

Abstract
Background
Recent epidemiological research has proven that air pollution triggers the risk of morbidity and mortality due to respiratory and cardiovascular-related diseases. More specifically, fine particulate matter with a diameter of <2.5 μm (PM2.5) can penetrate deeply into the lung and bloodstream, causing critical adverse effects on human health.
Objective
It is found that there is inadequate published research related to the health impact of ambient air pollution in the Middle East region. Some states are well studied, while others are not. This work aims to evaluate the health impact of long-term exposure to PM2.5 in the nine most populated countries in the Middle East region, with a total population of about 363 million (in 2012).
Methods
In this study, the human health impacts in terms of total mortality and the estimated attributable proportion (AP) due to long-term exposure to ambient PM2.5 were estimated using the World Health Organization method and software (AirQ+).
Results
In 2012, the annual median PM2.5 concentrations ranged from 34 μg/m3 in Turkey and Syria to 108 μg/m3 in Saudi Arabia. The total estimated mortalities in the nine most populated countries in the Middle East due to long-term exposure to fine particulate matter was about 152,925 (half of which were residents in Egypt). Moreover, the relative risk (RR) was the highest for Saudi Arabia at 1.8031 and the lowest for Turkey and Syria at a value of 1.1553. The highest AP (central value) was 44.5% in Saudi Arabia, while the lowest was 13.4% in Turkey and Syria.
Conclusions
The results indicate a significant impact of air pollution due to long-term exposure to fine particles resulting in early mortality. This urges the collaboration between the governments and different sectors to adopt stringent regulations to control the anthropogenic sources related to traffic and industrial emissions in the Middle East in order to reduce the health burden of air pollution.
Keywords: air pollution, AirQ+, WHO, health impact, burden of disease, mortality, fine particulate matter, Middle East
1. Introduction
Epidemiological investigations have shown that ambient air pollutants, exacerbated by climate change and other anthropogenic sources, increase the risk of respiratory, cardiovascular diseases, as well as lung cancer and would cause early mortality (1, 2). Air pollution is caused by several ambient harmful substances such as particulate matter (coarse and fine), nitrogen oxide, ozone, sulfur dioxide, and black carbon (3, 4). However, fine particulate matter with a diameter smaller than 2.5 μm (PM2.5) is of critical impact since it can penetrate into the lung's alveoli by inhalation causing adverse effects on human health (5, 6).
The ambient PM2.5 exposure caused about 1.1 million deaths due to ischemic heart diseases (IHD), and 240,000 deaths related to chronic obstructive pulmonary diseases (COPD) in 2012 worldwide (7). Particulate air pollution also directly impacts the material and human welfare such as buildings, historic monuments, paints, vehicles, and solar panels, among others (8, 9). Moreover, studies indicated a significant association between ambient PM2.5 inhalation and the incidence of several health endpoints such as asthma, bronchitis, and lung cancer (LC) related mortalities (10–12).
The Middle East region includes around 16 countries with a total population of 452.7 million in 2020. The long and short-term impact of air pollution on human health has not been well studied in all the countries in the regions. Several research papers have reported on selected adverse impacts on health in Iran (1, 13) and Saudi Arabia (14, 15), but the impact in other countries have not been reported, or are rarely studied (13, 16).
In order to facilitate the estimation of the long and short term health impact due to extensive exposure to air pollution, the World Health Organization (WHO) has developed an air quality health risk assessment impact model (AirQ+) (17, 18). This model is used to evaluate the burden of disease due to different air pollutants such as PM2.5, course particulate (PM10), nitrogen dioxide (NO2), ozone (O3), and black carbon (BC). The software has been used to report on several health endpoints around the world (5, 7, 19, 20).
The main objective of this study is to estimate the long-term impact of PM2.5 pollution exposure in the nine most populated countries in the Middle East (Egypt, Iran, Turkey, Iraq, Saudi Arabia, Yemen, Syria, United Arab Emirates (UAE), and Jordan) during 2012. The outcomes were evaluated in terms of total mortalities, attributable cases, and relative risk using AirQ+ model.
2. Materials and methods
2.1. Study area location
The Middle East (ME) is a geopolitical term that commonly refers to the region that includes around 16 countries with a total population of about 452.7 million in 2020. However, this study involves only the most populated countries with a total population equal or greater than 8 million in 2012 to match the year when PM2.5 levels were reported for all states. These include Egypt, Iran, Iraq, Turkey, Saudi Arabia, Yemen, Syria, United Arab Emirates (UAE), and Jordan which are all labeled with a red circle in Figure 1. The region is characterized by hot and dry climate in general with arid and semi-arid environment in most territories (22).
Figure 1.

Map of the Middle East countries. Red circles indicate the states included in this study (21).
Table 1 lists the nine countries included in this study in order from the most populated to the least which are: Egypt, Iran, Turkey, Iraq, Saudi Arabia, Yemen, Syria, UAE, and Jordan. The total population in 2012 ranged from 82.3 million in Egypt to 8.1 in Jordan.
Table 1.
