs using a standard formula 60 . 95% CIs for the PAFs were derived using a method previously validated 40 . For each association, we created 50,000 random RRs according to the RR 95% CI and 50,000 random prevalences according to the prevalence 95% CI. We then combined the random RRs and prevalences to derive 50,000 PAF estimations, from which we derived the PAF 95% CI.
While the PAF assumes a perfect intervention that fully eradicates the risk factor (i.e., 100% reduction of its prevalence) 61 , such a complete removal is usually unrealistic. We thus performed additional analyses by computing the GIF for factors with the largest PAFs (since the GIF is ≤PAF, the GIF analysis would be futile for smaller PAFs). The GIF estimates the proportional reduction in disease incidence given a graded reduction in the prevalence of a risk factor 61 .
All analyses were performed in R software, version 4.1.2, using a new evidence synthesis package developed to conduct umbrella reviews: the metaumbrella package50, 62, also available as a browser‐based graphical app (https://metaumbrella.org).
RESULTS
Database search results
The search identified 21,612 potentially relevant records, and 18,610 titles/abstracts were screened after duplicate removal (see Figure 1). Altogether, 551 full‐text papers were checked for eligibility, and 47 systematic reviews with meta‐analysis were eventually included in the umbrella review13, 19, 20, 22, 23, 24, 26, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102.
Figure 1.

PRISMA flow chart, JBI ‐ Joanna Briggs Institute
The systematic reviews were published between 2004 and 2022, including a total of 251 non‐overlapping primary (prospective) studies. They reported on 43 primary outcomes (disease‐specific mortality: n=17; all‐cause mortality: n=26) and 31 secondary outcomes (disease‐specific incidence: n=6; disease‐specific functioning and/or disability: n=1; disease‐specific symptom severity: n=7; disease‐specific recurrence or progression: n=8; major cardiac events: n=7; and treatment‐related outcomes: n=2). No disease‐specific quality of life outcome was reported.
The total number of participants included in each systematic review ranged from 159 75 to 11,309,529 13 (median: 3,717, interquartile range, IQR: 1,154‐22,786). The participants’ age ranged from 1772, 85 to 99 years 97 , and all but one systematic review 20 included both males and females. The number of primary (prospective) studies included in each systematic review ranged from 273, 75, 78, 95, 99 to 27 76 (median: 5, IQR: 3‐8); their follow‐up duration ranged from three 79 to 29 years 86 . About 79% of the primary studies in each systematic review were of high quality.
Most (n=38, 81%) systematic reviews examined associations between mood or anxiety disorders and clinical outcomes of physical diseases: 30 (63.8%) studied the associations of mood disorders19, 24, 63, 64, 65, 67, 68, 71, 72, 73, 74, 81, 82, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 96, 97, 98, 99, 100, 102, and five (10.8%) the associations of anxiety disorders22, 66, 70, 77, 95, mostly with outcomes of cardiovascular, neoplastic, endocrine, infectious, neurological or respiratory diseases. Three studies (6.4%) investigated the associations of both anxiety and mood disorders with outcomes of neoplastic, neurological and respiratory diseases20, 23, 78.
The other diagnostic blocks were less investigated. Four systematic reviews (8.5%) studied organic, including symptomatic, mental disorders in relation to outcomes of cardiovascular, infectious or neurological diseases26, 69, 76, 79. Two (4.2%) studied schizophrenia with regard to outcomes of neoplastic diseases83, 101; one (2.1%) studied both mood disorders and schizophrenia in relation to outcomes of cardiovascular diseases 13 ; one (2.1%) studied alcohol use disorders in regard to outcomes of liver diseases 75 ; and one (2.1%) separately studied anxiety disorders, depressive disorders and Alzheimer's disease in relation to outcomes of a neurological disease 75 .
More than half (n=30, 63.8%) of the systematic reviews ascertained mental disorders using a combination of standard diagnostic criteria or requirements (DSM/ICD), research criteria and validated assessment measures with established cut‐offs that map onto ICD/DSM diagnoses. Eleven (23.5%) ascertained mental disorders using exclusively the third of the above‐mentioned approaches20, 22, 63, 74, 75, 87, 89, 93, 95, 96, 102. Only six (12.7%) used standard diagnostic criteria or requirements (any version of DSM or ICD) exclusively26, 76, 80, 83, 99, 101 (for details, see supplementary information).
There were no systematic reviews with meta‐analysis examining the impact of mental disorders from the other ICD‐10 diagnostic blocks on clinical outcomes of physical diseases.
Risk of bias
An overall summary of the ROBIS assessment of the systematic reviews is provided in the supplementary information. A total of 26 (55.3%) reviews were at low risk of bias across all phase 2 domains. In Phase 2, 35 (74.5%) systematic reviews had a low risk of bias in domain 1, 34 (72.3%) in domain 2, 26 (55.3%) in domain 3, and 31 (66%) in domain 4. A total of 32 (68.1%) systematic reviews were rated as at low risk of bias in phase 3, which indexes the overall ROBIS risk of bias43, 45.
Summary of associations
A total of 74 associations were analyzed. Fifty‐three (71.6%) presented a statistically significant effect (p<0.05), but only 15 of those (28.3%) reached p<10−6. The number of cases was greater than 1,000 for 30 associations (40.5%). Twenty‐eight associations (37.8%) presented large inconsistency (I2>50%), while for 12 (16.2%) the 95% prediction interval did not include the null hypothesis. Additionally, the evidence for small‐study effects was noted for nine associations (12.1%), and excess significance bias was noted for 19 (25.6%) associations.
The summary of the associations for classes I‐IV is shown in Figures 2 and 3. Only two associations (2.7%) showed a convincing level of evidence (class I), and six (8.1%) showed highly suggestive evidence (class II). Of the remaining associations, three (4.1%) showed suggestive evidence (class III), 42 (56.7%) weak evidence (class IV), and 21 (28.4%) had no evidence. In the following sections, we primarily describe the associations with the highest classes (I‐III) of evidence.
Figure 2.
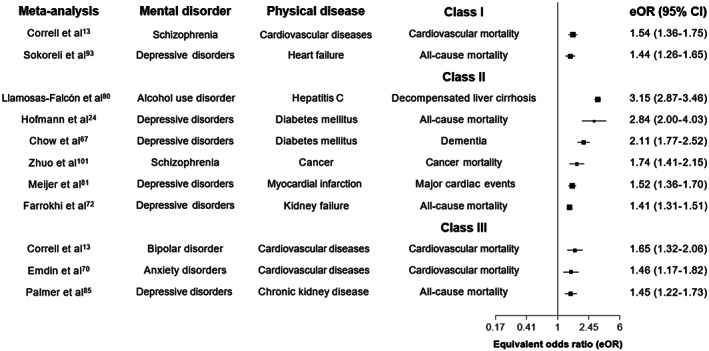
Forest plot of prospective associations between mental disorders and clinical outcomes of physical diseases, stratified by class I, II and III of evidence
Figure 3.
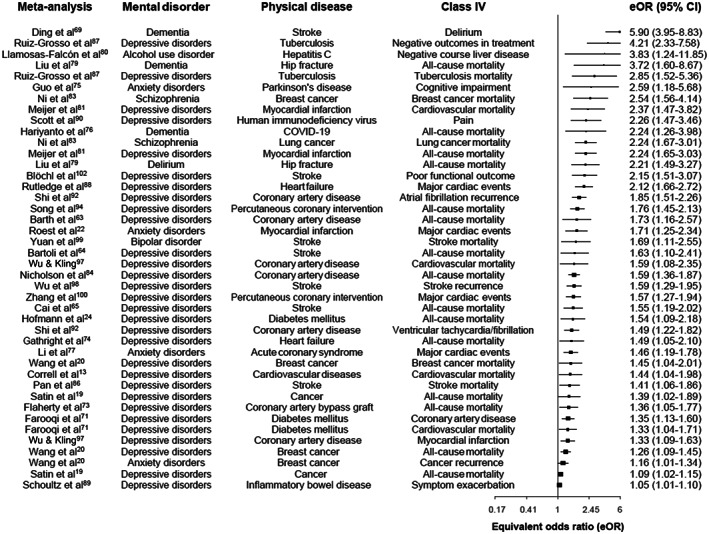
Forest plot of prospective associations between mental disorders and clinical outcomes of physical diseases, stratified by class IV of evidence
Associations of neurotic, stress‐related and somatoform disorders with clinical outcomes of physical diseases
None of the 13 associations in this diagnostic block was supported by convincing or highly suggestive evidence (class I and II) for either primary or secondary outcomes. Only the association between anxiety disorders and cardiovascular mortality in patients with cardiovascular diseases (RR=1.46, 95% CI: 1.17‐1.82) presented a suggestive evidence level (class III). There was weak evidence (class IV) for four associations concerning secondary outcomes. No evidence was found for the remaining eight associations concerning primary and secondary outcomes (see Figures 2 and 3, Table 1 and supplementary information).
Table 1.
Level of evidence for the association of neurotic, stress‐related and somatoform disorders with primary outcomes of physical diseases
| Study | Mental disorder | Physical disease | Outcome | k | Effect size (95% CI) | N cases | p random effects | I2 % | PI (95% CI) | SSE/ESB | LS | eOR | CE | CES |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Neurotic, stress‐related and somatoform disorders in patients with cardiovascular diseases | ||||||||||||||
| Emdin et al 70 | Anxiety disorders | Cardiovascular diseases | Cardiovascular mortality | 3 |
RR: 1.46 (1.17‐1.82) |
3,475 | 7.2e‐04 | 0.00 | 0.35‐6.04 | No/No | No | 1.46 | III | III |
| Celano et al 66 | Anxiety disorders | Coronary artery disease | All‐cause mortality | 8 |
OR: 1.25 (0.96‐1.64) |
904 | >0.05 | 43.85 | 0.7‐2.26 | No/Yes | No | 1.25 | NS | NS |
| Li et al 77 | Anxiety disorders | Acute coronary syndrome | All‐cause mortality | 5 |
RR: 1.03 (0.70‐1.51) |
961 | >0.05 | 44.05 | 0.35‐3.05 | No/No | No | 1.03 | NS | NS |
| Neurotic, stress‐related and somatoform disorders in patients with other physical diseases | ||||||||||||||
| Atlantis et al 23 | Anxiety disorders | Chronic obstructive pulmonary disease | All‐cause mortality | 3 |
RR: 1.11 (0.90‐1.36) |
32 | >0.05 | 0.00 | 0.29‐4.17 | No/No | No | 1.11 | NS | NS |
| Wang et al 20 | Anxiety disorders | Breast cancer | All‐cause mortality | 3 |
HR: 1.07 (0.92‐1.23) |
1,049 | >0.05 | 0.00 | 0.42‐2.69 | No/No | No | 1.07 | NS | NS |
CE – class of evidence, CES – class of evidence after sensitivity analysis (removing the N>1,000 cases criterion), CI – confidence interval, eOR – equivalent odds ratio, ESB – excess significance bias, HR – hazard ratio, LS – largest study with significant effect, NS – not significant, OR – odds ratio, RR – risk ratio, PI – prediction interval, SSE – small study effect
After removing the N>1,000 cases criterion in sensitivity analysis, the two associations between anxiety disorders and major cardiac events were upgraded from weak (class IV) to suggestive evidence (class III). The level of evidence of the other associations remained unchanged (see Table 1 and supplementary information).
