

Abstract
Background
Many patients do not receive guideline-recommended preventive, chronic disease, and acute care. One potential explanation is insufficient time for primary care providers (PCPs) to provide care.
Objective
To quantify the time needed to provide 2020 preventive care, chronic disease care, and acute care for a nationally representative adult patient panel by a PCP alone, and by a PCP as part of a team-based care model.
Design
Simulation study applying preventive and chronic disease care guidelines to hypothetical patient panels.
Participants
Hypothetical panels of 2500 patients, representative of the adult US population based on the 2017–2018 National Health and Nutrition Examination Survey.
Main Measures
The mean time required for a PCP to provide guideline-recommended preventive, chronic disease and acute care to the hypothetical patient panels. Estimates were also calculated for visit documentation time and electronic inbox management time. Times were re-estimated in the setting of team-based care.
Key Results
PCPs were estimated to require 26.7 h/day, comprising of 14.1 h/day for preventive care, 7.2 h/day for chronic disease care, 2.2 h/day for acute care, and 3.2 h/day for documentation and inbox management. With team-based care, PCPs were estimated to require 9.3 h per day (2.0 h/day for preventive care and 3.6 h/day for chronic disease care, 1.1 h/day for acute care, and 2.6 h/day for documentation and inbox management).
Conclusions
PCPs do not have enough time to provide the guideline-recommended primary care. With team-based care the time requirements would decrease by over half, but still be excessive.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11606-022-07707-x.
KEY WORDS: Team-based care, Primary care, Preventive care, Chronic disease care, Population health
INTRODUCTION
Patients benefit from guideline-based preventive, chronic disease, and acute care,1, 2 but many do not receive it.3 A limitation to providing high-quality care is insufficient time.4, 5 In 2003, Yarnall et al. estimated it would take 7.4 h/day for a primary care provider (PCP) to provide preventive care for a 2500 patient panel.6 A study by Privett et al. found it would take 8.6 h/day.7 A complementary study in 2005 by Østbye et al. calculated 10.6 h/day were needed for a PCP to manage the top ten chronic diseases.8 These studies suggested at least 18 h/per day are needed for a PCP to provide preventive and chronic care management, not accounting for other tasks.
Since 2005, there have been changes in the structure of primary care. Traditionally, PCPs cared for patients primarily by themselves. However, new team-based care models, such as the Comprehensive Primary Care Initiative Plus (CPC+), increasingly involve other care providers in providing patient care.9–11 Many healthcare organizations have encouraged this shift; for example, a National Academy of Medicine report urged new payment models to “pay for primary care teams to care for people, not doctors to deliver services.”12 These models may save PCP time by shifting tasks traditionally performed by the PCP to other members of the care team. Theoretically, the time savings may allow PCPs to focus on more advanced care, see more patients, or increase the delivery of guideline-based care. Because of the potential for team-based care to change primary care practice, we re-investigated the amount of time needed to provide preventive, chronic disease, and acute care without and with team-based care.
METHODS
Patient Panels and Study Design
Two recent surveys of family practice physicians calculated their average patient panel sizes as approximately 230013 and 290014 patients, respectively. A recent meta-analysis determining the optimal panel size was inconclusive, but panels ranged from 1200 to 3600.15 Given the uncertainty in the literature, we modeled patient panels of 2500 patients, and varied this assumption in sensitivity analysis. We created 1000 hypothetical panels of 2500 patients from the 5856 adult participants in the National Health and Nutrition Examination Survey (NHANES) 2017–2018 cohort.16 The chances of inclusion in the panels were proportional to each participant’s sampling weight,17 and each individual selected from the survey to include in a panel was replaced into the survey prior to selecting the next patient. For each panel, we quantified the time needed to address preventive, chronic disease, and acute care assuming the PCP worked alone and with a multidisciplinary team (Fig. 1).
Fig. 1.

Schematic displaying the creation of patient panels from an NHANES cohort, and the calculation of annual PCP preventive and chronic disease care time
Primary Care Services
Preventive Care
We included the Grade A and B preventive care services and immunizations recommended by the United States Preventive Services Task Force (USPSTF) and Advisory Committee on Immunization Practices (ACIP), respectively, in 2020 (Appendix Table 1).14, 15 For each preventive care service and immunization, we determined each NHANES participant’s eligibility based on their age, gender, and presence of chronic conditions/comorbidities. Information to determine eligibility for all services were publicly available in NHANES 2017–2018, except for sexual history, for which we substituted the distribution of responses from the publicly available NHANES 2015–2016 data. For each NHANES participant, we calculated the annual time needed to provide preventive care based on the annual time required for each service they were eligible for (Fig. 1). If the PCP could provide the service herself, that time was calculated. If the service required a referral, the time required for the PCP to coordinate the referral was calculated. These times were summed for each participant to calculate the annual time needed to provide preventive care for each hypothetical panel of 2500 patients.
The total annual time for each service was calculated based on USPSTF guidelines, their citations, and a literature search (Appendix Table 2) describing their annual visit frequency and time per visit. For the literature search, we prioritized in order meta-analyses, clinical trials, review articles, and cohort or case studies. If we found no evidence, we assumed the service would take the same amount of time as another similar service (Appendix Table 2). If a service required screening and follow-up care, the time for both components was calculated independently. If screening resulted in the diagnosis of a chronic disease, we assumed that time would be part of chronic disease care (see below).
