

Abstract
Cancer has become the leading cause of premature death in many counties in recent decades. Previous studies showed plenty of evidence that control of modifiable risk factors would reduce the cancer burden. Since modifiable risk factors could be eliminated by changing the lifestyles of individuals, a greater uptake of modifiable risk factors is critical to reducing cancer burden and inequality in cancer survival. However, climate change will widen cancer inequities through its complex connections with modifiable risk factors. In this perspective, complex connections between climate change and cancer risks via modifiable risk factors, including abnormal temperature, UV, air pollution, natural disasters, food (diet), water, infections, and inefficient physical activities, have been summarized. The associations between climate change and modifiable risk factors have no doubt expanded the inequities. People who face overlapping modifiable risk factors, but who are unable to change or adapt, are at the highest risk in the climate change–cancer linkage. Though individual actions to avoid exposure to modifiable risk factors have been recommended, limited benefits would be achieved unless the nations strive to ensure the basic needs of the people. No choice makes avoiding exposure to risk factors an empty phrase. Thus, government actions should be taken to reduce the expanded inequities in cancer risks.
Keywords: climate change, air pollution, cancer, modifiable factor, inequity
Cancer is the second cause of globally ranked premature death after cardiovascular disease1 and has become the top cause in many countries in recent decades.2 With around a 1.7 times increase in death counts from 1990 to 2019, as estimated by the Global Burden of Disease study, cancer burden3 cannot be neglected (Figure S1), and deaths attributable to risk factors are an increasing trend, except for drug use (Figure S2). Apart from lifestyle factors, air pollution and other environmental risks are also the main factors associated with cancer. The inequality that exists in overall cancer survival between different countries is predominantly due to the disparities in health awareness; early diagnoses; screenings; and accessible, affordable, and high-quality healthcare for patients with cancer.4 Data from the United States suggests that 42% of cancer incidence and 45% of cancer mortality were attributable to modifiable risk factors, a kind of behavior or exposure factors related to cancer risk that we could reduce or control, such as poor diet and physical inactivity.5 Findings from a population-based cohort study suggested that modifiable risk factors could explain 46% of inequities in cancer morbidity and mortality.6 Inequities exist in cancer burden because cancer survival and mortality burden are closely related to the treatment ability and care. The reduction of cancer burdens attributable to avoiding modifiable risk factors would provide an equitable strategy for cancer prevention and control. Therefore, it is critical to provide a supportive environment and educational programs on how to avoid modifiable risk factors is critical. However, climate change is challenging this approach and will widen cancer inequality.
Potential Critical Connections of Climate Change and Cancer Risk
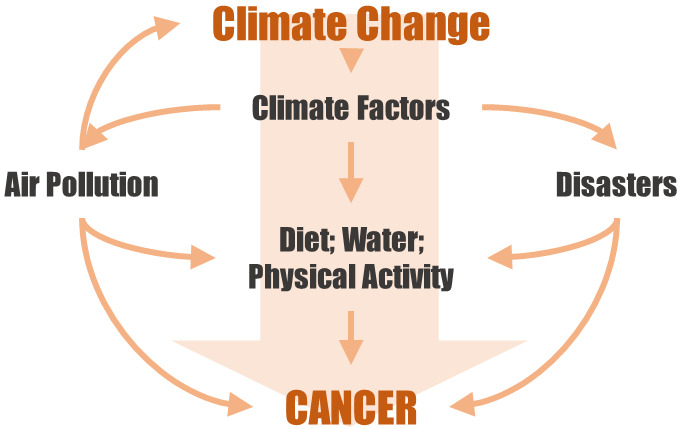
The potential linkage between climate change and factors that can modify cancer incidence and threaten cancer survival are shown in Figure 1. The combustion of fossil fuel seems to be the start of a vicious cycle since it increases greenhouse gas emissions (CO2, CH4, etc.) that aggravate climate change and produce air pollution. According to previous studies, cancers potentially associated with modifiable risk factors are highlighted in Figure 2.
Figure 1.

Potentially critical connections between climate change and cancer risk. UV: ultraviolet radiation; the dashed line indicates that high temperatures could amplify, or enhance, the effects of ambient air pollution. Natural disasters include heat waves, cold spells, wildfires, droughts, floods, hurricanes, typhoons, etc.
