

This cross-sectional study of 2 observational cohorts investigates if phosphorylated tau biomarkers are more associated with the presence of cerebral β-amyloidosis or tau neurofibrillary tangle aggregation.
Key Points
Question
Do soluble phosphorylated tau (p-tau) biomarkers preferentially reflect the presence of cerebral β-amyloidosis or tau neurofibrillary tangle aggregation?
Findings
In this cross-sectional study of 2 observational cohorts, 4 p-tau biomarkers in the cerebrospinal fluid (CSF; p-tau181, p-tau217, p-tau231, p-tau235) were significantly more closely associated with amyloid PET (positron emission tomography) than with tau PET. These results were replicated in an independent group of individuals with plasma p-tau181, p-tau217, and p-tau231 and in another independent cohort with CSF p-tau181.
Meaning
Results suggest that soluble p-tau biomarkers are more closely associated with cerebral amyloid-β than with tau aggregation assessed with PET; this finding supports the need for careful interpretation of p-tau biomarkers in the context of the amyloid/tau/neurodegeneration, or A/T/(N), framework.
Abstract
Importance
The recent proliferation of phosphorylated tau (p-tau) biomarkers has raised questions about their preferential association with the hallmark pathologies of Alzheimer disease (AD): amyloid-β plaques and tau neurofibrillary tangles.
Objective
To determine whether cerebrospinal fluid (CSF) and plasma p-tau biomarkers preferentially reflect cerebral β-amyloidosis or neurofibrillary tangle aggregation measured with positron emission tomography (PET).
Design, Setting, and Participants
This was a cross-sectional study of 2 observational cohorts: the Translational Biomarkers in Aging and Dementia (TRIAD) study, with data collected between October 2017 and August 2021, and the Alzheimer’s Disease Neuroimaging Initiative (ADNI), with data collected between September 2015 and November 2019. TRIAD was a single-center study, and ADNI was a multicenter study. Two independent subsamples were derived from TRIAD. The first TRIAD subsample comprised individuals assessed with CSF p-tau (p-tau181, p-tau217, p-tau231, p-tau235), [18F]AZD4694 amyloid PET, and [18F]MK6240 tau PET. The second TRIAD subsample included individuals assessed with plasma p-tau (p-tau181, p-tau217, p-tau231), [18F]AZD4694 amyloid PET, and [18F]MK6240 tau PET. An independent cohort from ADNI comprised individuals assessed with CSF p-tau181, [18F]florbetapir PET, and [18F]flortaucipir PET. Participants were included based on the availability of p-tau and PET biomarker assessments collected within 9 months of each other. Exclusion criteria were a history of head trauma or magnetic resonance imaging/PET safety contraindications. No participants who met eligibility criteria were excluded.
Exposures
Amyloid PET, tau PET, and CSF and plasma assessments of p-tau measured with single molecule array (Simoa) assay or enzyme-linked immunosorbent assay.
Main Outcomes and Measures
Associations between p-tau biomarkers with amyloid PET and tau PET.
Results
A total of 609 participants (mean [SD] age, 66.9 [13.6] years; 347 female [57%]; 262 male [43%]) were included in the study. For all 4 phosphorylation sites assessed in CSF, p-tau was significantly more closely associated with amyloid-PET values than tau-PET values (p-tau181 difference, 13%; 95% CI, 3%-22%; P = .006; p-tau217 difference, 11%; 95% CI, 3%-20%; P = .003; p-tau231 difference, 15%; 95% CI, 5%-22%; P < .001; p-tau235 difference, 9%; 95% CI, 1%-19%; P = .02) . These results were replicated with plasma p-tau181 (difference, 11%; 95% CI, 1%-22%; P = .02), p-tau217 (difference, 9%; 95% CI, 1%-19%; P = .02), p-tau231 (difference, 13%; 95% CI, 3%-24%; P = .009), and CSF p-tau181 (difference, 9%; 95% CI, 1%-21%; P = .02) in independent cohorts.
Conclusions and Relevance
Results of this cross-sectional study of 2 observational cohorts suggest that the p-tau abnormality as an early event in AD pathogenesis was associated with amyloid-β accumulation and highlights the need for careful interpretation of p-tau biomarkers in the context of the amyloid/tau/neurodegeneration, or A/T/(N), framework.
Introduction
Alzheimer disease (AD) is defined by the presence of cerebral amyloid-β plaques and tau neurofibrillary tangles.1,2 The A/T/(N) biomarker classification system identifies 3 classes of AD biomarkers: amyloid-β, tau, and neurodegeneration, in which amyloid-β and tau biomarkers are specific to AD.3,4 Amyloid-β biomarkers include amyloid positron emission tomography (PET) as well as cerebrospinal fluid (CSF) and plasma concentrations of amyloid-β. Tau biomarkers include quantification of insoluble neurofibrillary tangles using PET, as well as soluble phosphorylated tau (p-tau) in the CSF and plasma. Because of their specificity, amyloid-β and tau biomarkers are increasingly used in AD diagnosis5 and as inclusion criteria for disease-modifying clinical trials.6,7
Although soluble p-tau biomarkers are interpreted as biomarkers of tau pathology, several recent observational studies provide evidence that concentrations of p-tau are closely correlated with amyloid-β deposition.8,9,10,11,12,13,14 A longitudinal study in autosomal dominant AD provides evidence that concentrations of soluble p-tau biomarkers begin to rise in conjunction with amyloid-β aggregation, several years before neocortical tau abnormality.15 Furthermore, longitudinal biomarker studies in sporadic AD report that soluble p-tau217 mediates the association between amyloid-β and tau-PET change.8,16 Correspondingly, recent biomarker models of AD suggest that p-tau reflects a state between amyloid-β plaques and tau aggregation.16,17,18 However, it is unclear to what extent biofluid measurements of p-tau are preferentially associated with the presence of amyloid-β or tau neurofibrillary tangles in the brain.
