

Abstract
Background
The aim of the study was to present rare sinus syndromes known as silent sinus syndrome (SSS) and frontal sinus syndrome with excessive pneumatization and bone defects in the wall (pneumocele). The available literature describing pneumocele cases was reviewed.
Methodology
PubMed and Science Direct databases were searched by two independent reviewers. The primary outcome was finding descriptions of the sinus pneumocele. In the end, papers on frontal sinus pneumocele that was not the result of trauma, congenital defects or comorbidities were selected. Moreover, the authors presented their own cases of SSS and pneumocele.
Results
Twelve case reports of frontal sinus pneumocele were found, one own case was presented. In addition, 8 subjects with SSS, diagnosed and treated in the period from September 2017 to May 2022, were described.
Conclusions
With the increasing number of patients suffering from sinus diseases and the growing number of endoscopic surgeries, the knowledge of rare sinus syndromes will increase the safety of the procedures performed.
Keywords: Silent sinus syndrome, Pneumocele, Pneumosinus dilatans, Frontal sinus, Maxillary sinus
Introduction
Rare and seemingly completely different syndromes, namely, silent sinus syndrome (SSS) and pneumosinus dilatans (PD), can confuse even an experienced rhinologist. What they have in common is the lack of inflammatory lesions in the sinuses in imaging tests and no clinical symptoms until visual disturbances or facial deformities occur. In the case of silent sinus syndrome, it is caused by lower orbital wall lowering, and in the case of pneumosinus dilatans, by pushing down the eyeball by the gas-distended frontal sinus. This happens when symptoms concern the maxillary sinus (in SSS) and the frontal sinus (in PD). The process of diagnosing the syndromes becomes even more complicated when the disease affects other sinuses. Silent sinus syndrome is characterized by spontaneous enophthalmos and hypoglobus on the ipsilateral hypoplastic maxilla, secondarily causing orbital floor lowering. The silent sinus is sometimes described as hypoplastic. However, this term should be reserved for congenital unilateral or bilateral underdevelopment. A CT image in sinus hypoplasia is stable, whereas in SSS, changes in CT scans are progressing [1]. SSS can be diagnosed among both children [2, 3] and adults, with a slight predominance between the 3rd and 5th decade[4]. The pathophysiology of SSS remains uncertain. It is suggested that idiopathic obstruction of the ostiomeatal complex results in sinus hypoventilation and discharge. The resorption of secretion leads to the generation of subatmospheric pressure in the maxillary antrum causing maxillary sinus collapse [3, 5–8]. Only a few cases of silent frontal or ethmoid sinuses have been described in the literature [9, 10].
At the other extreme of ventilation disorders, the sinuses are excessively distended with gases, crossing the bone boundaries with or without their destruction.
Pneumosinus Dilatans was first reported in 1898 by Meyes, and the term PD was introduced by Benjamin in 1918, who described an excessively enlarged paranasal sinus filled with air and covered with unchanged mucosa [11]. In 2017, Ricci [12] provided a review of 117 papers describing 134 PD cases. Most often, the process concerned the frontal sinus (63%) followed by the sphenoid sinus (25%); the remaining cases related to the maxillary and ethmoid sinuses. In 84% of the cases, the process involved one sinus. Men between the ages of 20 and 40 suffered from the disease more often, but there were also cases at the age of 12–72 [13–15].
The term pneumosinus dilatans multiplex appears in the literature describing cases of involvement of more than one sinus with excessive aeration of the mastoid process or the frontal and ethmoid sinus complicated by meningocele and sphenoid wing PD associated with a huge arachnoid cyst [16].
Urken introduced the following nomenclature for excessively enlarged frontal sinuses [17]:
hypersinus—enlarged sinus with normal walls not extending beyond the boundary of the frontal bone,
pneumosinus dilatans—excessively enlarged frontal sinus with a raised front and/or back wall, and a thinner bone without defects,
pneumocele—the walls of the distended sinus cross the border of the frontal sinus with a partial bone loss. This kind of changes intrigued the authors of the study the most.
