

Abstract
We report a patient who developed frosted branch angiitis (FBA) and was diagnosed 1 month after the penetrating eye injury (PEI) repair. A 31-year-old male with no systemic comorbidities presented with defective vision following trauma to his left eye while cutting wood. His best-corrected visual acuity (BCVA) was 20/200. Anterior segment examinations showed a zone I full-thickness corneal tear with iris tissue incarceration. There was no clinical evidence of intraocular foreign body (IOFB) or endophthalmitis. He underwent PEI repair with iris abscission on the same day with intracameral moxifloxacin injection. His BCVA on postoperative day 45 was 20/200. Examination showed a resolving vitreous hemorrhage, venous tortuosity, and retinal perivascular infiltration affecting the venules from the posterior pole up to the periphery. He was treated with oral and topical steroids. The clinical signs resolved completely and BCVA improved to 20/20 after 1 month of treatment. FBA can complicate the recovery of eyes after PEI repair, even in the absence of endophthalmitis or sympathetic ophthalmia. A thorough search for IOFB or its tell-tale signs should be done in such eyes.
Keywords: Frosted branch angiitis, open globe injury, penetrating eye injury, repair, trauma
Introduction
Frosted branch angiitis (FBA) is an immune-mediated disorder of the retinal vasculature.[1] It was first described by Ito et al. in a 6-year-old boy. Its appearance has a striking resemblance to the ice-covered branches of a tree in winters.[1] It can either be idiopathic or occur secondary to infective, inflammatory, and neoplastic systemic diseases. However, it has rarely been reported secondary to ocular trauma.[2,3,4,5]
We report a patient who developed diffuse FBA, which was diagnosed 1 month after the penetrating eye injury (PEI) repair.
Case Report
A 31-year-old male with no systemic comorbidities presented few hours after trauma to his left eye while cutting wood. His best-corrected visual acuity (BCVA) was 20/20 in the right eye and 20/200 in the left eye. Anterior segment examinations of the left eye showed a 2 mm full-thickness, horizontal, linear corneal tear at 2 o'clock position in zone I; iris tissue incarcerated in the tear; an iridodialysis from 10 to 5 o'clock; and a clear crystalline lens. The posterior segment could not be evaluated due to the presence of vitreous hemorrhage (VH). B-scan ultrasonography showed no evidence of intraocular foreign body (IOFB), retinal detachment (RD), or choroidal detachment (CD). Orbital X-ray showed no evidence of metallic IOFB. Examination of the right eye was normal. He underwent corneal tear repair with iris abscission and an intracameral 0.5% moxifloxacin injection on the same day. He was advised oral ciprofloxacin 500 mg two times a day (BD) for 5 days and topical ofloxacin (0.3%) four times a day (QID), homatropine hydrobromide (2.0%) BD, and prednisolone acetate (1.0%) QID eyes drops. The topical medications were tapered over the next 6 weeks.
On the first postoperative day (POD), his BCVA was 20/200. Ocular examinations showed an exaggerated anterior segment inflammatory reaction. However, the patient did not complain of pain, limbus-to-limbus corneal edema was absent, and the intraocular pressure (IOP) was digitally normal. He received a single dose of an intramuscular dexamethasone sodium phosphate injection (8 mg/2 mL). His BCVA failed to improve even 1 week later. The anterior segment examinations showed a well-apposed corneal wound with no suture infiltrates; a reduced inflammatory reaction; a sectoral iridectomy from 10 to 4 o'clock; an iridodialysis from 4 to 5 o'clock; and a clear crystalline lens [Figure 1]. The central fundus could not be seen due to the presence of VH, while no pathology was noted in the peripheral retina. B-scan ultrasonography showed no evidence of RD or CD. He was advised weekly follow-up. The patient did not show any signs or symptoms of endophthalmitis or infection during any of the follow-up visits. A dilated fundus examination was performed at every visit; however, the central fundus could not be examined due to the presence of VH.
Figure 1.