The objective of the current study was to determine whether soluble p-tau biomarkers are preferentially associated with cerebral amyloid-β plaques or tau neurofibrillary tangles. We evaluated the association between 4 p-tau biomarkers in the CSF (p-tau181, p-tau217, p-tau231, p-tau235) and 3 in plasma (p-tau181, p-tau217, p-tau231) with amyloid-β and tau aggregation assessed with PET in the Translational Biomarkers in Aging and Dementia (TRIAD) study cohort. In addition, we evaluated the association between CSF p-tau181 with amyloid PET and tau PET in the Alzheimer Disease Neuroimaging Initiative (ADNI) cohort.
Methods
Participants
Translational Biomarkers in Aging and Dementia
This study was approved by the Montreal Neurological Institute PET working committee and the Douglas Mental Health University Institute Research Ethics Board. Written informed consent was obtained for all participants. For this cross-sectional study, we assessed 2 independent subsamples of participants in the TRIAD19 cohort: a CSF p-tau subsample (n = 181) and a plasma p-tau subsample (n = 171). Participants included in the CSF subsample had measures of CSF p-tau (p-tau181, p-tau217, p-tau231, p-tau235), amyloid PET with [18F]AZD4694, tau PET with [18F]MK6240, and magnetic resonance imaging (MRI). The median (IQR) time difference between CSF and PET data collection was 53 (86) days. In the second subsample (n = 171), individuals had measures of plasma p-tau (p-tau181, p-tau217, p-tau231), amyloid PET with [18F]AZD4694, tau PET with [18F]MK6240, and MRI. The median (IQR) time difference between plasma and PET data collection was 70 (112) days. The individuals in the second TRIAD subsample did not have CSF measures of p-tau and thus represent an independent sample of individuals. Participants had paired fluid p-tau and PET biomarker assessments available within a 9-month interval. All individuals were included between October 2017 and August 2021. Individuals from the following race and ethnicity categories were included: Asian, Black, Hawaiian/Pacific Islander, Hispanic/Latinx, non-Hispanic/Latinx, multiracial, White, and unknown/not reported. Race and ethnicity were identified using official National Institutes of Health classifications. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Cognitively unimpaired (CU) individuals had no objective cognitive impairment and a Clinical Dementia Rating (CDR) score of 0. Individuals with mild cognitive impairment had subjective and/or objective cognitive impairment and a CDR score of 0.5.20 Individuals with dementia had a CDR score of 1 or 2.21 Participants were excluded from this study if they had systemic conditions that were not adequately controlled through a stable medication regimen. Other exclusion criteria were active substance abuse, recent head trauma, recent major surgery, or MRI/PET safety contraindications. PET acquisition and processing are described in eMethods 1 of the Supplement. All p-tau residues measured from the CSF, as well as plasma p-tau181 and p-tau231, were quantified in the Clinical Neurochemistry Laboratory, University of Gothenburg, Mölndal, Sweden, by scientists blinded to participant clinical and PET information; this information is described in detail in eMethods 2 of Supplement. Plasma p-tau217 was quantified by scientists at Janssen Research & Development blinded to clinical and PET information.
Alzheimer Disease Neuroimaging Initiative
The ADNI study was approved by the institutional review boards of all participating institutions. All participants provided informed written consent. We examined the open-access ADNI cohort, a North American multisite cohort launched in 2003. All participants had amyloid PET with [18F]florbetapir, tau-PET with [18F]flortaucipir, and CSF p-tau181. ADNI PET acquisition and processing data are described in eMethods 1 of the Supplement, and CSF p-tau181 quantification is described in eMethods 2 of the Supplement. The median (IQR) time difference between CSF and PET data collection was 13 (29) days. CU participants had a CDR of 0, individuals with mild cognitive impairment had a CDR of 0.5, and individuals with dementia had a CDR score of 1 or 2. Full information regarding the ADNI inclusion and exclusion criteria is available on the ADNI informational site.22 Plasma p-tau181 was not investigated in ADNI due to the small number of individuals with plasma p-tau evaluations and tau PET at the same visit.
Statistical Analysis
Statistical analyses were performed in R, version 4.1.1 (R Foundation for Statistical Computing) and Matlab, version 2015a (MathWorks). Assumptions of normality were tested using the D’Agastino-Pearson normality test. Associations between p-tau biomarkers with [18F]AZD4694 PET and [18F]MK6240 PET were investigated using the Spearman nonparametric test. Statistical evaluation of whether correlations were significantly different was performed in R using the cocor package,23 a statistical framework for comparing associations between intercorrelated measurements. As secondary confirmatory analyses, we conducted partial correlation analyses to determine the extent to which p-tau biomarker concentrations were associated with amyloid PET when correcting for tau PET and tau PET correcting for amyloid PET using the ppcor package. We also conducted analyses correcting for age and sex. P values were 2-sided, and statistical significance was defined as P <.05.
Because PET measures of pathology reflect accumulation within specific brain regions, which may preferentially reflect protein aggregation at specific disease stages, we conducted supplementary sensitivity analyses stratified by cognitive impairment, and we used summary composite regions of interest (ROIs) considered to become positive earlier in the AD process. For amyloid PET, the Biofinder Early Aβ-PET ROI24 was used, and for tau PET, the inferior temporal cortical ROI was used, previously implemented to capture early tau aggregation in studies of CU individuals25,26 and in the early stages of autosomal dominant AD.27 We also compared global amyloid PET with tau-PET uptake in Braak I-II regions. We also compared CSF concentrations of Aβ (indexed by the Aβ42/40 ratio) with tau-PET uptake. Finally, we compared whole-cortex amyloid-PET and whole-cortex tau-PET standardized uptake value ratios (SUVRs).
