

Abstract
Background
Penetrating chest trauma can have lethal consequences. Anterior chest wall penetrating injury can cause fatal lacerations over the chest wall, lungs, pericardium, and the heart. There are few reports on these kinds of injuries and operative management.
Purpose
To describe a case of penetrating chest trauma with right atrium ruptured, after a fall from height. The patient was successfully managed with prompt resuscitation and definitive surgical intervention.
Case presentation
A 48-years-old gentleman presented with history of fall from height and right sided penetrating chest injury. The patient had a penetrating injury to the right-fourth intercostal space in parasternal region. Chest X-ray showed massive right-sided hemothorax and chest tube drained more than 1700 ml upon insertion. Emergency right thoracotomy was performed, after initial resuscitation with fluids and blood transfusion in the emergency department. He had injury to the intercostal arteries, lacerations of the pericardium and the right atrium ruptured, which was managed successfully with definitive repair.
Conclusion
Survival is rare after penetrating chest trauma with right atrium ruptured if not intervened on time. Prompt diagnosis and resuscitation, along with the definitive surgical repair were the key elements for successful management of the patients.
Keywords: Hemothorax, Penetrating chest trauma, Pericardium laceration, Right atrium ruptured, Intercostal artery injury
Introduction
Chest trauma patients can present in many different ways from stable to cardiovascular collapse requiring immediate attention. Blunt trauma chest is generally considered less deadly than penetrating chest trauma, especially when the force of impact is close to the heart and the pericardium. Penetrating chest trauma occurs mostly due to stabbing, gunshots, blast injuries fragments, industrial accidents, collisions, and falls from height [1].
Chest trauma has the highest mortality and up to 60 % has been reported in some studies depending on the pattern of trauma. Patents with injury to the cardiac chambers have less chance of survival in the absence of quick presentation, evaluation, and definitive surgical repair [2].
A 48-years-old male presented to emergency department with history of fall from around 15 ft height. He was under influence of alcohol and presented to us almost 6 h after the incidence. He had injury to head and 3 × 3 cm penetrating wound on the right anterior chest wall fourth intercostal space near the parasternal region (Fig. 1), and swelling of the right shoulder and right wrist.
Fig. 1.

Showing initial chest wall injury.
The patient gave a history of loss of consciousness for 30 min before arrival at the emergency department; however, there was no history of vomiting or ear, nose and throat bleeding, and the patient was drowsy but oriented to time and place. The blood pressure was around 80/60 mmHg and pulse rate and respiratory rate were 120 and 24 respectively with oxygen saturation of 92 % on 2 l oxygen. There was oozing of blood from the chest wound and there was a scalp laceration in the right fronto-parietal region with no active bleeding.
After the initial resuscitation, the blood pressure was 90/60 and chest X-ray AP view, CT scan head, and sonographic evaluation was done. X-ray and extended focused sonographic assessment scan showed right-sided massive haemothorax (Fig. 2). CT head showed a normal brain scan with scalp laceration. A chest tube was inserted for right-sided haemothorax which drained 1700 ml of blood upon insertion.
Fig. 2.
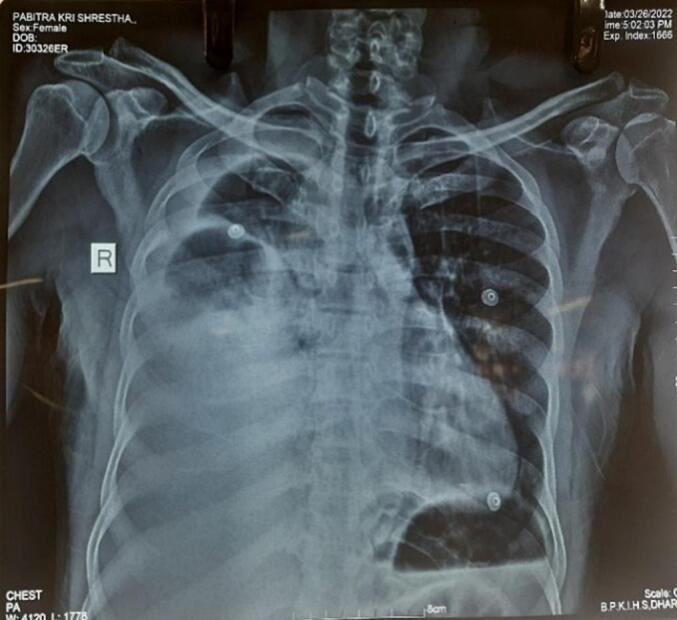
Shows right-sided hemothorax.
The patient was transferred immediately to the emergency operating room with blood products for emergency thoracotomy under general anesthesia. A central venous catheter was inserted and after induction, a broad-spectrum antibiotic was given. The patient had phimosis and a dorsal split was done for foley's catheter insertion. The patient was positioned supine with the right chest slightly up. The penetrating chest wound was inspected and was found to have multiple bleeders from the fractured ribs and intercostals vessels. The wound was extended laterally after control of the adjacent bleeders to inspect the underlying lungs and the pericardium (Fig. 3). A pericardial tear of about 3 × 3 cm was noted with clot and hemopericardium. Right atrium wall laceration and rupture was noted after removal of clot and blood from pericardial space (Fig. 4).
Fig. 3.

Pericardial breach.
Fig. 4.