Associations of mood disorders with clinical outcomes of physical diseases
Among the 49 associations in this diagnostic block, only that between depressive disorders and all‐cause mortality among patients with heart failure (HR=1.44, 95% CI: 1.26‐1.65) presented a convincing level of association (class I) (see Figure 2 and Table 2).
Table 2.
Level of evidence for the association of mood disorders with primary outcomes of physical diseases
| Study | Mental disorder | Physical disease | Outcome | k | Effect size (95% CI) | N cases | p random effects | I2% | PI (95% CI) | SSE/ESB | LS | eOR | CE | CES |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mood disorders in patients with cardiovascular diseases | ||||||||||||||
| Sokoreli et al 93 | Depressive disorders | Heart failure | All‐cause mortality | 4 |
HR: 1.44 (1.26‐1.65) |
1,377 | 1.4e‐07 | 0.00 |
1.07‐1.94 |
No/No | Yes | 1.44 | I | I |
| Gathright et al 74 | Depressive disorders | Heart failure | All‐cause mortality | 9 |
HR: 1.49 (1.05‐2.10) |
1,283 | 2.5e‐02 | 79.85 | 0.46‐4.79 | Yes/Yes | No | 1.49 | IV | IV |
| Correll et al 13 | Bipolar disorder | Cardiovascular diseases | Cardiovascular mortality | 6 |
RR: 1.65 (1.32‐2.06) |
8,923 | 9.0e‐06 | 80.43 | 0.86‐3.14 | No/No | Yes | 1.65 | III | III |
|
Meijer et al 81 |
Depressive disorders | Myocardial infarction | Cardiovascular mortality | 5 |
OR: 2.37 (1.47‐3.82) |
107 | 3.8e‐04 | 13.58 | 0.78‐7.22 | No/No | No | 2.37 | IV | III |
| Meijer et al 81 | Depressive disorders | Myocardial infarction | All‐cause mortality | 15 |
OR: 2.24 (1.65‐3.03) |
725 | 2.0e‐07 | 48.11 | 0.92‐5.44 | No/No | Yes | 2.24 | IV | II |
| Song et al 94 | Depressive disorders | Percutaneous coronary intervention | All‐cause mortality | 6 |
RR: 1.76 (1.45‐2.13) |
265 | 1.1e‐08 | 0.00 | 1.28‐2.41 | No/Yes | Yes | 1.76 | IV | II |
|
Barth et al 63 |
Depressive disorders | Coronary artery disease | All‐cause mortality | 6 |
HR: 1.73 (1.16‐2.57) |
1,097 | 7.1e‐03 | 72.4 | 0.49‐6.12 | No/Yes | Yes | 1.73 | IV | IV |
| Nicholson et al 84 | Depressive disorders | Coronary artery disease | All‐cause mortality | 10 |
RR: 1.59 (1.36‐1.87) |
412 | 1.3e‐08 | 9.42 | 1.32‐1.93 | No/Yes | Yes | 1.59 | IV | II |
|
Yuan et al 99 |
Bipolar disorder | Stroke | Stroke mortality | 2 |
HR: 1.69 (1.11‐2.55) |
1,816 | 3.2e‐02 | 96.52 | NA | NA/NA | Yes | 1.69 | IV | IV |
|
Bartoli et al 64 |
Depressive disorders |
Stroke | All‐cause mortality | 5 |
RR: 1.63 (1.10‐2.41) |
237 | 1.5e‐02 | 58.87 | 0.49‐5.39 | No/No | No | 1.63 | IV | IV |
|
Cai et al 65 |
Depressive disorders | Stroke | All‐cause mortality | 8 |
HR: 1.55 (1.19‐2.02) |
24,022 | 1.0e‐03 | 74.47 | 0.69‐3.5 | Yes/Yes | Yes | 1.55 | IV | IV |
|
Wu & Kling 97 |
Depressive disorders | Coronary artery disease | Cardiovascular mortality | 5 |
HR: 1.59 (1.08‐2.35) |
1,654 | 1.9e‐02 | 82.00 | 0.41‐6.23 | Yes/Yes | Yes | 1.59 | IV | IV |
|
Correll et al 13 |
Depressive disorders | Cardiovascular diseases | Cardiovascular mortality | 5 |
OR: 1.44 (1.04‐1.98) |
8,319 | 2.6e‐02 | 86.29 | 0.46‐4.44 | No/No | No | 1.44 | IV | IV |
|
Pan et al 86 |
Depressive disorders | Stroke | Stroke mortality | 4 |
HR: 1.41 (1.06‐1.86) |
5,007 | 1.7e‐02 | 36.91 | 0.76‐2.59 | No/No | No | 1.41 | IV | IV |
| Flaherty et al 73 | Depressive disorders | Coronary artery bypass graft | All‐cause mortality | 2 |
HR: 1.36 (1.05‐1.77) |
239 | 2.1e‐02 | 0.00 | NA | NA/NA | Yes | 1.36 | IV | IV |
| Mood disorders in patients with chronic respiratory diseases | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atlantis et al 23 | Depressive disorders | Chronic obstructive pulmonary disease | All‐cause mortality | 6 | RR: 2.04 (0.87‐4.77) | 215 | >0.05 | 73.8 | 0.12‐34.24 | No/Yes | Yes | 2.04 | NS | NS |
| Courtwright et al 68 | Depressive disorders | Lung transplant | Posttransplant mortality | 2 | HR: 1.01 (0.99‐1.04) | 218 | >0.05 | 0.00 | NA | NA/NA | No | 1.01 | NS | NS |
| Study | Mental disorder | Physical disease | Outcome | k | Effect size (95% CI) | N cases | p random effects | I2% | PI (95% CI) | SSE/ESB | LS | eOR | CE | CES |
| Mood disorders in patients with endocrine system diseases | ||||||||||||||
| Farrokhi et al 72 | Depressive disorders | Kidney failure | All‐cause mortality | 6 |
HR: 1.41 (1.31‐1.51) |
1,834 | 1.0e‐22 | 12.85 | 1.28‐1.55 | Yes/Yes | Yes | 1.41 | II | II |
| Hofmann et al 24 |
Depressive disorders |
Diabetes mellitus |
All‐cause mortality |
7 |
HR: 2.84 (2.00‐4.03) |
2,108 | 4.7e‐09 | 88.81 | 0.88‐9.15 | No/No | Yes | 1.93 | II | II |
| Hofmann et al 24 | Depressive disorders | Diabetes mellitus | All‐cause mortality | 6 |
HR: 1.54 (1.09‐2.18) |
3,725 | 1.4e‐02 | 85.18 | 0.48‐4.99 | No/Yes | No | 1.54 | IV | IV |
| Palmer et al 85 | Depressive disorders | Chronic kidney disease | All‐cause mortality | 13 |
HR: 1.45 (1.22‐1.73) |
2,066 | 2.0e‐05 | 40.69 | 0.95‐2.22 | Yes/Yes | Yes | 1.45 | III | III |
| Farooqi et al 71 | Depressive disorders |
Diabetes mellitus |
Cardiovascular mortality | 3 |
HR: 1.33 (1.04‐1.71) |
468 | 2.3e‐02 | 14.51 | 0.27‐6.66 | No/No | No | 1.33 | IV | IV |
| van Dooren et al 96 | Depressive disorders | Diabetes mellitus | Cardiovascular mortality | 2 |
HR: 1.60 (0.69‐3.72) |
169 | >0.05 | 77.41 | NA | NA/NA | No | 1.60 | NS | NS |
| Mood disorders in patients with cancer | ||||||||||||||
|
Satin et al 19 |
Depressive disorders |
Cancer |
All‐cause mortality |
3 |
RR: 1.39 (1.02‐1.89) |
55 | 3.5e‐02 | 0.00 | 0.19‐10.08 | No/No | No | 1.39 | IV | IV |
|
Satin et al 19 |
Depressive disorders | Cancer | All‐cause mortality | 8 |
HR: 1.09 (1.02‐1.15) |
1,490 | 5.2e‐03 | 60.07 | 0.95‐1.24 | Yes/No | No | 1.09 | IV | IV |
| Wang et al 20 | Depressive disorders | Breast cancer | Breast cancer mortality | 2 |
HR: 1.45 (1.04‐2.01) |
313 | 2.7e‐02 | 0.00 | NA | NA/NA | No | 1.45 | IV | IV |
| Wang et al 20 | Depressive disorders | Breast cancer | All‐cause mortality | 6 |
HR: 1.26 (1.09‐1.45) |
2,021 | 1.3e‐03 | 0.00 | 1.03‐1.53 | No/No | No | 1.26 | IV | IV |
|
Shi et al 91 |
Depressive disorders | High‐grade brain tumor | All‐cause mortality | 3 |
HR: 1.31 (0.86‐1.99) |
836 | >0.05 | 0.00 | 0.09‐19.69 | No/No | No | 1.31 | NS | NS |
| Shi et al 91 | Depressive disorders | Glioma | Glioma mortality | 5 | RR: 0.74 (0.54‐1.02) | 627 | >0.05 | 48.61 | 0.27‐2.07 | No/No | No | 0.74 | NS | NS |
| Mood disorders in patients with other physical diseases | ||||||||||||||
|
Ruiz‐Grosso et al 87 |
Depressive disorders | Tuberculosis | Tuberculosis mortality | 2 |
OR: 2.85 (1.52‐5.36) |
53 | 1.1e‐03 | 0.00 | NA | NA/NA | Yes | 2.85 | IV | IV |
CE – class of evidence, CES – class of evidence after sensitivity analysis (removing the N>1,000 cases criterion), CI – confidence interval, eOR – equivalent odds ratio, ESB – excess significance bias, HR – hazard ratio, LS – largest study with significant effect, NA – not assessable, NS – not significant, OR – odds ratio, RR – risk ratio, PI – prediction interval, SSE – small study effect
Highly suggestive evidence (class II) was found for associations between depressive disorders and all‐cause mortality in patients with kidney failure (HR=1.41, 95% CI: 1.31‐1.51) and in those with diabetes mellitus (HR=2.84, 95% CI: 2.00‐4.03); for the association between depressive disorders and major cardiac events in patients with myocardial infarction (OR=1.52, 95% CI: 1.36‐1.70); and for the association between depressive disorders and dementia in patients with diabetes mellitus (HR=2.11, 95% CI: 1.77‐2.52) (see Figure 2, Table 2 and supplementary information).