The population in 2012 of the most populated nine countries in the Middle East selected in this study.
| Country | Population (million) |
|---|---|
| Egypt | 82.3 |
| Iran | 78.9 |
| Turkey | 74.9 |
| Iraq | 33.7 |
| Saudi Arabia | 28.7 |
| Yemen | 25.6 |
| Syria | 22.5 |
| UAE | 8.1 |
| Jordan | 8.1 |
| Total | 362.8 |
2.2. Air quality data
The annual PM2.5 concentrations for the selected countries were adopted from the World Health Organization report (Ambient air pollution: A global assessment of exposure and burden of disease) (7). This is due to the absence of consistent published measured PM2.5 concentrations for each country for the same duration. Table 2 shows the minimum, maximum and median average concentrations of fine particulate matter over the nine selected countries in 2012. It can be seen that the minimum annual PM2.5 concentration has exceeded the annual World Health Organization (WHO) 2006 Air Quality Guideline value of 10 μg/m3 for all the countries. This value has been reviewed and stated by the WHO in 2021 to be 5 μg/m3 which further indicates that there is almost no minimum PM2.5 concentration for safe exposure without inducing risk on the human health. For the long-term PM2.5 exposure health impact in terms of mortality evaluation, relative risk, and the attributable proportion (AP), the annual median PM2.5 concentrations were considered. The rational in this case is to avoid extremities when sudden short-term events take place such as the sandstorms which elevate PM concentration significantly. It is worth noting that some of the countries in this study witness such events, but not the others (23–25). Hence; excluding outlier values is preferred for the sake of outcome comparison on the same basis.
Table 2.
The minimum, median, and maximum annual PM2.5 concentrations in rural and urban areas over the selected countries, adopted from WHO report (7).
| PM 2.5 (μm/m3) rural and urban (2012) | |||
|---|---|---|---|
| Country | Median | Min | Max |
| Egypt | 93 | 50 | 171 |
| Iran | 42 | 27 | 63 |
| Turkey | 34 | 22 | 50 |
| Iraq | 50 | 18 | 141 |
| Saudi Arabia | 108 | 67 | 174 |
| Yemen | 43 | 11 | 173 |
| Syria | 34 | 12 | 98 |
| UAE | 64 | 39 | 104 |
| Jordan | 36 | 24 | 53 |
2.3. Health impact assessment tool
In order to estimate the long-term impact of air pollution due to the exposure to fine particulate matter in the most populated countries in the Middle East, the Air Quality Health Impact Assessment (AirQ+) tool developed by the WHO was used. The software evaluates the mortality and morbidity in terms of several health endpoints such as respiratory diseases, daily hospitalization, lung cancer, COPD and IHD. It can be also used to evaluate the impact of several air pollutants other than PM2.5 which include coarse particulate matter, ozone, black carbon, and nitrogen oxides. The main outcome is the relative risk (RR) which is estimated via the following equation (1):
| (1) |
Figure 2 shows the flow of the steps related to the methodology in this work to obtain the long-term impact of PM2.5 exposure. The input data for each country include the area in km2, the total population in the year of the study, the average annual concentration of the criteria pollutant (in this case PM2.5), and the base line incidence rate (in this case mortality). The output data shall include the relative risk of total mortality, the attributable total number of cases and percentage.
Figure 2.
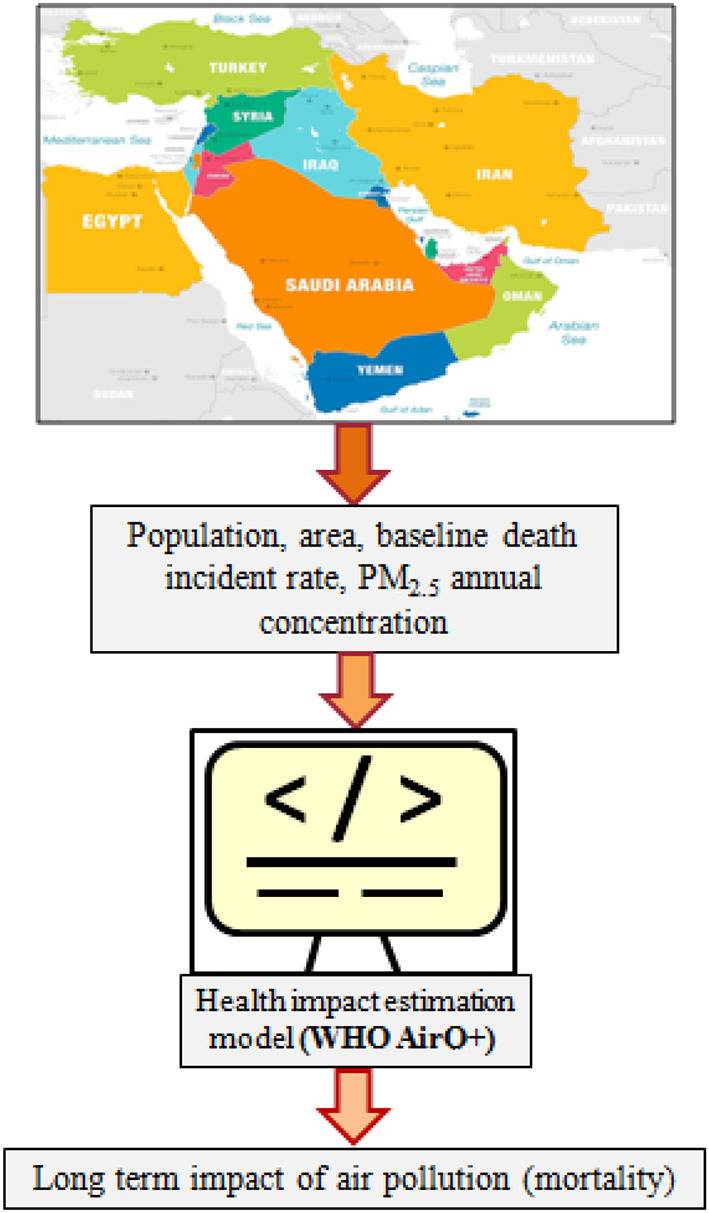
The steps followed in the methodology in this work.