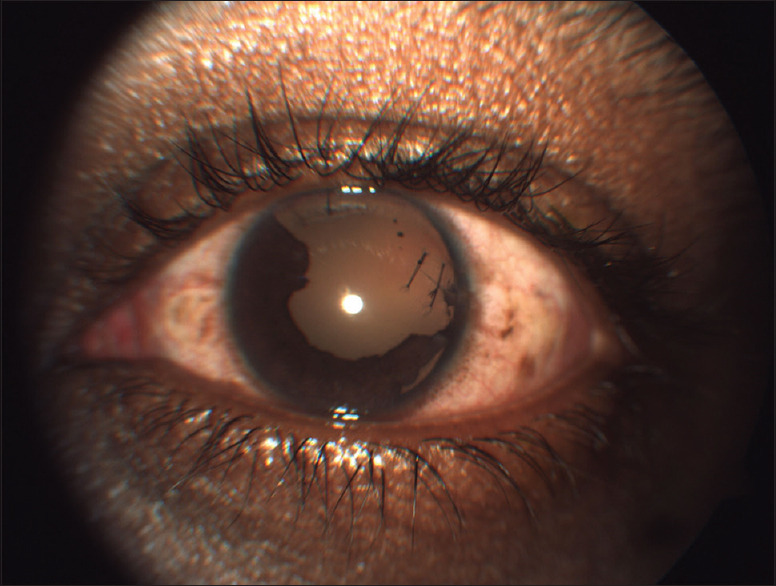
Clinical image of the left eye on postoperative day 15, showing a well-apposed corneal wound, a sectoral iridectomy from 10 to 4 o’clock, an iridodialysis from 4 to 5 o’clock, and a clear crystalline lens
On POD 45, BCVA was 20/20 in the right eye and 20/200 in the left eye. Examinations of the right eye did not reveal any evidence of anterior or posterior inflammation. Anterior segment examinations of the left eye showed no signs of inflammation. The fundus view became relatively clearer as the VH had started to resolve. Posterior segment examination showed normal optic disc, venous tortuosity, and translucent retinal perivascular infiltration affecting the venules from the posterior pole up to the periphery [Figure 2a]. Fundus fluorescein angiography showed normal arm-to-retina and arteriovenous transit time; leakage from the affected vessels and corresponding late vessel staining; and peripheral capillary nonperfusion areas [Figure 2b-d]. Optical coherence tomography (OCT) showed absence of macular edema.
Figure 2.
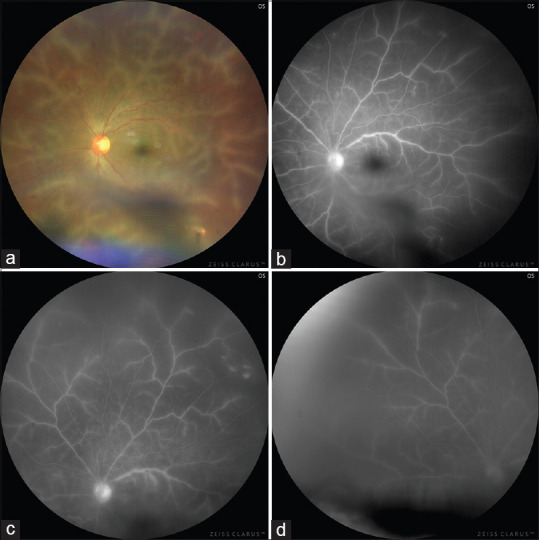
Left eye on post-operative day 45. (a) Ultra-wide field image (Clarus 500, Zeiss, Carl Zeiss Meditech Inc., Dublin, USA) showing resolving vitreous hemorrhage, a normal optic disc, venous tortuosity, and translucent retinal perivascular infiltration affecting the venules from the posterior pole up to the periphery. (b-d) Fundus fluorescein angiography showing leakage of the affected vessels, late vessel staining, and peripheral capillary nonperfusion areas
Blood workup for autoimmune markers such as complete blood count, erythrocyte sedimentation rate, rheumatoid factor, antinuclear antibodies, antineutrophil cytoplasmic antibodies, and angiotensin-converting enzyme was negative. Serology for infectious causes such as hepatitis B and C, human immunodeficiency virus, syphilis, herpes simplex virus, varicella-zoster virus, cytomegalovirus, and toxoplasma was also negative. The Mantoux test did not show significant induration. Chest X-ray did not show any consolidation or lymphadenopathy.
The patient was diagnosed with left eye FBA probably secondary to PEI. He was treated with oral prednisolone (1 mg/kg) and topical steroid (prednisolone acetate, 1.0%) and cycloplegics (homatropine hydrobromide, 2.0%) drops. The perivascular sheathing reduced and BCVA improved to 20/80 after 1 week of treatment. The clinical signs resolved completely and his BCVA improved to 20/20 after 1 month of treatment [Figure 3a]. The media clarity improved as the VH continued to resolve and a linear chorioretinal scar measuring around one disc diameter was noted along one of the vessels in the midperiphery of the inferotemporal quadrant [Figure 3b and c]. OCT showed absence of macular edema. The oral and topical treatments were slowly tapered. There was no recurrence of the disease till the last follow-up, i.e., 4 months, after the treatment was stopped.
