

Abstract
Background
Acupuncture has become one of the most popular alternative medical treatments in the world. However, if the needle is inserted incorrectly into the body, various adverse events can occur and, in such cases, the needle should be removed. Acupuncture needles are very thin and fragile, making them difficult to detect and to confirm breakage or residual needle fragments during surgery. We report a case of a patient's self-placed acupuncture needle migrating into the cervical spinal canal and its surgical removal. We used cone-beam computed tomography in the hybrid operating room to confirm that the needle was removed in its entirety.
Case presentation
A 37-year-old man presented with neck pain and gait disturbance.
While he was self-acupuncturing, an acupuncture needle accidentally broke, and the remaining part of the needle penetrated and made contact with the cervical spinal cord. Cervical spine radiographs showed a metallic foreign body between the C1 and C2 spinous processes in the direction of the anterior cervical spine. Computed tomography images revealed that the acupuncture needle was penetrating the spinal canal and was in contact with the cervical cord. The acupuncture needle was removed under general anesthesia. The use of cone-beam computed tomography in the hybrid operating room allowed intraoperative confirmation that there was no breakage during needle removal, and no needle fragments were left behind. His symptoms disappeared without any complications after the operation.
Conclusion
To the best of our knowledge, this is the first report of the removal of an acupuncture needle that migrated into the cervical spinal canal using cone-beam computed tomography in a hybrid operating room. Intraoperative cone-beam computed tomography is useful in patients with small, fragile foreign bodies for confirmation of the location of the object and to check for the presence of residual fragments.
Keywords: Acupuncture, Cervical cord, Cone-beam computed tomography, Foreign body, Hybrid operating room, Spinal canal
Introduction
Acupuncture is a form of traditional East-Asia medicine that treats musculoskeletal pain by applying needles to specific points on the body; the technique is now used throughout the world [1]. Several injuries have been reported as complications of acupuncture [2], [3], especially in the cervical region. Reports include iatrogenic injuries with needle migration into the medulla oblongata and cervical spinal cord [4], [5]. Acupuncture needles are very thin and fragile, making them difficult to detect in imaging studies and difficult to determine whether their surgical removal is complete. We report a case in which a patient performed acupuncture on himself, and a broken acupuncture needle migrated into the cervical spinal canal. Complete surgical removal of the needle was confirmed by cone-beam computed tomography (CT) in a hybrid operating room.
Case presentation
A 37-year-old male presented to our institute with chief complaints of neck pain and gait disturbance. He had been suffering from neck pain for a long time, and had sought treatment at an acupuncture clinic. He decided to try it by himself, bought acupuncture needles on the internet, and started to use them. After performing the procedure several times on his own, the acupuncture needles were accidentally broken and remained in his neck. His local doctor instructed him to consult a spinal surgeon, but the patient chose not to do so and continued with several self-treatments. A few days after his final self-treatment, he presented to another hospital because of neck pain and weakness in the lower extremities. He was then referred to our hospital, and 5 days later he visited our department. He reported that the neck pain was mild, and on physical examination, there was no limitation in the range of cervical motion. His symptoms were diagnosed as Brown–Sequard syndrome (hypesthesia of the right side of the body and weakness of the left lower extremity) and a droopy left eyelid suggestive of Hornell's syndrome. Lateral radiographs of the cervical spine showed that the acupuncture needle had entered the cervical canal between the C1 and C2 spinous processes (Fig. 1). Cervical spine CT angiogram and CT myelogram revealed that the acupuncture needle had penetrated the cervical spinal canal and the dura mater, contacting the cervical spinal cord (Fig. 2). Preoperative imaging showed no hematoma, abscess, or findings suggestive of CSF leakage. Removal of the foreign body was performed in the prone position under general anesthesia in a hybrid operating room containing a cone-beam CT system. A 5-cm incision was made in the midline of the neck, exposing the C1 posterior arch and C2 spinous process, and finally the needle tip was found (Fig. 3a). The needle was carefully extracted without any spinal fluid leakage, bleeding, or apparent breakage of the needle (Fig. 3b). Because acupuncture needles are very thin, cone-beam CT was used to check for residual needle fragments. After confirming the absence of any remaining needle fragments (Fig. 4), the surgery was completed. Preoperative symptoms improved, and the patient was discharged symptom-free 10 days after surgery.
Fig. 1.

Lateral cervical spine radiograph showing the barely discernible embedded acupuncture needle (white arrow).
Fig. 2.
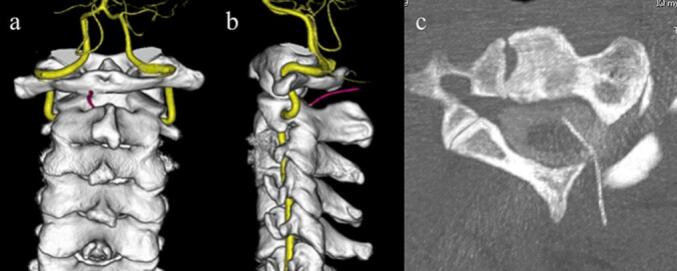
Three-dimensional computed tomography (CT) images demonstrate the orientation of the acupuncture needle from between the C1 posterior arch and C2 spinous process to the anterior cervical spine (a, b). Axial CT myelogram shows that the acupuncture needle penetrated the dura mater and was in contact with the cervical spinal cord.
Fig. 3.
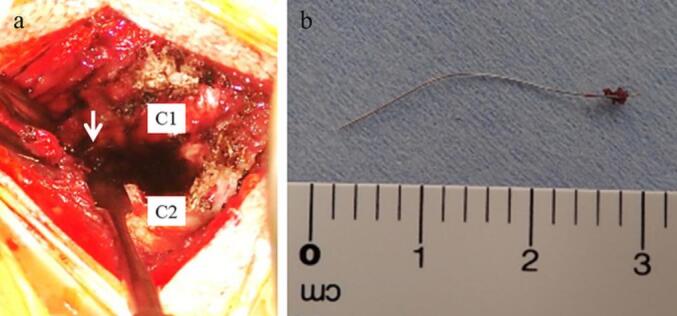
Intraoperative photograph showing that the acupuncture needle (white arrow) was barely visible between C1 and C2 on the left side (a). Photograph of the removed acupuncture needle (b).
Fig. 4.

