

Abstract
Objective:
While self-monitoring can help mitigate alcohol misuse in young adults, engagement with digital self-monitoring is suboptimal. The present study investigates the utility of two types of digital prompts (reminders) to encourage young adults to self-monitor their alcohol use. These prompts leverage information that is self-relevant (i.e., represents and is valuable) to the person.
Method:
591 college students (Mage=18; 61%=female, 76%=White) were enrolled in an 8-week intervention study involving biweekly digital self-monitoring of their alcohol use. At baseline, participants selected an item they would like to purchase for themselves and their preferred charitable organization. Then, biweekly, participants were micro-randomized to a prompt highlighting the opportunity to either (a) win their preferred item (Self-Interest Prompt); or (b) donate to their preferred charity (Prosocial Prompt). Following self-monitoring completion, participants allocated reward points toward lottery drawings for their preferred item or charity.
Results:
The Self-Interest (vs. Prosocial) Prompt was significantly more effective in promoting proximal self-monitoring at the beginning of the study (Est=exp(.14)=1.15; 95% CI:[1.01, 1.29]), whereas the Prosocial (vs. Self-Interest) Prompt was significantly more effective at the end (Est=exp(−.17)=0.84; 95% CI:[0.70, 0.98]). Further, the Prosocial (vs. Self-Interest) Prompt was significantly more effective among participants who previously allocated all their reward points to drawings for their preferred item (Est=exp(−.15)=0.86; 95% CI:[.75, .97]).
Conclusions:
These results suggest that the advantage of prompts that appeal to a person’s self-interest (vs. prosocial) motives varies over time and based on what reward options participants prioritized in previous decisions. Theoretical and practical implications for intervention design are discussed.
Keywords: engagement, self-monitoring, alcohol use, self-relevance, micro-randomized trial
Alcohol use among young adults is a prevalent and important public health problem in the United States. Extant research indicates that approximately 65% of college undergraduates regularly consume alcohol, and about a quarter report binge drinking (i.e., 5+ drinks in a row) at least once within a two-week period (Schulenberg et al., 2020). Self-monitoring holds great promise for reducing alcohol use and the associated negative consequences (National Institute on Alcohol Abuse and Alcoholism, 2019). Typically, self-monitoring is defined as a technique used to deliberately promote behavior change through the systematic observation and documentation of one’s own behavior in a naturalist setting, across a pre-specified time period (König et al., 2022; Korotitsch & Nelson-Gray, 1999; Nelson & Hayes, 1981). Self-monitoring may occur daily, weekly, or even biweekly (Gatto et al., 2022; Simpson et al., 2005).
Systematic reviews indicate that self-monitoring is one of the most effective intervention components for behavior change across a variety of health domains (cf. Garnett et al., 2015; Hennessy et al., 2020; Michie et al., 2009). Self-monitoring promotes behavior change by increasing self-reflection and self-awareness (cf. Epstein et al., 2008; Klasnja et al., 2011) and by allowing opportunities for the provision of feedback to support self-regulation. Additionally, self-monitoring provides information that can be useful for tailoring (i.e., informing subsequent intervention decisions) for reducing alcohol use to address the changing needs of individuals (Patrick et al., 2020; Patrick et al., 2021).
Advances in mobile and wireless technology can be used to increase the convenience and accessibility of self-monitoring tools (Bidargaddi et al., 2018; Rabbi et al., 2018). Yet, engagement (i.e., energy invested in a focal task or stimulus; Nahum-Shani et al., 2022) with digital tools remains a critical barrier as individuals abandon digital self-monitoring quickly and after minimal use (Nahum-Shani et al., 2021). For example, a recent systematic review of digital self-monitoring in weight loss interventions found modest engagement in digital self-monitoring, with very few interventions meeting an average threshold of 75% completion (Patel et al., 2021). Identifying strategies to increase engagement in self-monitoring has the potential to attenuate risky alcohol use among college students.
Financial incentives are commonly used to motivate behavior (Camerer & Hogarth, 1999), with evidence supporting their utility in promoting intervention engagement among young adults, including college students (An et al., 2006; Mitchell et al., 2013). However, interventions that rely solely on large monetary incentives are relatively costly and less scalable to the population of young adults in the United States at risk for alcohol misuse (Merrill & Carey, 2016). Financial incentives are also not universally beneficial and can undermine intrinsic motivation and hinder sustained engagement, particularly when provided to individuals who are already motivated (Camerer & Hogarth, 1999; Gneezy et al., 2011). Strategies grounded in decision science can be leveraged to address these challenges and to design incentive systems that rely less heavily on financial incentives (Nahum-Shani et al., 2021).
Extant research in psychology and decision science suggests that engagement can be enhanced by offering information that is self-relevant; that is, information that represents and is valuable to the self (Short et al., 2015; Vansteenkiste et al., 2018). The self-relevance of a relatively modest financial incentive may be enhanced by highlighting self-interest motives and/or prosocial motives (Muir et al., 2021). Self-interest motives concern the desire to benefit oneself (Folger & Salvador, 2008), which is primarily driven by a focus on economic and reputational benefits (Muir et al., 2021). For example, individuals may be motivated to engage in a given task because the monetary incentives they receive for engaging can be used to purchase desired items, such as a tablet or a laptop (Alba & Williams, 2013). Prosocial motives concern the desire to invest effort in helping other people (Grant, 2008). Many individuals strive to be altruistic and socially responsible, which often translates into donations to a charitable cause (Aknin et al., 2020; Bekkers & Wiepking, 2011). Thus, connecting minimal monetary incentives to self-interest and prosocial motives holds great potential for increasing engagement. The present study aims to investigate the potential utility of leveraging these strategies to promote engagement in self-monitoring of alcohol use in the context of an adaptive preventive intervention for college students. Hypotheses for the present study were specified in an open science protocol prior to data analysis (Carpenter et al., 2021; https://osf.io/dkvz3).
Self-Monitoring of Alcohol Use in an Adaptive Preventive Intervention
Adaptive preventive interventions (APIs) represent a promising approach for addressing alcohol misuse because they provide the right type of intervention to those who need it, when they need it (Collins et al., 2004; Hall et al., 2019). Integrating self-monitoring into an alcohol use API can provide useful information about if and when an individual is in need of intervention. The API developed by Patrick and colleagues (Patrick et al., 2020; Patrick et al., 2021) was designed to reduce binge drinking. It included encouraging undergraduates to self-monitor their alcohol use and associated consequences biweekly during the first semester of college. This intervention transitioned incoming, first-year college students who self-reported heavy drinking from universal (i.e., low-intensity programs delivered to all students regardless of their level of risk) to indicated (i.e., more intensive programs delivered to higher risk groups who already showed detectable symptoms that signal elevated risk) alcohol prevention resources during the Fall semester. The universal intervention included two components: (i) personalized normative feedback and (ii) bi-weekly self-monitoring of alcohol use. Students who reported heavy drinking during the self-monitoring period transitioned out of the universal intervention and were encouraged to access indicated interventions to address their heavy drinking (see Patrick et al., 2020; Patrick et al., 2021 for more details). Students who did not report heavy drinking continued to self-monitor their alcohol use.
This API provided an opportunity to investigate the utility of engagement strategies based on decision science principles because for this intervention to be scalable, only relatively minimal financial incentives could be offered for self-monitoring. Specifically, participants received $2 for completion of each of up to 4 biweekly self-monitoring assessments. This incentive is considered relatively modest given that extant substance use studies often pay between $2 and $5 for daily assessments and yield average completion rates of less than 65% for young adults (cf. Bonar et al., 2018; Dworkin et al., 2017). Importantly, studies that explicitly focused on repeated assessments of alcohol use (e.g., every week or several weeks) either employed financial incentives that are not guaranteed (e.g., a prize draw to win a £25 voucher; Bewick et al., 2010) and achieved relatively low (e.g., less than 65%) completion rates, or yielded higher completion rates (e.g., 75%−86%) by combining minimal guaranteed incentives (e.g., $.50, $2) with relatively high completion-based bonuses (e.g., an extra $20 each semester for completing the majority of assessments; Barnett et al., 2015) or human support to encourage completion, which is both costly and complex to implement (Nahum-Shani et al., 2021). Thus, an important question is whether and how self-relevance can be leveraged to increase the perceived value of self-monitoring when only relatively minimal financial incentives are provided.
