

Abstract
While radiologists are familiar with the masticator space, the surgeons are more familiar with the infratemporal fossa (ITF). Though often used interchangeably, there exists a subtle difference between them, which needs to be understood. The close anatomical relationship of the infratemporal fossa to critical structures makes timely diagnosis vital. In this pictorial review, we present a spectrum of various pathologies affecting ITF.
Keywords: Infratemporal Fossa, Anatomy, Pathologies, Computed Tomography
Introduction
Infratemporal fossa (ITF) is an extremely important landmark in head and neck imaging that needs to be evaluated carefully since it communicates with several surrounding regions. A variety of infections, inflammation, and neoplasms such as an oral cavity, nasopharyngeal cancers, and lymphoma can involve it. It can also be involved in lesions of the skull base. Therefore, familiarity with the anatomy and boundaries is important to improve diagnostic accuracy as well as in surgical management. The primary role of cross-sectional imaging in evaluating ITF is in the pre-operative assessment of the extent of disease and determining its relation to vital neurovascular structures. This article aims to illustrate and acquaint the reader with imaging anatomy, boundaries, and some major pathological conditions affecting ITF.
Anatomy
ITF is a quadrangular shaped structure situated deep to masseter muscle and zygomatic arch. The boundaries of ITF are as follows (Fig. 1):
Laterally: ramus of mandible along with the coronoid and condylar process
Medially: lateral pterygoid plate and pharyngeal mucosal space
Anteriorly: posterior border of the maxillary sinus
Posteriorly: mastoid temporal bone
Roof: greater wing of the sphenoid
Fig. 1.

Anatomy of infratemporal fossa. Axial (A) and coronal (B) CT sections show outline of the infratemporal fossa (yellow) and masticator space (purple)
The inferior limit is soft tissue; hence, any space-occupying lesion can easily extend in the inferior direction[1].
The fossa communicates with the pterygopalatine fossa (PPF) via the pterygomaxillary fissure (PMF), with the middle cranial fossa (MCF) through the foramen ovale and spinosum, and via the inferior orbital fissure with the orbit. The temporal fossa communicates directly with the ITF.
Contents
The contents of infratemporal fossa are as follows:
Muscles: medial and lateral pterygoids and insertion of the temporalis muscle.
Nerves: mandibular division of trigeminal nerve, chorda tympani branch of the facial nerve, and otic parasympathetic ganglion
Vessels: maxillary artery and branches of pterygoid vein plexus
The non-fascia lined ITF thus contains a major portion of masticator space, PPS, and retroantral buccal space [2]. Masseter muscle is not a content of ITF.
Clinical and Surgical Importance of Infratemporal Fossa
The diseases involving ITF tend to spread to other adjacent regions and vice versa. They can also spread to inferior parapharyngeal space as well as intracranially involving cavernous sinus. ITF acts as a crossroad for many neurovascular structures traversing to and from the brain. Hence, malignancies in this location usually present with numerous surgical challenges due to the involvement of the skull base and extensive perineural spread[3]. Traditionally, cT4b tumors of buccal mucosa have been called unresectable in 6th edition of AJCC; however, the current 7th edition of AJCC reclassifies it as advanced disease. The reason being that many cases of masticator space involvement may be amenable for resection.
Mandibular notch is used as a demarcation line to classify the disease as supranotch and infranotch (Fig. 2), with the supranotch disease being associated with the worst clinical outcomes. The supranotch compartment includes the lateral pterygoid muscles, tendon of temporalis, and upper 2/3rd of pterygoid plates. The infranotch compartment includes the bulk of the masseter, medial pterygoid muscle, and lower part of the pterygoid plates. A clear understanding of the complex anatomy of ITF is essential to prevent surgical complications such as iatrogenic vascular injury, facial nerve injury, and temporomandibular joint abnormalities.
Fig. 2.
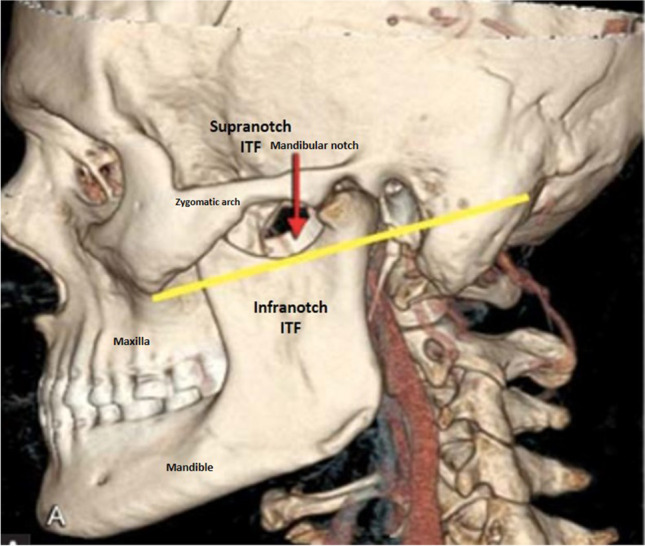
CT volume rendered technique reconstruction image showing mandibular notch as a demarcation line to classify as supranotch and infranotch compartment of ITF
Pathologies Affecting Infratemporal Fossa
Infections
Infections in ITF usually spread from contiguous spaces. Common sources of infection here are maxillary sinus, peritonsillar space, submandibular space, and masticator space (dental origin)[4]. The venous drainage of ITF is by pterygoid venous plexus which communicates with the cavernous sinus; hence, infections here can extent into the orbit and middle cranial fossa. Fungal infections of paranasal sinuses (acute invasive fungal sinusitis, AIFS) can affect the ITF via the pteryomaxillary fissure (Fig. 3). The role of imaging is to define the extent of involvement, intracranial, or intraorbital extension and also to evaluate for complications like cavernous sinus thrombosis and pseudoaneurysm formation[5]. With the involvement of the ITF, surgical debridement is often challenging.
Fig. 3.