Figure 2.

Potential associations between climate-change-related risk factors and cancer.
The International Agency for Research on Cancer (IARC) has classified outdoor air pollution as a Group 1 carcinogen. Increasing evidence has suggested that the association may not be limited to lung cancer, but also cancer of other sites.7 Increased incidence and shorter survival of cancer affected by air pollution were observed in previous studies.7 In addition to the greenhouse gases emitted by the combustion of fossil fuels contributing to climate change, climate change may worsen air quality by changing the ventilation, dilution, precipitation and other removal processes, and the amplification of atmospheric chemistry.8 Accumulative evidence suggests that climate change is expected to increase particulate matter ≤ 2.5 μm (PM2.5)-related mortalities even under the scenario of a moderate projection of greenhouse gas emissions.9 Though the interplay of climate change and air pollution on health has been well documented, the evidence for cancer warrants investigation.10
Besides outdoor air pollution, household air pollution is also a part of the linkage.11 There are still millions of people who are not able to cook with clean energy, which results in severe indoor air pollution as well as greenhouse gases, that is, the major factor affecting climate change.12 Indoor emissions from the household combustion of coal are a Group 1 carcinogen. The household combustion of biomass fuels and emissions from high-temperature frying have been concluded to be possibly carcinogenic to humans by the IARC. It is estimated that 3.8 million premature deaths (8% from lung cancer) are attributable to household air pollution from cooking with kerosene or solid fuels each year. The Global Burden of Disease Study also suggested that indoor air pollution is associated with the risk of esophageal squamous cell carcinoma.13 “The forgotten 2.6 billion people” who have less access to cleaner fuels, mostly in low- and middle-income countries (LMICs), suffer an increasing cancer burden and are also exposed to a huge amount of air pollution. The vicious cycle of climate change, air pollution, and cancer will keep rolling and provide a devastating cancer burden without intervention.
With the accumulation of greenhouse gases, global warming, and changing meteorological factors, there is an increasing frequency of abnormally hot and cold temperatures, which are the direct expression of climate variability. Although it is not clear whether it is the increased temperature of warm months, carcinomatous meningitis was observed to have a higher incidence in these months.14 Evidence from more studies is warranted to confirm the causal association. The direct effects of extreme temperatures like heat waves may worsen the conditions of cancer patients because of their impaired thermoregulation and immune function.15 Occupational heat exposure, exacerbated by climate change,16 is also associated with several cancers, e.g., female breast cancer.17 The climate-change-induced ozone depletion led to increasing ultraviolet radiation (UV) exposure, which will lead to increased risks of melanoma and other skin cancers (e.g., squamous cell skin cancer).18 In consequence, melanoma survivors have an increased risk of developing second primary cancers, such as prostate cancer.19
The changing temperature and precipitation will also lead to changes in natural disasters and food production, which may increase the risk of cancer indirectly. Take wildfires as an example of a natural disaster that has shown an increasing trend in frequency and duration globally.20 Long-term exposure to wildfires has been suggested to increase the incidence of lung cancer and brain tumors.21 Extreme weather and natural disasters caused by climate change may reduce people’s physical activity by limiting active venues and suitable temperatures. Less physical activity could increase the risks of colon, female breast, and uterine cancers.5 Furthermore, inactivity-induced excess body weight also increases the risk of cancers of the gastrointestinal tract, genital organs, and female breast.