3. Results and discussion
It has been reported that there are several natural sources of air pollution in the Middle East region, such as windblown dust (26, 27), however, intensive anthropogenic activities related to urban development, industrial activities and transportation are the most dominant sources of air pollutants that played a critical role in increasing the air pollution burden of disease (23, 28–30).
Recent studies have reported on the adverse health impacts due to PM2.5 exposure (31–33). In order to better understand the impact of particulate matter on inducing several diseases in human beings, the mechanism shall be briefly described. At concentrations as low as 30 μg/m3, the epidemiological evidence suggests that PM2.5 that contains large number of soluble toxic metals are capable of redox cycling and oxidative stress (34). Oxidative stress refers to any disturbance in the pro- and anti-oxidant balance that would lead to a potential damage, and was first introduced in biology by Sies (35). More specifically, air pollutants contain various free radicals or highly oxidative gases. Upon inhaling the particulate matter, the release of reactive oxygen from lung cells attacks and oxidizes other cell components in the lungs. This leads to tissue, protein, and deoxyribonucleic acid (DNA) damage caused by the inflammatory reaction. The role of fine particulate matter to induce oxidative stress is represented schematically in Figure 3.
Figure 3.
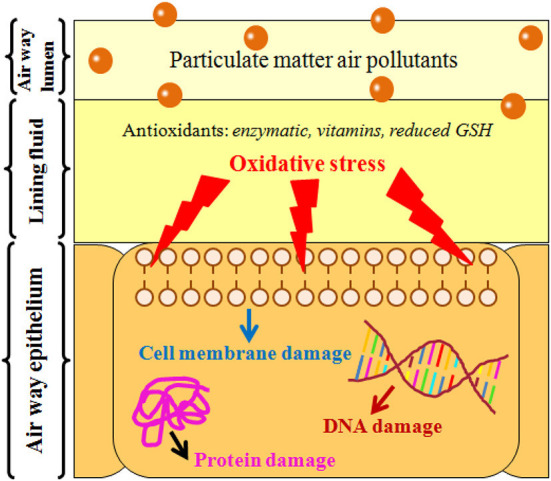
Mechanisms of airway injury by inhaling particulate matter.
It can be shown that the oxidative stress plays a critical role to explain the mechanism of how air pollution adversely impacts human health when they are in contact with human cells and tissues (36). The generated reactive oxidative stress (ROS) overwhelms the antioxidant defenses in the body. Consequently, the ROS causes several pathological consequences due to the reactions that might take place with the DNA, lipids, and proteins in the cells. If these reactions were not stopped, they eventually cause a permanent damage of the cell that ends up with its death (36).
Table 3 shows the relative risk of mortality obtained from AirQ+ due to the long-term exposure to PM2.5. The relative risk indicates the probability of experiencing certain health effect (in this case, mortality) when certain pollutant (in this case, PM2.5) concentration increases at 10 μg/m3 increments (5).
Table 3.
The relative risk (RR) of total mortality due to long term exposure to PM2.5 in the highest populated ME countries.