The condition for diagnosing pneumocele is proper aeration without inflammatory lesions in the paranasal sinuses, trauma, or previous surgical interventions. The aetiology of the disease is unknown. Theoretically, ball-valve mechanism, fibro-osseous dysregulation, draining mucocele, genetic predisposition with hormonal trigger during puberty, gas forming bacteria, hormonal dysregulation of bone metabolism are taken into consideration [12]. Unfortunately, there is no evidence for unequivocal confirmation of any of the mechanisms. The fact is that the sinus is over-distended with air, with the mucosa unchanged and the lack of an obvious cause in the structure of the sinus and its ostium. This is in opposition to SSS, where the sinus ostium is closed by drawing the uncinate process into the medial wall of the sinus filled with mucous secretions, gradual absorption of which causes the suction of the sinus walls. In the case of SSS within the maxillary sinus and PD in the frontal sinus (which is the most common), patients do not report symptoms characteristic of chronic rhinosinusitis (CRS) according to the definition of the European Position Paper on Rhinosinusitis and Nasal Polyps 2020 (EPOS 2020) [18]. The problem appears relatively late, when craniofacial deformity or visual disturbances occur as a consequence of eyeball lowering. Rarely do patients report local headaches, pressure in the area of the affected sinus. This might also be the reason for such low recognition of the disease.
The aim of the authors of the study was to review the literature to investigate the frequency of extreme distension of the paranasal sinuses with bone loss, especially in the frontal sinus. Data on gender, age, previous sinusitis or head injuries, comorbidities, and, above all, further treatment of patients diagnosed with pneumocele were investigated.
The authors of the study present their own experiences with SSS of the maxillary sinuses and describe the case of frontal sinus pneumocele, radiological documentation and the adopted surgical strategy.
Materials and methods
The systematic review was performed according to the PRISMA 2020 checklist [19]. Electronic databases Pubmed and Science Direct were searched from March 1st 2022 until May 1st 2022. Two reviewers (M.K., K.G.) independently executed the comprehensive literature search. The following free-text terms were used for the database search: pneumosinus dilatans, pneumocele, frontal sinus. Although no year limitation was imposed, only studies published in English were considered for inclusion. The search was restricted to humans only. Neither informed consent nor ethics approval was required as this study was a systemic review of published papers.
The study selection process was executed independently by two reviewers (M.K. and K.G.). The criteria for the inclusion and exclusion of the studies in this review were defined.
The inclusion criteria were as follows: (1) case report, (2) diagnosed frontal sinus pneumocele, (3) pneumocele frontalis not caused by head trauma, congenital defects or other diseases. Studies with a putative but unconfirmed link between a head injury and the presence of pneumocele frontalis were included. There was no sex or age restriction.
The exclusion criteria were as follows: (1) patients with pneumocele of the nasal sinuses other than the frontal ones, (2) patients with pneumocele of the frontal sinuses caused by a traumatic brain injury, congenital defects or other diseases, (3) no case report, (4) no access to the full-text paper. Non-English publications were also excluded.
Two authors (M.K and K.G) independently extracted the relevant data from the included studies. When there was insufficient information for extraction or imputation, the corresponding author of that study was contacted for more information. Problems or conflicts during screening and extraction were resolved by discussion among the authors or with the final decision made by the main author (G.S-M).
The following data were recorded from each of the eligible studies: first author, year of publication, sex, age, CRS symptoms, history of head trauma, comorbidities, associated complications, treatment, follow-up.
The risk of bias within the included studies was evaluated by two authors (M.K and K.G.) using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool, assessing possible bias in four different categories: patient selection, index test, reference standard, and flow and timing [20].
The authors of the study also performed a literature review focusing on SSS, which was presented in a previously published study [21]. In the period from September 2017 to May 2022, 1766 patients (742 females and 1024 males) with paranasal sinus diseases were admitted and operated on at the Department of Laryngology and Laryngological Oncology in Katowice–Ochojec. SSS patients were selected from this group.
Results
A total of 262 studies were retrieved through the systematic search of bibliographic databases. After removing 19 duplicates, 243 papers were eligible for title and abstract screening. After title and abstract screening, the authors excluded 243 articles and read the full text of 41 papers. In the end, 12 publications containing case reports of 13 patients with pneumocele of the frontal sinuses were included in meta-analysis. 22 papers were rejected due to the presence of pneumocele in the paranasal sinuses other than the frontal ones, 3 papers were not available in English, in 2 studies, the described cases were proven to be related to a head injury or congenital defect, 1 publication did not contain a case report, and 1 had no open access. The selection process is presented in Fig. 1. The risk of bias for all studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool [20].
Fig. 1.

Literature search strategy
All 12 studies were written in English and published from 1974 to 2018. Of the 13 patients, the majority were male (11 men and 2 women). The mean age was 37.7 years, the oldest was a 67-year-old woman and the youngest was an 18-year-old man. All patients were diagnosed with pneumocele of the frontal sinuses. One person had pneumocele of the frontal and sphenoidal sinuses simultaneously.