Less food availability and deteriorating food security induced by climate change have been observed. A modeling study revealed that by 2050, the global food availability would decrease by about 3.2%, and a 4.0% fruit and vegetable consumption reduction would be attributable to climate change.22 Parental malnutrition and exposure to air pollution exacerbated by climate change are significantly associated with serious adverse pregnancy outcomes,23,24 which are associated with higher breast cancer risk in early adult life.25 Lower consumption of fresh vegetables and fruit would also increase the risk of cancer from the respiratory and digestive tracts. Polycyclic aromatic hydrocarbons (PAHs) from high-temperature pyrogenic processes and vehicular emissions, which are related to the higher risk of breast cancer and colorectal cancer,27 were also found in commonly consumed leafy vegetables.26 The increase in the temperature led by climate change may increase appetite suppression and reduce conception rate of livestock because of heat stress, as well as reduce milk production.28 Lower dairy product consumption has been observed in line with increased breast cancer and colorectal cancer.27 Temperature and moisture significantly influenced aflatoxin production.29 Aflatoxin B1 production in maize will have consequences on aflatoxin M1 contamination in milk30 and might increase the liver cancer risk.31 Similarly, the diversity, distribution, and biology of fish populations are also affected by climate change. It is estimated that for every 1 °C of global warming, global fish catches are expected to decline by 3 million tonnes.32 Liver and colorectal cancer risks will be increased27 due to the lack and unaffordable fish consumption, especially in low-income countries.33 Climatic variability has always been the main factor responsible for fluctuations in coffee productivity worldwide.34 Coffee consumption is suggested to reduce the risk of oral and liver cancers.27 Apart from food, water quality is also affected. Climate change is likely to exacerbate the increasing bromide levels in public water systems, which would increase the excess lifetime bladder cancer risk35 and the cyanotoxins in drinking water that are associated with liver and colorectal cancer.36
Inequities in Modifiable Factors of Climate Change–Cancer Linkage
People who are most exposed to modifiable risk factors, but unable to change or adapt, are at the highest risk in the climate change–cancer linkage (Table 1). Modifiable risk factors such as excess body weight, poor diet, and physical inactivity accounted for a higher proportion in women than men for both cancer incidence and mortality.5 The more complex structures of developed countries could be more easily adjusted to account for food safety issues led by climate change compared with LMICs.37 The accessibility to cancer care in LMICs is much less than in high-income countries.4 This means that cancer care for people living in LMICs, especially those who live in rural or remote areas, is more likely to be disrupted by natural disasters. Meanwhile, they often have less capacity to deal with climate-change-related disasters. For patients diagnosed at late cancer stages, the delay of treatment could be deadly while for early diagnosed patients, they may miss out on optimal treatment opportunities. This makes the impacts of climate change on people with less access to cancer care even worse.
Table 1. Main Actions That Individual People and Government Can Take to Reduce the Inequities in Climate Change and Cancer Risk Linkagea.

Note: dot in blue represents individual actions and the dot in red represents government actions.
Overlapping inequities put some people at severe risk. As an example, women in LMICs who take the lead role in cooking and farming may suffer a higher inability to modify cancer risk factors. Women engaged in farming or other kinds of labor working to get food and earn money will also experience the adverse effects of heat exposure in their attempt to reduce poverty and improve health. Along with the heat-related cancer risks, heat stress can also cause labor and earning losses and increase working poverty, especially in sub-Saharan Africa and Southern Asia.16 Poverty and lack of food security, which are important modifiable risk factors for cancer, can lead to malnutrition, especially in women who are most hungry in low-income families. Exposures to indoor air pollution and malnutrition of other members of the household indicate that risk may indeed be multigenerational as a result of the impact of climate change. Babies in papoose carriers are also exposed to cooking fumes and indoor air pollution, which may also increase their risk of cancer.
Though some individual actions are provided (Table 1), little can be done at the individual level to reduce modifiable risk factors. Air pollution and abnormal temperatures, disasters, food shortages, and food and water safety problems led by climate change are often risk factors that cannot be avoided at the individual level. It is difficult for people, especially those who work to support their living, to avoid exposure in a positive way. Besides actions from the policymakers, self-protection such as wearing protective clothing in the sunshine seems to be the only way at the individual level to mitigate risk. However, people often need health education and living guidelines provided to make these actions clear. Climate change mitigation actions at the national and global levels are warranted.