Self-Interest versus Prosocial Appeals
One way to increase the value of minimal monetary incentives for self-monitoring is to highlight their self-relevance in the request (i.e., prompt) to self-monitor. Extant literature in decision science suggests that the self-relevance of relatively minimal rewards can be enhanced via appeals to the person’s self-interest and/or prosocial motives (Aknin et al., 2020; Alba & Williams, 2013; Muir et al., 2021). Although people are typically motivated to enhance their own personal welfare, they also strive to enhance the welfare of other people or entities that are tied to their identity, beliefs, or values (Bekkers & Wiepking, 2011; Goldstein et al., 2011). This motivation can be so strong that it may lead people to sacrifice their own resources to support those valued people or entities (Batson & Shaw, 1991; O’Reilly & Chatman, 1986). However, the accumulation and display of resources are particularly important to young adults (Freund & Blanchard-Fields, 2014; Freund & Riediger, 2001) due to their focus on the pursuit of expansive goals (e.g., making connections, acquiring resources) that are anticipated to lead to personal successes in the future (Carstensen et al., 2003). Consistent with this literature, empirical evidence suggests that young adults (relative to older adults) are less likely to donate money to a good cause than to keep it for themselves (Freund & Blanchard-Fields, 2014). Further, empirical evidence over the past two decades suggests that college students in the United States tend to score highly on measures of narcissism (Wetzel et al., 2020; Wood et al., 2021). While narcissistic individuals may still engage in prosocial behaviors, they tend to donate or volunteer when others are watching and not when anonymous (Konrath et al., 2016). Hence, we posed (see Carpenter et al., 2021) the following preliminary hypothesis:
H1: A self-f-interest motives is more likely to promote self-monitoring of monitoring prompt that appeals to young adults’ selalcohol use than a prompt that appeals to their prosocial motives.
The Role of Mental Health
Empirical evidence suggests that mental health likely shapes whether and how people respond to different types of self-relevant information. Specifically, research has shown that anxiety, depression, and chronic stress are associated with a heightened focus on the self, which reduces charitable giving (Mor & Winquist, 2002; Pulcu et al., 2015) and altruism (i.e., a motivational state with the ultimate goal to increase the welfare of others; Batson & Powell, 2003). For example, the results of a study with depressed and non-depressed college students suggest that self-preoccupation in depression tends to reduce the salience (or accessibility) of altruistic standards, thus diminishing the likelihood of altruistic behavior (Morris & Kanfer, 1983). A more recent study involving healthy subjects, patients in full remission, and currently depressed patients, found that currently depressed individuals were less altruistic on both a charitable donation and an interpersonal cooperation task (Pulcu et al., 2015). In a number of studies, Batson (2014) found that a lack of helpful, altruistic behavior may be due to personal distress— a form of self-focused worry and discomfort that tends to generate egoistic motivation to reduce one’s own aversive arousal. Further, in a meta-analysis synthesizing 226 effect sizes reflecting the association between negative affect and self-focused attention, Mor and Winquist (2002) found that depression is more strongly associated with private self-focus, which reflects egocentric goals, rather than public self-focus in which the needs, desires, or reactions of others are considered. Indeed studies have found that altruism is associated with better psychological health, including lower levels of stress, anxiety, and depression (Inagaki & Orehek, 2017; Post, 2005). Empirical evidence also suggests that individuals experiencing anxiety, depression, and chronic stress tend to acquire material items as a coping strategy to increase perceived control and restore positive feelings (Darrat et al., 2016; Moschis, 2007). Thus, we hypothesized:
H2a: The effect of a self-monitoring prompt that appeals to young adults’ self-interest (vs. prosocial) motives on self-monitoring of alcohol use is amplified to the extent that young adults report higher baseline depression, anxiety, or stress.
H2b: A self-monitoring prompt that appeals to young adults’ prosocial (vs. self-interest) motives is more likely to promote self-monitoring of alcohol use to the extent that young adults report lower baseline depression, anxiety, or stress.
Present Study
The current study included an incentive system designed to test the potential utility of appeals to young adults’ self-interest versus prosocial motives to promote self-monitoring of alcohol use. Each young adult had four opportunities (i.e., assessment times) to self-monitor their biweekly alcohol use. At each assessment time, if the participant completed the biweekly alcohol use assessment, then they earned $2 and were also entered into one of four $500 drawings. Two of the four drawings were intended for the participant’s preferred item (i.e., self-interest motives), and the other two were intended for donation to their preferred charity (i.e., prosocial motives). Prior to each of up to four assessment times, a prompt to self-monitor was delivered via email. At each time, a participant was randomized (with 0.5 probability) to two types of prompts: (1) a prompt highlighting the opportunity to win their preferred item (Self-Interest Prompt) vs (2) a prompt highlighting the opportunity to donate to their preferred charity (Prosocial Prompt). The proximal outcome is engagement in the subsequent self-monitoring task, operationalized as completion of the alcohol use assessment (see Figure 1).
Figure 1.
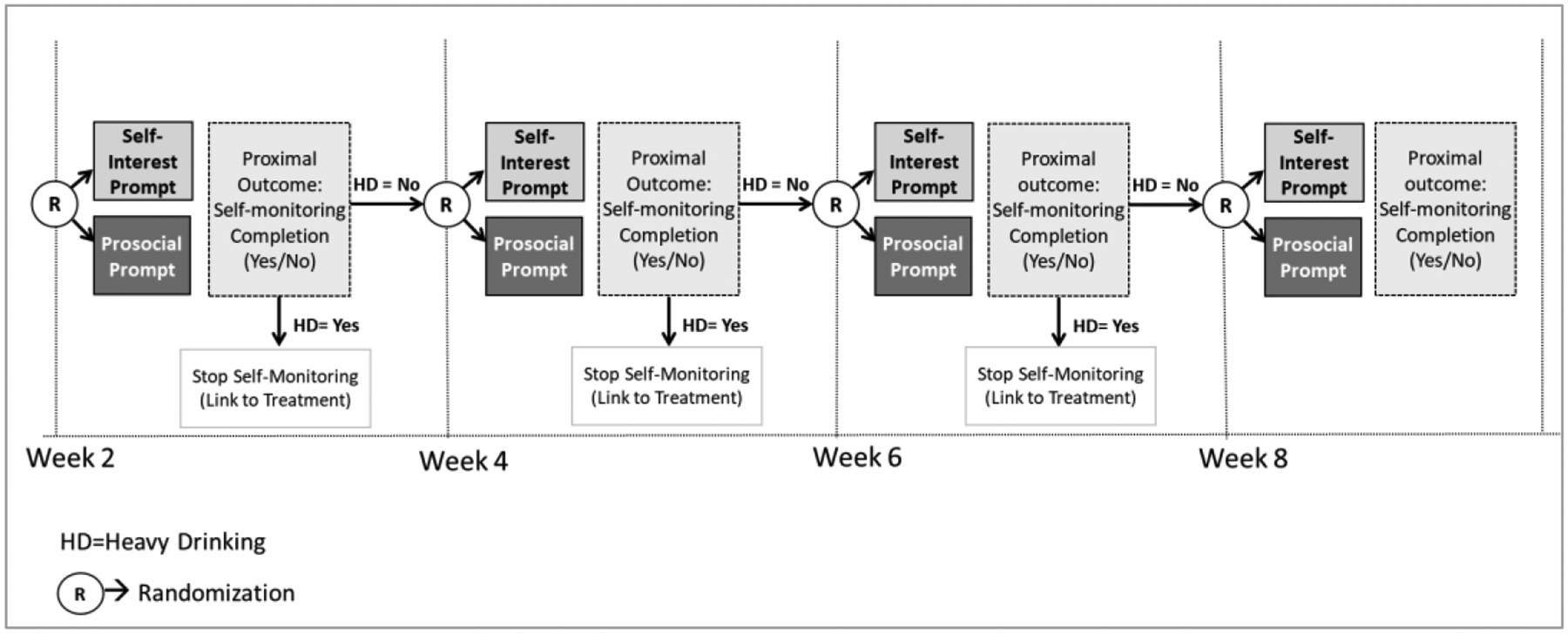
Study Design
Methods
Transparency and Openness
In this article, we report how the sample size was determined based on participant enrollment, and all data exclusions, manipulations, and measures included in the present study. We also follow the JARS (Appelbaum et al., 2018) reporting criteria. The study design and analysis plan were preregistered on the open science framework (osf) website prior to the conduct of analyses (see Carpenter et al., 2021; https://osf.io/dkvz3). The preregistered hypotheses and analyses relate only to the present study. Information about trial data availability and the R analysis code are provided at https://github.com/jamieyap/mbridge-randomized-trial.