Right atrium defect with blood spurting.
A tangential Satinsky clamp was applied on lacerated right atrial wall (Fig. 5). The heart rate dropped to 115/m from 180 per minute and blood pressure increased to 90/60 mmHg. The camped right atrium wall was repaired using 5-0 double arm polypropylene suture in double layers till the hemostasis was achieved. The thoracic cavity was reinspected for any injury or bleeders and all hemostasis was secured.
Fig. 5.

RA wall clamp by Satinsky clamp.
The thoracic cavity was washed with normal saline and closed in layers after the insertion of two chest drains. The patient was then shifted to the intensive care unit for further evaluation, monitoring, and management. The patient was extubated on the second postoperative day, following which the patient developed restlessness and delirium for which echocardiography, CT head and chest was done which was normal. A psychiatry consultation was done for possible alcohol withdrawal. The patient was reintubated the following day due to increased heart rate and respiratory rate and was extubated on the fourth postoperative day and transferred to the ward on the eight postoperative days.
Repeat X-ray showed moderate right-sided pleural effusion and pleural tapping was done. Orthopedic consultation was done for a right wrist injury and the patient was managed with closed reduction with slab application for right lunate dislocation with a further plan to reevaluate once patient was stable. The patient was discharged on the eleventh postoperative day. The patient was doing well after three months of follow up (Fig. 6).
Fig. 6.

Postoperative X-ray.
Discussion
Blunt and penetrating chest trauma continues to be challenging for the emergency physicians and the attending surgeons. Surgical emergencies like traumatic cardiac chamber rupture display great diagnostic dilemma. However, proper diagnosis and prompt surgical intervention provides great therapeutic reward. The initial primary survey, resuscitation and a high level of suspicion of underlying injury are important factors for survival after the trauma [3], [4].
Our case presented almost 6 h after the injury and high level of a suspicion of underlying injury were made after understanding the mechanism and location of impact on the chest wall. The penetrating injury was just above the right atrium which raised the possibility of injury to the right side of the heart. Massive bleeding from the chest tube after its insertion indicated major internal hemorrhage. The patient was immediately transferred to the operating room along with blood products, resuscitation being done simultaneously.
Chest traumas leading to cardiac lacerations and rupture is a relatively rare phenomenon mostly occurring in gunshot injuries in the war. The most common chamber involved in projectile injuries of the heart is the right atrium and ventricle due to its anatomical location [2]. There are three primary physiological disturbances associated with cardiac trauma; hemorrhage, pericardial tamponade, and cardiac failure [5]. Frequently the dominant physiological injury in surviving patients is cardiac tamponade which provides an early opportunity for survival by delaying or stopping bleeding from cardiac lacerations, which was seen in this case scenario.
Andres et al. in the retrospective study of penetrating cardiac injuries, which were mostly due to stab and gunshots, showed that there were high pre-hospitalization mortality associated with penetrating cardiac injury and pericardial window was the preferred diagnostic method followed by sternotomy for a definitive surgical approach [6].
In our case, the penetrated wound was large and had active bleeding. In the view to control the adjacent intercostal vessels bleeding, and view the structures beneath, the incision was further elaborated down which caught our site to the lacerated pericardium and the right atrium. The right atrium is the most common site of injury due to its thin wall and low pressure. The patient usually has cardiac tamponade on presentation and needs an urgent pericardial window [7], [8]. However, our patient developed hypotension and tachycardia at the time of induction which made us rush for definitive surgical repair. The patient recovered well due to the combined team effort and was discharged on the eleventh postoperative day and has been doing well in the follow-up.
Conclusion
Penetrating chest traumatic and right atrium rupture survival is rare and prompt diagnosis, resuscitation with fluids and blood, along with definitive surgical repairs were the keys elements for the successful management of the patients.
References
- 1.Scott M.F., Sava J.A. Penetrating injuries to the lung and heart: resuscitation, diagnosis, and operative indications. Curr. Trauma Rep. 2015;1:203–211. [Google Scholar]
- 2.Lasek J., Jadczuk E. Thoracic trauma - principals of surgical management. Eur. J. Transl. Clin. Med. 2020;3:66–73. [Google Scholar]
- 3.Jain A., Sekusky A.L., Burns B. Common Surgical Diseases: An Algorithmic Approach to Problem Solving. Third Edition. 2021. Penetrating chest trauma; pp. 41–43. [Google Scholar]
- 4.Elkhonezy B.A., Abdelmoaty H.M., Gamil I.K. Factors improve outcome of penetrating chest trauma. Egypt. J. Hosp. Med. 2021;83:1400–1405. [Google Scholar]
- 5.Gosavi S., Tyroch A.H., Mukherjee D. Cardiac trauma. Angiology. 2016;67:896–901. doi: 10.1177/0003319715627954. [DOI] [PubMed] [Google Scholar]
- 6.Isaza-Restrepo A., Bolívar-Sáenz D.J., Tarazona-Lara M., et al. Penetrating cardiac trauma: analysis of 240 cases from a hospital in Bogota, Colombia. World Journal of Emergency Surgery; 2017:12. doi: 10.1186/S13017-017-0138-1. Epub ahead of print 12 June. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Johnny C.S., Vasudeva M., Gooi J., et al. Right atrial appendage rupture and cardiac tamponade secondary to blunt trauma. Trauma Case Reports. 2022;38 doi: 10.1016/j.tcr.2022.100620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rajabifard P., Agarwal A., Skillington P., et al. Pericardial rupture and chronic subluxation of the heart: a case report. World J. Cardiovasc. Surg. 2021;11:75–81. [Google Scholar]