| Country | Lower | Central | Upper |
|---|---|---|---|
| Egypt | 1.3847 | 1.6475 | 1.9382 |
| Iran | 1.1337 | 1.2122 | 1.2906 |
| Turkey | 1.0987 | 1.1553 | 1.2109 |
| Iraq | 1.1698 | 1.2720 | 1.3756 |
| Saudi Arabia | 1.4686 | 1.8031 | 2.1845 |
| Yemen | 1.1381 | 1.2195 | 1.3009 |
| Syria | 1.0987 | 1.1553 | 1.2109 |
| UAE | 1.2310 | 1.3754 | 1.5259 |
| Jordan | 1.1073 | 1.1692 | 1.2303 |
The results show that the central values of relative risk ranges from 1.1553 for Turkey and Syria to 1.8031 for Saudi Arabia under the median PM2.5 concentration. That indicates that for each 10 μg/m3 increase in PM2.5 concentration, the risk for mortality increases by 80.31% for Saudi Arabia, and so on for other countries. In Iran, the relative risk for total mortality ranged between 1.1337 and 1.2906 over all the country. Similarly, Kermani et al., estimated the short-term effects of ambient air pollution in Iran. They found that PM2.5 had the most significant impact on the health of 19,048,000 residents in eight Iranian cities, causing total mortality of 5,670 out of 87,907 total deaths during a one-year time-period in 2012 (31). Borsi et al. (18), recently studied the health endpoints due to the exposure to several criteria air pollutants (ozone, PM10, SO2, and NO2) in Ahvaz city in Iran using AirQ+ model. They found that the annual cases of cardiovascular mortality due to PM10 exposure during the period 2010-2014 have reached up to 506 deaths yearly. Their results also showed that the number of hospital admissions due to cardiovascular disease related to ambient PM10 exposure was up to 586 during the same period. In another recently published work, Moradi et al. (37), estimated the health effects due to long and short term exposure to PM2.5 in Ardabil/ Iran using AirQ+ model. The first observation was that the PM2.5 average concentration in Ardabil in 2018 was around 15 μg/m3. This value is significantly less than the reported average values in 2012 by the World Health Organization as presented in Table 2 for Iran with an annual PM2.5 concentration range of 22–50 μg/m3. Moreover, the outcome of their research showed that exposure to ambient particulate matter, even at low concentrations, is associated with an increased risk of overall mortality and hospital admissions for respiratory and cardiovascular diseases. More specifically, a total number of deaths due to acute lower respiratory infections (ALRI), COPD, lung cancer, ischemic heart diseases, and stroke on average during the study period were estimated to be 73, 11, 7, 15, and 14; respectively (37).
It is worth noting that there is lack of research in this domain for several countries in the Middle East. In Rome, which is close to the ME region, the attributable proportion cases due to PM2.5 exposure was 16.5% for ischemic heart diseases and 8.5% for chronic obstructive pulmonary diseases mortality in 2015. Moreover, 947 premature deaths due to ischemic heart diseases and 244 due to chronic obstructive pulmonary diseases could have been avoided if PM2.5 concentrations would have not exceeded 10 μg/m3 (5). Moreover, Sicard et al. (20), reported that the relative risk for total mortality was about 1.062 and 1.015 in Iran and France; respectively.
The main sources of PM2.5 in the Middle East region have been attributed to anthropogenic sources which should be controlled and minimized (28, 30, 38). Momtazan et al. (39), drew attention to the adverse health impact due to air pollution and dust storms witnessed in the southwestern part of Iran. Their study investigated the relationship between hospital admissions for cardiovascular diseases and dust storms in Abadan and Khorramshahr (located southwest in Iran) in 2014–2016. They focused on estimating the number of people suffering from cardiovascular diseases attributed to PM10 exposure during the period 2014, 2015, and 2016, which were found to be 237, 259, and 274; respectively. They also reported that there was a significant relationship between PM10 concentrations in dusty days and the cases of cardiovascular diseases in both cities. In a 10-year data study conducted by Dastoorpoor et al. (40), to investigate the relation between air pollution and cardiovascular hospital admissions in Ahwaz/Iran, they found that there was a significant increase in hospital admissions and women's population specially in the case of ozone exposure. Moreover, there was a significant increase in hospital admissions for cardiovascular diseases in the whole population as well as gender and age groups associated with nitrogen dioxide (NO2) and nitrogen monoxide (NO) ambient levels.
A recent review by Nasser et al. (38), identified the major sources of air pollution in the urban cities in the main Middle East countries. In Egypt, the main air pollution sources attributed to human activities were due to traffic, industrial emissions, and burning in the open air. In Jordan, the emissions were mainly related to traffic. In Kuwait and Saudi Arabia, in addition to traffic, the emissions were attributed to industrial oil combustion and power plants emissions. In Lebanon and Turkey, the main sources were related to waste burning and traffic. In Qatar, the sources were attributed to traffic as well as to mega construction projects. In the UAE, air pollution was mainly due to industrial activities as well as traffic and marine activities in the ports. In Iran, emissions from anthropogenic sources were mainly due to transportation, industries and dust storms (41–43).
Moreover, the results show that the relative risk is significantly linked with the annual concentration of PM2.5 as shown in Figure 4.
Figure 4.
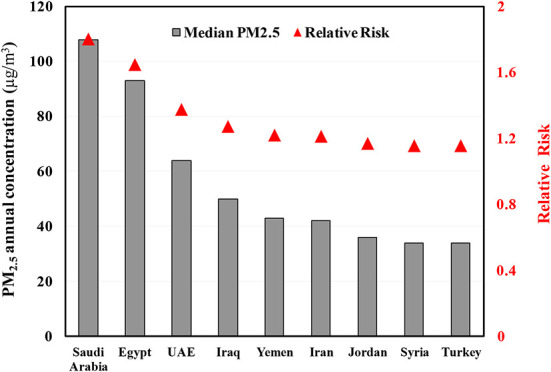
Relation between PM2.5 concentration and the relative risk of total mortality.
The highest risk is corresponding with the highest PM2.5 concentration. This is due to the fact that the RR is proportional with the air pollutant concentration as per the following equation (7):
Where; x is the annual average mean concentration of the air pollutant (in this case PM2.5), xo represents the background concentration of PM2.5 (10 μg/ m3) as per the World Health Organization air quality guidelines, and β is the risk function coefficient.