Cone-beam computed tomography in a hybrid operating room enabled intraoperative confirmation that no broken or residual acupuncture needles remained (left, sagittal view; right, axial view).
Consent for publication was obtained from the patient.
Discussion
Cases of cervical foreign bodies have been reported [6], [7], and there have also been reports of acupuncture needles straying from the head into the cervical spine. In some instances, the needles had been self-inserted [3]. With the spread of the internet, similar cases are expected to occur in the future.
In this case, the clinical features of contact between the foreign body and the spinal cord were symptoms of Horner's and Brown–Sequard syndromes. Because of the reported delayed onset [8], the risk of infection [2], and hematoma [3], improperly embedded acupuncture needles should be removed as soon as possible before symptoms appear or become severe.
Previous reports have described cases of spinal fluid fistulas caused by acupuncture needles, and caution is warranted in their removal [9]. Fortunately, no spinal fluid leak was observed after the needle extraction, and no postoperative hypomyelination symptoms were noted in this case. Meningitis was also a concern, but there were no such symptoms.
Intraoperative problems include the fact that needles are very thin and fragile, making them undetectable, and they can be damaged with pieces left behind during attempts at removal. In this case, we were able to confirm intraoperatively that there were no acupuncture residuals by using cone-beam CT in a hybrid operating room. CT is effective in detecting foreign bodies, especially metals, and their relationship to tissues such as blood vessels and nerves [10]. Cone-beam CT may be very useful in the removal of such small foreign bodies.
Conclusion
We provide the first report of the removal of an acupuncture needle that migrated into the cervical spinal canal using cone-beam CT in a hybrid operating room. Intraoperative cone-beam CT may be useful in locating foreign bodies and confirming the presence of residual fragments.
Declaration of competing interest
None.
Acknowledgment
We thank Andrea Baird, MD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
References
- 1.Kaptchuk T.J. Acupuncture: theory, efficacy, and practice. Ann. Intern. Med. 2002;136:374–383. doi: 10.7326/0003-4819-136-5-200203050-00010. [DOI] [PubMed] [Google Scholar]
- 2.Bang M.S., Lim S.H. Paraplegia caused by spinal infection after acupuncture. Spinal Cord. 2006;44:258–259. doi: 10.1038/sj.sc.3101819. [DOI] [PubMed] [Google Scholar]
- 3.Eghbal K., Ghaffarpasand F. An acute cervical subdural hematoma as the complication of acupuncture: case report and literature review. World Neurosurg. 2016;95(616):e11–e13. doi: 10.1016/j.wneu.2016.08.090. [DOI] [PubMed] [Google Scholar]
- 4.Miyamoto S., Ide T., Takemura N. Risks and causes of cervical cord and medulla oblongata injuries due to acupuncture. World Neurosurg. 2010;73:735–741. doi: 10.1016/j.wneu.2010.03.020. [DOI] [PubMed] [Google Scholar]
- 5.Fang X., Tian Z., Xie B., Guo H. Removal of an acupuncture needle accidentally broken in the neck. Asian J. Surg. 2019;42:582–583. doi: 10.1016/j.asjsur.2018.12.017. [DOI] [PubMed] [Google Scholar]
- 6.Nathoo N., Sarkar A., Varma G., Mendel E. Nail-gun injury of the cervical spine: simple technique for removal of a barbed nail. J. Neurosurg. Spine. 2011;15:60–63. doi: 10.3171/2011.3.SPINE10718. [DOI] [PubMed] [Google Scholar]
- 7.Arizumi F., Inoue S., Tachibana T., Maruo K., Yoshiya S. A sewing needle in contact with the cervical dura mater and vertebral artery: a case report. Medicine. 2016;95 doi: 10.1097/MD.0000000000005764. [Correction: Medicine (Baltimore) 2017;96;e6797.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abumi K., Anbo H., Kaneda K. Migration of an acupuncture needle into the medulla oblongata. Eur. Spine J. 1996;5:137–139. doi: 10.1007/BF00298396. [DOI] [PubMed] [Google Scholar]
- 9.Ulloth J.E., Haines S.J. Acupuncture needles causing lumbar cerebrospinal fluid fistula.Case report. J. Neurosurg. Spine. 2007;6:567–569. doi: 10.3171/spi.2007.6.6.9. [DOI] [PubMed] [Google Scholar]
- 10.Tao K., Xu S., Liu X.-Y., et al. Small metal soft tissue foreign body extraction by using 3D CT guidance: a reliable method. Eur. J. Radiol. 2012;81:3339–3343. doi: 10.1016/j.ejrad.2012.01.002. [DOI] [PubMed] [Google Scholar]