There was suggestive evidence (class III) for two associations: that between bipolar disorder and cardiovascular mortality in patients with cardiovascular diseases (RR=1.65, 95% CI: 1.32‐2.06), and that between depressive disorders and all‐cause mortality in patients with chronic kidney disease (RR=1.45, 95% CI: 1.22‐1.73). There was either weak (class IV) or no evidence of association for all other primary and secondary outcomes (see Figure 3, Table 2 and supplementary information).
After removing the N>1,000 cases criterion in sensitivity analysis, there was no change in the level of class I, II and III evidence (see Table 2).
Three associations between depressive disorders and primary outcomes were upgraded from weak (class IV) to highly suggestive evidence (class II): those with all‐cause mortality in patients with myocardial infarction, percutaneous coronary intervention, and coronary artery disease (see Table 2). The same upgrade was observed for the associations between depressive disorders and two secondary outcomes: major cardiac events in patients with heart failure, and atrial fibrillation recurrence in patients with coronary artery disease (see supplementary information).
One association between depressive disorders and a primary outcome was upgraded from weak (class IV) to suggestive evidence (class III): that with cardiovascular mortality in patients with myocardial infarction (see Table 2). The same upgrade was observed for seven associations between depressive disorders and secondary outcomes: poor functional outcome and stroke recurrence in patients with stroke; major cardiac events in patients with percutaneous coronary intervention; ventricular tachycardia/fibrillation in patients with coronary artery disease; coronary artery disease in patients with diabetes mellitus; negative treatment outcomes in patients with tuberculosis; and pain in patients with HIV infection (see supplementary information).
Associations of mental and behavioural disorders due to psychoactive substance use with clinical outcomes of physical diseases
No association in this diagnostic block was supported by convincing evidence (class I), and there were no data on primary outcomes. The association between alcohol use disorder and decompensated liver cirrhosis in patients with hepatitis C (RR=3.15, 95% CI: 2.87‐3.46) presented highly suggestive evidence (class II). After removing the N>1,000 cases criterion in sensitivity analysis, there was no change in the level of evidence (see supplementary information).
Associations of schizophrenia with clinical outcomes of physical diseases
In this diagnostic block, one association presented convincing evidence (class I): that between schizophrenia and cardiovascular mortality in patients with cardiovascular diseases (RR=1.54, 95% CI: 1.36‐1.75). One further association was supported by highly suggestive evidence (class II): that between schizophrenia and cancer mortality in patients with cancer (SMR=1.74, 95% CI: 1.41‐2.15) (see Figure 2 and Table 3). Two associations presented weak evidence (class IV): those between schizophrenia and cancer mortality in patients with breast and lung cancer (see Figure 3 and Table 3).
Table 3.
Level of evidence for the association of schizophrenia and organic, including symptomatic, mental disorders with primary outcomes of physical diseases
| Study | Mental disorder | Physical disease | Outcome | k | Effect size (95% CI) | N cases | p random effects | I2% | PI (95% CI) | SSE/ESB | LS | eOR | CE | CES |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Schizophrenia in patients with cardiovascular diseases and cancer | ||||||||||||||
| Correll et al 13 |
Schizophrenia |
Cardiovascular diseases | Cardiovascular mortality | 7 |
RR: 1.54 (1.36‐1.75) |
9,097 | 2.2e‐11 | 27.82 | 1.19‐2.00 | No/No | No | 1.54 | I | I |
| Zhuo et al 101 |
Schizophrenia |
Cancer | Cancer mortality | 3 | SMR: 1.74 (1.41‐2.15) | 6,145 | 2.9e‐07 | 66.53 | 0.17‐17.56 | No/No | Yes | 1.72 | II | II |
| Ni et al 83 |
Schizophrenia |
Breast cancer | Breast cancer mortality | 2 | RR: 2.54 (1.56‐4.14) | 175 | 1.7e‐04 | 0.00 | NA | NA/NA | Yes | 2.54 | IV | III |
| Ni et al 83 |
Schizophrenia |
Lung cancer | Lung cancer mortality | 2 |
RR: 2.24 (1.67‐3.01) |
192 | 9.0e‐08 | 0.00 | NA | NA/NA | Yes | 2.24 | IV | II |
| Organic, including symptomatic, mental disorders in patients with infectious and musculoskeletal system diseases | ||||||||||||||
| Liu et al 79 |
Dementia |
Hip fracture | All‐cause mortality | 2 |
HR: 3.72 (1.6‐8.67) |
384 | 2.3e‐03 | 72.52 | NA | NA/NA | Yes | 3.72 | IV | IV |
| Liu et al 79 |
Delirium |
Hip fracture | All‐cause mortality | 6 |
HR: 2.21 (1.49‐3.27) |
638 | 7.5e‐05 | 64.54 | 0.65‐7.51 | No/No | Yes | 2.21 | IV | III |
| Hariyanto et al 76 | Dementia | COVID‐19 | All‐cause mortality | 2 | RR: 2.24 (1.26‐3.98) | 4,417 | 5.8e‐03 | 89.51 | NA | NA/NA | Yes | 2.24 | IV | IV |
| Liu et al 26 | Dementia | COVID‐19 | All‐cause mortality | 2 |
OR: 3.27 (0.34‐31.43) |
148 | >0.05 | 47.02 | NA | NA/NA | Yes | 3.27 | NS | NS |
CE – class of evidence, CES – class of evidence after sensitivity analysis (removing the N>1,000 cases criterion), CI – confidence interval, eOR – equivalent odds ratio, ESB – excess significance bias, HR – hazard ratio, LS – largest study with significant effect, NA – not assessable, NS – not significant, OR – odds ratio, RR – risk ratio, PI – prediction interval, SMR – standardized mortality ratio, SSE – small study effect
After removing the N>1,000 cases criterion in sensitivity analysis, the association between schizophrenia and cancer mortality was upgraded from weak (class IV) to highly suggestive (class II) in patients with lung cancer, and from weak (class IV) to suggestive (class III) in patients with breast cancer. The level of evidence of the other two associations remained unchanged (see Table 3).
Associations of organic, including symptomatic, mental disorders with clinical outcomes of physical diseases
No association in this diagnostic block was supported by convincing, highly suggestive, or suggestive evidence (classes I, II and III). There was weak evidence (class IV) of the association between both dementia and delirium with all‐cause mortality in patients with hip fracture; of the association between dementia and all‐cause mortality in patients with COVID‐19 infection; and of the association between dementia and delirium in patients with stroke (see Table 3 and supplementary information).
After removing the N>1,000 cases criterion in sensitivity analysis, the association between dementia and delirium in patients with stroke was upgraded from weak (class IV) to convincing evidence (class I), while the association between delirium and all‐cause mortality in patients with hip fracture was upgraded from weak (class IV) to suggestive (class III) evidence (see Table 3 and supplementary information).
Subgroup analyses
Not all planned subgroup analyses were possible, due to the lack of data (see supplementary information).
When restricting the analyses to standard diagnostic criteria (any version of DSM or ICD), the class II association between depressive disorders and all‐cause mortality in patients with diabetes mellitus was downgraded to weak (class IV) evidence. When restricting the analyses to studies formulating a diagnosis of mental disorder before the diagnosis of physical disease (of course, clinical outcomes always followed the diagnosis of a mental disorder), the level of evidence of class I and II associations remained unchanged.
When restricting the analyses to follow‐up duration >5 years, the class I association between schizophrenia and cardiovascular mortality in patients with cardiovascular diseases, and the class II associations between depressive disorders and all‐cause mortality in patients with kidney failure and diabetes mellitus were downgraded to suggestive or weak evidence (class III and IV). When restricting the analyses to adjusted estimates, only the class I association between schizophrenia and cardiovascular mortality in patients with cardiovascular diseases was downgraded to weak (class IV) evidence.
When restricting the analyses to age of participants <50 years, the class I association between schizophrenia and cardiovascular mortality in cardiovascular diseases was downgraded to weak (class IV) evidence. When restricting the analyses to samples exposed to psychiatric treatments, all class I and II associations were downgraded to either suggestive (class III) or weak (class IV) evidence.
When restricting the analyses to studies including in their samples a majority of males, the class I association between schizophrenia and cardiovascular mortality in patients with cardiovascular diseases, and between depressive disorders and all‐cause mortality in patients with heart failure, were downgraded to highly suggestive (class II) or weak (class IV) evidence. The class II associations between depressive disorders and all‐cause mortality in patients with kidney failure and diabetes mellitus were downgraded to suggestive or weak evidence (class III or IV).
It is important to note that all the subgroup analyses were conducted in a very small number of primary studies (see supplementary information) and are, therefore, highly underpowered.
Population attributable fraction (PAF) and generalized impact fraction (GIF)
The largest PAF was that for the association of alcohol use disorder with decompensated liver cirrhosis in patients with hepatitis C (30.56%, 95% CI: 27.67‐33.49) (see Table 4). GIF analysis showed that alcohol use disorder should be reduced by 33% to prevent 10% of decompensated liver cirrhosis in hepatitis C (see also supplementary information).
Table 4.