The results suggest that stringent measures should be taken to reduce the impact of air pollution in the urban context. Several studies suggested the use of clean transportation (30, 44), green vegetation planning of urban cities (45–47), and the use of nanotechnology to remove pollutants from the air (48–50). Among the most efficient feasible strategies to abate particulate pollution is the use of urban trees that require minimum irrigation and care needs and are well suited to grow in any location. These trees can be efficient to reduce particulate matter concentration in the air by acting as barriers for the incoming polluted air flow and by capturing air borne particles over the sticky or structured surface of the leaf (46). Other studies have shown the impact of using clean fuel and electric vehicles in urban cities to reduce the emissions of particulate matter (30). Moreover, the use of catalytic convertor filters embedded with noble nanomaterials has proven to remove around 95% of particulate matter emissions before they are released to the atmosphere (30).
Moreover, Table 4 shows that attributable percentage of total annual mortalities that are linked with long-term exposure to fine particulate ranges from 13.4% for Turkey and Syria to 39.3% for Egypt.
Table 4.
Total mortality due to air pollution in the highest populated ME countries due to PM2.5 exposure.
| Country | Estimated AP (%) | Estimated total annual cases | Estimated cases per 100,000 | Study period | References | ||||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Central | Upper | Lower | Central | Upper | ||||
| Egypt | 27.8 | 39.3 | 48.4 | 52,870 | 74,785 | 92,109 | 133 | 2012 | Current study |
| – | 43,531 | – | (4) | ||||||
| Turkey | 8.9 | 13.4 | 17.4 | 23,177 | 34,683 | 44,934 | 56 | 2012 | Current study |
| – | 32,668 | – | (4) | ||||||
| Iran | 11.8 | 17.5 | 22.5 | 11,114 | 16,499 | 21,220 | 80 | 2012 | Current study |
| – | 26,267 | – | (4) | ||||||
| 6.45 | 5,670 | (2011–2012) | (27) | ||||||
| Iraq | 14.5 | 21.4 | 27.3 | 9,539 | 14,050 | 17,941 | 73 | 2012 | Current study |
| – | 10,085 | – | (4) | ||||||
| Saudi Arabia | 31.9 | 44.5 | 54.2 | 5,861 | 8,181 | 9,960 | 71 | 2012 | Current study |
| – | 8,119 | – | (4) | ||||||
| Yemen | 12.1 | 18.0 | 23.1 | 1,165 | 1,728 | 2,221 | 27 | 2012 | Current study |
| – | 2,411 | – | (4) | ||||||
| Syria | 8.9 | 13.4 | 17.4 | 898 | 1,344 | 1,741 | 18 | 2012 | Current study |
| – | 2,097 | – | (4) | ||||||
| Jordan | 9.7 | 14.5 | 18.7 | 693 | 1,034 | 1,338 | 27 | 2012 | Current study |
| – | 1,483 | – | (4) | ||||||
| UAE | 18.8 | 27.3 | 34.5 | 428 | 621 | 784 | 14 | 2012 | Current study |
| – | 655 | – | (4) | ||||||
The outcomes of AirQ+ software is also shown in Figure 5 for Egypt as an example. The results also indicate that for each 100,000 deaths in Egypt, 133 are attributed to diseases linked with exposure to PM2.5 air pollution.
Figure 5.

An example of the outcomes as per AirQ+ screen for Egypt.
The results in Table 4 were compared with some studies that do not cover the whole country, but rather one city or some cities per research cited (Table 4). For instance, Khaniabadi et al., (17) estimated that the relative risk for total mortality due to PM2.5 exposure in one city in Iran (Khorramabad, 540,000 inhabitants) was in the range of 1.015-1.019. In another study related to Dubai and Abu Dhabi in the UAE (51), it was estimated that 307,667 health care visits due to cardiovascular diseases were attributable to ambient PM10 daily exposure. The total overall estimated mortalities in this work have summed up to 152,925 compared with the World Health Organization report for the same year that summed up to 127,316 from the same 9 countries. The main difference was the lack of accurate demographic data for some countries by age group which caused the exposed population to vary. The lack of research that estimates the health impact of air pollution is mainly due to the lack of accurate measured or published air quality data on regular basis. This has also impacted the fact that there have been no national strategies aiming at assessing and mitigating the adverse health impact of air pollution (38).
4. Conclusions
In conclusion, the air pollution in the Middle East specially where high population with anthropogenic activities prevail have caused critical health issues that increased the burden of disease in the region. However, several countries with high population lack research on the impact of ambient air pollution on human health.
In order to estimate the long-term impact of PM2.5 exposure, the AirQ+ software was used to estimate the total mortality over the nine most populated countries in the Middle East. The results are in alignment with the published data by the World Health Organization for 2012. The highest annual mortalities were found in Egypt, while the lowest in the UAE.
The results of our study can be of substantial importance for researchers, policy makers, medical, public health, and scientific experts. Also, this study can influence the governments for the adoption of laws to minimize air pollution and achieve international air quality standards. The main recommendation is to urge local authorities to propose strict policies to reduce the emissions from traffic and other anthropogenic sources. This can be attained through proper sustainable urban planning, use of new technologies in vehicles, and the encouragement to sue public transportation and clean vehicles.