Because of heterogeneity in data availability for time estimates, we classified the quality of evidence as “strong,” “moderate,” or “weak,” depending on the evidence source (Table 1). Data from a meta-analysis or randomized control trial was considered “strong”; evidence from cohort or case studies was considered “moderate.” Weak evidence was based on expert opinion or author estimates. If estimates from a similar service were used, we downgraded the strength of evidence by one level.
Table 1.
Estimated Time Needed to Provide Guideline-Based Preventive and Chronic Disease Care for an Average US 2500 Adult Patient Panel
| PCP-only care | Team-based carea | Strength of evidence for time estimatesb | |||
|---|---|---|---|---|---|
| PCP time (h/day) | PCP time (h/day) | Non-PCP time (h/day) | |||
| Preventive care services | Weight loss to prevent obesity-related morbidity and mortality in adults: counseling | 4.11 | 0.34 | 3.77 | Strong |
| Healthy diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: behavioral counseling interventions | 2.36 | 0.20 | 2.16 | Moderate | |
| Unhealthy alcohol use in adults: counseling | 1.77 | 0.30 | 1.48 | Strong | |
| Abnormal blood glucose and type 2 diabetes mellitus: counseling | 1.39 | 0.12 | 1.27 | Moderate | |
| Tobacco smoking cessation in adults: counseling | 0.89 | 0.15 | 0.74 | Strong | |
| Sexually transmitted infections: behavioral counseling | 0.74 | 0.12 | 0.62 | Strong | |
| Unhealthy drug use: counseling | 0.47 | 0.08 | 0.39 | Strong | |
| Depression in adults: screening | 0.31 | 0.00 | 0.31 | Moderate | |
| Intimate partner violence, elder abuse, and abuse of vulnerable adults: counseling | 0.18 | 0.01 | 0.17 | Strong | |
| Statin use for the primary prevention of cardiovascular disease in adults: counseling | 0.18 | 0.18 | 0.00 | Strong | |
| Weight loss to prevent obesity-related morbidity and mortality in adults: screening | 0.17 | 0.00 | 0.17 | Strong | |
| Unhealthy alcohol use in adults: screening | 0.17 | 0.00 | 0.17 | Strong | |
| Tobacco smoking cessation in adults: screening | 0.17 | 0.00 | 0.17 | Strong | |
| Unhealthy drug use: screening | 0.17 | 0.00 | 0.17 | Strong | |
| Cervical cancer: screening | 0.15 | 0.06 | 0.09 | Moderate | |
| Hypertension in adults: screening | 0.12 | 0.00 | 0.12 | Weak | |
| Lung cancer: screening | 0.10 | 0.10 | 0.00 | Moderate | |
| Statin use for the primary prevention of cardiovascular disease in adults: screening | 0.09 | 0.09 | 0.00 | Strong | |
| Depression in adults: referral | 0.09 | 0.09 | 0.00 | Moderate | |
| Influenza vaccine | 0.09 | 0.00 | 0.09 | Weak | |
| Falls prevention in community-dwelling older adults: screening | 0.07 | 0.07 | 0.00 | Moderate | |
| Intimate partner violence, elder abuse, and abuse of vulnerable adults: screening | 0.05 | 0.00 | 0.05 | Strong | |
| Skin cancer prevention: behavioral counseling | 0.05 | 0.05 | 0.00 | Moderate | |
| Latent tuberculosis infection: screening | 0.03 | 0.00 | 0.03 | Moderate | |
| Colorectal cancer: screening | 0.03 | 0.03 | 0.00 | Strong | |
| Abnormal blood glucose and type 2 diabetes mellitus: screening | 0.03 | 0.00 | 0.03 | Moderate | |
| Breast cancer: screening | 0.02 | 0.02 | 0.00 | Moderate | |
| Screening for chlamydia | 0.01 | 0.00 | 0.01 | Moderate | |
| Screening for gonorrhea | 0.01 | 0.00 | 0.01 | Moderate | |
| Hepatitis B virus infection in adults: screening | 0.01 | 0.00 | 0.01 | Moderate | |
| Prevention of human immunodeficiency virus infection: preexposure prophylaxis | 0.01 | 0.01 | 0.00 | Moderate | |
| Tetanus, diphtheria, pertussis vaccine | 0.01 | 0.00 | 0.01 | Weak | |
| Osteoporosis to prevent fractures: screening | 0.01 | 0.01 | 0.00 | Moderate | |
| Screening for syphilis infection in nonpregnant adults | 0.01 | 0.00 | 0.01 | Moderate | |
| Aspirin use to prevent cardiovascular disease and colorectal cancer: counseling | <0.01 | <0.01 | 0.00 | Strong | |
| Human papillomavirus vaccine | <0.01 | 0.00 | <0.01 | Weak | |
| Aspirin use to prevent cardiovascular disease and colorectal cancer: screening | <0.01 | <0.01 | 0.00 | Strong | |
| Hepatitis C virus infection in adults: screening | <0.01 | 0.00 | <0.01 | Moderate | |
| Immunodeficiency Virus infection: screening | <0.01 | 0.00 | <0.01 | Moderate | |
| Folic acid for the prevention of neural tube defects: preventive medication | <0.01 | <0.01 | 0.00 | Moderate | |
| Abdominal aortic aneurysm: screening | <0.01 | <0.01 | 0.00 | Strong | |
| Pneumococcal conjugate vaccine | <0.01 | 0.00 | <0.01 | Weak | |
| Pneumococcal polysaccharide vaccine | <0.01 | 0.00 | <0.01 | Weak | |
| Zoster recombinant vaccine | <0.01 | 0.00 | <0.01 | Weak | |
| BRCA-related cancer: risk assessment | <0.01 | 0.00 | <0.01 | Moderate | |
| BRCA-related cancer: genetic counseling | <0.01 | 0.00 | <0.01 | Moderate | |
| Medication use to reduce risk of breast cancer: screening | <0.01 | <0.01 | 0.00 | Moderate | |
| Medication use to reduce risk of breast cancer: counseling | <0.01 | <0.01 | 0.00 | Moderate | |