Meta‐analytical population attributable fraction (PAF) for the associations supported by the largest evidence (classes I, II and III)
| Mental disorder | Physical disease | Outcome | Risk ratio (95% CI) | Prevalence of mental disorder in physical disease (95% CI) | PAF (95% CI) |
|---|---|---|---|---|---|
| Depressive disorders | Heart failure | All‐cause mortality |
1.44 (1.26‐1.65) |
17.72% (16.89‐18.56) |
7.25% (4.38‐10.34) |
| Schizophrenia | Cardiovascular diseases | Cardiovascular mortality |
1.54 (1.36‐1.75) |
25.17% (25.08‐25.30) |
11.99% (8.29‐15.84) |
| Depressive disorders | Diabetes mellitus | Dementia |
2.11 (1.77‐2.52) |
6.66% (6.60‐6.71) |
6.89% (4.87‐9.19) |
| Depressive disorders | Kidney failure | All‐cause mortality |
1.41 (1.31‐1.51) |
32.11% (31.30‐32.93) |
11.59% (9.09‐14.14) |
| Depressive disorders | Diabetes mellitus | All‐cause mortality |
2.84 (2.00‐4.03) |
19.91% (19.07‐20.79) |
26.81% (16.61‐37.67) |
| Alcohol use disorder | Hepatitis C | Decompensated liver cirrhosis |
3.15 (2.87‐3.46) |
20.50% (20.30‐20.70) |
30.56% (27.67‐33.49) |
| Depressive disorders | Myocardial infarction | Major cardiac events |
1.52 (1.36‐1.70) |
30.58% (29.62‐31.56) |
13.68% (9.87‐17.58) |
| Schizophrenia | Cancer | Cancer mortality |
1.74 (1.41‐2.14) |
11.05% (10.75‐11.36) |
7.53% (4.31‐11.21) |
| Bipolar disorder | Cardiovascular diseases | Cardiovascular mortality |
1.65 (1.32‐2.06) |
3.41% (3.81‐4.10) |
2.17% (1.16‐3.76) |
| Anxiety disorders | Cardiovascular diseases | Cardiovascular mortality |
1.46 (1.17‐1.82) |
5.50% (5.41‐5.64) |
2.47% (0.93‐4.33) |
| Depressive disorders | Chronic kidney disease | All‐cause mortality |
1.45 (1.22‐1.73) |
10.50% (10.01‐10.96) |
4.53% (2.24‐7.12) |
The PAFs for the association of depressive disorders with all‐cause mortality in patients with diabetes mellitus and kidney failure were respectively 26.81% (95% CI: 16.61‐37.67) and 11.59% (95% CI: 9.09‐14.14). The PAF for the association of depressive disorders with cardiac events in patients with myocardial infarction was 13.68% (95% CI: 9.87‐17.58) (see Table 4). GIF analyses showed that depressive disorders should be reduced by 37% and by 86% to prevent 10% of all‐cause mortality in patients with diabetes mellitus and kidney failure, respectively, and be reduced by 73% to prevent 10% of major cardiac events in patients with myocardial infarction (see Figure 4 and supplementary information).
Figure 4.
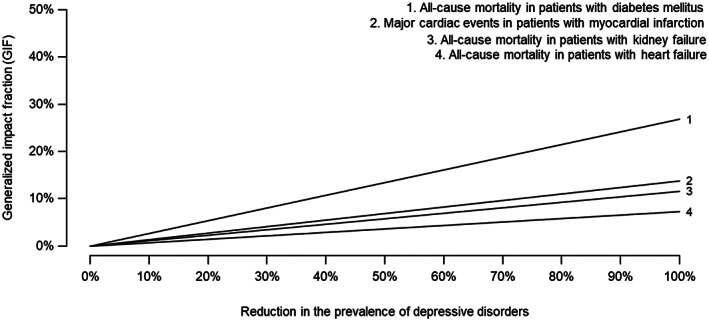
Meta‐analytic generalized impact fraction (GIF) of depressive disorders for all‐cause mortality and major cardiac events in several physical diseases
The PAF of the association of schizophrenia with cardiovascular mortality in patients with cardiovascular diseases was 11.99% (95% CI: 8.29‐15.84) (see Table 4). GIF analysis showed that schizophrenia prevalence should be reduced by 83% to prevent 10% of cardiovascular mortality in patients with cardiovascular diseases (see supplementary information).
The PAFs for other class I‐III associations are reported in Table 4. They were 7.53% (95% CI: 4.31‐11.21) for the association between schizophrenia and cancer mortality in patients with cancer; 7.25% (95% CI: 4.38‐10.34) for the association between depressive disorders and all‐cause mortality in patients with heart failure; 4.53% (95% CI: 2.24‐7.12) for the association between depressive disorders and all‐cause mortality in patients with chronic kidney disease; 2.47% (95% CI: 0.93‐4.33) for the association between anxiety disorders and cardiovascular mortality in patients with cardiovascular diseases; and 2.17% (95% CI: 1.16‐3.76) for the association between bipolar disorder and cardiovascular mortality in patients with cardiovascular diseases.
DISCUSSION
In this umbrella review, we evaluated 47 systematic reviews with meta‐analysis, including 251 non‐overlapping primary studies, testing 74 prospective associations between mental disorders and 43 primary and 31 secondary clinical outcomes of physical diseases. This is the first attempt to comprehensively evaluate the impact of the entire spectrum of mental disorders on the clinical outcomes of physical diseases, using established grading criteria that control for several biases. This is also the first study to employ metaumbrella, a comprehensive suite of statistical packages developed for conducting umbrella reviews 50 , 62 . We also estimated for the first time the meta‐umbrella preventive capacity (meta‐analytic PAFs) of the associations supported by class I‐III evidence to establish reliable, evidence‐based and actionable targets that can be prioritized in clinical practice.
An additional strength of this work is the in‐depth screening of primary studies included in each systematic review to selectively include only data reflecting prospective associations. This choice mitigates the reverse causality bias and ensures the temporality of the examined associations, where exposures (mental disorders) always preceded the event investigated (clinical outcomes of physical diseases). Furthermore, we also screened primary studies to include only those using robust diagnostic or research criteria, or validated instruments with specific cut‐offs mapped to discrete categories of mental disorders. This approach overcomes the significant noise derived from studies that mistake continuous symptoms or self‐reported subjective “experiences” for categorical mental disorders, which characterizes the existing transdiagnostic literature 103 , 104 . Our refined evidence synthesis method resulted in more than two‐thirds (68%) of the included systematic reviews having a low risk of bias and nearly 80% of the selected primary studies scoring high on quality assessments.
Mood disorders (especially depressive disorders) emerged as credible risk factors for adverse clinical outcomes in cardiovascular diseases, as most associations in this class were supported by the largest evidence (classes I, II or III). The most robust association (class I) was that between depressive disorders and all‐cause mortality among patients with heart failure, which remained at the same level of evidence after conducting subgroup analyses accounting for confounders. Other highly suggestive/suggestive associations were those between depressive disorders and the risk of major cardiac events in patients with myocardial infarction (class II), and between bipolar disorder and the risk of cardiovascular mortality in patients with cardiovascular disease (class III).
Overall, the association between depressive disorders and cardiovascular diseases is a consolidated area of research across psychiatry and somatic medicine 7 , 105 , 106 , 107 , 108 , although the underlying mechanisms are not fully understood 107 . The pathophysiology of these conditions may share common mechanisms, including behavioral, biological and medication‐related ones 108 , 109 , 110 , 111 , 112 , forming an interdependent network 113 .
Behavioral mechanisms may include unhealthy habits (smoking, excessive alcohol consumption, physical inactivity, unhealthy diet, medication non‐adherence) that accelerate pathophysiological processes, such as atherosclerosis, leading to poor health outcomes and increased mortality 109 , 110 , 112 , 113 , 114 .
Biological mechanisms may include alterations in the autonomic nervous system, plasminogen activator inhibitor‐1 and fibrinogen levels, endothelial function, and neurohormonal factors, as well as diminished heart rate variability, and genetic alterations of the serotonin transporter 109 , 110 , 112 , 113 , 114 . Molecular inflammatory mechanisms involving interleukins (IL‐6 and IL‐1β) and C‐reactive protein, as well as an oxidative stress imbalance, may also point to common pathways between mood and cardiovascular condictions 109 , 115 , 116 , 117 , 118 .
Mechanisms associated with treatment (for example, antidepressants use) may include cardiotoxicity 109 , 110 , 113 , 114 , or the alteration of platelet activation 111 leading to an increased incidence of major cardiac events and sudden death 109 , 110 , 111 , 113 , 114 . However, the latter is unlikely a strong mechanism, especially when using selective serotonin reuptake inhibitors, which reduce platelet aggregation 119 , 120 .
We also found highly suggestive (class II) evidence that depressive disorders increase all‐cause mortality risk in patients with diabetes mellitus and kidney failure. The increased mortality in diabetes mellitus is due to insulin resistance and metabolic factors (e.g., abdominal obesity and dyslipidemia). These factors are aggravated by depressive disorders, which are independently associated with insulin resistance 121 and metabolic syndrome (elevated adipose tissue and dyslipidemia 122 , 123 ). The increased mortality in depressed patients with kidney failure may be due to suboptimal compliance with complex medication regimens 123 , 124 , 125 .
Highly suggestive (class II) evidence was similarly found for the association between depressive disorders and an increased risk of dementia in patients with diabetes mellitus 67 . Both depressive disorders and diabetes mellitus have been shown to increase the incidence of dementia individually and synergistically 126 , with the metabolic‐brain axis as a key mediator connecting these conditions 126 . Depressive disorders are associated with micro/macro vascular alterations 127 , 128 , insulin resistance 121 and neuroinflammation 129 ; these factors may increase the risk of dementia in this patient population 130 , 131 . Stress and psychosocial determinants of health may also be key mediators in how these systems interact 126 .
These are clinically highly relevant findings, as depression prevention and/or treatment has great potential to improve overall health and outcomes in common physical diseases that are associated with severe biopsychosocial and societal burden (e.g., dementia is a rising problem in ageing societies 132 ) and premature mortality. Our PAF analysis directly informs the prioritization of these approaches and associated resources on the basis of evidence‐based potential preventive gains. For example, this study provides the first robust meta‐umbrella evidence showing that preventing depressive disorders could reduce up to one‐third of mortality rates across various physical conditions.
Screening for depression in patients with cardiovascular diseases is recommended by the US Preventive Services Task Force and the American Heart Association 133 , 134 . Furthermore, independent meta‐analyses showed that psychotherapy/psychoeducation can have a preventive effect by reducing the severity of symptoms before the onset of depressive disorders 135 , 136 , 137 . Randomized controlled trials demonstrated that collaborative care, which includes patient preferences, cognitive intervention and/or lifestyle advice, drug treatment management, and relapse prevention 138 , or physical exercise 139 , 140 , can specifically reduce depression in patients with cardiovascular diseases or diabetes, including low‐ and middle‐income countries 141 , 142 . These interventions could, at the same time, have an impact on depressive disorders and improve self‐management of physical diseases in patients with mental and physical multimorbidity 143 . Our GIF analysis confirms these benefits; the reduction of mortality rates remains clinically relevant even if preventive interventions are only partially effective. Taken together, these findings call for a new generation of translational research validating preventive approaches for depressive disorders in physical conditions.