Moreover, this work draws attention for the need to study the impact of long and short-term exposure to pollution. The obvious lack of published studies in several states in the Middle East, while abundance is available for others such as Iran, urges the research community to investigate widely in this domain.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
RI is the sole author and contributor to this manuscript which includes conceptualization, structuring, and writing of the article.
Abbreviations
AP, Attributable proportion (%); COPD, chronic obstructive pulmonary diseases; DNA, deoxyribonucleic acid; IHD, ischemic heart diseases; ME, Middle East; NO, Nitrogen monoxide; NO2, Nitrogen dioxide; O3, Ozone; PM2.5, Fine particulate matter; PM10, Course particulate matter; ROS, reactive oxidative stress; RR, Relative Risk; UAE, United Arab Emirates; WHO, World Health Organization.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
- 1.Effatpanah M, Effatpanah H, Jalali S, Parseh I, Goudarzi G, Barzegar G, et al. Hospital admission of exposure to air pollution in Ahvaz megacity during 2010–2013. Clin Epidemiol Glob Heal. (2020) 8:550–6. 10.1016/j.cegh.2019.12.001 [DOI] [Google Scholar]
- 2.Goudarzi G, Geravandi S, Idani E, Hosseini SA, Baneshi MM, Yari AR, et al. An evaluation of hospital admission respiratory disease attributed to sulfur dioxide ambient concentration in Ahvaz from 2011 through 2013. Environ Sci Pollut Res. (2016) 23:22001–7. 10.1007/s11356-016-7447-x [DOI] [PubMed] [Google Scholar]
- 3.Hormati M, Mohammadi MJ, Iswanto AH, Mansourimoghadam S, Taifi A, Maleki H, et al. Consequences and health effects of toxic air pollutants emission by industries. J Air Pollut Heal. (2022) 7:95–108. 10.18502/japh.v7i1.8923 [DOI] [Google Scholar]
- 4.Geravandi S, Goudarzi GR, Vousoghi Niri M, Mohammadi MJ, Saeidimehr S. Estimate of cardiovascular and respiratory mortality related to sulfur dioxide pollutant in Ahvaz. J Environ Stud. (2015) 41:341–50. [Google Scholar]
- 5.Amoatey P, Sicard P, De Marco A, Khaniabadi YO. Long-term exposure to ambient PM2, 5. and health impacts in megacity of Rome, Italy. Clin Epidemiol Glob Heal. (2019) 57:49–57. 10.1016/j.cegh.2019.11.009 [DOI] [Google Scholar]
- 6.Nikmanesh Y, Mohammadi MJ, Yousefi H, Mansourimoghadam S, Taherian M. The effect of long-term exposure to toxic air pollutants on the increased risk of malignant brain tumors. Rev Environ Health. (2022) 2022–33. 10.1515/reveh-2022-0033 [DOI] [PubMed] [Google Scholar]
- 7.WHO . Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease, 2016. (2016). Available online at: https://www.who.int/phe/publications/air-pollution-global-assessment/en/ (accessed April 21, 2022).
- 8.Al-Thani H, Koç M, Isaifan RJ. A review on the direct effect of particulate atmospheric pollution on materials and its mitigation for sustainable cities and societies. Environ Sci Pollut Res. (2018) 25:27839–57. 10.1007/s11356-018-2952-8 [DOI] [PubMed] [Google Scholar]
- 9.Fares E, Buffiere M, Figgis B, Haik Y, Isaifan RJ. Soiling of photovoltaic panels in the Gulf Cooperation Council countries and mitigation strategies. Sol Energy Mater Sol Cells. (2021) 231:111303. 10.1016/j.solmat.2021.111303 [DOI] [Google Scholar]
- 10.Bener A, Kamal M, Shanks N. Impact of asthma and air pollution on school attendance of primary school children: are they at increased risk of school absenteeism?. J Asthma. (2007) 44:249–52. 10.1080/02770900701246725 [DOI] [PubMed] [Google Scholar]
- 11.Omidi Y, Sicard P, Takdastan A, Hopke PK, Matthew A, Omidi F, et al. Mortality and morbidity due to ambient air pollution in Iran. Clin Epidemiol Glob Heal. (2018) 7:222–7. [Google Scholar]
- 12.Loxham M, Nieuwenhuijsen MJ. Health effects of particulate matter air pollution in underground railway systems—A critical review of the evidence, Part. Fibre Toxicol. (2019) 16:1–24. 10.1186/s12989-019-0296-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Amini H, Trang Nhung NT, Schindler C, Yunesian M, Hosseini V, Shamsipour M, et al. Short-term associations between daily mortality and ambient particulate matter, nitrogen dioxide, and the air quality index in a Middle Eastern megacity. Environ Pollut. (2019) 254:113121. 10.1016/j.envpol.2019.113121 [DOI] [PubMed] [Google Scholar]
- 14.Abdel-Magid MIM, Abdel-Magid IM. Health quality index for desert cities and populations in Kingdom of Saudi Arabia: A concept paper. Indian J Heal Well-Being. (2019) 10:337–43. [Google Scholar]