Figure 3.

Ultra-wide field image (Clarus 500, Zeiss, Carl Zeiss Meditech Inc., Dublin, USA) of the left eye showing resolving vitreous hemorrhage and the perivascular infiltration, and a linear chorioretinal scar measuring around one disc diameter along one of the vessels in the midperiphery of the inferotemporal quadrant at (a) 1 month, (b) 2 months, and (c) 3 months after the start of treatment
Discussion
FBA is a bilateral, nonocclusive vasculitis with female preponderance and bimodal age distribution.[1] The perivascular sheathing occurs due to vascular exudation and immune-complex deposition in response to various antigens. It has been reported in association with ocular diseases such as viral retinitis and toxoplasmosis and systemic diseases such as sarcoidosis, multiple sclerosis, Behçet's disease, antiphospholipid antibody disease, lymphoma, and Crohn's disease.[1]
We presented a patient who developed a diffuse FBA-like picture, which was diagnosed 6 weeks after the initial PEI repair. We evaluated the patient for the various possible causes responsible for the development of FBA. The presence of associated systemic disease (s) was carefully ruled out with the help of a thorough systemic workup. There was no clinical evidence of endophthalmitis either at presentation or during the follow-up course. Hence, culture from the corneal wound, aqueous or vitreous, was not taken. However, the patient received a prophylactic intracameral moxifloxacin injection during the initial repair. Several authors have reported the development of toxic anterior segment syndrome secondary to intracameral moxifloxacin.[6,7,8,9,10] However, FBA has never been reported following the use of this antibiotic. The repaired eye showed an exaggerated anterior segment inflammatory reaction on the first POD. However, it was not associated with pain, elevated IOP, or limbus-to-limbus corneal edema. The exaggerated inflammation may be attributed to disruption of the blood-aqueous barrier secondary to the PEI and the surgery, especially iris abscission. The peculiar chorioretinal scar in the inferotemporal quadrant may be a tell-tail sign of a tiny wooden IOFB, which got incarcerated in the deep retina at the time of the trauma. An incarcerated wooden IOFB is unlikely to be imaged on either X-ray or B-scan ultrasonography as it is neither radiopaque nor is its reflectivity different from that of the retina. We believe that the increased vascular permeability occurred due to a combination of immunological response to the antigens released secondary to iris abscission and/or the foreign antigens introduced during the wooden stick injury, the resultant VH, blood–retinal barrier (BRB) disruption, and consequent intraocular inflammation. The timing of the development of FBA remains debatable. We believe that the disease may have developed earlier, but the presence of VH and poor media clarity delayed its recognition. However, the absence of complications such as macular edema, macular scarring, and retinal fibrosis along with a good visual outcome suggests that the disease may not have been very long standing.
Kahloun et al. reported a localized FBA-like picture in a 14-year-old child 1 day after closed-globe injury. They proposed that hypersensitivity response against self-antigens released due to ocular trauma may have led to the deposition of immune complexes.[3] Arend and Thurau reported pseudoarteritis in a 58-year-old patient who suffered from trauma 4 months ago. They proposed that the degradation products released from the endothelium cells may be responsible for the formation of the “frost” along the arteries.[4] Madanagopalan et al. reported a localized FBA-like picture in a 54-year-old male who suffered a PEI with a metallic IOFB. Since the clinical picture resolved after vitrectomy, they believed that the retained IOFB may have triggered the development of FBA. The authors proposed that post-trauma FBA can develop secondary to VH, the introduction of proteins such as plasma kallikrein in the vitreous, and breakdown of BRB.[2,11] Annamalai and Biswas reported FBA-like features in an eye that developed sympathetic ophthalmia 8 months after PEI in the contralateral eye.[5] FBA has also been reported secondary to endophthalmitis caused by intravenous drug abuse and intravitreal injection.[12,13] After a detailed examination, we did not find any evidence of IOFB, endophthalmitis, or sympathetic ophthalmia in our case. However, the presence of a wooden FB incarcerated in the deep retina cannot be completely ruled out.
The prognosis in eyes with FBA is usually variable. It may be complicated by macular scarring, retinal fibrosis, epiretinal membrane, retinal vascular occlusion, retinal tear, and/or optic atrophy.[1] The prognosis of the patients who developed FBA after ocular trauma has been poor in most of the reported cases.[2,3,4] However, our patient regained complete vision.