Sample
Participants in this study were part of a larger trial to inform the development of an API for reducing binge drinking among undergraduates enrolled as first-year students in a large Midwestern University for the 2019–2020 academic year (N = 891, 62.4% female, 76.8% White; see Patrick et al., 2021 for baseline characteristics). This larger trial involved assigning two-thirds of participants (N=591) to a condition where they were asked to self-monitor their drinking behaviors by completing (up to four) biweekly assessments during their first semester of college (see Patrick et al., 2021 for more details). Those N=591 participants comprised the sample for the current study, which aimed to investigate the utility of different types of self-relevant prompts to encourage self-monitoring of alcohol use. The trial, including the present study, was approved by the University of Minnesota Institutional Review Board.
Procedures
A link to the baseline survey was sent via mail on July 30, 2019, emailed invitations were sent on August 5, 2019, and email reminders were sent on August 10, 2019 and August 15, 2019. Upon navigating to the invitation link, students were asked to fill out a consent form. Those who consented were enrolled in the study and were then immediately directed to an online baseline survey. Participants were also informed that they would be asked to complete biweekly (a total of up to four) self-monitoring assessments. For each completed assessment they would receive $2 (for maximum earnings of $8) as well as have the opportunity to collect points to be entered into four prize drawings. Specifically, at the end of the 4-month period, the names of two participants would be drawn without replacement for each to receive $500 to purchase their preferred item (to appeal to the person’s self-interest motives), and the names of two other participants would be drawn for each to receive $500 to donate to their preferred charity (to appeal to the person’s prosocial motives).
Participants were asked to select a preferred item and a preferred charity, one each from two lists, respectively. Each list was compiled based on informally asking undergraduates currently enrolled at two large Midwestern universities what item they would be most excited to buy and what charitable organization they would be most excited to support. Asking participants to choose their preferred item and charity was intended to increase the likelihood that these selections would meet their personal self-interest and prosocial motives. The preferred item and charity selected by each participant were automatically integrated into the message prompts delivered to them as part of the study (see below).
Participants were also informed that any individual participant could only win one of the four $500 prizes, and that two reward points for these four drawings would be obtained each time they completed the biweekly self-monitoring assessment. At the end of each assessment, participants could choose to allocate (a) two points to the item drawing and no points to the charity drawing; (b) one point to the item drawing and one point to the charity drawing (the default option); and (c) two points to the charity drawing and no points to the item drawing.
Randomizations
A Micro-Randomized Trial (MRT) design (Liao et al., 2016; Qian et al., 2022) was employed to randomize participants biweekly during the first semester (up to a total of 4 times), with a probability 0.5, to two types of prompts: (1) a prompt that encouraged self-monitoring completion by highlighting the opportunity to win a $500 prize that the participant could use to purchase their preferred item (i.e., Self-Interest Prompt); or (2) a message that encouraged self-monitoring completion by highlighting the opportunity to win a $500 prize that the participant could donate to their preferred charity (i.e., Prosocial Prompt). Table 1 includes examples of these two types of prompts. In both conditions, if a participant did not complete the survey within three days, they were sent a reminder through email and text messaging.
Table 1.
Example Self-Relevant Self-Monitoring (SM) Invitation Prompts
| Prize Type | Engagement Message Examples | |
|---|---|---|
| Invitation Message | Follow-up Message | |
| Chosen Charity | Want to make a difference in the world? Complete <<SM link>> to enter into a drawing to win $500 you can donate to the Domestic Abuse Project! You will also receive $2 for completing the check-in. | Think about what you can do for the Domestic Abuse Project! Take the <<SM link >> for a chance to win $500. |
| Chosen Item | Want to get a Smartwatch? Complete <<SM link>> to enter into a drawing to win $500 toward your purchase! You will also receive $2 for completing the check-in. | “Don’t miss out on a Smartwatch! Take the <<SM link>> for a chance to win $500. |
Not all participants were randomized to a prompt at every assessment time. As part of the adaptive preventive intervention, whenever a participant was classified as a heavy drinker based on their self-monitoring assessment, (i) prompts to self-monitor were halted, and (ii) the participant was, instead, sent a link to an indicated intervention (see details in Patrick et al., 2021).
Allocation of Reward Points and Drawings
As described above, at the end of each biweekly self-monitoring assessment, participants received two reward points for allocation to their preferred item and/or charity. After the 4-month study was completed, names were drawn without replacement for the four $500 drawings. The two winners of the $500 item drawing received an award notification reminding them that they planned to use this award to purchase their preferred item. The two winners of the $500 charity drawing received an award notification reminding them that they planned to use this award to donate to their preferred charity.
Measures
Primary Proximal Outcome:
The proximal outcome is whether the participant completed the self-monitoring of alcohol use assessment within three days (i.e., before the delivery of any reminders). Specifically, the alcohol use assessment was considered complete if the participant answered the following item: “Did you have any alcohol (more than a few sips) in the last two weeks?”
Moderators:
All candidate moderators were measured at baseline. Depression was assessed with the 9-item Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001), anxiety was assessed using the 7-item General Anxiety Disorder Questionnaire (GAD-7; Spitzer et al., 1999), and stress was measured with the global measure of perceived stress scale (PSS; Cohen et al., 1983).
Control variables:
All analyses controlled for covariates expected to be highly correlated with self-monitoring, including gender (female vs. others), race (White vs. others), baseline drinking (i.e., the number of drinking days and the quantity of alcohol consumed on those days, in the past 30 days), and time in the study (i.e., number of days since the first micro-randomization).
Analysis Plan
Hypotheses 1–3 were tested using a generalization of regression method developed to ensure unbiased estimates of causal effects of time-varying digital prompts (Boruvka et al., 2017) and extended to accommodate a binary outcome (Bidargaddi et al., 2018; Qian et al., 2021). These analyses pool data across assessment times and participants. Using a log-link function, the causal effect among eligible participants (i.e., who were not classified as heavy drinkers at the prior self-monitoring assessment) is expressed on the “risk-ratio” scale, which measures the probability (“risk”) of self-monitoring completion when a Self-Interest Prompt was delivered, divided by the probability of self-monitoring completion when a Prosocial Prompt was delivered.
Separate analyses were conducted to test the main effect of the two types of prompts on proximal self-monitoring completion (H1) and to investigate the moderating effects of chronic stress, anxiety, and depression (H2a and H2b). In exploratory analyses, we investigated whether the effect of the type of prompt on proximal self-monitoring completion varies (a) over time during the study, and (b) by how participants chose to allocate the two points they received at the prior assessment time.