The association between schizophrenia and increased cardiovascular and cancer mortality in patients with these physical diseases was also supported by convincing or highly suggestive evidence (class I and II, respectively). The higher mortality risk in schizophrenia compared to the general population is substantial and particularly marked during the early stages of the disorder 144 . The increased risk of cardiovascular and cancer mortality may be due to suboptimal cardiovascular 145 , 146 and cancer screening 147 in patients with schizophrenia, coupled with high cigarette smoking 145 , frequent metabolic syndrome (obesity, hypertension, diabetes, hyperlipidemia) 148 , 149 , 150 , 151 , 152 , physical inactivity, drug and alcohol use, and poor adherence to medication 153 , 154 , 155 .
Although antipsychotics can lead to adverse cardiometabolic effects that are a risk factor for cardiovascular mortality 156 , a recent meta‐analysis showed that all‐cause mortality risk at the population level is substantially reduced with antipsychotic use versus no antipsychotic use (RR=0.71) 144 . The reason for this paradoxical relationship can be found in a nationwide database within‐subject analysis, where ongoing antipsychotic treatment was associated with higher adherence to statins, antihypertensive and antidiabetic medications 157 . Thus, greater psychiatric stability via antipsychotic treatment improves not only healthy lifestyle behaviors but also adherence to medications for secondary physical illness prevention 144 .
Furthermore, our PAF analysis suggests that preventing psychosis in young people at clinical high risk can produce physical health benefits in terms of reduced cardiovascular and cancer mortality, in addition to improved mental health outcomes 158 , 159 , 160 , 161 , 162 , 163 , 164 , 165 (indicated prevention).
Highly suggestive evidence (class II) was also found for the association of alcohol use disorder with decompensated liver cirrhosis in patients infected with hepatitis C virus. Indeed, alcohol use disorder leads to alterations in cytokine production, lipopolysaccharide‐TLR4 signalling, and reactive oxygen species 166 , factors that increase hepatotoxicity 167 , 168 . Patients with alcohol use disorder are also frequently medically ineligible for hepatitis C treatment 169 .
Our PAF analysis demonstrates that about one‐third of decompensated liver cirrhosis in patients with hepatitis C could be averted by preventing alcohol use disorder (the largest PAF in our study). Thus, alcohol use disorder should be identified and managed as much as possible to improve psychiatric as well as physical health outcomes. Screening for unhealthy alcohol use in primary care settings in adults, including pregnant women, and providing brief behavioral counselling interventions is an evidence‐based approach to reducing unhealthy alcohol use, as recommended by the US Preventive Services Task Force 170 .
There are some limitations to this study. First, while we avoided the limitations of retrospective or case‐control study designs by selecting only prospective systematic reviews with meta‐analysis and prospective primary studies, the observed associations do not represent pathophysiological causality. For example, although we preferably focused on adjusted estimates, we could not specifically address the role of single confounders, such as genetic effects, body mass index or metabolic risk factors, which may at least partially account for the observed associations. Second, there were few relevant systematic reviews with meta‐analysis in child and adolescent populations, and for mental disorders other than depressive disorders. For example, we did not find any relevant meta‐analysis that considered patients with anorexia nervosa or personality disorders. Third, the results of the subgroup analyses should be viewed with caution, due to the granularity of the reported data and the very limited statistical power. Finally, our PAF findings are specific to the populations affected with physical diseases and cannot be applied to the general population.
Acknowledging these caveats, our study has several implications. We demonstrated at a meta‐umbrella review level that mental disorders significantly impair the health and life expectancy of individuals with physical diseases, and quantified for the first time the associated preventive capacity. Our findings may be particularly relevant for informing the prioritization of preventive approaches for physical diseases via improved detection and management of mental disorders, with currently the best evidence and actionable targets for alcohol use disorders, depression and schizophrenia.
These approaches are likely to be particularly relevant for young people, given the early age at onset of most mental disorders 40 , 171 . Prevention for youth is currently driven by initiatives siloed in physical diseases, such as cancer and obesity 143 , 165 . However, preventing the onset of mental disorders can become a tantalizing strategy for reducing at the same time the risk of developing physical diseases 143 . Indeed, the cost and risk associated with preventive approaches (e.g., ethical concerns 172 ) can be offset by concurrently reducing the burden of both psychiatric disorders and physical diseases 165 , 173 . Integrating early detection and prevention of mental health and physical conditions may be particularly cost‐effective in resource‐constrained settings 142 .
This strategy would require innovative integrated or, at least, co‐located clinical services for emerging mental and physical conditions, overcoming the limited preventive capacity of current health care services 165 . Indeed, youth‐friendly mental and physical health care services are being developed and tested worldwide 174 , 175 , 176 , 177 , and promise to achieve the much‐needed cross‐disciplinary fertilization of expertise which is essential to reduce the Cartesian dichotomy between mental and physical knowledge, education and research.
In conclusion, this umbrella review demonstrates that mental disorders increase the risk of several poor clinical outcomes in patients with physical diseases. Prevention targeting mental disorders – particularly alcohol use disorders, depressive disorders, and schizophrenia – can reduce the incidence of adverse clinical outcomes in physical diseases. These findings can inform clinical practice and trans‐speciality preventive approaches cutting across psychiatric and somatic medicine.
ACKNOWLEDGEMENTS
G. Arrondo is supported by the European Social Fund and the Spanish Research Agency (RYC2020‐030744‐I/AEI/10.13039/501100011033). M. Berk is supported by National Health and Medical Research Council (NHMRC) Senior Principal Research Fellowship and Leadership 3 Investigator grants (1156072 and 2017131). Supplementary information on this study is available at https://github.com/eldragio/DRAGIOTI_UR_2022/raw/main/Supplementary%20information.pdf.
REFERENCES
- 1. GBD 2019 Diseases and Injuries Collaborators . Global burden of 369 diseases and injuries in 204 countries and territories, 1990‐2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1204‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. GBD 2019 Mental Disorders Collaborators . Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990‐2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022;9:137‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Cortese S, Sun S, Zhang J et al. Association between attention deficit hyperactivity disorder and asthma: a systematic review and meta‐analysis and a Swedish population‐based study. Lancet Psychiatry 2018;5:717‐26. [DOI] [PubMed] [Google Scholar]
- 4. Lim LF, Solmi M, Cortese S. Association between anxiety and hypertension in adults: a systematic review and meta‐analysis. Neurosci Biobehav Rev 2021;131:96‐119. [DOI] [PubMed] [Google Scholar]
- 5. Cortese S, Moreira‐Maia CR, St Fleur D et al. Association between ADHD and obesity: a systematic review and meta‐analysis. Am J Psychiatry 2016;173:34‐43. [DOI] [PubMed] [Google Scholar]
- 6. Kim JY, Choi MJ, Ha S et al. Association between autism spectrum disorder and inflammatory bowel disease: a systematic review and meta‐analysis. Autism Res 2022;15:340‐52. [DOI] [PubMed] [Google Scholar]
- 7. Vancampfort D, Correll CU, Galling B et al. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta‐analysis. World Psychiatry 2016;15:166‐74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Arrondo G, Solmi M, Dragioti E et al. Associations between mental and physical conditions in children and adolescents: an umbrella review. Neurosci Biobehav Rev 2022;137:104662. [DOI] [PubMed] [Google Scholar]
- 9. Machado MO, Veronese N, Sanches M et al. The association of depression and all‐cause and cause‐specific mortality: an umbrella review of systematic reviews and meta‐analyses. BMC Med 2018;16:112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Scott KM, Lim C, Al‐Hamzawi A et al. Association of mental disorders with subsequent chronic physical conditions: World Mental Health Surveys from 17 countries. JAMA Psychiatry 2016;73:150‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Correll CU, Detraux J, De Lepeleire J et al. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry 2015;14:119‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Leucht S, Burkard T, Henderson J et al. Physical illness and schizophrenia: a review of the literature. Acta Psychiatr Scand 2007;116:317‐33. [DOI] [PubMed] [Google Scholar]
- 13. Correll CU, Solmi M, Veronese N et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large‐scale meta‐analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017;16:163‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Mezuk B, Eaton WW, Albrecht S et al. Depression and type 2 diabetes over the lifespan: a meta‐analysis. Diabetes Care 2008;31:2383‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Rugulies R. Depression as a predictor for coronary heart disease. a review and meta‐analysis. Am J Prev Med 2002;23:51‐61. [DOI] [PubMed] [Google Scholar]
- 16. Momen NC, Plana‐Ripoll O, Agerbo E et al. Association between mental disorders and subsequent medical conditions. N Engl J Med 2020;382:1721‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Morris G, Puri BK, Walker AJ et al. Shared pathways for neuroprogression and somatoprogression in neuropsychiatric disorders. Neurosci Biobehav Rev 2019;107:862‐82. [DOI] [PubMed] [Google Scholar]
- 18. Lando J, Williams SM, Williams B et al. A logic model for the integration of mental health into chronic disease prevention and health promotion. Prev Chronic Dis 2006;3:A61. [PMC free article] [PubMed] [Google Scholar]
- 19. Satin JR, Linden W, Phillips MJ. Depression as a predictor of disease progression and mortality in cancer patients: a meta‐analysis. Cancer 2009;115:5349‐61. [DOI] [PubMed] [Google Scholar]
- 20. Wang X, Wang N, Zhong L et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta‐analysis of 282,203 patients. Mol Psychiatry 2020;25:3186‐97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Meijer A, Conradi HJ, Bos EH et al. Adjusted prognostic association of depression following myocardial infarction with mortality and cardiovascular events: individual patient data meta‐analysis. Br J Psychiatry 2013;203:90‐102. [DOI] [PubMed] [Google Scholar]