1 subject suffered a head injury 21 years before, but as the authors add “the relationship between head trauma and the frontal pneumocele is not clear”. 4 out of 13 patients had symptoms of chronic sinusitis. Only 3 patients had additional conditions: (1) dilated sphenoidal sinuses, orbital and frontal subcutaneous aerocele, (2) type III frontal recess air cell and (3) respiratory epithelial adenomatoid hamartoma with nasal polyps. Complications caused by pneumocele developed in seven patients. Two were complicated by pneumocephalus. Ocular complications occurred in four patients (orbital roof defect, orbital emphysema, proptosis, hypoglobus and orbital swelling). In all but one of the cases, surgery was the recommended method of treatment. Four patients underwent endoscopic surgery and three refused to undergo the surgical procedure.
The subjects whose health status was observed after accepting (or refusing) treatment, showed complete or partial regression of symptoms caused by pneumocele in the frontal sinuses.
The characteristics of the twelve included studies are summarised in Table 1.
Table 1.
Study characteristics
| Papers | Lead Author [ref] (year) | Sex | Age | Chronic Sinusitis Symptoms | Head Trauma History | Comorbidies | Associated complications | Treatment | Follow-up | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Abnormally large frontal sinus. II. Nomenclature, pathology, and symptoms | Urken ML et al. [17] (1987) | Male | 33 | No | None | None | None | Surgery refused by the patient | None |
| Male | 36 | No | None | None | None | Osteoplastic flap procedure with fat obliteration of the sinus | None | |||
| 2 | Pneumocele vs. pneumosinus dilatans: review of the literature with a case of frontal sinus pneumocele | Acar M. et al. [42] (2004) | Male | 23 | No | None | None | None | Surgery refused by the patient | None |
| 3 | Enlargement of Frontal Sinus, Case Report | Andejani D. et al. [43] (2018) | Male | 26 | Yes | None | None | None | FESS and Open Reshaping of the Anterior Table | No evident recurrence |
| 4 | Frontal Sinus Pneumocele Associated with Respiratory Epithelial Adenomatoid Hamartoma and Nasal Polyps | Gu Z. et al. [44] (2011) | Male | 32 | Yes | None | Respiratory Epithelial Adenomatoid Hamartoma, Nasal Polyps | None | Endoscopic Sinus Surgery | Postoperative headache disappearance |
| 5 | Spontaneous pneumocephalus associated with pneumocele of the frontal sinus | Park CY. et al. [37] (2010) | Male | 35 | No | None | None | Pneumocephalus | Conservative Treatment | Complete resolution of symptoms and pneumocephalus |
| 6 | Pneumocele of the frontal sinus producing orbital roof defect: case report and review of literature | Abdel-Aal AK. et al. [36] (2008) | Female | 31 | Yes | None | Type III frontal recess air cell | Orbital roof defect | Large left frontal endoscopic sinusotomy and resection of the obstructing air cells; frontal sinus stent insertion | None |
| 7 | A case of Orbital Emphysema Associated with Frontal Sinus Pneumocele | Sasaki T. et al. [39] (2013) | Female | 67 | No | None | None | Orbital Emphysema | Left Frontal Craniotomy | No appearance of an orbital emphysema |
| 8 | Post-traumatic Pneumocele of the Frontal Sinus | Karadag D. et al. [45] (2008) | Male | 46 | No | Head trauma 21 years prior* | None | None | Surgery refused by the patient | None |
| 9 | Pneumocele—A rare Cause of Air in the Orbit | Boulos PR. et al. [46] (2004) | Male | 52 | Yes | Nasal fracture at age 7 | None | Proptosis and Hypoglobus | Anterior Orbitotomy and Endoscopic sinusotomy | Decrease of the exophthalmos |
| 10 | Surgical Correction of an Extensive Skull Base Defect as a Result of Pneumocele | Ramprasad VH et al. [35] (2016) | Male | 54 | No | None | None | Pneumocephalus |
48-h bed rest Surgery: the posterior table defect reconstruction with a pericranial flap |
No recurrence of pneumocephalus |
| 11 | Pneumocele of the frontal and sphenoidal sinuses | Jarvis JF. et al. [47] (1974) | Male | 18 | No | None | Dilated sphenoidal sinuses, Orbital and Frontal Subcutaneous Aerocele | Orbital swelling | Surgery: external Frontoethmoidectomy Incision, Opening into the Nose and its Drainage | No sign of swelling |
| 12 | Frontal sinus pneumocele | Eskandary H. et al.[48] (1999) | Male | 37 | No | None | None | Frontal bossing | Surgery: the removal of the anterior wall of the frontal sinus | 3 years, no complication, appropriate contour of forehead |
*Authors add that relationship between head trauma and the frontal pneumocele is not clear
The silent sinus syndrome was diagnosed in 8 patients, 4 men and 4 women, The mean age of diagnosis was 45.4 years (the youngest patient was 31, the oldest was 75) (Fig. 2A, B).