Results
Participants
A total of 609 participants (mean [SD] age, 66.9 [13.6] years; 347 female [57%]; 262 male [43%]) were included in the study. The first TRIAD subsample included 181 participants; the second subsample included 171 participants. The mean (SD) age of participants in the CSF TRIAD subsample was 61.7 (17.9) years, with 196 female individuals (55.7%) and 156 male individuals (44.3%). The mean (SD) age of participants in the plasma TRIAD subsample was 66.3 (15.2) years, with 113 female individuals (66.1%) and 58 male individuals (33.9%). The ADNI cohort included a total of 257 participants (mean [SD] age, 70.6 [6.7] years; 131 female [51.0%]; 126 male [49.0%]). Our study included the following race and ethnicity groups: 17 Asian (2.8%), 17 Black (2.8%), 1 Hawaiian/Pacific Islander (0.2%), 10 Hispanic/Latinx (1.6%), 577 non-Hispanic/Latinx (94.7%), 4 multiracial (0.7%), 551 White (90.5%), and 19 unknown/not reported (3.1%). Demographic, clinical, and biomarker information for all samples is reported in the Table.
Table. Demographic Characteristics of the Samples.
| Characteristic | No. (%) | |||
|---|---|---|---|---|
| Young adults | Cognitively unimpaired older adults | Mild cognitive impairment | Dementia | |
| A: TRIAD cerebrospinal fluid sample | ||||
| No. | 27 | 86 | 45 | 23 |
| Age, mean (SD), y | 22.8 (1.9) | 69.5 (8.0) | 71.3 (7.5) | 62.4 (6.5) |
| Sex | ||||
| Male | 11 (40.7) | 32 (37.2) | 18 (40.0) | 12 (52.2) |
| Female | 16 (59.3) | 54 (62.8) | 27 (60.0) | 11 (47.8) |
| Education, mean (SD), y | 16.7 (1.5) | 14.8 (3.5) | 14.9 (3.2) | 15.1 (3.5) |
| APOE ε4 carriers, % | 6 (22.2) | 25 (29.1) | 17 (37.7) | 13 (56.5) |
| MMSE, mean (SD) | 29.8 (0.5) | 29.1 (1.0) | 27.7 (1.8) | 18.7 (5.6) |
| Self-reported race | ||||
| American Indian/Alaskan Native | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Asian | 9 (33.3) | 0 (0) | 1 (2.2) | 1 (4.3) |
| Black | 1 (3.7) | 1 (1.2) | 0 (2.3) | 0 (0) |
| Hawaiian/Pacific Islander | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Multiracial | 1 (3.7) | 0 (0) | 0 (0) | 0 (0) |
| White | 16 (59.3) | 78 (90.7) | 42 (93.3) | 21 (91.3) |
| Unknown/not reported | 0 (0) | 7 (8.1) | 2 (4.4) | 1 (4.3) |
| Self-reported ethnicity | ||||
| Hispanic/Latinx | 0 (0) | 1 (1.2) | 0 (0) | 0 (0) |
| Not Hispanic/Latinx | 27 (100) | 78 (90.7) | 43 (95.5) | 21 (91.3) |
| Unknown/not reported | 0 (0) | 7 (8.1) | 2 (4.4) | 2 (8.7) |
| B: TRIAD plasma sample | ||||
| No. | 9 | 88 | 43 | 31 |
| Age, mean (SD), y | 22.6 (1.6) | 69.5 (12.2) | 67.2 (11.4) | 69.0 (9.7) |
| Sex | ||||
| Male | 2 (22.2) | 27 (30.7) | 17 (39.5) | 12 (38.7) |
| Female | 7 (77.8) | 61 (69.3) | 26 (60.5) | 19 (61.3) |
| Education, mean (SD), y | 16.1 (1.4) | 15.9 (4.0) | 15.2 (4.1) | 13.8 (3.6) |
| APOE ε4 carriers, % | 3 (33.3) | 19 (21.6) | 15 (38.5) | 15 (48.3) |
| MMSE, mean (SD) | 30.0 (0.0) | 29.2 (1.1) | 28.0 (1.8) | 20.0 (5.9) |
| Self-reported race | ||||
| American Indian/Alaskan Native | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Asian | 4 (44.4) | 0 (0) | 1 (2.3) | 1 (3.2) |
| Black | 0 (0) | 1 (1.1) | 1 (2.3) | 0 (0) |
| Hawaiian/Pacific Islander | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Multiracial | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| White | 5 (55.6) | 80 (90.9) | 41 (95.3) | 28 (90.3) |
| Unknown/not reported | 0 (0) | 7 (7.9) | 0 (0) | 2 (6.5) |
| Self-reported ethnicity | ||||
| Hispanic/Latinx | 0 (0) | 1 (1.1) | 0 (0) | 0 (0) |
| Not Hispanic/Latinx | 9 (100) | 80 (90.1) | 43 (100) | 29 (93.5) |
| Unknown/not reported | 0 (0) | 7 (7.8) | 0 (0) | 2 (6.5) |
| C: ADNI CSF sample | ||||
| No. | 0 | 153 | 88 | 16 |
| Age, mean (SD), y | NA | 71.4 (6.3) | 69.7 (7.1) | 67.9 (8.0) |
| Sex, No. (%) | ||||
| Male | NA | 63 (41.2) | 54 (61.4) | 9 (56.2) |
| Female | 90 (58.8) | 34 (38.6) | 7 (43.8) | |
| Education, mean (SD), y | NA | 16.8 (2.4) | 16.6 (2.6) | 15.4 (2.2) |
| APOE ε4 carriers, % | NA | 50 (32.9) | 34 (41.5) | 11 (68.8) |
| MMSE, mean (SD) | NA | 29.1 (1.2) | 27.9 (2.0) | 20.9 (2.8) |
| Self-reported race, No. (%) | ||||
| American Indian/Alaska Native | NA | 0 (0) | 0 (0) | 0 (0) |
| Asian | 0 (0) | 0 (0) | 0 (0) | |
| Black | 10 (6.5) | 2 (2.3) | 1 (6.3) | |
| Hawaiian/Pacific Islander | 0 (0) | 1 (1.1) | 0 (0) | |
| Multiracial | 3 (2.0) | 0 (0) | 0 (0) | |
| White | 140 (91.5) | 85 (96.6) | 15 (93.7) | |
| Unknown/not reported | 0 (0) | 0 (0) | 0 (0) | |
| Self-reported ethnicity, No. (%) | ||||
| Hispanic/Latinx | NA | 6 (3.9) | 2 (2.3) | 0 (0) |
| Not Hispanic/Latinx | 145 (94.8) | 86 (97.7) | 16 (100) | |
| Unknown/not reported | 2 (1.3) | 0 (0) | 0 (0) | |
Abbreviations: ADNI, Alzheimer’s Disease Neuroimaging Initiative; APOE, apolipoprotein E; CSF, cerebrospinal fluid; MMSE, Mini-Mental State Examination; NA, not applicable; SUVR, standardized uptake value ratio; TRIAD, the Translational Biomarkers in Aging and Dementia.