Perspectives on Reducing the Inequality Gap
The warming climate will continue to exacerbate the inequalities in the cancer burden. The significance of this issue should not be underestimated. Fortunately, calls for climate change adaptation and adequate attention to LIMCs, women, and youth are louder than ever following the 26th UN Climate Change Conference of Parties (COP26). COP26 demonstrated a growing consensus for supporting the adaptation and resilience for vulnerable communities. We believe that in the coming COP27 these consensus perspectives will still be emphasized. It is essential to highlight women and children in LMICs as part of the intricate linkage between cancer and climate, multisector collaborations between academics, and policymakers and health officials. The rights and interests of these disadvantaged populations can be protected by rescuing more people from poverty and hunger. No choice makes avoiding exposure to risk factors an empty phrase. As such, these exposures are unavoidable risk factors until nations strive to ensure the basic needs of the people. It is vital to assess the impact of climate change and cancer burden quantitatively and to investigate cost-effective interventions and innovative technologies for vulnerable populations and regions. Health National Adaptation Plans ought to be developed and tailored for vulnerable populations to help them cope with climate change and reduce modifiable factors for cancer (e.g., increase healthcare accessibility for vulnerable populations on the basis of ensuring basic living conditions). Ultimately, responsible and immediate climate change mitigation should be the long-term strategy for all these challenges in cancer burden and inequality because it will provide a healthier planet and a more equal future.
Acknowledgments
P.Y., R.X., T.Y. were supported by China Scholarship Council funds (number 201906210065 for P.Y., 201806010405 for R.X., and 201906320051 for T.Y.); S.L. was supported by an Emerging Leader Fellowship (GNT2009866) of the Australian National Health and Medical Research Council; and Y.G. was supported by a Career Development Fellowship (GNT1163693) and Leader Fellowship (GNT2008813) of the Australian National Health and Medical Research Council.
Glossary
Abbreviations
- COP
UN Climate Change Conference of Parties
- IARC
International Agency for Research on Cancer
- UV
ultraviolet radiation
Supporting Information Available
The Supporting Information is available free of charge at https://pubs.acs.org/doi/10.1021/acsenvironau.2c00012.
Causes of death (Level 2) during 1990 to 2019 globally and attributable mortality from 1990 to 2019 globally (PDF)
The authors declare no competing financial interest.
Supplementary Material
References
- Global Burden of Disease Collaborative Network . Global Burden of Disease Study 2019 (GBD 2019) Air Pollution Exposure Estimates 1990–2019. Institute for Health Metrics and Evaluation (IHME), Seattle, WA, 2021. https://doi.org/10.6069/70JS-NC54. [Google Scholar]
- Bray F.; Laversanne M.; Weiderpass E.; Soerjomataram I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127 (16), 3029–3030. 10.1002/cncr.33587. [DOI] [PubMed] [Google Scholar]
- Global Burden of Disease Collaborative Network . Global Burden of Disease Study 2019 (GBD 2019) Results. Institute for Health Metrics and Evaluation (IHME), Seattle, WA, 2020. https://vizhub.healthdata.org/gbd-results/. [Google Scholar]
- Allemani C.; Matsuda T.; Di Carlo V.; Harewood R.; Matz M.; Nikšić M.; Bonaventure A.; Valkov M.; Johnson C. J.; Estève J.; Ogunbiyi O. J.; Azevedo E Silva G.; Chen W. Q.; Eser S.; Engholm G.; Stiller C. A.; Monnereau A.; Woods R. R.; Visser O.; Lim G. H.; Aitken J.; Weir H. K.; Coleman M. P.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391 (10125), 1023–1075. 10.1016/S0140-6736(17)33326-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Islami F.; Goding Sauer A.; Miller K. D.; Siegel R. L.; Fedewa S. A.; Jacobs E. J.; McCullough M. L.; Patel A. V.; Ma J.; Soerjomataram I.; Flanders W. D.; Brawley O. W.; Gapstur S. M.; Jemal A. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J. Clin 2018, 68 (1), 31–54. 10.3322/caac.21440. [DOI] [PubMed] [Google Scholar]