Fig. 2.
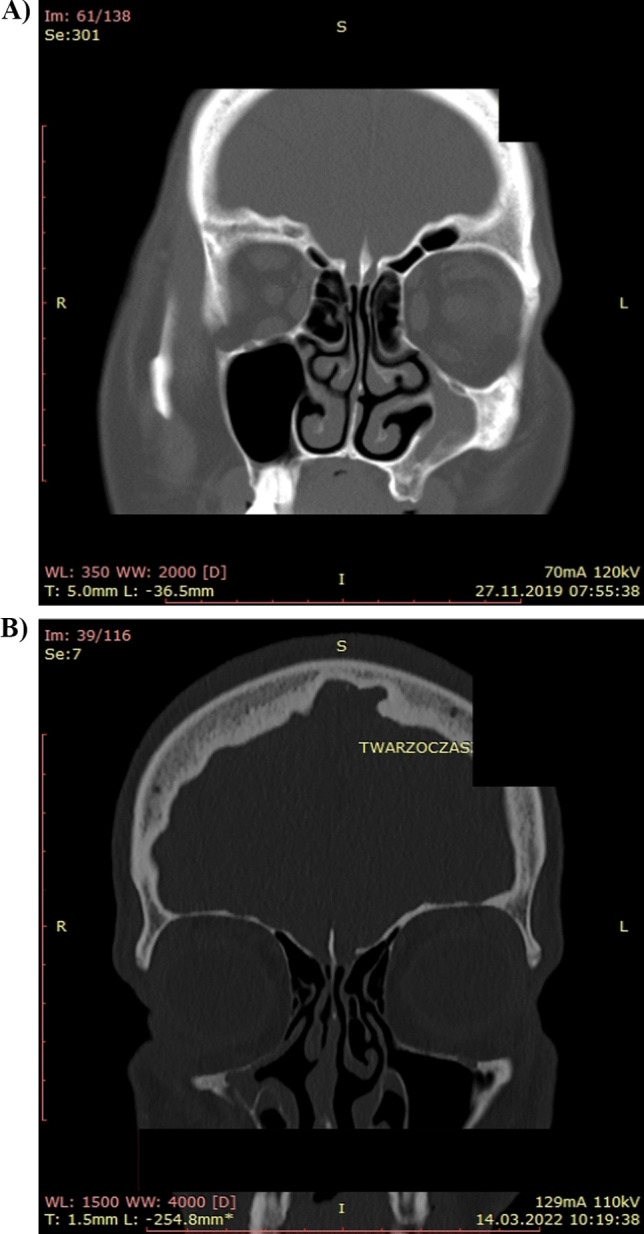
CT images, A–B show the silent sinus syndrome involving the maxillary sinus. A 58-year-old female with SSS of the left maxillary sinus. B 40-year-old female with SSS of the right maxillary sinus
In the patients with SSS, the problem concerned the maxillary sinuses. All the patients were treated endoscopically, each time anteroethmidectomy of the diseased maxillary sinus was performed, ensuring its proper drainage.
In March 2022, a 32-year-old man was admitted to the Department of Laryngology and Laryngological Oncology in Katowice–Ochojec, reporting tissue bulging in the right frontal area. The skin on the forehead was pale and painless. With stronger pressure, defects were felt in the scale of the frontal bone. The patient reported headaches when the ambient temperature changed. Since 2017, he had had frequent sinus infections in the fall and winter period. In October 2019, he noticed a concavity of tissues in the glabella area sized 2 × 2 cm.
After the secretion was blown from the nasal cavity, there was swelling of the lower eyelid of the right eye. On September 20, 2020, the patient was qualified for plastic surgery of the septum. The operation was uneventful. After the procedure, at the beginning of 2020, there was swelling in the frontal area that was gradually increasing.
The patient did not report any comorbidities, including atopy. Outpatient diagnostics for microvasculitis did not confirm the disease.
CT and MRI showed defects in the anterior and posterior walls of the frontal sinus (Fig. 3 A, B). The airiness of the paranasal sinuses and the patency of the ostiomeatal complexes were preserved. Bacteriological examination of the nasal cavity revealed the growth of the physiological bacterial flora and Candida fungi. Endoscopic examination of the nasal cavity showed no abnormalities. Pneumocele was diagnosed and the patient was offered endoscopic surgical treatment consisting in widening the right frontal sinus ostium. Until the publication preparation, the patient had not consented to surgery.