Associations Between CSF p-Tau and PET Biomarkers
Figure 1 displays voxelwise associations between CSF p-tau181, p-tau217, p-tau231, and p-tau235 with amyloid PET and with tau PET in the TRIAD cohort. CSF p-tau231 and p-tau217 had the strongest associations with amyloid PET across the cerebral cortex. Lower correlations were observed across the cerebral cortex for CSF p-tau181, p-tau217, p-tau231, and p-tau235 with tau PET. For all CSF p-tau phosphorylation sites, correlations above 0.65 were restricted to the medial temporal cortices. Frequency distributions of correlations are displayed in Figure 1C. For all p-tau biomarkers, associations with amyloid PET were more widespread across the brain.
Figure 1. Association of Cerebrospinal Fluid (CSF) Phosphorylated Tau (p-Tau) Biomarkers With Amyloid Positron Emission Tomography (PET) and Tau PET Across the Cerebral Cortex.
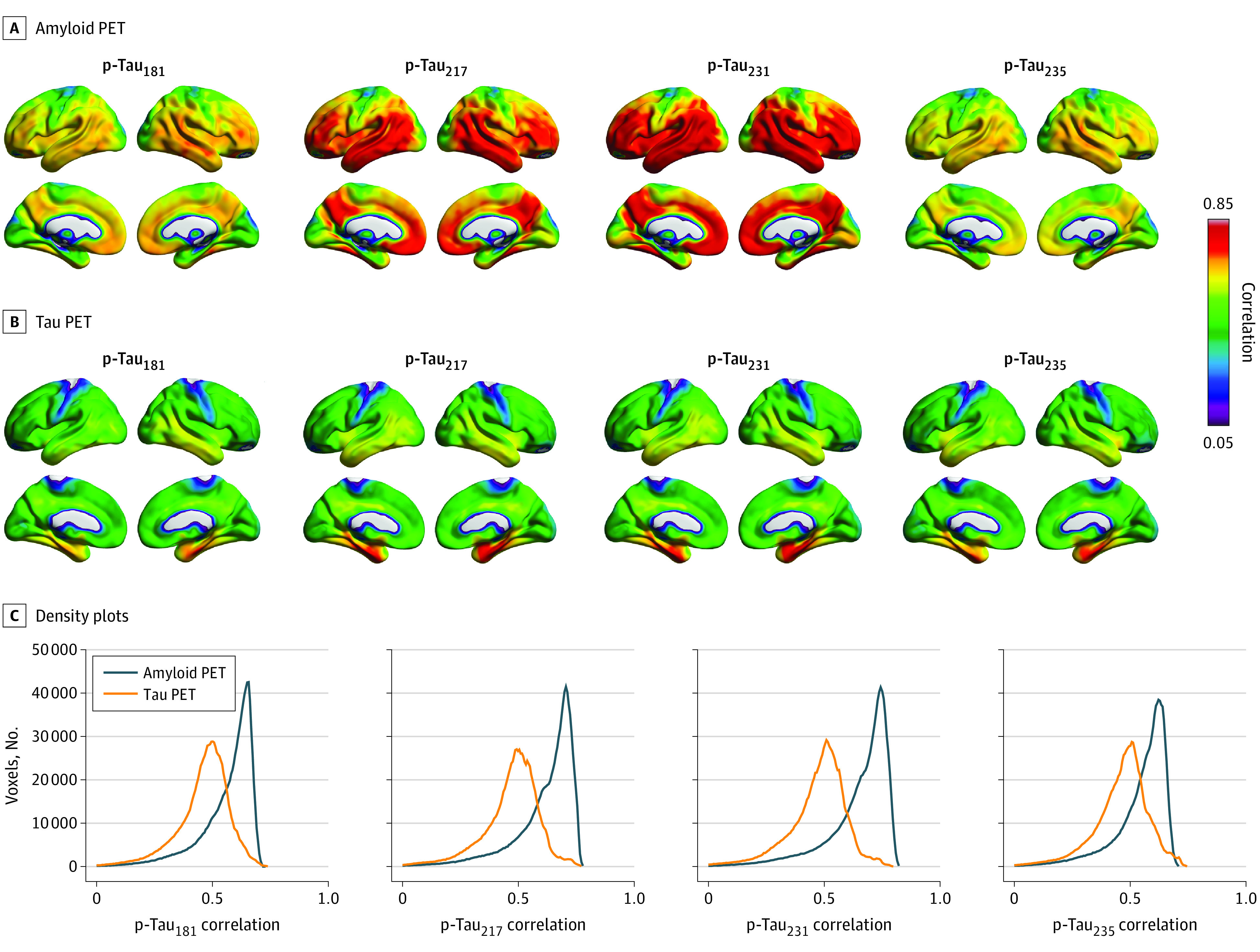
Brain images show the distribution of associations between CSF p-tau biomarkers (p-tau181, p-tau217, p-tau231, and p-tau235) and [18F]AZD4694 amyloid PET (A) and [18F]MK6240 tau PET (B). C, Density plots depict the magnitude and frequency of the correlations in voxels per CSF p-tau epitope and imaging biomarker. For all CSF p-tau phosphorylation sites, most voxels had correlation values with amyloid PET between 0.65 and 0.75. In contrast, the majority of voxels had correlations around 0.50 with tau PET, with limited numbers of voxels having correlations between 0.65 and 0.75.