- 22. Roest AM, Martens EJ, Denollet J et al. Prognostic association of anxiety post myocardial infarction with mortality and new cardiac events: a meta‐analysis. Psychosom Med 2010;72:563‐9. [DOI] [PubMed] [Google Scholar]
- 23. Atlantis E, Fahey P, Cochrane B et al. Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta‐analysis. Chest 2013;144:766‐77. [DOI] [PubMed] [Google Scholar]
- 24. Hofmann M, Kohler B, Leichsenring F et al. Depression as a risk factor for mortality in individuals with diabetes: a meta‐analysis of prospective studies. PLoS One 2013;8:e79809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Iversen MM, Nefs G, Tell GS et al. Anxiety and depressive symptoms as predictors of all‐cause mortality among people with insulin‐naive type 2 diabetes: 17‐year follow‐up of the second Nord‐Trondelag Health Survey (HUNT2), Norway. PLoS One 2016;11:e0160861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Liu L, Ni SY, Yan W et al. Mental and neurological disorders and risk of COVID‐19 susceptibility, illness severity and mortality: a systematic review, meta‐analysis and call for action. EClinicalMedicine 2021;40:101111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Rogers JP, Chesney E, Oliver D et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta‐analysis with comparison to the COVID‐19 pandemic. Lancet Psychiatry 2020;7:611‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Vai B, Mazza MG, Marisa CD et al. Joint European policy on the COVID‐19 risks for people with mental disorders: an umbrella review and evidence‐ and consensus‐based recommendations for mental and public health. Eur Psychiatry 2022;65:e47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bray F, Soerjomataram I. Population attributable fractions continue to unmask the power of prevention. Br J Cancer 2018;118:1031‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Shield KD, Parkin DM, Whiteman DC et al. Population attributable and preventable fractions: cancer risk factor surveillance, and cancer policy projection. Curr Epidemiol Rep 2016;3:201‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Whiteman DC, Webb PM, Green AC et al. Cancers in Australia in 2010 attributable to modifiable factors: summary and conclusions. Aust N Z J Public Health 2015;39:477‐84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Rezende LF, Eluf‐Neto J. Population attributable fraction: planning of diseases prevention actions in Brazil. Rev Saude Publica 2016;50:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Radua J, Ramella‐Cravaro V, Ioannidis JPA et al. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry 2018;17:49‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Dragioti E, Solmi M, Favaro A et al. Association of antidepressant use with adverse health outcomes: a systematic umbrella review. JAMA Psychiatry 2019;76:1241‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Ioannidis JP. Integration of evidence from multiple meta‐analyses: a primer on umbrella reviews, treatment networks and multiple treatments meta‐analyses. CMAJ 2009;181:488‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Sartorius N. Comorbidity of mental and physical diseases: a main challenge for medicine of the 21st century. Shanghai Arch Psychiatry 2013;25:68‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;10:89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Dekkers OM, Vandenbroucke JP, Cevallos M et al. COSMOS‐E: Guidance on conducting systematic reviews and meta‐analyses of observational studies of etiology. PLoS Med 2019;16:e1002742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Arango C, Dragioti E, Solmi M et al. Risk and protective factors for mental disorders beyond genetics: an evidence‐based atlas. World Psychiatry 2021;20:417‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Dragioti E, Radua J, Solmi M et al. Global population attributable fraction of potentially modifiable risk factors for mental disorders: a meta‐umbrella systematic review. Mol Psychiatry 2022; doi: 10.1038/s41380-022-01586-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Spitzer RL, Endicott J, Robins E. Research Diagnostic Criteria: rationale and reliability. Arch Gen Psychiatry 1978;35:773‐82. [DOI] [PubMed] [Google Scholar]
- 42. Kroenke K, Spitzer RL, Williams JB. The PHQ‐9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Whiting P, Savovic J, Higgins JP et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016;69:225‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Buhn S, Mathes T, Prengel P et al. The risk of bias in systematic reviews tool showed fair reliability and good construct validity. J Clin Epidemiol 2017;91:121‐8. [DOI] [PubMed] [Google Scholar]
- 45. Li L, Yang L, Luo B et al. Acupuncture for post‐stroke cognitive impairment: an overview of systematic reviews. Int J Gen Med 2022;15:7249‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Wells GA, Shea B, O'Connell D et al. The Newcastle‐Ottawa scale (NOS) for assessing the quality of non‐randomised studies in meta‐analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm.
- 47. Fusar‐Poli P, Radua J. Ten simple rules for conducting umbrella reviews. Evid Based Ment Health 2018;21:95‐100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Borenstein M, Hedges LV, Higgins JPT et al. Introduction to meta‐analysis. Hoboken: Wiley, 2009. [Google Scholar]
- 49. Fisher ZF, Tipton E. robumeta: an R‐package for robust variance estimation in meta‐analysis. arXiv:1503.02220.
- 50. Gosling CJ, Cartigny A, Mellier BC et al. Efficacy of psychosocial interventions for autism spectrum disorder: an umbrella review. Mol Psychiatry 2022; doi: 10.1038/s41380-022-01670-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Higgins JP, Thompson SG, Deeks JJ et al. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta‐analyses. BMJ 2011;342:d549. [DOI] [PubMed] [Google Scholar]
- 53. Sterne JA, Sutton AJ, Ioannidis JP et al. Recommendations for examining and interpreting funnel plot asymmetry in meta‐analyses of randomised controlled trials. BMJ 2011;343:d4002. [DOI] [PubMed] [Google Scholar]
- 54. Stanley TD, Doucouliagos H, Ioannidis JPA et al. Detecting publication selection bias through excess statistical significance. Res Synth Methods 2021;12:776‐95. [DOI] [PubMed] [Google Scholar]
- 55. Belbasis L, Bellou V, Evangelou E et al. Environmental risk factors and multiple sclerosis: an umbrella review of systematic reviews and meta‐analyses. Lancet Neurol 2015;14:263‐73. [DOI] [PubMed] [Google Scholar]
- 56. Markozannes G, Aretouli E, Rintou E et al. An umbrella review of the literature on the effectiveness of psychological interventions for pain reduction. BMC Psychol 2017;5:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Mukadam N, Sommerlad A, Huntley J et al. Population attributable fractions for risk factors for dementia in low‐income and middle‐income countries: an analysis using cross‐sectional survey data. Lancet Glob Health 2019;7:e596‐603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Levin ML. The occurrence of lung cancer in man. Acta Unio Int Contra Cancrum 1953;9:531‐41. [PubMed] [Google Scholar]
- 59. Lin C‐K, Chen S‐T. Estimation and application of population attributable fraction in ecological studies. Environ Health 2019;18:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Zhang J, Yu KF. What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998;280:1690‐1. [DOI] [PubMed] [Google Scholar]
- 61. Mansournia MA, Altman DG. Population attributable fraction. BMJ 2018;360:k757. [DOI] [PubMed] [Google Scholar]
- 62. Gosling CJ, Solanes A, Fusar‐Poli P et al. metaumbrella: the first comprehensive suite to perform data analysis in umbrella reviews with stratification of the evidence. Evid Based Ment Health (in press). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Barth J, Schumacher M, Herrmann‐Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta‐analysis. Psychosom Med 2004;66:802‐13. [DOI] [PubMed] [Google Scholar]
- 64. Bartoli F, Di Brita C, Crocamo C et al. Early post‐stroke depression and mortality: meta‐analysis and meta‐regression. Front Psychiatry 2018;9:530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Cai W, Mueller C, Li YJ et al. Post stroke depression and risk of stroke recurrence and mortality: a systematic review and meta‐analysis. Ageing Res Rev 2019;50:102‐9. [DOI] [PubMed] [Google Scholar]
- 66. Celano CM, Millstein RA, Bedoya CA et al. Association between anxiety and mortality in patients with coronary artery disease: a meta‐analysis. Am Heart J 2015;170:1105‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Chow YY, Verdonschot M, McEvoy CT et al. Associations between depression and cognition, mild cognitive impairment and dementia in persons with diabetes mellitus: a systematic review and meta‐analysis. Diabetes Res Clin Pract 2022;185:109227. [DOI] [PubMed] [Google Scholar]
- 68. Courtwright AM, Salomon S, Lehmann LS et al. The effect of pretransplant depression and anxiety on survival following lung transplant: a meta‐analysis. Psychosomatics 2016;57:238‐45. [DOI] [PubMed] [Google Scholar]
- 69. Ding G, Hua S, Chen J et al. Does cognitive decline/dementia increase delirium risk after stroke? Psychogeriatrics 2021;21:605‐11. [DOI] [PubMed] [Google Scholar]
- 70. Emdin CA, Odutayo A, Wong CX et al. Meta‐analysis of anxiety as a risk factor for cardiovascular disease. Am J Cardiol 2016;118:511‐9. [DOI] [PubMed] [Google Scholar]
- 71. Farooqi A, Khunti K, Abner S et al. Comorbid depression and risk of cardiac events and cardiac mortality in people with diabetes: a systematic review and meta‐analysis. Diabetes Res Clin Pract 2019;156:107816. [DOI] [PubMed] [Google Scholar]
- 72. Farrokhi F, Abedi N, Beyene J et al. Association between depression and mortality in patients receiving long‐term dialysis: a systematic review and meta‐analysis. Am J Kidney Dis 2014;63:623‐35. [DOI] [PubMed] [Google Scholar]
- 73. Flaherty LB, Wood T, Cheng A et al. Pre‐existing psychological depression confers increased risk of adverse cardiovascular outcomes following cardiac surgery: a systematic review and meta‐analysis. J Thorac Cardiovasc Surg 2017;154:1578‐86.e1. [DOI] [PubMed] [Google Scholar]
- 74. Gathright EC, Goldstein CM, Josephson RA et al. Depression increases the risk of mortality in patients with heart failure: a meta‐analysis. J Psychosom Res 2017;94:82‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Guo Y, Liu FT, Hou XH et al. Predictors of cognitive impairment in Parkinson's disease: a systematic review and meta‐analysis of prospective cohort studies. J Neurol 2021;268:2713‐22. [DOI] [PubMed] [Google Scholar]
- 76. Hariyanto TI, Putri C, Arisa J et al. Dementia and outcomes from coronavirus disease 2019 (COVID‐19) pneumonia: a systematic review and meta‐analysis. Arch Gerontol Geriatr 2021;93:104299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Li J, Ji F, Song J et al. Anxiety and clinical outcomes of patients with acute coronary syndrome: a meta‐analysis. BMJ Open 2020;10:e034135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Li JQ, Tan L, Wang HF et al. Risk factors for predicting progression from mild cognitive impairment to Alzheimer's disease: a systematic review and meta‐analysis of cohort studies. J Neurol Neurosurg Psychiatry 2016;87:476‐84. [DOI] [PubMed] [Google Scholar]