Fig. 3.

MRI (A) and CT (B) images show the enlargement of the frontal sinus with bone thining
On August 16th 2022, after obtaining the patient’s consent, a decision was made to perform frontal sinus ostial dilatation. Bilateral balloon sinuplasty was performed under general anesthesia, under negative pressure, under control of the navigation (NuVent EM Sinus Dilatation System, Frontal 6 × 17 mm, Medtronic). During the procedure, after decontamination of the nasal vestibule skin, bacteriological material was collected on both sides from the middle nasal meatus for culture examination in aerobic and anaerobic conditions. The patient’s condition after the surgery was very good, he did not report any nasal bleeding or pain. Methicillin-susceptible Staphylococcus epidermidis was isolated in all four bacteriological studies. The patient was instructed to stay under constant laryngological observation.
Discussion
The authors of the study present rare diseases involving deformation of the paranasal sinuses, which, if incorrectly diagnosed, may surprise the surgeon and lead to postoperative complications. The literature review suggests that pneumocele not caused by head trauma or comorbidities is rare. So far, the cause of the disease has not been identified and no treatment guidelines have been developed. Our literature review found 12 papers describing 13 patients with pneumocele of the frontal sinus. In only three cases, endoscopic sinus surgery was sufficient, the remaining cases required osteotomy and reconstruction of the damaged sinus wall. Two cases were complicated by pneumocephalus, and three involved orbital lesions.
Pneumocele does not give symptoms for a long time, hence perhaps the reason for such a rare diagnosis of the disease. Similarly, in the early stage of SSS, the patient does not report any symptoms. In the material collected by the authors, the silent sinus syndrome was in all cases accompanied by inflammatory lesions in other sinuses and the patients manifested symptoms typical of CRS, which facilitated the diagnosis of SSS. In SSS, without facial deformity and diplopia, treatment consists in restoring proper drainage of the diseased sinus [22, 23]. When the disease is advanced, reconstruction of the superior wall of the maxillary sinus is considered [24–28].
It is much more difficult to deal with excessive distension of the frontal sinus, PD and pneumocele. The unknown cause of gas accumulation in the sinus translates to difficulties in making a treatment decision. In the case of bone deformity of the scales of the frontal bone in PD, the anterior table of the frontal sinus is removed.
The bone fragment can be secured with low profile titanium mini-plates [29–32].
Patel et al. presented surgical management of the excessively distended frontal sinus (without local defects) depending on the patency of the nasofrontal duct, recommending endoscopic restoration of function in the absence of a cosmetic defect. In contrast, frontal bossing requires an open procedure [33–35]. After correcting the shape of the frontal bone scales, the sinus mucosa is removed by filling the sinus lumen with autogenous bone, adipose tissue or hydroxyapatite.
Due to its rarity, there are no set treatment standards for pneumocele. There are reports of endoscopic widening of the frontal sinus ostium without disturbing the continuity of the mucosa and removing the bony partitions separating the frontal recess from supraorbital cells, intersinus septal cells, and frontal recess cells [36, 37]. Similarly, the authors of the study proposed endoscopic surgery to widen the frontal sinus ostium.
The limitation of our observations was the low recognition of SSS and pneumocele in the daily clinical practice of an ENT specialist and a short period of observation of patients after surgery. The presented cases of rare diseases of the paranasal sinuses may surprise every rhinologist performing endoscopic operations. It should be noted that in approximately 25% of patients with symptomatic frontal sinus pneumocele having comorbid intracranial pathology, the most common is meningioma [38–40].
Paranasal sinus diseases affect about 10.9% of the European population [41], the number of operations is increasing, and therefore, the chance of encountering SSS or PD in everyday practice is real.
Acknowledgements
Not applicable.
Abbreviations
- SSS
Silent sinus syndrome
- PD
Pneumosinus dilatans
- CT
Computed tomography
- CRS
Chronic rhinosinusitis
- MRI
Magnetic resonance imaging
Author contributions
GS-M: idea for the study, methodology, validation, formal analysis, investigation, and original draft preparation, MK: methodology, data curation, review preparation, and visualization, KG: methodology, data curation, and review preparation, OK-B: software, sources, and data curation, MM: methodology, investigation, review preparation and supervision, BK: validation, supervision. All authors contributed to the paper and have read and agreed to the published version of manuscript.
Funding
No funding was received for conducting this study.