| Total time | 14.06 | 2.01 | 12.05 | ||
| Chronic disease carea | Hypertension | 1.72 | 0.86 | 0.86 | Weak |
| Anxiety disorders | 1.60 | 0.80 | 0.80 | Weak | |
| Mood disorders | 1.27 | 0.64 | 0.64 | Weak | |
| Lipid disorders | 0.69 | 0.35 | 0.35 | Weak | |
| Osteoarthritis | 0.68 | 0.34 | 0.34 | Weak | |
| Diabetes mellitus | 0.50 | 0.25 | 0.25 | Weak | |
| Asthma | 0.33 | 0.17 | 0.17 | Weak | |
| Inflammatory joint disorders | 0.26 | 0.13 | 0.13 | Weak | |
| Coronary atherosclerosis | 0.11 | 0.06 | 0.06 | Weak | |
| Other upper respiratory disorders | 0.04 | 0.02 | 0.02 | Weak | |
| Total Time | 7.20 | 3.60 | 3.60 | ||
Abbreviations: PCP, primary care provider; BRCA, breast cancer gene
aThe time required for chronic disease care for team-based care was assumed to be divided evenly between PCPs and non-PCPs.
bThe quality of evidence was classified as “strong,” “moderate,” or “weak,” depending on the evidence source. Data from a meta-analysis or randomized control trial was considered “strong”; evidence from cohort or case studies was considered “moderate,” and data based on expert opinion or author estimates was considered “weak.”
Chronic Disease Care
We selected the ten most prevalent chronic diseases based on published data from the 2014 Medical Expenditure Panel Survey (Table 1).18 We defined each chronic disease using NHANES data (Appendix Table 3), distinguishing between “controlled” and “uncontrolled” disease based on lab or physical exam data (such as a HbA1c >7 for diabetes). Then, for each participant in NHANES, we assessed whether they had each chronic disease, and whether it was “controlled” or “uncontrolled.” The annual time needed to address each chronic disease for each patient was based on the annual visit frequency, which varied based on whether the disease was controlled or uncontrolled, and the time per visit. These times were summed for each participant to calculate the annual time needed to provide chronic disease care for each hypothetical panel.
To estimate the annual visit frequency, we reviewed published guidelines (Appendix Table 4), and collected data on the number of visits required to address controlled vs uncontrolled disease.8, 19–27 If no evidence existed, clinical authors (J.P, C.B, N.L.) independently estimated the annual visits needed, and discussed until consensus. Little data existed quantifying the time needed per visit for each chronic disease. Similar to previous analyses,8 we assumed 10 min per visit to address each chronic disease and tested this assumption in sensitivity analyses.
Acute Care
To account for acute care, we examined nationally representative studies of primary care office visits. These studies found PCPs had approximately 637 visits per 1000 adult patients per year,28 and a mean visit duration of approximately 21 min.29 The time needed to address acute care for each panel was calculated by taking the product of the average number of annual acute care visits per patient, the number of patients per panel, and the mean visit duration.
Documentation and Inbox Management
We estimated this time based on evidence that PCPs spend 3.2 h per day on average on documentation, paperwork, and after visit care.30, 31
Team-Based Care
Preventive Care
We re-estimated the time needed to provide care when dividing time between a PCP and other care team members. We modeled estimates based on the team members in CPC+ because this advanced model allowed us to estimate times for a wide scope of disciplines.9, 32 We determined which preventive care tasks could be done by non-PCP team members by reviewing scope of practice guidelines for each discipline, and calculated the time spent for each team member. We used national guidelines published by governing bodies for each discipline, or Illinois guidelines if national guidelines were not available.33–36 We assumed non-PCP team members performed all services within their scope of practice instead of the PCP.33–36
Chronic Disease and Acute Care
Estimates for the time spent on chronic disease and acute care that could be offset by team-based care models were determined by literature review. For seven of ten chronic diseases, we found evidence non-PCP team members could perform some chronic disease management independently from the PCP,37–43 but little data existed quantifying the time saved. We assumed 50% of PCP time could be saved for chronic disease and acute care, and examined this assumption in sensitivity analyses.
Documentation and Inbox Management
We found evidence medical assistants could screen inboxes for PCPs,44–46 but little data existed quantifying the time saved. We assumed 20% of PCP time could be saved and examined this assumption in sensitivity analysis.
Analysis
For each of the 1000 hypothetical panels of 2500 NHANES participants, the time needed to address preventive care, chronic disease care, acute care, and documentation/inbox management was calculated as outlined above. The means of these data were aggregated, and are displayed in our results.