- 15.Al-Ahmadi, K, Al-Zahrani, A. NO2 and Cancer Incidence in Saudi Arabia, (2013) 5844–5862. 10.3390/ijerph10115844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Karimzadegan H, Rahmatian M, Farhud D, Yunesian M. Economic valuation of air pollution health impacts in the Tehran area, Iran. Iran J Public Heal. (2008) 37:20–30. [Google Scholar]
- 17.Khaniabadi YO, Sicard P, Khaniabadi AO, Keishams F, Takdastan A, Najafi A, et al. Human and ecological risk assessment : an international air quality modeling for health risk assessment of ambient PM 10, PM 2. 5 and SO 2 in Iran. Hum Ecol Risk Assess 0. (2018) 1–13. [Google Scholar]
- 18.Borsi SH, Goudarzi G, Sarizadeh G, Dastoorpoor M, Geravandi S, Shahriyari HA, et al. Health endpoint of exposure to criteria air pollutants in ambient air of on a populated in Ahvaz City, Iran. Front Public Heal. (2022) 10. 10.3389/fpubh.2022.869656 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Naddafi K, Hassanvand MS, Yunesian M, Momeniha F. Environmental health impact assessment of air pollution in megacity of Tehran. Iran. (2012) 1–7. 10.1186/1735-2746-9-28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sicard P, Khaniabadi YO, Perez S, Gualtieri M, De Marco A. Effect of O3, PM10 and PM2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ Sci Pollut Res. (2019) 26:32645–65. 10.1007/s11356-019-06445-8 [DOI] [PubMed] [Google Scholar]
- 21.World Atlas . How Many Countries are there in The Middle East? (2022). Available online at: https://www.worldatlas.com/articles/which-are-the-middle-eastern-countries.html (accessed April 21, 2022).
- 22.Climate Center. Middle East Climate Fact Sheet (2022). [Google Scholar]
- 23.Roshan DR, Koc M, Isaifan R, Shahid MZ, Fountoukis C. Aerosol optical thickness over large urban environments of the Arabian Peninsula—speciation, variability, and distributions. Atmosphere (Basel). (2019) 10:228–49. 10.3390/atmos10050228 [DOI] [Google Scholar]
- 24.Hussein T, Juwhari H, Al Kuisi M, Alkattan H, Lahlouh B, Al-Hunaiti A, et al. Accumulation and coarse mode aerosol concentrations and carbonaceous contents in the urban background atmosphere in Amman, Jordan. Arab J Geosci. (2018) 11. 10.1007/s12517-018-3970-z [DOI] [Google Scholar]
- 25.Akbari S. Dust storms, sources in the Middle East and economic model for survey it's impacts. Aust J Basic Appl Sci. (2011) 5:227–33. [Google Scholar]
- 26.UNEP (2020). Actions Taken by Governments to Improve Air Quality. Available online at: https://www.unep.org/resources/report/actions-air-quality-global-summary-policies-and-programmes-reduce-air-pollution (accessed March 17, 2022).
- 27.Prakash PJ, Stenchikov G, Kalenderski S, Osipov S, Bangalath H, Jish Prakash P, et al. The impact of dust storms on the Arabian Peninsula and the Red Sea. Atmos Chem Phys. (2015) 15:199–222. 10.5194/acp-15-199-2015 [DOI] [Google Scholar]
- 28.Al-Thani H, Koc M, Isaifan RJ. Investigations on deposited dust fallout in Urban Doha : characterization, source apportionment and mitigation. Environ Ecol Res. (2018) 6:493–506. 10.13189/eer.2018.060510 [DOI] [Google Scholar]
- 29.Roshan DR, Koc M, Abdallah A, Martin-pomares L, Isaifan RJ, Fountoukis C. UV index forecasting under the influence of desert dust : evaluation against surface and satellite-retrieved data. Atmosphere (Basel). (2020) 11:1–17. 10.3390/atmos11010096 [DOI] [Google Scholar]
- 30.Al-Thani H, Koç M, Fountoukis C, Isaifan RJ. Evaluation of particulate matter emissions from non-passenger diesel vehicles in Qatar. J Air Waste Manage Assoc. (2020) 70:228–42. 10.1080/10962247.2019.1704939 [DOI] [PubMed] [Google Scholar]
- 31.Kermani M, Goudarzi G, Shahsavani A, Dowlati M, Asl FB, Karimzadeh S, et al. Estimation of short-term mortality and morbidity attributed to fine particulate matter in the ambient air of eight Iranian cities. Ann Glob Heal. (2018) 84:408–18. 10.29024/aogh.2308 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cohen AJ, Anderson HR, Ostro B, Pandey KD, Krzyzanowski M, Künzli N, et al. The global burden of disease due to outdoor air pollution. J Toxical Environ Heal A. (2005) 68:1301–7. 10.1080/15287390590936166 [DOI] [PubMed] [Google Scholar]
- 33.World Health Organisation . Mortality and burden of disease from ambient air pollution, WHO. (2020). Available online a: https://www.who.int/gho/phe/outdoor_air_pollution/burden_text/en/ (accessed on March 10, 2020).