Results
Sample Characteristics
Out of the 591 participants who were enrolled in the MRT, eight were excluded because they did not select their preferred item or charity at baseline, and two were excluded because they had missing values in one or more of the control variables. Hence, the analysis included a total of 581 participants. Table 2 shows how many participants were randomized at each assessment time during the study. Participants included in the analyses were, on average 18.07 years old (SD = .26); 61% female, and 77% White.
Table 2.
Participants Randomized and Points Allocated at each Assessment Time
| Assessment time | Participants randomized at each assessment time | Point allocation at each assessment time: Total number of participants | Point allocation at each assessment time: % participants | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total number of participants randomized (i.e., eligible) | % Participants eligible | Total number of participants who completed self-monitoring | % Participants who completed self-monitoring out of eligible | Item: 2 Charity: 0 |
Item: 1 Charity: 1 |
Item: 0 Charity: 2 |
Item: 2 Charity: 0 |
Item: 1 Charity: 1 |
Item: 0 Charity: 2 |
|
| 1 | 581 | 100% | 464 | 80% | 215 | 233 | 16 | 46% | 50% | 3% |
| 2 | 490 | 84% | 363 | 74% | 158 | 189 | 16 | 44% | 52% | 4% |
| 3 | 453 | 78% | 294 | 65% | 123 | 156 | 15 | 42% | 53% | 5% |
| 4 | 437 | 75% | 263 | 60% | 116 | 136 | 11 | 44% | 52% | 4% |
Self-Monitoring Completion
Our results (see Table 2) indicate that the rate of self-monitoring completion was relatively high at the beginning of the study, but declined substantially over time. Specifically, the self-monitoring completion rate (out of those eligible at each assessment time) was 80% (464 out of 581 eligible) at the first assessment time, 74% (363 out of 490 eligible) at the second assessment time, 65% (294 out of 453 eligible) at the third assessment time, and 60% (263 out of 437 eligible) at the fourth assessment time.
MRT Results
For the primary hypothesis (H1), the results (Table 3) indicated that individuals, on average, were 1% more likely (Est = exp(.01)=1.01, ns; 95% CI: [0.92, 1.09]) to complete the bi-weekly alcohol use self-monitoring following the Self-Interest (vs. Prosocial) Prompt. However, there was insufficient evidence to reject the null hypothesis that there is no difference between the two types of prompts. Nonetheless, exploratory analyses investigating whether this effect varied over time revealed a significant interaction between the type of prompt and days since the start of the MRT (interaction = −0.01; 95% CI: [−0.01, −0.002]). The results depicted in Figure 2 indicate that at the beginning of the study (first assessment time), individuals were 15% more likely (Est = exp(.14)=1.15; 95% CI: [1.01, 1.29]) to complete the self-monitoring assessment following the Self-Interest (vs. Prosocial) Prompt. However, this effect was reversed toward the end of the study (last assessment time), with participants being (on average) 16% less likely (Est = exp(−.17) = 0.84; 95% CI: [0.70, 0.98]) to complete the self-monitoring assessment following the Self-Interest (vs. Prosocial) Prompt. Overall, while there was no evidence of an effect of prompt type at the second and third assessment times (the 95% CI for this effect include zero at both times), there is evidence in favor of the Self-Interest prompt at the beginning of the self-monitoring period as well as evidence in favor of the prosocial prompt at the end of the self-monitoring period.
Table 3.
Main Effect (H1) and Exploratory Time Trend and Point Allocation Moderation Analyses
| Main Effect (H1)
Analysis1
(N= 581) |
Time Trend Analysis (N= 581) |
Moderators Analysis (N= 373)3 |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Beta | SE (95% CI) | Exp (beta) | Beta | SE (95% CI) | Exp (beta) | Beta | SE (95% CI) | Exp (beta) | ||
| Control Variables2 | Number of drinking days | −.09 | .06 [−.21, .03] |
.91 | −.09 | .07 [−.22, .03] |
.91 | .02 | .05 [−.08, .12] |
1.02 |
| Number of drinks per day | −.03 | .04 [−.10, .05] |
.97 | −.02 | .04 [−.11, .06] |
.98 | −.04 | .04 [−.11, .04] |
0.96 | |
| Race (White=1; Otherwise=0) | .05 | .07 [−.09, .19] |
1.05 | .07 | .08 [−.08, .21] |
1.07 | .13 | .07 [.00, .26] |
1.14 | |
| Gender (Female=1; Otherwise=0) | .05 | .07 [−.08, .18] |
1.05 | .04 | .07 [−.10, .17] |
1.04 | −.03 | .06 [−.14, .09] |
.97 | |
| Number of days (since entering study) | −.01*** | .001 [−.01, .−005] |
.99 | −.002 | .002 [−.01, .002] |
1 | ||||
| Causal Effects | Prompt type (Self-Interest=1; Prosocial=0) | .01 | .04 [−.08, .09] |
1.01 | .14* | .06 [.02, .26] |
1.15 | −.15* | .07 [−.28, −.03] |
0.86 |
| Prompt type * Number of Days | −.01** | .003 [−.01, .−002] |
.99 | |||||||
| Prompt type * Points Allocation (1=Equal; 0= Otherwise) | .21* | .10 [.01, .40] |
1.23 | |||||||
| Prompt type * Points Allocation (1=Entirely to Charity; 0=Otherwise) | .26 | .26 [−.25, .77] |
1.30 | |||||||
p<0.05;
p<0.01;
p<0.001
Note. 95% Confidence Intervals are provided in the square brackets— [lower bound, upper bound].
Hypotheses pre-specified (see open science protocol in Carpenter et al., 2021).
Although estimates for the control variables are provided for completeness, we caution readers against interpreting them since correct specification of this part of the model is not required to yield consistent estimates of the causal effect of prompt type (see Boruvka et al., 2017).
This point allocation moderator analysis is restricted to those who completed prior self-monitoring, and hence received reward points that they were allowed to allocate: n=373 completed the first self-monitoring assessment; n=326 completed the second, and n=278 completed the third. Following self-monitoring completion, all participants made reward points allocations.
Figure 2.