- Nejatinamini S.; Godley J.; Minaker L. M.; Sajobi T. T.; McCormack G. R.; Cooke M. J.; Nykiforuk C. I. J.; Koning L.; Olstad D. L. Quantifying the contribution of modifiable risk factors to socio-economic inequities in cancer morbidity and mortality: a nationally representative population-based cohort study. Int. J. Epidemiol 2021, 50 (5), 1498–1511. 10.1093/ije/dyab067. [DOI] [PubMed] [Google Scholar]
- Yu P.; Guo S.; Xu R.; Ye T.; Li S.; Sim M. R.; Abramson M. J.; Guo Y. Cohort studies of long-term exposure to outdoor particulate matter and risks of cancer: A systematic review and meta-analysis. Innovation (Camb) 2021, 2 (3), 100143. 10.1016/j.xinn.2021.100143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiore A. M.; Naik V.; Leibensperger E. M. Air quality and climate connections. J. Air Waste Manag Assoc 2015, 65 (6), 645–85. 10.1080/10962247.2015.1040526. [DOI] [PubMed] [Google Scholar]
- Chen K.; Vicedo-Cabrera A. M.; Dubrow R. Projections of Ambient Temperature- and Air Pollution-Related Mortality Burden Under Combined Climate Change and Population Aging Scenarios: a Review. Curr. Environ. Health Rep 2020, 7 (3), 243–255. 10.1007/s40572-020-00281-6. [DOI] [PubMed] [Google Scholar]
- Orru H.; Ebi K. L.; Forsberg B. The Interplay of Climate Change and Air Pollution on Health. Curr. Environ. Health Rep 2017, 4 (4), 504–513. 10.1007/s40572-017-0168-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Josyula S.; Lin J.; Xue X.; Rothman N.; Lan Q.; Rohan T. E.; Hosgood H. D. 3rd. Household air pollution and cancers other than lung: a meta-analysis. Environ. Health 2015, 14, 24. 10.1186/s12940-015-0001-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoner O.; Lewis J.; Martínez I. L.; Gumy S.; Economou T.; Adair-Rohani H. Household cooking fuel estimates at global and country level for 1990 to 2030. Nat. Commun. 2021, 12 (1), 5793. 10.1038/s41467-021-26036-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamangar F.; Nasrollahzadeh D.; Safiri S.; Sepanlou S. G.; Fitzmaurice C.; Ikuta K. S.; Bisignano C.; Islami F.; Roshandel G.; Lim S. S.; et al. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020, 5 (6), 582–597. 10.1016/S2468-1253(20)30007-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koutras A.; Sakellakis M.; Makatsoris T.; Psachoulia C.; Kardari M.; Nikolakopoulos A.; Gogos C.; Kalofonos H. P. Seasonal variability in the incidence of carcinomatous meningitis. J. Neurosurg 2015, 122 (3), 543–6. 10.3171/2014.11.JNS14174. [DOI] [PubMed] [Google Scholar]
- Zhao Q.; Guo Y.; Ye T.; Gasparrini A.; Tong S.; Overcenco A.; Urban A.; Schneider A.; Entezari A.; Vicedo-Cabrera A. M.; Zanobetti A.; Analitis A.; Zeka A.; Tobias A.; Nunes B.; Alahmad B.; Armstrong B.; Forsberg B.; Pan S. C.; Íñiguez C.; Ameling C.; De la Cruz Valencia C.; Åström C.; Houthuijs D.; Dung D. V.; Royé D.; Indermitte E.; Lavigne E.; Mayvaneh F.; Acquaotta F.; de’Donato F.; Di Ruscio F.; Sera F.; Carrasco-Escobar G.; Kan H.; Orru H.; Kim H.; Holobaca I. H.; Kyselý J.; Madureira J.; Schwartz J.; Jaakkola J. J. K.; Katsouyanni K.; Hurtado Diaz M.; Ragettli M. S.; Hashizume M.; Pascal M.; de Sousa Zanotti Stagliorio Coélho M.; Valdés Ortega N.; Ryti N.; Scovronick N.; Michelozzi P.; Matus Correa P.; Goodman P.; Nascimento Saldiva P. H.; Abrutzky R.; Osorio S.; Rao S.; Fratianni S.; Dang T. N.; Colistro V.; Huber V.; Lee W.; Seposo X.; Honda Y.; Guo Y. L.; Bell M. L.; Li S. Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: a three-stage modelling study. Lancet Planet Health. 2021, 5 (7), e415–e425. 10.1016/S2542-5196(21)00081-4. [DOI] [PubMed] [Google Scholar]