CECT of paranasal sinuses of 36-year-old COVID patient with invasive fungal sinusitis. CECT axial (A) and coronal (B) reformatted images show soft tissue mucosal thickening in bilateral maxillary sinuses with extension into the infratemporal fossa via pterygopalatine fissure
Neoplasms
Primary tumors are relatively rare in the infratemporal fossa. Most of the lesions are a direct extension of masses from adjoining structures. Direct invasion of ITF is seen in tumors of nasophraynx, oral malignancies, paranasal sinuses, etc.
Benign Tumors
Juvenile Nasal Angiofibroma
Juvenile nasal angiofibromas are benign, but locally invasive vascular tumors of the nasopharynx occurring exclusively in adolescent boys. On imaging, JNAs appear as soft tissue mass epicentered in the region of the sphenopalatine fossa which is often widened. Post-contrast images show intense enhancement with multiple areas of flow voids indicating its highly vascular stroma. The extrapharyngeal extension is not uncommon and occurs due to spread along the pterygopalatine fissure to the infratemporal fossa (Fig. 4). The high vascularity of tumor contradicts biopsy and preoperative embolisation is necessary.
Fig. 4.

CE-MRI of a 17-year-old male with juvenile nasal angiofibroma. Post-contrast T1 fat sat images reveal an avidly enhancing mass in the bilateral nasal cavity extending into the right infratemporal fossa with widened pterygomaxillary fissure
Neurogenic Tumors
Nerve sheath tumors are known to occur commonly in the infratemporal fossa and are usually benign, though malignant tumors also have been reported. When located in the infratemporal fossa, extension into the intracranial compartment is also not uncommon. On MRI imaging, they are isointense to hypointense on T1W images and their appearance on T2 weighted images depending on the cellularity, presence of hemorrhage, and amount of degeneration (Fig. 5). On post-contrast images, it shows enhancement with sharp demarcation from the surrounding structures due to capsule formation.
Fig. 5.