Figure 2 displays associations between CSF p-tau biomarkers with summary measures of amyloid PET and tau PET in the TRIAD cohort. CSF concentrations of p-tau217 and p-tau231 were the most closely associated with neocortical summary measurements of amyloid PET (p-tau217, ρ = 0.77; 95% CI, 0.69-0.82; P < .001; p-tau231, ρ = 0.80; 95% CI, 0.73-0.85; P < .001). Correlations for CSF p-tau181 and p-tau235 with summary amyloid-PET SUVR were relatively lower (p-tau181, ρ = 0.70; 95% CI, 0.61-0.77; P < .001; p-tau235, ρ = 0.70; 95% CI, 0.60-0.76; P < .001). When investigating associations between CSF p-tau phosphorylation and tau-PET summary measurements, we observed that p-tau217 and p-tau231 biomarkers were most closely associated with tau PET in the temporal meta-ROI (p-tau217, ρ = 0.66; 95% CI, 0.57-0.74; P < .001; p-tau231, ρ = 0.65; 95% CI, 0.56-0.73; P < .001). Lower correlations were observed for p-tau181 and p-tau235 (p-tau181, ρ = 0.57; 95% CI, 0.46-0.66; P < .001; p-tau235, ρ = 0.61; 95% CI, 0.50-0.70; P < .001). Comparison of correlations revealed that for all p-tau phosphorylation sites, p-tau was significantly more closely associated with summary measurements of amyloid PET than with summary measures of tau-PET (p-tau181 difference, 13%; t value = 2.54; P = .006; 95% CI, 0.03-0.22; p-tau217 difference, 11%; t value = 2.77; P = .003; 95% CI, 0.03-0.20; p-tau231 difference, 15%; t value = 3.96; P < .001; 95% CI, 0.05-0.22; p-tau235 difference, 9%; t value = 1.98; 95% CI, 0.01-0.19; P = .02). In sensitivity analyses using the early amyloid PET from the Biomarkers for Identifying Neurodegenerative Disorders Early and Reliably (BioFINDER) study and inferior temporal ROIs, all p-tau biomarkers were more closely associated with amyloid PET than tau PET (eResults, eFigure 1, and eTable 5 in the Supplement). A summary of correlation comparisons for summary PET measures in the CSF TRIAD sample is provided in eTable 1 in the Supplement. A similar pattern of results was observed when examining CSF Aβ42/40 and tau-PET (eResults, eFigure 2, and eTable 2 in the Supplement). The CSF Aβ42/40 ratio was more closely associated with amyloid PET than tau PET (eFigure 3 in the Supplement). In analyses stratified by the presence of cognitive impairment, p-tau biomarkers were much more strongly associated with amyloid PET in CU individuals, whereas no differences were detected in cognitively impaired individuals (eTables 3 and 4 in the Supplement). Analyses comparing amyloid PET and tau PET across the entire cerebral cortex yielded the same pattern of results, although the results were stronger in magnitude (eTable 6 in the Supplement). In analyses comparing global amyloid PET to tau PET in Braak I-II regions, only p-tau217 and p-tau231 were significantly more closely associated with amyloid PET (eTable 7 in the Supplement). Partial correlation analyses revealed that CSF p-tau biomarkers were more closely associated with amyloid PET when controlling for tau-PET (eTable 8 in the Supplement). The same pattern of results held when controlling for age (eTable 9 in the Supplement) and sex (eTable 10 in the Supplement). Furthermore, CSF p-tau181 in ADNI was more closely correlated with summary measurements of amyloid PET than with summary measurements of tau PET (t value, 2.21; 95% CI, 0.01-0.21; P < .05) (Figure 3). Subgroup analyses are reported in the eTable 11 in the Supplement.
Figure 2. Association of Cerebrospinal Fluid (CSF) Phosphorylated Tau (p-Tau) Biomarkers With Summary Amyloid Positron Emission Tomography (PET) and Tau PET Outcomes.

Scatterplots show the association between CSF p-tau181, p-tau217, p-tau231, p-tau235, and summary measures of amyloid PET and tau PET in the Translational Biomarkers in Aging and Dementia study. ROI indicates region of interest; SUVR, standardized uptake value ratio.
Figure 3. Association of Cerebrospinal Fluid (CSF) Phosphorylated Tau (p-Tau)181 Biomarkers With Summary Amyloid Positron Emission Tomography (PET) and Tau PET in the Alzheimer’s Disease Neuroimaging Initiative.

Scatterplots show the association between CSF p-tau181 and summary measures of [18F]florbetapir amyloid PET and [18F]flortaucipir tau PET in the Alzheimer Disease Neuroimaging Initiative study. ROI indicates region of interest; SUVR, standardized uptake value ratio.