Sensitivity/Scenario Analysis
We conducted additional analyses to evaluate the robustness of the results. We varied patient panel size between 1500, 2000, and 3000 patients. We also re-estimated the chronic disease visit time, assuming treating multiple concordant chronic conditions would take less time than treating each condition separately.47, 48 We created four clusters of related conditions: “metabolic disorders” (hypertension, hyperlipidemia, diabetes, and coronary artery disease), “psychiatric disorders” (mood disorders and anxiety disorders), “respiratory disorders” (asthma and other upper respiratory disorders), and “musculoskeletal disorders” (osteoarthritis and inflammatory joint disorders). The time needed for each cluster was based on the sum of each patient’s annual visits needed to address each chronic disease within the cluster, assuming that the first three visits would take 10 min each and each additional visit would take 5 min. We created a separate sensitivity analysis assuming chronic disease visits would take 5 min, instead of 10 min. Lastly, we varied the percentage of PCP time for chronic disease and acute care saved by team-based care by ±25% (75% and 25%), and for documentation/inbox management by ±10% (30% and 10%).
RESULTS
For an average 2500-patient panel, a PCP would require 26.7 h/day to provide preventive, chronic, and acute care with documentation/inbox management (Fig. 2). Preventive care alone would require about 14.1 h. Each preventive care task time varied from less than 1 s/day (medication to reduce breast cancer) to 4.1 h/day (obesity counseling) (Table 1). Over 10 h would be spent on counseling tasks, especially dietary or obesity counseling. Chronic disease care alone required about 7.2 h/day. Acute care would require 2.2 h/day, while documentation and inbox management would require 3.2 h/day.30, 31
Fig. 2.
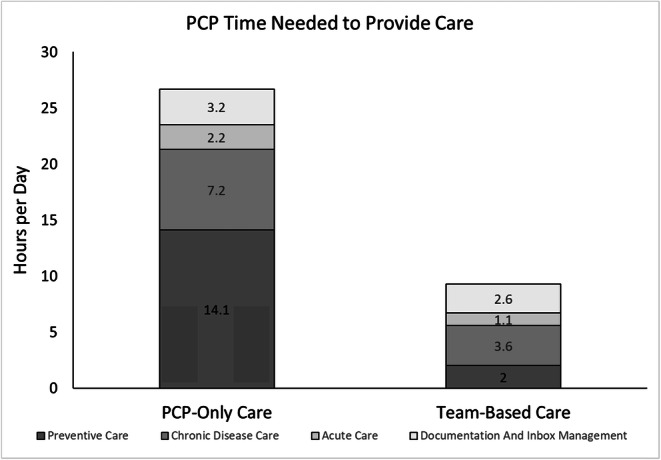
Primary care provider time needed to provide care for average US adult panel of 2500 patients.
With team-based care, the total PCP time decreased to about 9.3 h/day. Non-PCP team members could partially or completely perform 29 preventive care tasks, leaving about 2.0 h of preventive care tasks per day for the PCP. The majority of time reduction was due to 10.8 h of counseling tasks being transferred to dieticians or counselors. Chronic disease care would decrease to 3.6 h/day, acute care to 2.2 h/day, and documentation/inbox management to 2.6 h/day. Overall, 17.4 h could be shifted to other members of the health care team (Figs. 2 and 3).
Fig. 3.
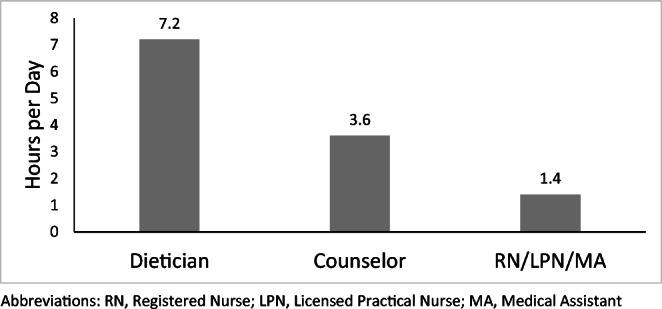
Additional preventive care time shifted to non-PCP team members in a team-based care model. Abbreviations: RN, registered nurse; LPN, licensed practical nurse; MA, medical assistant.
Sensitivity/Scenario Analysis
Using best-case assumptions (a 1500-patient panel, team-based care, 5 min per chronic disease visit, 75% of chronic disease/acute care time, and 30% of documentation time performed by other team members), a PCP would require 4.5 h/day. However, using the worst-case assumptions (a 3000-patient panel, no team-based care), total time increased to 32.0 h/day.
Changing the panel size to 1500, 2000, and 3000 patients resulted in −10.7, −5.3, and +5.3 h change in PCP time without team-based care, and −3.7, −1.9, and +1.9 h change with team-based care (Figs. 4 and 5). Accounting for multimorbidity by “clustering” chronic diseases decreased the PCP time by 0.6 and 1.2 h with and without team-based care, respectively. Assuming a 5-min chronic disease visit time decreased the PCP time by 1.8 h with and 3.6 h without team-based care. Assuming 25% or 75% of chronic disease care could be done by non-PCP team members resulted in a ±1.8 h change in PCP time.
Fig. 4.

Sensitivity/scenario analyses: change in PCP time with PCP-only care. Abbreviations: PCP, primary care provider.
Fig. 5.

Sensitivity/scenario analyses: percent change in PCP time with team-based care. Abbreviations: PCP, primary care provider.
DISCUSSION
Our study found that a PCP would need an infeasible 26.7 h/day to provide preventive, chronic disease, and acute care for an average US adult patient panel. If a PCP worked in a team-based care model, up to 65% of his services could be performed by other healthcare team members. Only under the best-case assumptions could total PCP time fit into a standard 8-h workday.