MRI of a 43-year- old male of trigeminal schwannoma. Axial T2-weighted images (A) show solid cystic lesion involving the right infratemporal fossa showing heterogenous enhancement on post-contrast images (B). It is involving posterolateral wall of maxillary wall
Rosai Dorfman Disease
Rosal Dorfman disease (sinus histiocytosis with massive lymphadenopathy) is a rare benign histiocytic disorder of unknown etiology. It classically presents with bilateral painless cervical lymphadenopathy. Extranodal involvement also occurs frequently in the head and neck region, the common sits being the paranasal sinuses, nasopharynx, infratemporal fossa, orbits, etc. (Fig. 6)[6].
Fig. 6.

CT images of a 45-year-old male patient of Rosai Dorfman disease. CT images show soft tissue mass in the right infratemporal fossa (A) as well as intraorbital, extraconal mass in left orbit (B)
Desmoid
Desmoid or fibromatosis is a benign but locally aggressive tumor with a high recurrence rate post-surgery. The most common sites include the abdomen, limbs, shoulder, and pelvic muscles. Only 5% of the desmoids occur in the head and neck region.[7] Desmoids in ITF usually present as painless trismus. On CT, most desmoids are well-circumscribed masses, while few may appear locally aggressive with ill-defined margins.
Malignant Lesions
Oral Cavity Malignancy
Oral cavity malignancy can arise from buccal mucosa, lips, the floor of mouth, tongue, palate, or the retromolar trigone. Squamous cell carcinoma of the buccal mucosa is one of the most common forms of oral cancer in India[8]. Most commonly, these patients are in their 4–6th decade with a history of betel chewing, smoking, or alcohol consumption. It is more commonly seen in male patients. Despite easy self-assessment, many patients present with advanced disease. Patients with tumors in buccal mucosa or the RMT more commonly involve the infratemporal fossa or the masticator space etc (Fig. 7). Hence, cross-sectional imaging is crucial for evaluating the extent of the malignancy. Computed tomography is the method of choice for the evaluation of bony involvement, especially early cortical erosion. Magnetic resonance (MRI) has an excellent soft-tissue resolution and helps in better delineation of mass and evaluation of perineural spread. On CT, the spread of disease in high ITF (supranotch) is associated with poor surgical outcomes and surgical morbidity[9].
Fig. 7.

CECT of a 51-year-old female patient of right buccal carcinoma. CECT images show enhancing mass in the right buccal space extending into the infratemporal fossa
Lymphoma
Lymphomas are of two types — HL and NHI — and are further subdivided into subtypes according to WHO classification. HL arises in lymph nodes predominantly and only 1–4% of HL are involved in extranodal locations while 25–30% of NHL can occur in extra-nodal sites[10]. Because of late and few symptoms, they are difficult to diagnose. It usually affects patients between 50 and 60 years of age. Most extranodal lymphoma in the head and neck occurs in Waldeyer’s ring but can arise in the paranasal sinus, jaw, orbit, oral cavity, and rarely in the masticator or paraphrayngeal space (Fig. 8). Imaging is required for diagnosis, staging, and also accessing site for biopsy. For localized disease (stages I and II), radiotherapy is the most commonly used treatment modality while for disseminated lymphoma combined chemotherapy with or without radiotherapy is recommended.
Fig. 8.

CECT of a 40-year-old female patient with lymphoma. CECT coronal reformatted images show a homogenous nodal mass on the right side of the neck, extending into the infratemporal fossa
Rhabdomyosarcoma
Rhabdomyosarcoma (RMS) is the most common soft tissue sarcoma in pediatric patients. It has a bimodal age of presentation — first peak at 6–8 years of age and the second peak at 11–14 years of age. In head and neck, the prognosis and surgical outcome of these tumors depends on the location as either parameningeal or nonparameningeal sites. The parameningeal sites are the nasal cavity/nasopharynx, middle ear, and the infratemporal fossa/pterygopalatine space (Fig. 9). Nonparameningeal RMS has a relatively better prognosis in terms of better surgical outcomes. Distant metastases can be seen in 9–23% of the cases[11]. The most common sites of metastases are the lungs, bone, and lymph nodes.
Fig. 9.