- Working on a warmer planet: The impact of heat stress on labour productivity and decent work. International Labour Office: Geneva, Switzerland, 2019. [Google Scholar]
- Hinchliffe A.; Kogevinas M.; Pérez-Gómez B.; Ardanaz E.; Amiano P.; Marcos-Delgado A.; Castaño-Vinyals G.; Llorca J.; Moreno V.; Alguacil J.; Fernandez-Tardón G.; Salas D.; Marcos-Gragera R.; Aragonés N.; Guevara M.; Gil L.; Martin V.; Benavente Y.; Gomez-Acebo I.; Santibáñez M.; Ángel Alba M.; García A. M.; Pollán M.; Turner M. C. Occupational Heat Exposure and Breast Cancer Risk in the MCC-Spain Study. Cancer Epidemiol Biomarkers Prev 2021, 30 (2), 364–372. 10.1158/1055-9965.EPI-20-0732. [DOI] [PubMed] [Google Scholar]
- Bernhard G. H.; Neale R. E.; Barnes P. W.; Neale P. J.; Zepp R. G.; Wilson S. R.; Andrady A. L.; Bais A. F.; McKenzie R. L.; Aucamp P. J.; Young P. J.; Liley J. B.; Lucas R. M.; Yazar S.; Rhodes L. E.; Byrne S. N.; Hollestein L. M.; Olsen C. M.; Young A. R.; Robson T. M.; Bornman J. F.; Jansen M. A. K.; Robinson S. A.; Ballare C. L.; Williamson C. E.; Rose K. C.; Banaszak A. T.; Hader D.-P.; Hylander S.; Wangberg S.-A.; Austin A. T.; Hou W.-C.; Paul N. D.; Madronich S.; Sulzberger B.; Solomon K. R.; Li H.; Schikowski T.; Longstreth J.; Pandey K. K.; Heikkila A. M.; White C. C.; et al. Environmental effects of stratospheric ozone depletion, UV radiation and interactions with climate change: UNEP Environmental Effects Assessment Panel, update 2019. Photochem. Photobiol. Sci. 2020, 19 (5), 542–584. 10.1039/D0PP90011G. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimlin M. G.; Youlden D. R.; Brodie A. M.; DiSipio T.; Youl P.; Nair-Shalliker V.; Baade P. D. Risk of Second Primary Cancer in Survivors of In Situ Melanoma. J. Invest Dermatol 2019, 139 (4), 842–847. 10.1016/j.jid.2018.11.001. [DOI] [PubMed] [Google Scholar]
- Xu R.; Yu P.; Abramson M. J.; Johnston F. H.; Samet J. M.; Bell M. L.; Haines A.; Ebi K. L.; Li S.; Guo Y. Wildfires, Global Climate Change, and Human Health. N Engl J. Med. 2020, 383 (22), 2173–2181. 10.1056/NEJMsr2028985. [DOI] [PubMed] [Google Scholar]
- Korsiak J.; Pinault L.; Christidis T.; Burnett R. T.; Abrahamowicz M.; Weichenthal S. Long-term exposure to wildfires and cancer incidence in Canada: a population-based observational cohort study. Lancet Planet Health. 2022, 6 (5), e400–e409. 10.1016/S2542-5196(22)00067-5. [DOI] [PubMed] [Google Scholar]
- Springmann M.; Mason-D’Croz D.; Robinson S.; Garnett T.; Godfray H. C.; Gollin D.; Rayner M.; Ballon P.; Scarborough P. Global and regional health effects of future food production under climate change: a modelling study. Lancet 2016, 387 (10031), 1937–46. 10.1016/S0140-6736(15)01156-3. [DOI] [PubMed] [Google Scholar]
- da Cruz R. S.; Carney E. J.; Clarke J.; Cao H.; Cruz M. I.; Benitez C.; Jin L.; Fu Y.; Cheng Z.; Wang Y.; de Assis S. Paternal malnutrition programs breast cancer risk and tumor metabolism in offspring. Breast Cancer Res. 2018, 20 (1), 99. 10.1186/s13058-018-1034-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bekkar B.; Pacheco S.; Basu R.; DeNicola N. Association of Air Pollution and Heat Exposure With Preterm Birth, Low Birth Weight, and Stillbirth in the US: A Systematic Review. JAMA Netw Open. 2020, 3 (6), e208243 10.1001/jamanetworkopen.2020.8243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mellemkjaer L.; Olsen M. L.; Sørensen H. T.; Thulstrup A. M.; Olsen J.; Olsen J. H. Birth weight and risk of early-onset breast cancer (Denmark). Cancer Causes Control 2003, 14 (1), 61–4. 10.1023/A:1022570305704. [DOI] [PubMed] [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research . Diet, Nutrition, Physical Activity and Cancer: a Global Perspective. Continuous Update Project Expert Report, 2018.