Our estimates for preventive care time (14.1 h) were higher than estimates by Yarnall et al. (7.4 h) or Privett et al. (8.6 h).6, 7 This difference is largely explained by differences in calculating the time needed for counseling tasks. We based our estimates on USPSTF meta-analyses, which demonstrated that effective counseling interventions are extremely time intensive.49–51 For example, obesity counseling requires “12 or more sessions” per year to provide evidence of benefit,52 with most studies taking more time than our conservative estimate of 72 total minutes per patient per year.50, 52 Privett estimated counseling times more conservatively. Our estimates for chronic disease care (7.2 h) were lower than Østbye et al.’s estimates, as current chronic disease guidelines recommend fewer visits per year.20, 21
Given the large gap between the time required to provide guideline-based care and the limits of a clinic day, many clinicians are likely not completing specific services, not completing them according to the guidelines, or working overtime. If time pressures are driving a gap between guideline-based and clinical medicine, it might explain why national health outcomes are worse than expected.53 It may also drive physician burnout, which is often associated with large panel sizes54 and the subjective feeling of being overworked.4 Low income and racial/ethnic minority status are strongly associated with insufficient access to primary care.55 To the extent that the excessive time required to provide guideline-based care is exacerbating the physician shortage, it may be contributing to unequal access to care. If clinical guidelines do not consider the time opportunity cost of an intervention, the gap between guideline-based and clinical medicine will persist.
Advanced team-based care may reduce the time needed for PCPs to deliver guideline-based care. Counseling tasks are extremely time intensive,49–51, 56 but the majority of PCP time saved occurred by shifting those tasks to other team members. Our findings support a 2012 study which concluded that non-PCPs could complete 77% of preventive care guidelines and 47% of chronic disease care.57
Team-based care models may save PCPs time at the expense of fragmented patient care. However, the efficiency gains from providers working at the top of their license and well-functioning team-based care models may limit this downside. Overall, team-based care models may be associated with increased adherence to quality measures at marginally lower total costs.58
We chose the CPC+ model as it was a functioning care model that incentivized a broad range of team-based care services. Other models in the community (and even individual CPC+ clinics) may not have access to all the team members envisioned by our idealized model. As a result, their ability to save PCP time may be more limited. Conversely, if a team-based care model included a broader range of team-members, such as dentists or physical therapists, more PCP time could be saved. Our estimates of PCP time with and without team-based care represent two polar scenarios for a PCP to provide guideline-based care, and individual results may vary.
Some innovative care models incentivize adoption of team-based care;32, 58 however, fee-for-service healthcare reimbursement does not allow many non-PCP team members to be paid for services.59, 60 Dietician performed dietary counseling is only reimbursed by Medicare if the patient has diabetes, renal disease, or a renal transplant,61 though USPSTF guidelines also recommend dietary counseling for other populations. Even with a transition to value-based care, the debate of whether each potential team member adds sufficient value to be hired will remain.
The challenge of implementing team-based care models is compounded by low PCP compensation. PCPs are reimbursed at lower rates than specialists, are more likely to maintain high-volume clinics,62 and spend large amounts of time doing uncompensated between-visit work.63 In this setting, it would be a challenge for a PCP to handle the costs of hiring new employees without additional payment. Unless new compensation models are implemented, these team-based care models might not be feasible.
Significantly lowering the panel size to less than 1500 patients may allow time to provide guideline-based care, and the emergence of “direct primary care” models may reflect this opportunity.54 However, the membership fees necessary to support these models may preclude their dissemination, and smaller panels would exacerbate the current PCP shortage.
Our study had several limitations. Little evidence existed on the time needed to address each chronic disease at each visit, but even assuming a 5-min visit time or accounting for time saved from clustering concordant chronic diseases did not change our conclusions. Assuming different panel sizes resulted in proportional changes to our results, but even a 1500-patient panel required 16.0 h/day of PCP time. Under every scenario our conclusion was the same: providing ideal guideline-based preventive, chronic disease, and acute care services places an unreasonable time burden on a PCP that is only partially mitigated by team-based care models and smaller panel sizes.
Our calculations represent a lower bound estimate for PCP time. We consistently chose the most conservative time estimate for which there were data, included only ten chronic diseases, limited our preventive care services to USPSTF recommendations, and did not account for breaks in time between patients. We also did not account for inefficiencies associated with combining visits for all the separate preventive care/chronic disease/acute care services into discrete clinic time slots. Additionally, the 2020 COVID-19 pandemic has at least temporarily increased the workload for PCPs, leading to large increases in electronic work which is not accounted for in this analysis.64, 65 Finally, many common patient-specific factors and conditions requiring PCP time were not addressed. Issues such as aging/frailty, language concordance, or homelessness were indirectly addressed insofar as they are associated with a higher risk for chronic diseases, but were not accounted for independently.
Overall, it would take an infeasible 26.7 h per day for a PCP to provide guideline-based care for a 2500 patient panel in 2020. This time could be decreased to 9.3 h per day with team-based care. These findings explain why improvements in the quality of primary care have eluded the USA for the last two decades. Models of primary care that leverage and reimburse appropriately for interdisciplinary teams can only partially rectify the US healthcare system.
Supplementary information
(DOCX 40 kb)
Declarations
Conflict of interest
Cynthia Boyd: Dr. Boyd was funded by NIA K24AG056578.
Neda Laiteerapong: Dr. Laiteerapong was funded by NIDDK P30 DK092949.