CT of 4-year-old patient with rhabdomyosarcoma. CECT images reveals soft tissue mass epicentered in right infratemporal fossa. The medial and lateral pterygoid muscles are not seen separate from the mass
Metastasis/Deposits
Metastatic deposits to infratemporal fossa are rare. Few case reports of metastasis from carcinoma of cervix, carcinoma of thyroid, and adenocarcinoma of unknown primary have been documented. Granulocytic sarcomas are rare solid tumors comprising myeloid precursor cells. It is a rare manifestation of AML, occurring more commonly seen in pediatric patients[12]. Involvement of the head and neck is relatively rare. Granulocytic sarcoma /chloroma of the maxilla-facial region extending into the infratemporal fossa and PPF is therefore one of the rare causes of proptosis in children (Fig. 10).
Fig. 10.

Metastasis/deposits involving ITF. A CT of 14-year-old child — known case of acute myeloid leukemia (AML) with granulocytic sarcoma. CECT image shows soft tissue deposit in the left infratemporal fossa extending into the inferior orbital fissure. B CECT images of a 7-year-old patient with adrenal neuroblastoma with a metastatic deposit in the infratemporal fossa. CECT images show enhancing soft tissue in the right infratemporal fossa extending into the extraconal compartment of right orbit
Primary Jaw Tumors
Various odontogenic and nonodontogenic tumors arising from jaw bone or maxilla show lytic/sclerotic destruction of bone with associated soft tissue component, which can extend into the infratemporal fossa. Imaging plays important role in demonstrating both soft tissue extend and bony details (Fig. 11).
Fig. 11.

Primary jaw tumors involving ITF. A, B CECT images of 5-year-old male child with desmoplastic fibroma left hemimandible show lytic destruction of ramus and angle of mandible on the left side with associated soft tissue in the infratemporal fossa. C, D CECT images of a 10-year-old female patient of osteogenic sarcoma show lytic sclerotic destruction of the left roof of orbit with a large soft tissue component extending into the infratemporal fossa and left nasal cavity. E, F CT images of 14 year of a male patient with jaw PNET shows destruction of the right angle of the mandible with spiculated periosteal reaction and a large soft tissue component in the infratemporal fossa and right submandibular space
Nasopharyngeal Malignancies
Most nasopharyngeal neoplasms are malignant tumors, which show aggressive local infiltration along pre-defined pathways. Anteriorly, it can spread to the nasal cavity from which the tumor can easily infiltrate the pterygopalatine fossa. Once in the PPF, it can spread to the following :
Infratemporal fossa via the pterygomaxillary fissure (Fig. 12)
Foramen rotundum along the maxillary nerve
Vidian canal along the pterygoidean nerve
Fig. 12.