Availability of data and materials
The data sets used and/or analysed during the current study are either included in this published article or are available from the corresponding author on reasonable request.
Declarations
Conflict of interest
The authors have no conflict of interest to declare.
Ethics approval
Ethical approval was waived by the local Ethics Committee of Medical Univeristy os Silesia.
Consent
Patients signed informed consent regarding publishing their data and photographs.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Buono LM. The silent sinus syndrome: maxillary sinus atelectasis with enophthalmos and hypoglobus. Curr Opin Ophtalmol. 2004;15(6):486–489. doi: 10.1097/01.icu.0000142510.68451.32. [DOI] [PubMed] [Google Scholar]
- 2.Freiser ME, McCoy J, Shaffer AD, Stapleton AL. Silent sinus syndrome in children. Int J Pediatr otorhinolar. 2020;134:110034. doi: 10.1016/j.ijporl.2020.110034. [DOI] [PubMed] [Google Scholar]
- 3.Farneti P, Sciarretta V, Macri G, Piccin O, Pasquini E. Silent sinus syndrome and maxillary sinus atelectasis in children. Int J Pediatr Otorhinolaryngol. 2017;98:150–157. doi: 10.1016/j.ijporl.2017.05.005. [DOI] [PubMed] [Google Scholar]
- 4.Hunt SM, Tami TA. Sinusitis-induced enophthalmos: the silent sinus syndrome. ENT Ear Nose Throat J. 2000;79(8):576, 579–581, 584. [PubMed] [Google Scholar]
- 5.Kass ES, Salman S, Rubin PA, Weber AL, Montogmery WW. Chronic maxillary atelectasis. Ann Otol Rhinol Laryngol. 1997;106(2):109–116. doi: 10.1177/000348949710600204. [DOI] [PubMed] [Google Scholar]
- 6.Gillman GS, Schaitkin BM, May M. Asymptomatic enophthalmos: the silent sinus syndrome. Am J Rhinol. 1999;13:459–462. doi: 10.2500/105065899781329629. [DOI] [PubMed] [Google Scholar]
- 7.Davidson JK, Soparkar CN, Williams JB, Patrinely JR. Negative sinus pressure and normal predisease imaging in silent sinus syndrome. Arch Ophthalmol. 1999;117(12):1653–1654. [PubMed] [Google Scholar]
- 8.Antonelli PJ, Duvall AJ, Teitelbaum SL. maxillary sinus atelectasis. Ann Otol Rhinol Laryngol. 1992;101(12):977–981. doi: 10.1177/000348949210101203. [DOI] [PubMed] [Google Scholar]
- 9.McArdle B, Perry C. Ethmoid silent sinus syndrome causing inward displacement of the orbit: case report. J Laryngol Otol. 2010;124(2):206–208. doi: 10.1017/s0022215109990521. [DOI] [PubMed] [Google Scholar]
- 10.Naik RM, Khemani S, Saleh HA. Frontal silent sinus syndrome. Otolaryngol Head Neck Surg. 2013;148(2):354–355. doi: 10.1177/0194599812466646. [DOI] [PubMed] [Google Scholar]
- 11.Benjamin CE. Pneumosinus frontalis dilatans. Acta Otolaryngol. 1918;1:412–422. doi: 10.3109/00016481809122008. [DOI] [Google Scholar]
- 12.Ricci JA. Pneumosinus dilatans: over 100 years without an etiology. J Oral Maxillofac Surg. 2017;75(7):1519–1526. doi: 10.1016/j.joms.2017.02.010. [DOI] [PubMed] [Google Scholar]
- 13.Lombardi G, Passerini A, Cecchini A. Pneumosinus dilatans. Acta Radiol Diagn (Stockh) 1968;7(6):535–542. doi: 10.1177/028418516800700609. [DOI] [PubMed] [Google Scholar]
- 14.Pospisil OA, Balmer MC. Pneumosinus dilatans. Br J Oral Maxillofac Surg. 1988;26(5):375–380. doi: 10.1016/0266-4356(88)90089-7. [DOI] [PubMed] [Google Scholar]
- 15.Zhao C, Zhao Y, Yang J, Wang Z. Two rare cases of maxillary pneumocoele. Br J Oral Maxillofac Surg. 2019;57(6):590–593. doi: 10.1016/j.bjoms.2019.01.026. [DOI] [PubMed] [Google Scholar]
- 16.Kiroglu Y, Karabulut N, Sabir NA, Ygaci AB, Gakmak V, Ozguler U. Pneumosinus dilatans and multiplex: report of three rare cases and review of the literature. Dentomaxillofacial Radiol. 2007;36(5):298–303. doi: 10.1259/dmfr/59290441. [DOI] [PubMed] [Google Scholar]