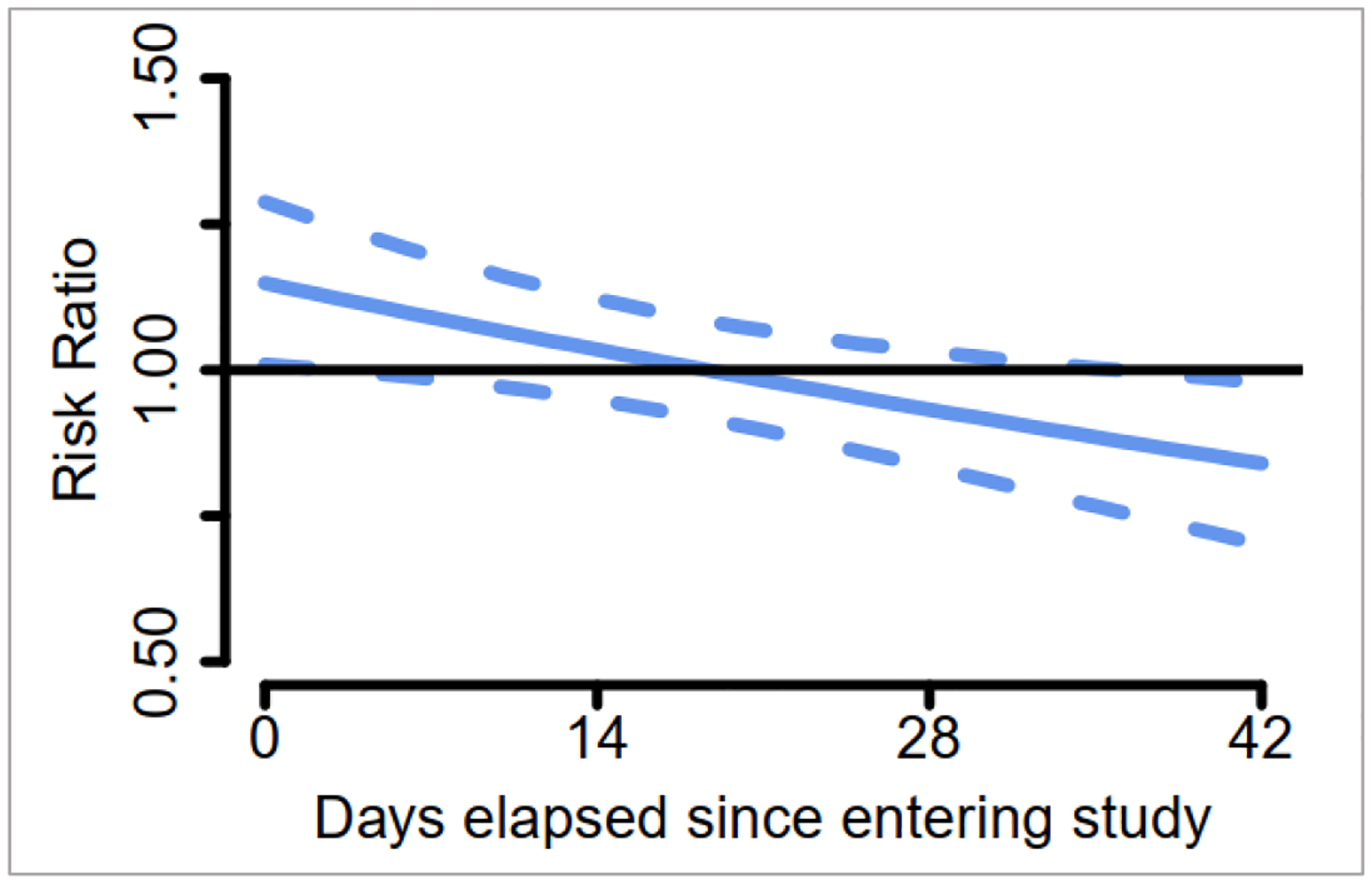
Proximal effect (risk ratio with 95% confidence interval) of self-interest versus prosocial prompt on proximal self-monitoring of alcohol use over the study duration
Regarding the moderation hypotheses (H2a and H2b), the results (Appendix A) indicated that the difference between the two types of prompts in terms of proximal self-monitoring completion did not vary significantly based on baseline anxiety (interaction estimate = −.004, ns; 95% CI: [−.04, .03]), depression (interaction estimate = .02, ns; 95% CI: [−.02, .05]), or chronic stress (interaction estimate = −.005, ns; 95% CI: [−.03, .01]).
Results of the reward point allocation (Table 2) indicated that, in most cases, participants allocated their points equally to the drawings for their preferred item and charity (50%−53%) or entirely to their preferred item (42%−46%). Participants were substantially less likely (3%−5%) to allocate their points entirely to the drawing for their preferred charity. Table 3 summarizes the results of an exploratory analysis investigating whether the allocation of reward points following completion of the previous self-monitoring assessment (time t-1) moderated the effect of current prompt type (time t) on proximal self-monitoring completion. Note that at each randomization point t, this analysis was restricted to eligible participants (i.e., those who were not classified as heavy drinkers based on prior self-monitoring) and those who completed the prior (t-1) self-monitoring and thus received reward points for allocation. The results indicate that the difference between the two types of prompts in terms of proximal self-monitoring completion varied significantly depending on how the participant chose to allocate their reward points. Participants who allocated both points to their preferred item drawing were 14% less likely (Est = exp(−.15)=0.86; 95% CI: [.75, .97]) to complete the next self-monitoring if the prompt focused on the opportunity to win their preferred item (i.e., Self-Interest Prompt) rather than the opportunity to donate to their preferred charity (i.e., Prosocial Prompt). However, there was no significant difference between the two prompt types if the participant allocated their reward points equally (Est = exp(.06)=1.06; 95% CI: [.91, 1.21]) or entirely to the drawing for their charity (Est = exp(.11)=1.11; 95% CI: [.57, 1.66]).
Discussion
This study was designed to investigate the utility of two types of self-relevant prompts in promoting the completion of repeated, digital self-monitoring of alcohol use among young adult college students. These self-relevant prompts were designed to either appeal to the individual’s self-interest motives (by focusing on the opportunity to win a preferred item) or prosocial motives (by focusing on the opportunity to donate to one’s preferred charity). Overall, the results suggest that the incentive system used in the current study successfully leveraged self-relevance to increase the perceived value of self-monitoring in a setting where relatively minimal financial incentives were guaranteed. Recall that many substance use studies that pay between $2 and $5 for daily assessment completion yield average completion rates of less than 65% (Bonar et al., 2018; Dworkin et al., 2017). Further, biweekly and weekly alcohol self-monitoring studies that yield higher completion rates (86%; 70% respectively) combine minimal incentives for self-monitoring completion ($2; $.50 cents, respectively) with either relatively high completion-based bonuses (Barnett et al., 2015) or human support which is costly and complex to implement (Nahum-Shani et al., 2021). It is thus notable that the current study achieved a 70% completion rate on average despite only guaranteeing $2 per completion of each self-monitoring assessment (i.e., up to $8 throughout the study). However, similar to other studies showing a decline over time in digital self-monitoring (Griffin & Patrick, 2015; Krukowski et al., 2013; Turner-McGrievy et al., 2019), the current study found that self-monitoring completion declined from 80% to 60% over eight weeks. This calls for additional research to investigate the utility of other strategies in promoting sustained engagement with self-monitoring.
The results also suggest that a prompt appealing to young adults’ self-interest motives may be more beneficial in promoting engagement at the beginning of the self-monitoring period, whereas a prompt that appeals to their prosocial motives may be more beneficial as young adults approach the end of the self-monitoring period. One explanation for these findings may be grounded in the desire to avoid or minimize anticipated negative emotions such as regret (a negative emotional state experienced when an individual realizes that their present situation would have been better had they acted differently; Zeelenberg, 1999) and/or guilt (a negative emotional state associated with an action that oneself or others may perceive as being “in the wrong” or as a failure to have done something right; Baumeister et al., 1994, p.245; Niedenthal et al., 1994). Specifically, prior empirical evidence suggests that individuals generally seek to avoid regret (see Brewer et al., 2016; Wong & Kwong, 2007) and/or guilt (see Baumeister et al., 2007), often by engaging in prosocial behavior (Lin et al., 2017; Zhang et al., 2021). Feelings of regret and guilt tend to be more intense if the individual attributes the cause of their wrongdoing to controllable factors, such as behaving in a selfish way or failing to do the right thing (Tracy & Robins, 2004; Wilkinson et al., 2015). Hence, it is possible that as participants approached the end of the self-monitoring period, when the drawings would take place, the potential consequences of their prior actions became more salient. This may have led to greater anticipated regret and guilt, which motivated participants to respond more favorably to appeals to their prosocial rather than self-interest motives. There are, however, several alternative explanations to these findings.
One alternative explanation is that unobserved social events (e.g., protests, major sports, or cultural events) that may have occurred at the end of the self-monitoring period caused a spike in altruism that amplified the efficacy of the Prosocial (vs. Self-Interest) prompt. While this explanation implies greater allocation of reward points to charity at the end of the self-monitoring period, the results indicated that allocation of both reward points to charity remains low and constant throughout the self-monitoring period (see Table 2). Specifically, consistently over time, only 3%−5% chose to allocate their reward points entirely to the drawing for their preferred charity, ruling out a possible spike in altruism at the end of the self-monitoring period. Similarly, the rate of allocating reward points equally to the preferred item and charity remained constant throughout the self-monitoring period, ranging from 50%−53%.