CT images of a 15-year-old male patient of nasopharyngeal carcinoma CT images show enhancing mass epicentered in nasopharynx on right side extending into ipsilateral infratemporal fossa via the pterygomaxillary fissure
MRI best depicts perineural spread and early marrow infiltration, while CT is useful in detecting skull base cortical erosion.
Conclusion
A clear understanding of the anatomy and boundaries of ITF is necessary for precise communication between the surgeon and radiologist. ITF by virtue of its deep location is inaccessible to clinical and endoscopic evaluation. Hence, cross-sectional imaging like CT and MRI (magnetic resonance imaging) plays indispensable role in the evaluation of infratemporal fossa pathologies, accessing its extent and respectability, etc. Information from imaging can also predict surgical outcomes.
Declarations
Conflict of Interest
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Kaplan JN, Duckert LG. Lesions metastatic to the infratemporal fossa: report of a case and review of the literature. Otolaryngol Head Neck Surg. 1984;92(2):241–6. doi: 10.1177/019459988409200221. [DOI] [PubMed] [Google Scholar]
- 2.Jain S, Kumar A, Dhongade H, Varma R, Hathiram BT, Khattar VS. Imaging of parapharyngeal space and infratemporal fossa. Int J Otorhinolaryngol Clin. 2012;4(3):113–121. doi: 10.5005/jp-journals-10003-1096. [DOI] [Google Scholar]
- 3.Amit M, Bell D, Hunt PJ, Hanna E, Su SY, Kupferman M, Aashiq M, Takahashi H, Gidley PW, Nader ME, DeMonte F. Surgical management of carcinomas of the infratemporal fossa and skull base: patterns of failure and predictors of long-term outcomes. J Neurosurg. 2020;134(5):1392–1398. doi: 10.3171/2020.3.JNS192630. [DOI] [PubMed] [Google Scholar]
- 4.Shin JH, Lee HK, Kim SY, Choi CG, Suh DC. Imaging of parapharyngeal space lesions: focus on the prestyloid compartment. Am J Roentgenol. 2001;177(6):1465–1470. doi: 10.2214/ajr.177.6.1771465. [DOI] [PubMed] [Google Scholar]
- 5.Aribandi M, McCoy VA, Bazan C., III Imaging features of invasive and noninvasive fungal sinusitis: a review. Radiographics. 2007;27(5):1283–1296. doi: 10.1148/rg.275065189. [DOI] [PubMed] [Google Scholar]
- 6.Wenig BM, Abbondanzo SL, Childers EL, Kapadia SB, Heffner DR. Extranodal sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) of the head and neck. Hum Pathol. 1993;24(5):483–492. doi: 10.1016/0046-8177(93)90160-I. [DOI] [PubMed] [Google Scholar]
- 7.Tse GM, Chan KF, Ahuja AT, King AD, Pang PC, To EW. Fibromatosis of the head and neck region. Otolaryngol-Head Neck Surg: Off J Am Acad Otolaryngol-Head Neck Surg. 2001;125(5):516–9. doi: 10.1016/S0194-5998(01)53547-0. [DOI] [PubMed] [Google Scholar]
- 8.Trivedi NP, Kekatpure VD, Shetkar G, Gangoli A, Kuriakose MA. Pathology of advanced buccal mucosa cancer involving masticator space (T4b) Indian J Cancer. 2015;52(4):611. doi: 10.4103/0019-509X.178410. [DOI] [PubMed] [Google Scholar]
- 9.Arya S, Chaukar D, Pai P. Imaging in oral cancers. Indian J Radiol Imaging. 2012;22(3):195. doi: 10.4103/0971-3026.107182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Weber AL, Rahemtullah A, Ferry JA. Hodgkin and non-Hodgkin lymphoma of the head and neck: clinical, pathologic, and imaging evaluation. Neuroimaging Clinics. 2003;13(3):371–392. doi: 10.1016/S1052-5149(03)00039-X. [DOI] [PubMed] [Google Scholar]
- 11.Reilly BK, Kim A, Peña MT, Dong TA, Rossi C, Murnick JG, Choi SS. Rhabdomyosarcoma of the head and neck in children: review and update. Int J Pediatr Otorhinolaryngol. 2015;79(9):1477–1483. doi: 10.1016/j.ijporl.2015.06.032. [DOI] [PubMed] [Google Scholar]
- 12.Pui MH, Fletcher BD, Langston JW. Granulocytic sarcoma in childhood leukemia: imaging features. Radiology. 1994;190(3):698–702. doi: 10.1148/radiology.190.3.8115614. [DOI] [PubMed] [Google Scholar]