- 17.Urken ML, Soon PM, Lawsen W, Edelstein D, Weber AL, Iller HF. Abnormally large frontal sinus. Nomenclature, pathology and symptoms. Laryngoscope. 1987;97(5):606–611. doi: 10.1288/00005537-198705000-00014. [DOI] [PubMed] [Google Scholar]
- 18.Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. doi: 10.4193/rhin20.600. [DOI] [PubMed] [Google Scholar]
- 19.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–536. doi: 10.7326/0003-4819-155-8-201110180-00009. [DOI] [PubMed] [Google Scholar]
- 21.Stryjewska-Makuch G, Goroszkiewicz K, Szymocha J, Lisowska G, Misiołek M. Etiology, early diagnosis and proper treatment of silent sinus syndrome based on review of the literature and own experience. J Oral Maxillofac Surg. 2022;80(1):113.e1–113.e8. doi: 10.1016/j.joms.2021.08.166. [DOI] [PubMed] [Google Scholar]
- 22.Pawar SS, Hong S, Poetker DM. Delayed presentation of silent sinus syndrome after orbital trauma. Am J Otolaryngol. 2010;31(1):61–63. doi: 10.1016/j.amjoto.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 23.Sivasubramaniam R, Sacks R, Thornton M. Silent sinus syndrome: dynamic changes in the position of the orbital floor after restoration of normal sinus pressure. J Laryngol Otol. 2011;125(12):1239–1243. doi: 10.1017/s0022215111001952. [DOI] [PubMed] [Google Scholar]
- 24.Ferri A, Ferri T, Sesenna E. Bilateral silent sinus syndrome: case report and surgical solution. J Oral Maxillofac Surg. 2012;70(1):e103–e106. doi: 10.1016/j.joms.2011.08.008. [DOI] [PubMed] [Google Scholar]
- 25.Clarós P, Ahmed H, Minka Ngom EG, Clarós A. Le silent sinus syndrome: reconstruction orbitaire par implant Medpor [The silent sinus syndrome: A reconstruction of the orbital floor with Medpor implant] Rev Laryngol Otol Rhinol (Bord) 2015;136(1):37–40. [PubMed] [Google Scholar]
- 26.Baig MZ, Weber JF, Bhora F, Al Shetawi AH. Surgical advances in the management of the silent sinus syndrome: our experience and review of the literature. J Oral Maxillofac Surg. 2020;78(12):2289–2295. doi: 10.1016/j.joms.2020.07.026. [DOI] [PubMed] [Google Scholar]
- 27.Clarós P, Sobolewska AZ, Cardesa A, Lopez-Fortuny M, Claros A. Silent sinus syndrome: combined sinus surgery and orbital reconstruction—report of 15 cases. Acta Otolaryngol. 2019;139(1):64–69. doi: 10.1080/00016489.2018.1542161. [DOI] [PubMed] [Google Scholar]
- 28.Cohn JE, Sokoya M, Hararah M, Kadakia S, Ducic Y. Management of enophthalmos from silent sinus syndrome with a customized orbital implant. Otoral Case Rep. 2018;8:17–19. [Google Scholar]
- 29.Ricci JA, Desai NS, Vendemia N. Correction of a contour deformity associated with frontal pneumosinus dilatans using surgical navigation technology. J Oral Maxillofac Surg. 2015;73(3):529–533. doi: 10.1016/j.joms.2014.08.023. [DOI] [PubMed] [Google Scholar]
- 30.Taub PJ, Narayan P. Surgical navigation technology for treatment of pneumosinus dilatans. Cleft Palate Craniofac J. 2007;44(5):562–566. doi: 10.1597/06-144.1. [DOI] [PubMed] [Google Scholar]
- 31.Galiè M, Consorti G, Clauser LC, Kawamoto HK. Craniofacial surgical strategies for the correction of pneumosinus dilatans frontalis. J Craniomaxillofac Surg. 2013;41(1):28–33. doi: 10.1016/j.jcms.2012.05.016. [DOI] [PubMed] [Google Scholar]
- 32.Bouguila J, Rejeb MB, Omezzine M, et al. Pneumosinus dilatans: rare cause of slowly changing frontal contours. Aestet Surg J. 2015;35(3):47–53. doi: 10.1093/asj/sju045. [DOI] [PubMed] [Google Scholar]
- 33.Patel AC, Hammoudeb JA, Urata MM. Pneumosinus dilatans: a rare cause of frontal sinus expansion-case report and review of literature. J Oral Maxillofac Surg. 2008;66(11):2380–2386. doi: 10.1016/j.joms.2008.06.075. [DOI] [PubMed] [Google Scholar]