Justin Porter: None
M. Reza Skandari: None
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Grade Definitions - US Preventive Services Task Force. Accessed September 30, 2019. https://www.uspreventiveservicestaskforce.org/Page/Name/grade-definitions
- 2.O’Connor PJ. Adding value to evidence-based clinical guidelines. JAMA. 2005;294(6):741–743. doi: 10.1001/jama.294.6.741. [DOI] [PubMed] [Google Scholar]
- 3.McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635–2645. doi: 10.1056/NEJMsa022615. [DOI] [PubMed] [Google Scholar]
- 4.Campion EW. A Symptom of Discontent. N Engl J Med. 2001;344(3):223–225. doi: 10.1056/NEJM200101183440311. [DOI] [PubMed] [Google Scholar]
- 5.Heponiemi T, Hyppönen H, Kujala S, et al. Predictors of physicians’ stress related to information systems: a nine-year follow-up survey study. BMC Health Serv Res. 2018;18(1):284. doi: 10.1186/s12913-018-3094-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yarnall KSH, Pollak KI, Østbye T, Krause KM, Michener JL. Primary care: is there enough time for prevention? Am J Public Health. 2003;93(4):635–641. doi: 10.2105/ajph.93.4.635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Privett N, Guerrier S. Estimation of the time needed to deliver the 2020 USPSTF preventive care recommendations in primary care. Am J Public Health. 2021;111(1):145-149. 10.2105/AJPH.2020.305967 [DOI] [PMC free article] [PubMed]
- 8.Østbye T, Yarnall KSH, Krause KM, Pollak KI, Gradison M, Michener JL. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med. 2005;3(3):209–214. doi: 10.1370/afm.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Creating Patient-centered Team-based Primary Care. :27.
- 10.The role of patient care teams in chronic disease management | The BMJ. Accessed October 10, 2019. https://www.bmj.com/content/320/7234/569 [DOI] [PMC free article] [PubMed]
- 11.Swankoski KE, Peikes DN, Palakal M, Duda N, Day TJ. Primary care practice transformation introduces different staff roles. Ann Fam Med. 2020;18(3):227–234. doi: 10.1370/afm.2515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Implementing High-Quality Primary Care | National Academies. Accessed April 26, 2022. https://www.nationalacademies.org/our-work/implementing-high-quality-primary-care
- 13.Dai M, Ingham R, Peterson L. Scope of practice and patient panel size of family physicians who work with nurse practitioners or physician assistants. Fam Med. 2019;51(4):311–318. doi: 10.22454/FamMed.2019.438954. [DOI] [PubMed] [Google Scholar]
- 14.Angstman KB, Horn JL, Bernard ME, et al. Family medicine panel size with care teams: impact on quality. J Am Board Fam Med. 2016;29(4):444–451. doi: 10.3122/jabfm.2016.04.150364. [DOI] [PubMed] [Google Scholar]
- 15.Shekelle PG, Paige NM, Apaydin EA, et al. What is the Optimal Panel Size in Primary Care? A Systematic Review [Internet]. Washington (DC): Department of Veterans Affairs (US); 2019 Aug. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553674/ [PubMed]
- 16.NHANES - National Health and Nutrition Examination Survey Homepage. Published February 4, 2021. Accessed February 14, 2021. https://www.cdc.gov/nchs/nhanes/index.htm
- 17.National Health and Nutrition Examination Survey, 2015−2018: Sample Design and Estimation Procedures. (2020, April 1). National Center for Health Statistics. Accessed February 14, 2021. https://www.cdc.gov/nchs/data/series/sr_02/sr02-184-508.pdf [PubMed]
- 18.Buttorff, Christine, Teague Ruder, and Melissa Bauman, Multiple Chronic Conditions in the United States. Santa Monica, CA: RAND Corporation, 2017. https://www.rand.org/pubs/tools/TL221.html
- 19.2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:e127-e248. [DOI] [PubMed]
- 20.Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Circulation. 2014;129(25_suppl_2):S1–S45. doi: 10.1161/01.cir.0000437738.63853.7a. [DOI] [PubMed] [Google Scholar]
- 21.Ng CWM, How CH, Ng YP. Managing depression in primary care. Singapore Med J. 2017;58(8):459–466. doi: 10.11622/smedj.2017080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Standards of Medical Care in Diabetes—2018 abridged for primary care providers. Clin Diabetes Publ Am Diabetes Assoc. 2018;36(1):14-37. 10.2337/cd17-0119 [DOI] [PMC free article] [PubMed]
- 23.National Collaborating Centre for mental health. Generalised Anxiety Disorder in Adults: The NICE Guidelines on Management in Primary, Secondary and Community Care. RCPsych Publications; 2011.