- 79. Liu Y, Wang Z, Xiao W. Risk factors for mortality in elderly patients with hip fractures: a meta‐analysis of 18 studies. Aging Clin Exp Res 2018;30:323‐30. [DOI] [PubMed] [Google Scholar]
- 80. Llamosas‐Falcon L, Shield KD, Gelovany M et al. Alcohol use disorders and the risk of progression of liver disease in people with hepatitis C virus infection – a systematic review. Subst Abuse Treat Prev Policy 2020;15:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Meijer A, Conradi HJ, Bos EH et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta‐analysis of 25 years of research. Gen Hosp Psychiatry 2011;33:203‐16. [DOI] [PubMed] [Google Scholar]
- 82. Mourao RJ, Mansur G, Malloy‐Diniz LF et al. Depressive symptoms increase the risk of progression to dementia in subjects with mild cognitive impairment: systematic review and meta‐analysis. Int J Geriatr Psychiatry 2016;31:905‐11. [DOI] [PubMed] [Google Scholar]
- 83. Ni L, Wu J, Long Y et al. Mortality of site‐specific cancer in patients with schizophrenia: a systematic review and meta‐analysis. BMC Psychiatry 2019;19:323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta‐analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J 2006;27:2763‐74. [DOI] [PubMed] [Google Scholar]
- 85. Palmer SC, Vecchio M, Craig JC et al. Association between depression and death in people with CKD: a meta‐analysis of cohort studies. Am J Kidney Dis 2013;62:493‐505. [DOI] [PubMed] [Google Scholar]
- 86. Pan A, Sun Q, Okereke OI et al. Depression and risk of stroke morbidity and mortality: a meta‐analysis and systematic review. JAMA 2011;306:1241‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Ruiz‐Grosso P, Cachay R, de la Flor A et al. Association between tuberculosis and depression on negative outcomes of tuberculosis treatment: a systematic review and meta‐analysis. PLoS One 2020;15:e0227472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Rutledge T, Reis VA, Linke SE et al. Depression in heart failure a meta‐analytic review of prevalence, intervention effects, and associations with clinical outcomes. J Am Coll Cardiol 2006;48:1527‐37. [DOI] [PubMed] [Google Scholar]
- 89. Schoultz M, Beattie M, Gorely T et al. Assessment of causal link between psychological factors and symptom exacerbation in inflammatory bowel disease: a systematic review utilising Bradford Hill criteria and meta‐analysis of prospective cohort studies. Syst Rev 2020;9:169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Scott W, Arkuter C, Kioskli K et al. Psychosocial factors associated with persistent pain in people with HIV: a systematic review with meta‐analysis. Pain 2018;159:2461‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Shi C, Lamba N, Zheng LJ et al. Depression and survival of glioma patients: a systematic review and meta‐analysis. Clin Neurol Neurosurg 2018;172:8‐19. [DOI] [PubMed] [Google Scholar]
- 92. Shi S, Liu T, Liang J et al. Depression and risk of sudden cardiac death and arrhythmias: a meta‐analysis. Psychosom Med 2017;79:153‐61. [DOI] [PubMed] [Google Scholar]
- 93. Sokoreli I, de Vries JJG, Pauws SC et al. Depression and anxiety as predictors of mortality among heart failure patients: systematic review and meta‐analysis. Heart Fail Rev 2016;21:49‐63. [DOI] [PubMed] [Google Scholar]
- 94. Song X, Song J, Shao M et al. Depression predicts the risk of adverse events after percutaneous coronary intervention: a meta‐analysis. J Affect Disord 2020;266:158‐64. [DOI] [PubMed] [Google Scholar]
- 95. Taggart Wasson L, Shaffer JA, Edmondson D et al. Posttraumatic stress disorder and nonadherence to medications prescribed for chronic medical conditions: a meta‐analysis. J Psychiatr Res 2018;102:102‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. van Dooren FE, Nefs G, Schram MT et al. Depression and risk of mortality in people with diabetes mellitus: a systematic review and meta‐analysis. PLoS One 2013;8:e57058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Wu Q, Kling JM. Depression and the risk of myocardial infarction and coronary death: a meta‐analysis of prospective cohort studies. Medicine 2016;95:e2815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Wu QE, Zhou AM, Han YP et al. Poststroke depression and risk of recurrent stroke: a meta‐analysis of prospective studies. Medicine 2019;98:e17235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Yuan M, Xiao ZL, Zhou HY et al. Bipolar disorder and the risk for stroke incidence and mortality: a meta‐analysis. Neurol Sci 2022;43:467‐76. [DOI] [PubMed] [Google Scholar]
- 100. Zhang WY, Nan N, Song XT et al. Impact of depression on clinical outcomes following percutaneous coronary intervention: a systematic review and meta‐analysis. BMJ Open 2019;9:e026445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Zhuo C, Tao R, Jiang R et al. Cancer mortality in patients with schizophrenia: systematic review and meta‐analysis. Br J Psychiatry 2017;211:7‐13. [DOI] [PubMed] [Google Scholar]
- 102. Blochl M, Meissner S, Nestler S. Does depression after stroke negatively influence physical disability? A systematic review and meta‐analysis of longitudinal studies. J Affect Disord 2019;247:45‐56. [DOI] [PubMed] [Google Scholar]
- 103. Fusar‐Poli P. TRANSD recommendations: improving transdiagnostic research in psychiatry. World Psychiatry 2019;18:361‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Fusar‐Poli P, Solmi M, Brondino N et al. Transdiagnostic psychiatry: a systematic review. World Psychiatry 2019;18:192‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Whooley MA, Wong JM. Depression and cardiovascular disorders. Annu Rev Clin Psychol 2013;9:327‐54. [DOI] [PubMed] [Google Scholar]
- 106. Gan Y, Gong Y, Tong X et al. Depression and the risk of coronary heart disease: a meta‐analysis of prospective cohort studies. BMC Psychiatry 2014;14:371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. De Hert M, Detraux J, Vancampfort D. The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin Neurosci 2018;20:31‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108. Gold SM, Köhler‐Forsberg O, Moss‐Morris R et al. Comorbid depression in medical diseases. Nat Rev Dis Primers 2020;6:69. [DOI] [PubMed] [Google Scholar]
- 109. Shao M, Lin X, Jiang D et al. Depression and cardiovascular disease: shared molecular mechanisms and clinical implications. Psychiatry Res 2020;285:112802. [DOI] [PubMed] [Google Scholar]
- 110. Penninx BW. Depression and cardiovascular disease: epidemiological evidence on their linking mechanisms. Neurosci Biobehav Rev 2017;74:277‐86. [DOI] [PubMed] [Google Scholar]
- 111. Grippo AJ, Johnson AK. Biological mechanisms in the relationship between depression and heart disease. Neurosci Biobehav Rev 2002;26:941‐962. [DOI] [PubMed] [Google Scholar]
- 112. Joynt KE, Whellan DJ, O'Connor CM. Depression and cardiovascular disease: mechanisms of interaction. Biol Psychiatry 2003;54:248‐61. [DOI] [PubMed] [Google Scholar]
- 113. Stapelberg NJ, Neumann DL, Shum DH et al. A topographical map of the causal network of mechanisms underlying the relationship between major depressive disorder and coronary heart disease. Aust N Z J Psychiatry 2011;45:351‐69. [DOI] [PubMed] [Google Scholar]
- 114. Hare DL, Toukhsati SR, Johansson P et al. Depression and cardiovascular disease: a clinical review. Eur Heart J 2014;35:1365‐72. [DOI] [PubMed] [Google Scholar]
- 115. Khandaker GM, Zuber V, Rees JMB et al. Shared mechanisms between coronary heart disease and depression: findings from a large UK general population‐based cohort. Mol Psychiatry 2020;25:1477‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Howren MB, Lamkin DM, Suls J. Associations of depression with C‐reactive protein, IL‐1, and IL‐6: a meta‐analysis. Psychosom Med 2009;71:171‐86. [DOI] [PubMed] [Google Scholar]
- 117. Jiménez‐Fernández S, Gurpegui M, Díaz‐Atienza F et al. Oxidative stress and antioxidant parameters in patients with major depressive disorder compared to healthy controls before and after antidepressant treatment: results from a meta‐analysis. J Clin Psychiatry 2015;76:1658‐67. [DOI] [PubMed] [Google Scholar]
- 118. Jiménez‐Fernández S, Gurpegui M, Garrote‐Rojas D et al. Oxidative stress parameters and antioxidants in adults with unipolar or bipolar depression versus healthy controls: systematic review and meta‐analysis. J Affect Disord 2022;314:211‐21. [DOI] [PubMed] [Google Scholar]
- 119. Taylor CB, Youngblood ME, Catellier D et al. Effects of antidepressant medication on morbidity and mortality in depressed patients after myocardial infarction. Arch Gen Psychiatry 2005;62:792‐8. [DOI] [PubMed] [Google Scholar]
- 120. O'Connor CM, Jiang W, Kuchibhatla M et al. Antidepressant use, depression, and survival in patients with heart failure. Arch Intern Med 2008;168:2232‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Fernandes BS, Salagre E, Enduru N et al. Insulin resistance in depression: a large meta‐analysis of metabolic parameters and variation. Neurosci Biobehav Rev 2022;139:104758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Penninx BWJH, Milaneschi Y, Lamers F et al. Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Med 2013;11:129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Vancampfort D, Correll CU, Wampers M et al. Metabolic syndrome and metabolic abnormalities in patients with major depressive disorder: a meta‐analysis of prevalences and moderating variables. Psychol Med 2014;44:2017‐28. [DOI] [PubMed] [Google Scholar]
- 124. Vian J, Pereira C, Chavarria V et al. The renin‐angiotensin system: a possible new target for depression. BMC Med 2017;15:144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Kobori H, Nangaku M, Navar LG et al. The intrarenal renin‐angiotensin system: from physiology to the pathobiology of hypertension and kidney disease. Pharmacol Rev 2007;59:251‐87. [DOI] [PubMed] [Google Scholar]
- 126. Rosenblat JD, Mansur RB, Cha DS et al. Depression, diabetes and dementia. In: Sartorius N, Holt RIG, Maj M (eds). Comorbidity of mental and physical disorders. Basel: Karger, 2015:42‐53. [Google Scholar]
- 127. Sullivan MD, Katon WJ, Lovato LC et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD‐MIND trial. JAMA Psychiatry 2013;70:1041‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Katon W, Pedersen HS, Ribe AR et al. Effect of depression and diabetes mellitus on the risk for dementia: a national population‐based cohort study. JAMA Psychiatry 2015;72:612‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Mousten IV, Sørensen NV, Christensen RHB et al. Cerebrospinal fluid biomarkers in patients with unipolar depression compared with healthy control individuals: a systematic review and meta‐analysis. JAMA Psychiatry 2022;79:571‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Brzezińska A, Bourke J, Rivera‐Hernández R et al. Depression in dementia or dementia in depression? Systematic review of studies and hypotheses. Curr Alzheimer Res 2020;17:16‐28. [DOI] [PubMed] [Google Scholar]