- 34.Tellado MG, Mendez R, Lopez-Cedrum JL, Fantini M, Martín-Sastre R, Somoza I, et al. Pneumosinus dilatans of frontal and ethmoidal sinuses;case report. J Craniomaxillofac Surg. 2002;30(1):62–64. doi: 10.1054/jcms.2001.0269. [DOI] [PubMed] [Google Scholar]
- 35.Ramprasad VH, Woodard CR, Jang DW. Surgical correction of an extensive skull base defect as a result of pneumocele. J Craniofac Surg. 2016;27(1):163–165. doi: 10.1097/scs.0000000000002315. [DOI] [PubMed] [Google Scholar]
- 36.Abdel-Aal AK, Abayazeed AH, Raghuram K, Curé JK. Pneumocele of the frontal sinus producing orbital roof defect: case report and review of literature. Am J Otolaryngol. 2010;31(3):202–204. doi: 10.1016/j.amjoto.2009.01.001. [DOI] [PubMed] [Google Scholar]
- 37.Park CY, Kim KS. Spontaneous pneumocephalus associated with pneumocele of the frontal sinus. Cephalalgia. 2010;30(11):1400–1402. doi: 10.1177/0333102410378047. [DOI] [PubMed] [Google Scholar]
- 38.Desai NS, Saboo SS, Khandelwal A, Ricci JA. Pneumosinus dilatans: is it more than an aesthetic concern? J Craniofac Surg. 2014;25(2):418–421. doi: 10.1097/scs.0000000000000694. [DOI] [PubMed] [Google Scholar]
- 39.Sasaki T, Yamoto T, Fujita K, Nakao N. A case of orbital emphysema associated with frontal sinus pneumocele. J Neurol Surg Rep. 2013;74(1):54–56. doi: 10.1055/s-0033-1347903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Timms S, Lakhani R, Connor S, Hopkins C. Complex frontal Pneumosinus dilatans associated with meningioma: a report of two cases and associated literature review. J Neurol Surg Rep. 2017;78(3):e97–e100. doi: 10.1055/s-0037-1600916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hastan D, Fokkens WJ, Bachert C, Newson RB, Bislimovska J, Bockelbrink A, et al. Chronic rhinosinusitis in European underestimated disease. A GA2LEN study. Allergy. 2011;66(9):1216–1223. doi: 10.1111/j.1398-9995.2011.02646.x. [DOI] [PubMed] [Google Scholar]
- 42.Acar M, Yucel A, Degirmenci B, Yilmaz MD, Albayrak R. Pneumocele vs. Pneumosinus dilatans: review of the literature with a case of frontal sinus pneumocele. Tohoku J Exp Med. 2004;202(4):295–297. doi: 10.1620/tjem.202.295. [DOI] [PubMed] [Google Scholar]
- 43.Andejani D, Mrad MA. Enlargement of Frontal Sinus, Case Report. Aesthetic Plast Surg. 2018;42(4):1013–1018. doi: 10.1007/s00266-018-1106-1. [DOI] [PubMed] [Google Scholar]
- 44.Gu Z, Cao Z. Frontal sinus pneumocele associated with respiratory epithelial adenomatoid hamartoma and nasal polyps. Otolaryngol Head Neck Surg. 2012;147(1):177–178. doi: 10.1177/0194599811432232. [DOI] [PubMed] [Google Scholar]
- 45.Karadag D, Calisir C, Adapinar B. Post-traumatic pneumocele of the frontal sinus. Korean J Radiol. 2008;9(4):379–381. doi: 10.3348/kjr.2008.9.4.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Boulos PR, Bernardino CR, Rubin PA. Pneumocele–a rare cause of air in the orbit. Am J Ophthalmol. 2004;138(1):168–169. doi: 10.1016/j.ajo.2004.02.054. [DOI] [PubMed] [Google Scholar]
- 47.Jarvis JF. Pneumocele of the frontal and sphenoidal sinuses. J Laryngol Otol. 1974;88(8):785–793. doi: 10.1017/s0022215100079354. [DOI] [PubMed] [Google Scholar]
- 48.Eskandary H, Reihani KH. Frontal sinus pneumocele. A case report. Int J Oral Maxillofac Surg. 1999;28(3):179–180. doi: 10.1016/S0901-5027(99)80133-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data sets used and/or analysed during the current study are either included in this published article or are available from the corresponding author on reasonable request.