- 24.Expert Panel Report 3 (EPR-3): Guidelines for the diagnosis and management of asthma–summary report 2007. J Allergy Clin Immunol. 2007;120(5, Supplement). 10.1016/j.jaci.2007.09.029 [DOI] [PubMed]
- 25.2013 ESC guidelines on the management of stable coronary artery disease. The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Rev Esp Cardiol Engl Ed. 2014;67(2):135. 10.1016/j.rec.2013.11.008 [DOI] [PubMed]
- 26.Hueston WJ. Treatment of hypothyroidism. Am Fam Physician. 2001 Nov 15;64(10):1717-24. Erratum in: Am Fam Physician 2002 Jun 15;65(12):2438. PMID: 11759078 [PubMed]
- 27.Siafakas NM, Vermeire P, Pride NB, et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). The European Respiratory Society Task Force. Eur Respir J. 1995;8(8):1398–1420. doi: 10.1183/09031936.95.08081398. [DOI] [PubMed] [Google Scholar]
- 28.Chou SC, Venkatesh AK, Trueger NS, Pitts SR. Primary care office visits for acute care dropped sharply in 2002-15, while ed visits increased modestly. Health Aff Proj Hope. 2019;38(2):268–275. doi: 10.1377/hlthaff.2018.05184. [DOI] [PubMed] [Google Scholar]
- 29.Chen LM, Farwell WR, Jha AK. Primary care visit duration and quality: does good care take longer? Arch Intern Med. 2009;169(20):1866–1872. doi: 10.1001/archinternmed.2009.341. [DOI] [PubMed] [Google Scholar]
- 30.Tai-Seale M, Olson CW, Li J, et al. Electronic health record logs indicate that physicians split time evenly between seeing patients and desktop medicine. Health Aff (Millwood). 2017;36(4):655–662. doi: 10.1377/hlthaff.2016.0811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Akbar F, Mark G, Warton EM, et al. Physicians’ electronic inbox work patterns and factors associated with high inbox work duration. J Am Med Inform Assoc. 2020;(ocaa229). 10.1093/jamia/ocaa229 [DOI] [PMC free article] [PubMed]
- 32.Independent Evaluation of the Comprehensive Primary Care Plus (CPC+): Third Annual Report. Mathematica. Accessed February 21, 2021. https://www.mathematica.org/our-publications-and-findings/publications/independent-evaluation-of-the-comprehensive-primary-care-plus-cpc-third-annual-report
- 33.PART 1300 NURSE PRACTICE ACT : Sections Listing. Accessed July 15, 2019. http://www.ilga.gov/commission/jcar/admincode/068/06801300sections.html
- 34.Academy of Nutrition and Dietetics Scope of Practice for the Registered Dietitian. J Acad Nutr Diet. 2013;113(6):S17–S28. doi: 10.1016/j.jand.2012.12.008. [DOI] [PubMed] [Google Scholar]
- 35.National Society of Genetic Counselors : Model Legislative Provisions. Accessed February 26, 2020. https://www.nsgc.org/p/cm/ld/fid=18#scope
- 36.AMHCA Standards - American Mental Health Counselors Association. Accessed February 26, 2020. https://www.amhca.org/publications/standards
- 37.Carey N, Courtenay M. Clark et al. Nurse-led interventions used to improve control of high blood pressure in people with diabetes: a systematic review and meta analysis. Diabet Med. 2012;29(1):154–155. doi: 10.1111/j.1464-5491.2011.03424.x. [DOI] [PubMed] [Google Scholar]
- 38.Chiang CY, Choi KC, Ho KM, Yu SF. Effectiveness of nurse-led patient-centered care behavioral risk modification on secondary prevention of coronary heart disease: A systematic review. Int J Nurs Stud. 2018;84:28–39. doi: 10.1016/j.ijnurstu.2018.04.012. [DOI] [PubMed] [Google Scholar]
- 39.de Thurah A, Esbensen BA, Roelsgaard IK, Frandsen TF, Primdahl J. Efficacy of embedded nurse-led versus conventional physician-led follow-up in rheumatoid arthritis: a systematic review and meta-analysis. RMD Open. 2017;3(2):e000481. doi: 10.1136/rmdopen-2017-000481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wells MJ, Owen JJ, McCray LW, et al. Computer-assisted cognitive-behavior therapy for depression in primary care: systematic review and meta-analysis. Prim Care Companion CNS Disord. 2018;20(2):. 10.4088/PCC.17r02196 [DOI] [PubMed]
- 41.Wang Q, Shen Y, Chen Y, Li X. Impacts of nurse-led clinic and nurse-led prescription on hemoglobin A1c control in type 2 diabetes. Medicine (Baltimore). 2019;98(23). 10.1097/MD.0000000000015971 [DOI] [PMC free article] [PubMed]
- 42.Hofmann SG, Smits JAJ. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621–632. doi: 10.4088/JCP.v69n0415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kuethe MC, Vaessen-Verberne AAPH, Elbers RG, Aalderen WMV. Nurse versus physician-led care for the management of asthma. Cochrane Database Syst Rev. 2013;(2). 10.1002/14651858.CD009296.pub2 [DOI] [PMC free article] [PubMed]
- 44.Murphy DR, Satterly T, Giardina TD, Sittig DF, Singh H. Practicing clinicians’ recommendations to reduce burden from the electronic health record inbox: a mixed-methods study. J Gen Intern Med. 2019;34(9):1825–1832. doi: 10.1007/s11606-019-05112-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lieu TA, Altschuler A, Weiner JZ, et al. Primary care physicians’ experiences with and strategies for managing electronic messages. JAMA Netw Open. 2019;2(12):e1918287. doi: 10.1001/jamanetworkopen.2019.18287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hung DY, Truong QA, Liang SY. Implementing lean quality improvement in primary care: impact on efficiency in performing common clinical tasks. J Gen Intern Med. 2021;36(2):274–279. doi: 10.1007/s11606-020-06317-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Laiteerapong N, Huang ES, Chin MH. Prioritization of care in adults with diabetes and comorbidity. Ann N Y Acad Sci. 2011;1243(1):69–87. doi: 10.1111/j.1749-6632.2011.06316.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29(3):725. doi: 10.2337/diacare.29.03.06.dc05-2078. [DOI] [PubMed] [Google Scholar]