- 131. Jamieson A, Goodwill AM, Termine M et al. Depression related cerebral pathology and its relationship with cognitive functioning: a systematic review. J Affect Disord 2019;250:410‐8. [DOI] [PubMed] [Google Scholar]
- 132. Brayne C, Miller B. Dementia and aging populations – A global priority for contextualized research and health policy. PLoS Med 2017;14:e1002275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Siu AL, US Preventive Services Task Force (USPSTF) , Bibbins‐Domingo K et al. Screening for depression in adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016;315:380‐7. [DOI] [PubMed] [Google Scholar]
- 134. Fan RR, Rudnick SB, Minami HR et al. Depression screening in patients with vascular disease. Vascular 2022; doi: 10.1177/17085381221084817. [DOI] [PubMed] [Google Scholar]
- 135. Breedvelt JJF, Kandola A, Kousoulis AA et al. What are the effects of preventative interventions on major depressive disorder (MDD) in young adults? A systematic review and meta‐analysis of randomized controlled trials. J Affect Disord 2018;239:18‐29. [DOI] [PubMed] [Google Scholar]
- 136. Cuijpers P, van Straten A, Smit F et al. Preventing the onset of depressive disorders: a meta‐analytic review of psychological interventions. Am J Psychiatry 2008;165:1272‐80. [DOI] [PubMed] [Google Scholar]
- 137. Salazar de Pablo G, Solmi M, Vaquerizo‐Serrano J et al. Primary prevention of depression: an umbrella review of controlled interventions. J Affect Disord 2021;294:957‐70. [DOI] [PubMed] [Google Scholar]
- 138. Coventry P, Lovell K, Dickens C et al. Integrated primary care for patients with mental and physical multimorbidity: cluster randomised controlled trial of collaborative care for patients with depression comorbid with diabetes or cardiovascular disease. BMJ 2015;350:h638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Terada T, Cotie LM, Tulloch H et al. Sustained effects of different exercise modalities on physical and mental health in patients with coronary artery disease: a randomized clinical trial. Can J Cardiol 2022;38:1235‐43. [DOI] [PubMed] [Google Scholar]
- 140. Reed JL, Terada T, Cotie LM et al. The effects of high‐intensity interval training, Nordic walking and moderate‐to‐vigorous intensity continuous training on functional capacity, depression and quality of life in patients with coronary artery disease enrolled in cardiac rehabilitation: a randomized controlled trial (CRX study). Prog Cardiovasc Dis 2022;70:73‐83. [DOI] [PubMed] [Google Scholar]
- 141. Ali MK, Chwastiak L, Poongothai S et al. Effect of a collaborative care model on depressive symptoms and glycated hemoglobin, blood pressure, and serum cholesterol among patients with depression and diabetes in India: the INDEPENDENT randomized clinical trial. JAMA 2020;324:651‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Srinivasan K, Heylen E, Johnson Pradeep R et al. Collaborative care compared to enhanced standard treatment of depression with co‐morbid medical conditions among patients from rural South India: a cluster randomized controlled trial (HOPE Study). BMC Psychiatry 2022;22:394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Goldstein BI, Carnethon MR, Matthews KA et al. Major depressive disorder and bipolar disorder predispose youth to accelerated atherosclerosis and early cardiovascular disease: a scientific statement from the American Heart Association. Circulation 2015;132:965‐86. [DOI] [PubMed] [Google Scholar]
- 144. Correll CU, Solmi M, Croatto G et al. Mortality in people with schizophrenia: a systematic review and meta‐analysis of relative risk and aggravating or attenuating factors. World Psychiatry 2022;21:248‐71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Lambert AM, Parretti HM, Pearce E et al. Temporal trends in associations between severe mental illness and risk of cardiovascular disease: a systematic review and meta‐analysis. PLoS Med 2022;19:e1003960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Solmi M, Fiedorowicz J, Poddighe L et al. Disparities in screening and treatment of cardiovascular diseases in patients with mental disorders across the world: systematic review and meta‐analysis of 47 observational studies. Am J Psychiatry 2021;178:793‐803. [DOI] [PubMed] [Google Scholar]
- 147. Solmi M, Firth J, Miola A et al. Disparities in cancer screening in people with mental illness across the world versus the general population: prevalence and comparative meta‐analysis including 4 717 839 people. Lancet Psychiatry 2020;7:52‐63. [DOI] [PubMed] [Google Scholar]
- 148. Keenan TE, Yu A, Cooper LA et al. Racial patterns of cardiovascular disease risk factors in serious mental illness and the overall U.S. population. Schizophr Res 2013;150:211‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149. Ratliff JC, Palmese LB, Reutenauer EL et al. Obese schizophrenia spectrum patients have significantly higher 10‐year general cardiovascular risk and vascular ages than obese individuals without severe mental illness. Psychosomatics 2013;54:67‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150. Dickerson F, Origoni A, Schroeder J et al. Mortality in schizophrenia and bipolar disorder: clinical and serological predictors. Schizophr Res 2016;170:177‐83. [DOI] [PubMed] [Google Scholar]
- 151. Nordentoft M, Plana‐Ripoll O, Laursen TM. Cancer and schizophrenia. Curr Opin Psychiatry 2021;34:260‐5. [DOI] [PubMed] [Google Scholar]
- 152. Vancampfort D, Stubbs B, Mitchell AJ et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta‐analysis. World Psychiatry 2015;14:339‐47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153. Goff DC, Sullivan LM, McEvoy JP et al. A comparison of ten‐year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr Res 2005;80:45‐53. [DOI] [PubMed] [Google Scholar]
- 154. Crump C, Winkleby MA, Sundquist K et al. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am J Psychiatry 2013;170:324‐33. [DOI] [PubMed] [Google Scholar]
- 155. Kane JM, Kishimoto T, Correll CU. Non‐adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry 2013;12:216‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156. Pillinger T, McCutcheon RA, Vano L et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta‐analysis. Lancet Psychiatry 2020;7:64‐77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157. Solmi M, Tiihonen J, Lähteenvuo M et al. Antipsychotics use is associated with greater adherence to cardiometabolic medications in patients with schizophrenia: results from a nationwide, within‐subject design study. Schizophr Bull 2022;48:166‐75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158. Oliver D, Arribas M, Radua J et al. Prognostic accuracy and clinical utility of psychometric instruments for individuals at clinical high‐risk of psychosis: a systematic review and meta‐analysis. Mol Psychiatry 2022; doi: 10.1038/s41380-022-01611-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159. Estradé A, Salazar de Pablo G, Zanotti A et al. Public health primary prevention implemented by clinical high‐risk services for psychosis. Transl Psychiatry 2022;12:43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160. Salazar de Pablo G, Radua J, Pereira J et al. Probability of transition to psychosis in individuals at clinical high risk: an updated meta‐analysis. JAMA Psychiatry 2021;78:970‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161. Catalan A, Salazar de Pablo G, Vaquerizo Serrano J et al. Annual research review: Prevention of psychosis in adolescents – systematic review and meta‐analysis of advances in detection, prognosis and intervention. J Child Psychol Psychiatry 2021;62:657‐73. [DOI] [PubMed] [Google Scholar]
- 162. Fusar‐Poli P, Spencer T, De Micheli A et al. Outreach and support in South‐London (OASIS) 2001‐2020: twenty years of early detection, prognosis and preventive care for young people at risk of psychosis. Eur Neuropsychopharmacol 2020;39:111‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163. Fusar‐Poli P, Salazar de Pablo G, Correll CU et al. Prevention of psychosis: advances in detection, prognosis, and intervention. JAMA Psychiatry 2020;77:755‐65. [DOI] [PubMed] [Google Scholar]
- 164. Kotlicka‐Antczak M, Podgórski M, Oliver D et al. Worldwide implementation of clinical services for the prevention of psychosis: the IEPA early intervention in mental health survey. Early Interv Psychiatry 2020;14:741‐50. [DOI] [PubMed] [Google Scholar]
- 165. Fusar‐Poli P, Correll CU, Arango C et al. Preventive psychiatry: a blueprint for improving the mental health of young people. World Psychiatry 2021;20:200‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166. Nieto JC, Sánchez E, Román E et al. Cytokine production in patients with cirrhosis and TLR4 polymorphisms. World J Gastroenterol 2014;20:17516‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167. Fuster D, Sanvisens A, Bolao F et al. Alcohol use disorder and its impact on chronic hepatitis C virus and human immunodeficiency virus infections. World J Hepatol 2016;8:1295‐308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168. Hutchinson SJ, Bird SM, Goldberg DJ. Influence of alcohol on the progression of hepatitis C virus infection: a meta‐analysis. Clin Gastroenterol Hepatol 2005;3:1150‐9. [DOI] [PubMed] [Google Scholar]
- 169. Abassa KK, Wu XY, Xiao XP et al. Effect of alcohol on clinical complications of hepatitis virus‐induced liver cirrhosis: a consecutive ten‐year study. BMC Gastroenterol 2022;22:130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170. Curry SJ, Krist AH, Owens DK et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: US Preventive Services Task Force Recommendation Statement. JAMA 2018;320:1899‐909. [DOI] [PubMed] [Google Scholar]
- 171. Solmi M, Radua J, Olivola M et al. Age at onset of mental disorders worldwide: large‐scale meta‐analysis of 192 epidemiological studies. Mol Psychiatry 2022;27:281‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172. Fusar‐Poli P, Manchia M, Koutsouleris N et al. Ethical considerations for precision psychiatry: a roadmap for research and clinical practice. Eur Neuropsychopharmacol 2022;63:17‐34. [DOI] [PubMed] [Google Scholar]
- 173. O'Neil A, Jacka FN, Quirk SE et al. A shared framework for the common mental disorders and non‐communicable disease: key considerations for disease prevention and control. BMC Psychiatry 2015;15:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174. McGorry PD, Mei C, Chanen A et al. Designing and scaling up integrated youth mental health care. World Psychiatry 2022;21:61‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175. Perera S, Hetrick S, Cotton S et al. Awareness of headspace youth mental health service centres across Australian communities between 2008 and 2015. J Ment Health 2020;29:410‐7. [DOI] [PubMed] [Google Scholar]
- 176. Malla A, Boksa P, Joober R. Meeting the challenges of the new frontier of youth mental health care. World Psychiatry 2022;21:78‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177. Kieling C, Salum GA, Pan PM et al. Youth mental health services: the right time for a global reach. World Psychiatry 2022;21:86‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]