Associations Between Plasma p-Tau and PET Biomarkers
Finally, we investigated associations of plasma concentrations of p-tau181, p-tau217, and p-tau231 with amyloid PET and tau PET in a nonoverlapping subsample in TRIAD (the individuals in the plasma analyses reported here did not undergo CSF p-tau assessments). Voxelwise analyses revealed that plasma p-tau181, p-tau217, and p-tau231 had strong associations with amyloid PET across the neocortex (Figure 4). Furthermore, p-tau181, p-tau217, and p-tau231 were closely associated with summary measures of amyloid-PET uptake (p-tau181, ρ = 0.61; 95% CI, 0.49-0.70; P < .001; p-tau217, ρ = 0.74; 95% CI, 0.66-0.81; P < .001; p-tau231, ρ = 0.62; 95% CI, 0.51-0.73; P < .001). In comparison, associations between plasma concentrations of p-tau181, p-tau217, and p-tau231 with tau PET were lower (p-tau181, ρ = 0.50; 95% CI, 0.39-0.64; P < .001; p-tau217, ρ = 0.64; 95% CI, 0.54-0.73; P < .001; p-tau231, ρ = 0.49; 95% CI, 0.37-0.61; P < .001), including in medial temporal cortices. Comparison of correlations revealed that p-tau181, p-tau217, and p-tau231 were significantly more closely associated with amyloid PET than with tau PET (plasma p-tau181 difference, 11%; 95% CI, 1%-22%; P = .02; p-tau217 difference, 9%; 95% CI, 1%-19%; P = .02; p-tau231 difference, 13%; 95% CI, 3%-24%; P = .009). A summary of the correlation comparisons in the plasma TRIAD sample is provided in eTable 12 in the Supplement. Partial correlation analyses revealed that plasma p-tau biomarkers were more closely associated with amyloid PET when controlling for tau PET (eTable 13 in the Supplement). Results were similar when controlling for age (eTable 14 in the Supplement).
Figure 4. Association of Plasma Phosphorylated Tau (p-Tau) Biomarkers With Amyloid Positron Emission Tomography (PET) and Tau PET.
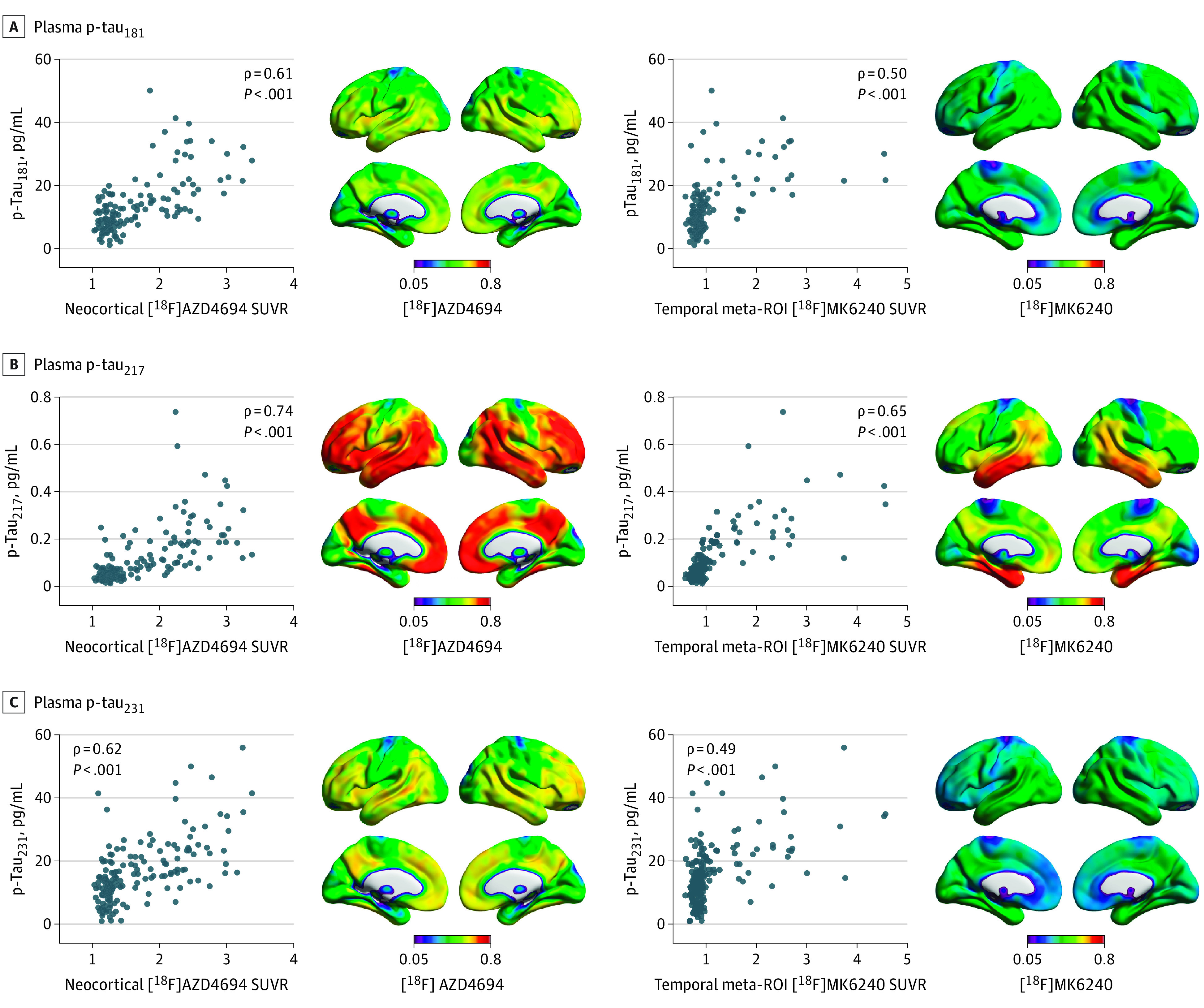
Scatterplots show the association between plasma p-tau181, p-tau217, p-tau231, and summary measures of amyloid PET and tau PET in the Translational Biomarkers in Aging and Dementia study. Brain images show the voxelwise associations of plasma p-tau181, p-tau217, and p-tau231 with [18F]AZD4694 standardized uptake value ratio (SUVR) and [18F]MK6240 SUVR. ROI indicates region of interest.