- 34.Kelly FJ. Oxidative stress: Its role in air pollution and adverse health effects. Occup Environ Med. (2003) 60:612–6. 10.1136/oem.60.8.612 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Sies H. Oxidative stress II. In: Oxidants and Antioxidants. (1991). London, UK: Academic Press, Inc. [Google Scholar]
- 36.Kim B, Lee S, Kim H, Lee E, Hong S. Environmental Changes, Microbiota, and Allergic Diseases, Allergy, Athsma. Immunol Res. (2014) 389–400. 10.4168/aair.2014.6.5.389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Moradi M, Mokhtari A, Mohammadi MJ, Hadei M, Vosoughi M. Estimation of long-term and short-term health effects attributed to PM2.5 standard pollutants in the air of Ardabil (using Air Q+ model). Environ Sci Pollut Res. (2022) 29:21508–16. 10.1007/s11356-021-17303-x [DOI] [PubMed] [Google Scholar]
- 38.Nasser Z, Salalmeh P, Nasser W, Abou Abbas L, Elias E, Leveque A, et al. Outdoor particulate (PM) and associated cardiovascular diseases in the Middle East. Int J Occup Med Environ Health. (2015) 28:641–61. 10.13075/ijomeh.1896.00186 [DOI] [PubMed] [Google Scholar]
- 39.Momtazan M, Geravandi S, Rastegarimehr B, Valipour A, Ranjbarzadeh A, Yari AR, et al. An investigation of particulate matter and relevant cardiovascular risks in Abadan and Khorramshahr in 2014–2016. Toxin Rev. (2019) 38:1–8. 10.1080/15569543.2018.1463266 [DOI] [Google Scholar]
- 40.Dastoorpoor M, Sekhavatpour Z, Masoumi K, Mohammadi MJ, Aghababaeian H, Khanjani N, et al. Air pollution and hospital admissions for cardiovascular diseases in Ahvaz, Iran. Sci Total Environ. (2019) 652:1318–30. 10.1016/j.scitotenv.2018.10.285 [DOI] [PubMed] [Google Scholar]
- 41.Khaefi M, Goudarzi G, Yari AR, Geravandi S, Dobaradaran S, Idani E, et al. An association between ambient pollutants and hospital admitted respiratory cases in Ahvaz, Iran. Fresenius Env Bull. (2016) 25:3955–61. 10.5812/jjcdc.26621 [DOI] [Google Scholar]
- 42.Yari AR, Goudarzi G, Geravandi S, Dobaradaran S, Yousefi F, Idani E, et al. Study of ground-level ozone and its health risk assessment in residents in Ahvaz City, Iran during 2013. Toxin Rev. (2016) 35:201–6. 10.1080/15569543.2016.1225769 [DOI] [Google Scholar]
- 43.Idani E, Geravandi S, Akhzari M, Goudarzi G, Alavi N, Yari AR, et al. Characteristics, sources, and health risks of atmospheric PM10-bound heavy metals in a populated middle eastern city. Toxin Rev. (2020) 39:266–74. 10.1080/15569543.2018.1513034 [DOI] [Google Scholar]
- 44.Slovic AD, de Oliveira MA, Biehl J, Ribeiro H. How Can Urban Policies Improve Air Quality and Help Mitigate Global Climate Change: a Systematic Mapping Review. J Urban Heal. (2016) 93:73–95. 10.1007/s11524-015-0007-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Isaifan RJ, Al-Thani H, Ayoub M, Aïssa B, Koc M, Aissa B, et al. The economic value of common urban trees in the State of Qatar from an air quality control perspective. J Environ Sci Pollut Res. (2018) 4:285–8. 10.30799/jespr.137.18040301 [DOI] [Google Scholar]
- 46.Isaifan RJ, Baldauf RW. Estimating economic and environmental benefits of urban trees in desert regions. Front Ecol. (2020) E8:1–14. 10.3389/fevo.2020.00016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Alsalama T, Koc M, Isaifan RJ. Mitigation of urban air pollution with green vegetation for sustainable cities: a review. Int J Glob Warm. (2021) 25:498–515. 10.1504/IJGW.2021.119014 [DOI] [Google Scholar]
- 48.Isaifan RJ, Couillard M, Baranova EA. Low temperature-high selectivity carbon monoxide methanation over yttria-stabilized zirconia-supported Pt nanoparticles. Int J Hydrogen Energy. (2017) 42:13754–62. 10.1016/j.ijhydene.2017.01.049 [DOI] [Google Scholar]
- 49.Isaifan RJ, Dole HAE, Obeid E, Lizarraga L, Baranova EA, Vernoux P, et al. Catalytic CO oxidation over Pt nanoparticles prepared from the polyol reduction method supported on Yttria-Stabilized Zirconia. ECS Trans. (2011) 35:43–57. 10.1149/1.3641818 [DOI] [Google Scholar]
- 50.Lortie M, Isaifan R, Liu Y, Mommers S. Synthesis of CuNi/C and CuNi/ γ -Alcatalysts for the reverse water gas shift reaction. Int J Chem Eng. (2015) 2015:1–9. 10.1155/2015/601709 [DOI] [Google Scholar]
- 51.MacDonald Gibson J, Thomsen J, Launay F, Harder E. Deaths and medical visits attributable to environmental pollution in the United Arab Emirates. PLoS ONE. (2013) 8:4. 10.1371/journal.pone.0057536 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.