- Tesi G. O.; Iniaghe P. O.; Lari B.; Obi-Iyeke G.; Ossai J. C. Polycyclic aromatic hydrocarbons (PAHs) in leafy vegetables consumed in southern Nigeria: concentration, risk assessment and source apportionment. Environ. Monit. Assess. 2021, 193, 443. 10.1007/s10661-021-09217-5. [DOI] [PubMed] [Google Scholar]
- Goma A. A.; Phillips C. J. C. The Impact of Anthropogenic Climate Change on Egyptian Livestock Production. Animals (Basel) 2021, 11 (11), 3127. 10.3390/ani11113127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milićević D.; Petronijević R.; Petrović Z.; Đjinović-Stojanović J.; Jovanović J.; Baltić T.; Janković S. Impact of climate change on aflatoxin M1 contamination of raw milk with special focus on climate conditions in Serbia. J. Sci. Food Agric 2019, 99 (11), 5202–5210. 10.1002/jsfa.9768. [DOI] [PubMed] [Google Scholar]
- Van der Fels-Klerx H. J.; Vermeulen L. C.; Gavai A. K.; Liu C. Climate change impacts on aflatoxin B1 in maize and aflatoxin M1 in milk: A case study of maize grown in Eastern Europe and imported to the Netherlands. PLoS One. 2019, 14 (6), e0218956 10.1371/journal.pone.0218956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nugraha A.; Khotimah K.; Rietjens I. M. C. M. Risk assessment of aflatoxin B1 exposure from maize and peanut consumption in Indonesia using the margin of exposure and liver cancer risk estimation approaches. Food Chem. Toxicol. 2018, 113, 134–144. 10.1016/j.fct.2018.01.036. [DOI] [PubMed] [Google Scholar]
- Cheung W. W.; Lam V. W.; Sarmiento J. L.; Kearney K.; Watson R. E.; Zeller D.; Pauly D. Large-scale redistribution of maximum fisheries catch potential in the global ocean under climate change. Global Change Biology 2010, 16 (1), 24–35. 10.1111/j.1365-2486.2009.01995.x. [DOI] [Google Scholar]
- Vianna G. M. S.; Zeller D.; Pauly D. Fisheries and Policy Implications for Human Nutrition. Curr. Environ. Health Rep 2020, 7 (3), 161–169. 10.1007/s40572-020-00286-1. [DOI] [PubMed] [Google Scholar]
- Dos Santos D. G.; Coelho C. C. S.; Ferreira A. B. R.; Freitas-Silva O. Brazilian Coffee Production and the Future Microbiome and Mycotoxin Profile Considering the Climate Change Scenario. Microorganisms 2021, 9 (4), 858. 10.3390/microorganisms9040858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Regli S.; Chen J.; Messner M.; Elovitz M. S.; Letkiewicz F. J.; Pegram R. A.; Pepping T. J.; Richardson S. D.; Wright J. M. Estimating Potential Increased Bladder Cancer Risk Due to Increased Bromide Concentrations in Sources of Disinfected Drinking Waters. Environ. Sci. Technol. 2015, 49 (22), 13094–102. 10.1021/acs.est.5b03547. [DOI] [PubMed] [Google Scholar]
- Lee J.; Lee S.; Jiang X. Cyanobacterial Toxins in Freshwater and Food: Important Sources of Exposure to Humans. Annu. Rev. Food Sci. Technol. 2017, 8, 281–304. 10.1146/annurev-food-030216-030116. [DOI] [PubMed] [Google Scholar]
- Lake I. R.; Hooper L.; Abdelhamid A.; Bentham G.; Boxall A. B.; Draper A.; Fairweather-Tait S.; Hulme M.; Hunter P. R.; Nichols G.; Waldron K. W. Climate change and food security: health impacts in developed countries. Environ. Health Perspect 2012, 120 (11), 1520–6. 10.1289/ehp.1104424. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.