FBA can rarely complicate the recovery of eyes after PEI repair, even in the absence of endophthalmitis, IOFB, or sympathetic ophthalmia. FBA should be suspected if the visual acuity remains poor despite improvement in media clarity. A thorough search for IOFB or its tell-tale signs should be done in such eyes. Early recognition and timely management can lead to a good outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. The patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initial will not be published and that efforts will be made to conceal identity.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare that there are no conflicts of interests in this paper.
References
- 1.Walker S, Iguchi A, Jones NP. Frosted branch angiitis: A review. Eye (Lond) 2004;18:527–33. doi: 10.1038/sj.eye.6700712. [DOI] [PubMed] [Google Scholar]
- 2.Madanagopalan VG, Nagesha CK, Velis G, Devulapally S, Balamurugan S. Frosted branch angiitis with penetrating ocular trauma and retained intraocular foreign body. Indian J Ophthalmol. 2018;66:1031–3. doi: 10.4103/ijo.IJO_1276_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kahloun R, Abroug N, Ammari W, Mahmoud A, Jelliti B, Ben Yahia S, et al. Acute retinal periphlebitis mimicking frosted branch angiitis associated with exudative retinal detachment after blunt eye trauma. Int Ophthalmol. 2014;34:1149–51. doi: 10.1007/s10792-014-9958-0. [DOI] [PubMed] [Google Scholar]
- 4.Arend N, Thurau S. Unilateral retinal pseudoarteritis after eyeball contusion. Ophthalmologe. 2012;109:1214–6. doi: 10.1007/s00347-012-2598-8. [DOI] [PubMed] [Google Scholar]
- 5.Annamalai R, Biswas J. Sympathetic ophthalmia presenting with signs of frosted branch angiitis: Report of a case. Oman J Ophthalmol. 2018;11:49–51. doi: 10.4103/ojo.OJO_99_2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sánchez-Sánchez C, Puerto B, López-Caballero C, Contreras I. Unilateral acute iris depigmentation and transillumination after glaucoma surgery with mitomycin application and intracameral moxifloxacin. Am J Ophthalmol Case Rep. 2020;18:100639. doi: 10.1016/j.ajoc.2020.100639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zubicoa A, Echeverria-Palacios M, Mozo Cuadrado M, Compains Silva E. Unilateral acute iris transillumination-like syndrome following intracameral moxifloxacin injection. Ocul Immunol Inflamm. 2020:1–2. doi: 10.1080/09273948.2020.1817495. [DOI] [PubMed] [Google Scholar]
- 8.Peñaranda-Henao M, Reyes-Guanes J, Muñoz-Ortiz J, Gutiérrez ÁM, De-La-Torre A. Anterior uveitis due to intracameral moxifloxacin: A case report. Ocul Immunol Inflamm. 2020:1–4. doi: 10.1080/09273948.2020.1757120. [DOI] [PubMed] [Google Scholar]
- 9.Gonul S, Bakbak B. Anterior uveitis due to intracameral moxifloxacin: A case report. Ocul Immunol Inflamm. 2020:1–2. doi: 10.1080/09273948.2020.1797118. [DOI] [PubMed] [Google Scholar]
- 10.Amireskandari A, Bean A, Mauger T. Toxic anterior segment syndrome with intracameral moxifloxacin: Case report and review of the literature. Case Rep Ophthalmol Med. 2021;2021:5526097. doi: 10.1155/2021/5526097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liu J, Clermont AC, Gao BB, Feener EP. Intraocular hemorrhage causes retinal vascular dysfunction via plasma kallikrein. Invest Ophthalmol Vis Sci. 2013;54:1086–94. doi: 10.1167/iovs.12-10537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gensure RH, Hsu J, Federman J, Park C, Spirn MJ. Coagulase-negative staphylococcus-induced frosted branch angiitis after intravitreal anti-vascular endothelial growth factor injection. Retin Cases Brief Rep. 2017;11:60–2. doi: 10.1097/ICB.0000000000000288. [DOI] [PubMed] [Google Scholar]
- 13.Gabriele P, Hutchins RK. Fusarium endophthalmitis in an intravenous drug abuser. Am J Ophthalmol. 1996;122:119–21. doi: 10.1016/s0002-9394(14)71976-2. [DOI] [PubMed] [Google Scholar]