Another alternative explanation is that the item chosen at the beginning of the study became less attractive to participants over time (e.g., because students purchased these items on their own during the semester), thereby weakening the appeal of the self-interest prompt. While this explanation implies reduced allocation of reward points to the preferred item over the course of the self-monitoring period, the results show that allocation of both reward points to the item drawing remained relatively high (42%−46%) and constant throughout the study. Moreover, the weakened attractiveness of the item does not explain the observed advantage of the Prosocial Prompt over the Self-Interest Prompt at the end of the self-monitoring period (but rather implies no difference between the two types of prompts).
Yet another alternative explanation is that the composition of participants in the study changed such that participants who remained in the study over time (i.e., those who did not self-report heavy drinking on the bi-weekly self-monitoring) were on average more other-oriented, and thus more likely to value and feel concerned for the well-being of others (Grant & Wrzesniewski, 2010). However, in sensitivity analysis (see Appendix B), results did not change when the sample was restricted to only participants who remained eligible (i.e., did not self-report heavy drinking) throughout the study.
Further, the proposed explanation concerning the role of negative emotions like regret or guilt is also consistent with the observed moderating role of the reward points allocation. These findings indicate that participants were more likely to self-monitor following a Prosocial (vs. Self-Interest) Prompt if they had previously allocated both reward points to drawings for their preferred item. Although the prosocial prompts in the current study were not designed to generate negative emotions, the choice to allocate their prior reward points entirely to their preferred item (i.e., to satisfy their self-interest motives) may have elicited guilt or regret in some individuals. Hence, it is possible that the Prosocial Prompt increased the salience of guilt and regret among those who chose to allocate their prior reward points entirely to the item, motivating self-monitoring completion as a way to reduce these negative feelings (Baumann et al., 1981). While these results highlight the importance of using information about a participant’s prior decisions to tailor the type of self-relevant prompt, future research should specifically investigate how prior interactions with the incentive system shape emotional responses to self-interest versus prosocial appeals to self-monitor.
Finally, the results did not support hypotheses H2a and H2b concerning the moderating role of baseline mental health. The proximal effect of prompt type on self-monitoring likelihood did not vary based on anxiety, depression, or chronic stress. Given the repeated nature of the current self-monitoring task, it is possible that dynamic fluctuations in affect play a more important role (compared to more static baseline constructs) in shaping young adults’ responses to self-interest versus prosocial appeals to self-monitor (Atalay & Meloy, 2011). Future research is needed to investigate whether and how dynamic affective states shape the effect of self-relevant prompts on digital self-monitoring.
Limitations
Although the current investigation offers practical and theoretical implications for research on engagement in digital self-monitoring, several limitations require acknowledgement. First, the current study focused exclusively on college students’ biweekly self-monitoring of alcohol use. Additional research is needed to investigate the extent to which the results can be generalized to other populations of young adults, other kinds of health behaviors (e.g., self-monitoring dietary intake or physical activity), and different self-monitoring frequencies. Second, the present study provided only minimal guaranteed financial incentives (up to $8) for self-monitoring. Since greater financial incentives would result in a costlier and hence less scalable intervention, our goal was to investigate ways to enhance engagement in self-monitoring when relatively minimal financial incentives are offered. Greater financial incentives have the potential to wash out the difference between the two types of digital prompts, by enhancing the value of self-monitoring regardless of the type of prompt delivered. Future research is needed to determine whether the present results are generalizable in settings that offer different financial incentive amounts. Third, the current study relied on emails as the primary modality of message delivery. Using push notifications or text messaging may amplify the effects found in the current study, because these modalities have the potential to more readily capture an individual’s attention in daily life. Future research is needed to determine the impact of utilizing different modalities to deliver self-relevant prompts. Fourth, future studies should systematically investigate whether the results of the current study can be generalized to settings in which no financial incentives are provided for self-monitoring beyond the drawings. This has the potential to further enhance the scalability of interventions that rely on self-monitoring of alcohol use or other health behaviors to tailor treatment. Finally, although sensitivity analysis indicated that the results remain the same when restricting the sample to those who did not report heavy drinking throughout the study, it is possible that the results only apply to those students who did not engage in heavy drinking in the early days of college enrollment. Additional research is needed to investigate the generalizability of the findings to settings in which self-monitoring continues regardless of drinking status.
Conclusion
The results of the current study provide initial support for the utility of self-relevant prompts in promoting digital self-monitoring of alcohol use among college students. These results suggest that the advantage of prompts that appeal to a person’s self-interest versus those that appeal to their prosocial motives varies over time as well as based on what reward options participants prioritized in previous decisions. These results have practical and theoretical implications for engaging young adults in digital self-monitoring of alcohol use and potentially other health behaviors. They also highlight the need for more systematic investigations of theoretically-grounded engagement strategies in digital intervention settings.
Supplementary Material
Public Health Significance:
This study suggests novel ways to encourage college students to self-monitor their alcohol intake in a binge drinking intervention. The advantage of different types of digital reminders in promoting self-monitoring is dynamic and depends on people’s prior decisions.
Acknowledgments
The analysis code for the results reported in this manuscript is available online (https://github.com/jamieyap/mbridge-randomized-trial), and the study design, hypotheses, and analysis plan were preregistered on the open science framework (Carpenter et al., 2021; https://osf.io/dkvz3). The authors have no known conflicts of interest. This study was funded by the following National Institute of Health grants: National Institute on Drug Abuse P50 DA054039 (Nahum-Shani & Almirall), National Cancer Institute U01 CA229437 (Nahum-Shani & Wetter), National Institute on Drug Abuse R01 DA039901 (Nahum-Shani & Almirall), and National Institute on Alcohol Abuse and Alcoholism R01 AA026574 (Patrick).
References
- Aknin LB, Dunn EW, Proulx J, Lok I, & Norton MI (2020). Does spending money on others promote happiness?: A registered replication report. Journal of personality and social psychology, 119(2), e15–e26. [DOI] [PubMed] [Google Scholar]
- Alba JW, & Williams EF (2013). Pleasure principles: A review of research on hedonic consumption. Journal of Consumer Psychology, 23(1), 2–18. [Google Scholar]
- An LC, Perry CL, Lein EB, Klatt C, Farley DM, Bliss RL, Hennrikus DJ, Pallonen UE, Lando HA, & Ahluwalia JS (2006). Strategies for increasing adherence to an online smoking cessation intervention for college students. Nicotine & Tobacco Research, 8(Suppl_1), S7–S12. [DOI] [PubMed] [Google Scholar]
- Appelbaum M, Cooper H, Kline RB, Mayo-Wilson E, Nezu AM, & Rao SM (2018). Journal article reporting standards for quantitative research in psychology: The APA Publications and Communications Board task force report. American Psychologist, 73(1), 3–25. [DOI] [PubMed] [Google Scholar]