Discussion
This cross-sectional study of 2 observational cohorts investigated the association between fluid measures of p-tau with amyloid-β plaques and tau neurofibrillary tangles assessed with PET. For all 4 p-tau phosphorylation sites examined in CSF, p-tau was more closely associated with cerebral amyloid-β plaques than with tau neurofibrillary tangles. These results were replicated with plasma p-tau181, p-tau217, and p-tau231 in an independent subsample and with CSF p-tau181 in a large independent cohort of individuals assessed with different amyloid-PET and tau-PET imaging agents. Our findings highlight the need for careful interpretation of p-tau biomarkers in the context of the A/T/(N) biomarker framework and for the biomarker-assisted identification of AD, especially in CU individuals.
Observational studies in humans have reported strong correlations between concentrations of amyloid PET and p-tau at various phosphorylation sites in individuals at different clinical stages of AD.14,17,28,29,30 Strong associations between antemortem plasma p-tau181, p-tau217, and p-tau231 with amyloid-β plaques at autopsy have also been reported.31 In longitudinal observational studies, CU individuals with elevated amyloid-PET burden had increased concentrations of plasma and CSF p-tau217 and p-tau181 in the absence of neocortical tau-PET deposition.16,32,33 Furthermore, soluble p-tau appeared to drive the association between amyloid-β plaques and insoluble tau aggregation measured with PET.16,33 In individuals with dominantly inherited AD, p-tau217 closely followed by p-tau181 increased in response to amyloid-β accumulation, subsequently followed by tau-PET abnormality several years later.15 Furthermore, plasma p-tau181 is elevated in individuals who are amyloid-PET positive but tau-PET negative (even in Braak I regions)32 and is elevated approximately 16 years before the onset of symptoms in dominantly inherited AD.34 Moreover, a study using PET-based Braak staging suggested that both amyloid-PET and p-tau concentrations in CSF plateau at late stages of tangle aggregation,35 in agreement with a recent autopsy study.36 Taken together, these studies provide converging evidence supporting strong associations between amyloid-β plaques and p-tau biomarkers, which both precede widespread neurofibrillary tangle aggregation.
Several recent preclinical studies have reported that soluble p-tau levels in cell media, human tissue samples, and mouse models rise in response to aggregated amyloid-β.37,38,39,40 In vitro models suggest that tau hyperphosphorylation is induced in neurons that take up neuronally secreted amyloid-β.37,38 Amyloid-β plaques are also linked to increased neuronal release of hyperphosphorylated tau.39 Studies in transgenic mice report that p-tau concentrations in CSF rise as a consequence of amyloid-β deposition,40 and human neural stem cell–derived cell culture systems overexpressing APP and PSEN1 induced tau phosphorylation closely linked with amyloid-β concentrations.41 A study using stable isotope labeling kinetics in humans demonstrated that soluble p-tau production was positively correlated with amyloid-PET signal but did not change in the presence of elevated tau PET.42 These studies support increased tau phosphorylation as an early event in the amyloid-β cascade, closely linked with concentrations of amyloid-β pathology.
Recent p-tau biomarker studies have raised questions about the preferential association of various p-tau epitopes with AD stage, severity, and neuropathological hallmarks.43 Tau can be phosphorylated at over 80 different sites on the tau protein,44 and the pathophysiological roles of phosphorylation at different sites are unclear.45 However, recent studies have provided evidence that specific p-tau phosphorylation sites appear to become elevated in a disease stage-dependent manner15,46 and that phosphorylation at specific peptides is associated with increased tau seeding activity and clinical disease progression.47 In our study, p-tau biomarkers were most closely associated with tau aggregation in medial temporal brain regions (though still less so than with global amyloid PET), supporting p-tau as an early biomarker. This result is consistent with a recent community-based study that observed a stronger association between plasma p-tau with entorhinal tau PET than commonly used summary measures of tau PET.48 Of the 4 p-tau biomarkers examined in CSF, p-tau217 and p-tau231 showed the highest association with amyloid PET. In plasma, p-tau217 was most closely associated with cerebral amyloid-PET concentrations. Although site-specific patterns of tau phosphorylation may provide information regarding disease stage in AD, it also will be crucial to understand the contribution of analytical properties of different assays.
Our study highlights the need for a granular approach to tau biomarkers, in which different tau biomarkers provide complementary but not interchangeable information.21,28,45,49,50 Although the tau biomarker category in the A/T/(N) framework currently includes tau PET and p-tau in biofluids,3,4 it is important to draw distinctions between both classes of biomarkers. Tau-PET ligands are considered to bind to insoluble neurofibrillary tangles, consisting of paired helical filament aggregates of hyperphosphorylated tau.51,52 Fluid biomarkers of soluble p-tau, in contrast, measure the concentration of tau phosphorylated at specific serine, threonine, or tyrosine amino acids on the tau protein, which have leaked from the extracellular space into the CSF or blood compartments. CSF and plasma p-tau biomarkers are reported to rise early in the AD pathophysiological process.8,16 Tau tangle aggregation measured with PET occurs later and is strongly predictive of cognitive decline.53 In this connection, the much higher association of p-tau biomarkers with amyloidosis than tangle burden in CU individuals suggests that p-tau biomarkers may be less well-positioned to predict future cognitive decline. In contrast, the high association of p-tau biomarkers with both amyloidosis and tangle burden in individuals with cognitive impairment suggest that abnormal p-tau biomarkers have a strong predictive value for AD in diagnostic settings. Taken together, these results highlight the need to distinguish between biomarkers of phosphorylated and aggregated tau in the A/T/(N) framework, particularly in CU individuals.