- 49.O’Connor EA, Perdue LA, Senger CA, et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;320(18):1910. doi: 10.1001/jama.2018.12086. [DOI] [PubMed] [Google Scholar]
- 50.LeBlanc EL, Patnode CD, Webber EM, Redmond N, Rushkin M, O’Connor EA. Behavioral and pharmacotherapy weight loss interventions to prevent obesity-related morbidity and mortality in adults: an updated systematic review for the U.S. Preventive Services Task Force. Agency for Healthcare Research and Quality (US); 2018. Accessed February 27, 2020. http://www.ncbi.nlm.nih.gov/books/NBK532379/ [PubMed]
- 51.Recommendation: Abnormal Blood Glucose and Type 2 Diabetes Mellitus: Screening | United States Preventive Services Taskforce. Accessed March 8, 2021. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/screening-for-abnormal-blood-glucose-and-type-2-diabetes
- 52.Final Recommendation Statement: Weight Loss to Prevent Obesity-Related Morbidity and Mortality in Adults: Behavioral Interventions - US Preventive Services Task Force. Accessed February 26, 2020. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/obesity-in-adults-interventions1 [DOI] [PubMed]
- 53.Marcotte-Chénard A, Deshayes TA, Ghachem A, Brochu M. Prevalence of the metabolic syndrome between 1999 and 2014 in the United States adult population and the impact of the 2007-2008 recession: an NHANES study. Appl Physiol Nutr Metab Physiol Appl Nutr Metab. 2019;44(8):861–868. doi: 10.1139/apnm-2018-0648. [DOI] [PubMed] [Google Scholar]
- 54.Rowe K, Rowe W, Umbehr J, Dong F, Ablah E. Direct primary care in 2015: a survey with selected comparisons to 2005 survey data. Kans J Med. 2017;10(1):3–6. doi: 10.17161/kjm.v10i1.8640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lucarelli C, Prince J, Simon K. The welfare impact of reducing choice in Medicare part D: a comparison of two regulation strategies*: reducing choice in medicare part d. Int Econ Rev. 2012;53(4):1155–1177. doi: 10.1111/j.1468-2354.2012.00715.x. [DOI] [Google Scholar]
- 56.USPSTF A and B Recommendations - US Preventive Services Task Force. Accessed July 11, 2019. https://www.uspreventiveservicestaskforce.org/Page/Name/uspstf-a-and-b-recommendations/
- 57.Altschuler J, Margolius D, Bodenheimer T, Grumbach K. Estimating a reasonable patient panel size for primary care physicians with team-based task delegation. Ann Fam Med. 2012;10(5):396–400. doi: 10.1370/afm.1400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Reiss-Brennan B, Brunisholz KD, Dredge C, et al. Association of integrated team-based care with health care quality, utilization, and cost. JAMA. 2016;316(8):826. doi: 10.1001/jama.2016.11232. [DOI] [PubMed] [Google Scholar]
- 59.Basu S, Landon BE, Williams JW, Bitton A, Song Z, Phillips RS. Behavioral health integration into primary care: a microsimulation of financial implications for practices. J Gen Intern Med. 2017;32(12):1330–1341. doi: 10.1007/s11606-017-4177-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Dowling R. Reimbursement for obesity counseling. Medical Economics. Published December 7, 2018. Accessed February 26, 2020. https://www.medicaleconomics.com/article/reimbursement-obesity-counseling
- 61.Medical Nutrition Therapy - Manuals. Accessed November 9, 2019. https://www.ngsmedicare.com/ngs/portal/ngsmedicare/newngs/home-lob/pages/Manuals/preventive%20services%20guide/medical%20nutrition%20therapy%20-%20preventive%20services%20guide/!ut/p/z0/nU9BbgIxDPxKOHBENhQqcYwoiBYhIfWy5FKFxSymwRuy2aX8vlnaQysVDvXJMxrPjMFABkZsw4WNXIp1Ca_N49tQP0_7_QkucLYYon59Gs8HevyAK4QXMEmAN0Zj6zAIy8myAONt3PdYdiVkUlRH2nJuA31b3Mn428IHakgiN6QqCg3nVKmi5i1B9mXtlNQxcPuJinsK1l9UT905gzUfTiejweSlRPqIv3peOYlC5y7-oK_Y1xuXUBtVdfFopbYuLTezkuZfFf272Yzc4XLWnc4nZ8vSWg!!/
- 62.Oddone EZ, Boulware LE. Primary care: medicine’s Gordian knot. Am J Med Sci. 2016;351(1):20–25. doi: 10.1016/j.amjms.2015.10.010. [DOI] [PubMed] [Google Scholar]
- 63.Young R, Burge S, Kumar K, Wilson J, Ortiz D. A time-motion study of primary care physicians’ work in the electronic health record era. Family Medicine. 10.22454/FamMed.2018.184803 [DOI] [PubMed]
- 64.Huston P, Campbell J, Russell G, et al. COVID-19 and primary care in six countries. BJGP Open. 2020;4(4). 10.3399/bjgpopen20X101128 [DOI] [PMC free article] [PubMed]
- 65.Morreel S, Philips H, Verhoeven V. Organisation and characteristics of out-of-hours primary care during a COVID-19 outbreak: A real-time observational study. PLOS ONE. 2020;15(8):e0237629. doi: 10.1371/journal.pone.0237629. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX 40 kb)