- Atalay AS, & Meloy MG (2011). Retail therapy: A strategic effort to improve mood. Psychology & Marketing, 28(6), 638–659. [Google Scholar]
- Barnett NP, Merrill JE, Kahler CW, & Colby SM (2015). Negative evaluations of negative alcohol consequences lead to subsequent reductions in alcohol use. Psychology of Addictive Behaviors, 29(4), 992–1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Batson CD (2014). The altruism question: Toward a social-psychological answer. Psychology Press. [Google Scholar]
- Batson CD, & Powell AA (2003). Altruism and prosocial behavior. In Millon T & Lerner MJ (Eds.), Handbook of psychology: Personality and social psychology (Vol. 5, pp. 463–484). John Wiley & Sons, Inc. [Google Scholar]
- Batson CD, & Shaw LL (1991). Evidence for altruism: Toward a pluralism of prosocial motives. Psychological inquiry, 2(2), 107–122. [Google Scholar]
- Baumann DJ, Cialdini RB, & Kendrick DT (1981). Altruism as hedonism: Helping and self-gratification as equivalent responses. Journal of personality and social psychology, 40(6), 1039–1046. [Google Scholar]
- Baumeister RF, Stillwell AM, & Heatherton TF (1994). Guilt: An interpersonal approach. Psychological bulletin, 115(2), 243–267. [DOI] [PubMed] [Google Scholar]
- Baumeister RF, Vohs KD, DeWall NC, & Zhang L (2007). How emotion shapes behavior: Feedback, anticipation, and reflection, rather than direct causation. Personality and Social Psychology Review, 11(2), 167–203. [DOI] [PubMed] [Google Scholar]
- Bekkers R, & Wiepking P (2011). A literature review of empirical studies of philanthropy: Eight mechanisms that drive charitable giving. Nonprofit and Voluntary Sector Quarterly, 40(5), 924–973. [Google Scholar]
- Bewick BM, West R, Gill J, O’May F, Mulhern B, Barkham M, & Hill AJ (2010). Providing web-based feedback and social norms information to reduce student alcohol intake: a multisite investigation. Journal of medical Internet research, 12(5), e1461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bidargaddi N, Almirall D, Murphy S, Nahum-Shani I, Kovalcik M, Pituch T, Maaieh H, & Strecher V (2018). To prompt or not to prompt? A microrandomized trial of time-varying push notifications to increase proximal engagement with a mobile health app. JMIR mHealth and uHealth, 6(11), e10123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonar EE, Cunningham RM, Collins RL, Cranford JA, Chermack ST, Zimmerman MA, Blow FC, & Walton MA (2018). Feasibility and acceptability of text messaging to assess daily substance use and sexual behaviors among urban emerging adults. Addiction Research & Theory, 26(2), 103–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boruvka A, Almirall D, Witkiewitz K, & Murphy SA (2017). Assessing time-varying causal effect moderation in mobile health. Journal of the American Statistical Association, 113(523), 1112–1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewer NT, DeFrank JT, & Gilkey MB (2016). Anticipated regret and health behavior: A meta-analysis. Health Psychololy, 35(11), 1264–1275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camerer CF, & Hogarth RM (1999). The effects of financial incentives in experiments: A review and capital-labor-production framework. Journal of Risk and Uncertainty, 19(1), 7–42. [Google Scholar]
- Carpenter SM, Patrick ME, Morrell N, & Nahum-Shani I (2021). Leveraging self-relevance to engage young adults in self-monitoring of alcohol use. Open Science Framework. 10.17605/OSF.IO/DKVZ3 [DOI] [Google Scholar]
- Carstensen LL, Fung HH, & Charles ST (2003). Socioemotional selectivity theory and the regulation of emotion in the second half of life. Motivation and Emotion, 27(2), 103–123. [Google Scholar]
- Cohen S, Kamarck T, & Mermelstein R (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. [PubMed] [Google Scholar]
- Collins LM, Murphy SA, & Bierman KL (2004). A conceptual framework for adaptive preventive interventions. Prevention Science, 5(3), 185–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darrat AA, Darrat MA, & Amyx D (2016). How impulse buying influences compulsive buying: The central role of consumer anxiety and escapism. Journal of Retailing and Consumer Services, 31, 103–108. [Google Scholar]
- Dworkin ER, Kaysen D, Bedard-Gilligan M, Rhew IC, & Lee CM (2017). Daily-level associations between PTSD and cannabis use among young sexual minority women. Addictive behaviors, 74, 118–121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein RM, Siegel DJ, & Silberman J (2008). Self‐monitoring in clinical practice: A challenge for medical educators. Journal of Continuing Education in the Health Professions, 28(1), 5–13. [DOI] [PubMed] [Google Scholar]
- Folger R, & Salvador R (2008). Is management theory too “self-ish”? Journal of Management, 34(6), 1127–1151. [Google Scholar]
- Freund AM, & Blanchard-Fields F (2014). Age-related differences in altruism across adulthood: Making personal financial gain versus contributing to the public good. Developmental Psychology, 50(4), 1125–1136. [DOI] [PubMed] [Google Scholar]
- Freund AM, & Riediger M (2001). What I have and what I do: The role of resource loss and gain throughout life. Applied Psychology, 50(3), 370–380. [Google Scholar]
- Garnett C, Crane D, West R, Brown J, & Michie S (2015). Identification of behavior change techniques and engagement strategies to design a smartphone app to reduce alcohol consumption using a formal consensus method. JMIR mHealth and uHealth, 3(2), e3895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gatto AJ, Miyazaki Y, & Cooper LD (2022). Help me help myself: Examining an electronic mental health self-monitoring system in college students. Higher Education, 83, 163–182. [Google Scholar]
- Gneezy U, Meier S, & Rey-Biel P (2011). When and why incentives (don’t) work to modify behavior. Journal of Economic Perspectives, 25(4), 191–210. [Google Scholar]
- Goldstein NJ, Griskevicius V, & Cialdini RB (2011). Reciprocity by proxy: A novel influence strategy for stimulating cooperation. Administrative Science Quarterly, 56(3), 441–473. [Google Scholar]
- Grant AM (2008). Does intrinsic motivation fuel the prosocial fire? Motivational synergy in predicting persistence, performance, and productivity. Journal of Applied Psychology, 93(1), 48–58. [DOI] [PubMed] [Google Scholar]
- Grant AM, & Wrzesniewski A (2010). I won’t let you down… or will I? Core self-evaluations, other-orientation, anticipated guilt and gratitude, and job performance. Journal of Applied Psychology, 95(1), 108–121. [DOI] [PubMed] [Google Scholar]
- Griffin J, & Patrick ME (2015). Understanding participation in a web-based measurement burst design: Response metrics and predictors of participation. Survey Practice, 8(2). [PMC free article] [PubMed] [Google Scholar]
- Hall KL, Nahum-Shani I, August GJ, Patrick ME, Murphy SA, & Almirall D (2019). Adaptive intervention designs in substance use prevention. In Sloboda Z, Petras H, Robertson E, & Hingson R (Eds.), Prevention of substance use (pp. 263–280). Springer. [Google Scholar]
- Hennessy EA, Johnson BT, Acabchuk RL, McCloskey K, & Stewart-James J (2020). Self-regulation mechanisms in health behavior change: a systematic meta-review of meta-analyses, 2006–2017. Health Psychology Review, 14(1), 6–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inagaki TK, & Orehek E (2017). On the benefits of giving social support: When, why, and how support providers gain by caring for others. Current Directions in Psychological Science, 26(2), 109–113. [Google Scholar]
- Klasnja P, Consolvo S, & Pratt W (2011). How to evaluate technologies for health behavior change in HCI research. Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, 3063–3072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- König LM, Allmeta A, Christlein N, Emmenis MV, & Sutton S (2022). A systematic review and meta-analysis of studies of reactivity to digital in-the-moment measurement of health behaviour. Health Psychology Review. [DOI] [PubMed] [Google Scholar]
- Konrath S, Ho M-H, & Zarins S (2016). The strategic helper: Narcissism and prosocial motives and behaviors. Current Psychology, 35(2), 182–194. [Google Scholar]
- Korotitsch WJ, & Nelson-Gray RO (1999). An overview of self-monitoring research in assessment and treatment. Psychological Assessment, 11(4), 415–425. [Google Scholar]
- Kroenke K, Spitzer RL, & Williams JB (2001). The PHQ‐9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krukowski RA, Harvey-Berino J, Bursac Z, Ashikaga T, & West DS (2013). Patterns of success: Online self-monitoring in a web-based behavioral weight control program. Health Psychology, 32(2), 164–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao P, Klasnja P, Tewari A, & Murphy SA (2016). Sample size calculations for micro‐randomized trials in mHealth. Statistics in Medicine, 35(12), 1944–1971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin SC, Zlatev JJ, & Miller DT (2017). Moral traps: When self-serving attributions backfire in prosocial behavior. Journal of Experimental Social Psychology, 70, 198–203. [Google Scholar]
- Merrill JE, & Carey KB (2016). Drinking over the lifespan: Focus on college ages. Alcohol Research: Current Reviews, 38(1), 103–114. [PMC free article] [PubMed] [Google Scholar]
- Michie S, Abraham C, Whittington C, McAteer J, & Gupta S (2009). Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701. [DOI] [PubMed] [Google Scholar]
- Mitchell MS, Goodman JM, Alter DA, John LK, Oh PI, Pakosh MT, & Faulkner GE (2013). Financial incentives for exercise adherence in adults: Systematic review and meta-analysis. American Journal of Preventive Medicine, 45(5), 658–667. [DOI] [PubMed] [Google Scholar]
- Mor N, & Winquist J (2002). Self-focused attention and negative affect: A meta-analysis. Psychological bulletin, 128(4), 638–662. [DOI] [PubMed] [Google Scholar]
- Morris SJ, & Kanfer FH (1983). Altruism and depression. Personality and Social Psychology Bulletin, 9(4), 567–577. [Google Scholar]
- Moschis GP (2007). Stress and consumer behavior. Journal of the Academy of Marketing Science, 35(3), 430–444. [Google Scholar]
- Muir CP, Sherf EN, & Liu JT (2021). It’s not only what you do, but why you do it: How managerial motives influence employees’ fairness judgments. Journal of Applied Psychology, Advance online publication. [DOI] [PubMed] [Google Scholar]
- Nahum-Shani I, Rabbi M, Yap J, Philyaw-Kotov ML, Klasnja P, Bonar EE, Cunningham RM, Murphy SA, & Walton MA (2021). Translating strategies for promoting engagement in mobile health: A proof-of-concept microrandomized trial. Health Psychology, 40(12), 974–987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nahum-Shani I, Shaw SD, Carpenter SM, Murphy SA, & Yoon C (2022). Engagement in digital interventions. American Psychologist, Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. (2019). College AIM Alcohol intervention matrix: Individual-level strategies. National Institutes of Health. https://www.collegedrinkingprevention.gov/CollegeAIM/IndividualStrategies/default.aspx [Google Scholar]
- Nelson RO, & Hayes SC (1981). Theoretical explanations for reactivity in self-monitoring. Behavior Modification, 5(1), 3–14. [Google Scholar]
- Niedenthal PM, Tangney JP, & Gavanski I (1994). “If only I weren’t” versus “If only I hadn’t”: Distinguishing shame and guilt in counterfactual thinking. Journal of personality and social psychology, 67(4), 585–595. [DOI] [PubMed] [Google Scholar]
- O’Reilly CA, & Chatman J (1986). Organizational commitment and psychological attachment: The effects of compliance, identification, and internalization on prosocial behavior. Journal of Applied Psychology, 71(3), 492–499. [Google Scholar]
- Patel ML, Wakayama LN, & Bennett GG (2021). Self‐monitoring via digital health in weight loss interventions: A systematic review among adults with overweight or obesity. Obesity, 29(3), 478–499. [DOI] [PubMed] [Google Scholar]
- Patrick ME, Boatman JA, Morrell N, Wagner AC, Lyden GR, Nahum-Shani I, King CA, Bonar EE, Lee CM, Larimer ME, Vock DM, & Almirall D (2020). A sequential multiple assignment randomized trial (SMART) protocol for empirically developing an adaptive preventive intervention for college student drinking reduction. Contemporary Clinical Trials, 96, 106089. 10.1016/j.cct.2020.106089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick ME, Lyden GR, Morrell N, Mehus CJ, Gunlicks-Stoessel M, Lee CM, King CA, Bonar EE, Nahum-Shani I, Almirall D, Larimer ME, & Vock DM (2021). Main outcomes of M-bridge: A sequential multiple assignment randomized trial (SMART) for developing an adaptive preventive intervention for college drinking. Journal of consulting and clinical psychology, 89(7), 601–614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Post SG (2005). Altruism, happiness, and health: It’s good to be good. International Journal of Behavioral Medicine, 12(2), 66–77. [DOI] [PubMed] [Google Scholar]
- Pulcu E, Thomas E, Trotter P, McFarquhar M, Juhász G, Sahakian B, Deakin J, Anderson I, Zahn R, & Elliott R (2015). Social-economical decision making in current and remitted major depression. Psychological Medicine, 45(6), 1301–1313. [DOI] [PubMed] [Google Scholar]
- Qian T, Walton A, Collins LM, Klasnja P, Lanza ST, Nahum-Shani I, Rabbi M, Russell MA, Waltom M, Yoo H, & Murphy SA (2022). The micro-randomized trial for developing digital interventions: Experimental design and data analysis considerations. Psychological Methods, Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qian T, Yoo H, Klasnja P, Almirall D, & Murphy SA (2021). Estimating time-varying causal excursion effects in mobile health with binary outcomes. Biometrika, 108(3), 507–527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabbi M, Kotov MP, Cunningham R, Bonar EE, Nahum-Shani I, Klasnja P, Walton M, & Murphy S (2018). Toward increasing engagement in substance use data collection: Development of the Substance Abuse Research Assistant app and protocol for a microrandomized trial using adolescents and emerging adults. JMIR research protocols, 7(7), e166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulenberg JE, Patrick ME, Johnston LD, O’Malley PM, Bachman JG, & Miech RA (2020). Monitoring the future national survey results on drug use, 1975–2020: Volume II, College students and adults ages 19–60. (Ann Arbor: Institute for Social Research, The University of Michigan; ). [Google Scholar]
- Short C, Rebar A, Plotnikoff R, & Vandelanotte C (2015). Designing engaging online behaviour change interventions: A proposed model of user engagement. The European Health Psychologist, 17(1), 32–38. [Google Scholar]
- Simpson TL, Kivlahan DR, Bush KR, & McFall ME (2005). Telephone self-monitoring among alcohol use disorder patients in early recovery: A randomized study of feasibility and measurement reactivity. Drug and alcohol dependence, 79(2), 241–250. [DOI] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB, & Patient Health Questionnaire Primary Care Study Group. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA, 282(18), 1737–1744. [DOI] [PubMed] [Google Scholar]
- Tracy JL, & Robins RW (2004). Putting the self into self-conscious emotions: A theoretical model. Psychological inquiry, 15(2), 103–125. [Google Scholar]
- Turner-McGrievy GM, Dunn CG, Wilcox S, Boutté AK, Hutto B, Hoover A, & Muth E (2019). Defining adherence to mobile dietary self-monitoring and assessing tracking over time: Tracking at least two eating occasions per day is best marker of adherence within two different mobile health randomized weight loss interventions. Journal of the Academy of Nutrition and Dietetics, 119(9), 1516–1524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vansteenkiste M, Aelterman N, De Muynck G-J, Haerens L, Patall E, & Reeve J (2018). Fostering personal meaning and self-relevance: A self-determination theory perspective on internalization. The Journal of Experimental Education, 86(1), 30–49. [Google Scholar]
- Wetzel E, Grijalva E, Robins RW, & Roberts BW (2020). You’re still so vain: Changes in narcissism from young adulthood to middle age. Journal of personality and social psychology, 119(2), 479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson MR, Ball LJ, & Alford D (2015). Counterfactual reasoning for regretted situations involving controllable versus uncontrollable events: The modulating role of contingent self-esteem. Advances in Cognitive Psychology, 11(1), 22–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong KFE, & Kwong JY (2007). The role of anticipated regret in escalation of commitment. Journal of Applied Psychology, 92(2), 545–554. [DOI] [PubMed] [Google Scholar]
- Wood AD, Borja K, & Hoke L (2021). Narcissism for Fun and Profit: An Empirical Examination of Narcissism and Its Determinants in a Sample of Generation Z Business College Students. Journal of Management Education, 45(6), 916–952. [Google Scholar]
- Zeelenberg M (1999). Anticipated regret, expected feedback and behavioral decision making. Journal of Behavioral Decision Making, 12(2), 93–106. [Google Scholar]
- Zhang X, Zeelenberg M, & Breugelmans SM (2021). Anticipated guilt and going against one’s self-interest. Emotion, 21(7), 1417–1426. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.