Limitations
Results of this study should be interpreted in the context of several limitations. First, tau (hyper)phosphorylation is a dynamic process, the understanding of which is anticipated to evolve with respect to the availability of more biomarkers. Because tau can be phosphorylated at over 80 sites, some of which are hypothesized to have site-specific associations with disease stage, it is unknown whether all future p-tau biomarkers will exhibit the preferential association with amyloid PET reported in this study. Another limitation is that PET biomarker signals (used in this study as measurements of amyloid-β plaques and tau tangles) are influenced by their affinities (1 / equilibrium dissociation constant [Kd]) for their target. However, because [18F]MK6240 has a higher affinity for tau tangles than [18F]AZD4694 does for amyloid-β plaques, the stronger association of p-tau with amyloid PET is unlikely to be driven by sensitivity issues. Replication in an independent cohort (ADNI) with different PET imaging agents helps further attenuate these concerns. Similar to PET biomarkers, biofluid assay performance can affect interpretation of the results in this study. For example, it is unclear to what degree the stronger associations of p-tau217 and p-tau231 with PET biomarkers are driven by biological properties of phosphorylation of a specific amino acid compared with differences in the assays used to detect them (ie, antibody affinity, robustness of individual reagents, assay platform). Other limitations of this study include the lack of availability of plasma p-tau235 in the TRIAD cohort and the lack of availability of plasma p-tau181 at the same time point as tau-PET in ADNI. Furthermore, the TRIAD and ADNI cohorts consist of individuals motivated to participate in a study of AD, which may limit generalizability. Finally, the cohorts are not demographically representative of the populations at risk for dementia in North America.
Conclusions
In conclusion, results of this cross-sectional study of 2 observational cohorts suggest that p-tau biomarkers better reflect the concentration of amyloid-β plaques than cerebral tau pathology quantified with PET. Our findings contribute to the growing understanding of the role of tau phosphorylation in the amyloid-β cascade and highlight the need for careful interpretation of p-tau biomarkers in CU individuals and as outcomes in disease-modifying clinical trials.7
eMethods 1. Positron Emission Tomography Image Acquisition and Processing
eMethods 2. CSF and Plasma Sample Handling and Assays
eResults. Sensitivity Analyses
eFigure 1. Relationship Between CSF p-Tau Biomarkers and Early PET ROIs
eFigure 2. Relationship Between CSF p-Tau Biomarkers and CSF Aβ42/40 and Tau-PET
eFigure 3. Relationship of CSF Aβ42/40 Ratio With Amyloid-PET and Tau-PET
eTable 1. Statistical Comparison of Correlation Between CSF p-Tau Biomarkers and Summary Amyloid- and Tau-PET Biomarkers in TRIAD
eTable 2. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers With CSF Aβ42/40 and Tau-PET Biomarkers in TRIAD
eTable 3. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in CU Individuals in TRIAD
eTable 4. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in CI Individuals in TRIAD
eTable 5. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Early Amyloid- and Tau-PET Biomarkers in TRIAD
eTable 6. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Whole-Cortex Amyloid-PET and Whole-Cortex Tau-PET in TRIAD
eTable 7. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Summary Amyloid-PET and Braak I-II Tau-PET Biomarkers in TRIAD
eTable 8. Statistical Comparison of Partial Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in TRIAD Correcting for Each Other
eTable 9. Statistical Comparison of Partial Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in TRIAD Correcting for Age
eTable 10. Statistical Comparison of CSF p-Tau Associations With Amyloid-PET and Tau-PET in TRIAD Correcting for Sex
eTable 11. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in ADNI
eTable 12. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers and Summary Amyloid-PET and Tau-PET Biomarkers in TRIAD
eTable 13. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers With Amyloid-PET and Tau-PET in TRIAD Correcting for Each Other
eTable 14. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers With Amyloid-PET and Tau-PET in TRIAD Correcting for Age
References
References
- 1.Montine TJ, Phelps CH, Beach TG, et al. ; National Institute on Aging; Alzheimer’s Association . National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease: a practical approach. Acta Neuropathol. 2012;123(1):1-11. doi: 10.1007/s00401-011-0910-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hyman BT, Phelps CH, Beach TG, et al. National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers Dement. 2012;8(1):1-13. doi: 10.1016/j.jalz.2011.10.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jack CR Jr, Bennett DA, Blennow K, et al. A/T/N: an unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology. 2016;87(5):539-547. doi: 10.1212/WNL.0000000000002923 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jack CR Jr, Bennett DA, Blennow K, et al. ; Contributors . NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535-562. doi: 10.1016/j.jalz.2018.02.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rabinovici GD, Gatsonis C, Apgar C, et al. Association of amyloid positron emission tomography with subsequent change in clinical management among Medicare beneficiaries with mild cognitive impairment or dementia. JAMA. 2019;321(13):1286-1294. doi: 10.1001/jama.2019.2000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mintun MA, Lo AC, Duggan Evans C, et al. Donanemab in early Alzheimer’s disease. N Engl J Med. 2021;384(18):1691-1704. doi: 10.1056/NEJMoa2100708 [DOI] [PubMed] [Google Scholar]
- 7.Budd Haeberlein S, Aisen PS, Barkhof F, et al. Two randomized phase 3 studies of aducanumab in early Alzheimer’s disease. J Prev Alzheimers Dis. 2022;9(2):197-210. doi: 10.14283/jpad.2022.30 [DOI] [PubMed] [Google Scholar]
- 8.Mattsson-Carlgren N, Janelidze S, Bateman RJ, et al. Soluble P-tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau. EMBO Mol Med. 2021;13(6):e14022. doi: 10.15252/emmm.202114022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Suárez-Calvet M, Karikari TK, Ashton NJ, et al. ; ALFA Study . Novel tau biomarkers phosphorylated at T181, T217 or T231 rise in the initial stages of the preclinical Alzheimer’s continuum when only subtle changes in Aβ pathology are detected. EMBO Mol Med. 2020;12(12):e12921. doi: 10.15252/emmm.202012921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lantero-Rodriguez J, Snellman A, Benedet AL, et al. P-tau235: a novel biomarker for staging preclinical Alzheimer’s disease. EMBO Mol Med. 2021;13(12):e15098. doi: 10.15252/emmm.202115098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brier MR, Gordon B, Friedrichsen K, et al. Tau and Aβ imaging, CSF measures, and cognition in Alzheimer’s disease. Sci Transl Med. 2016;8(338):338ra66. doi: 10.1126/scitranslmed.aaf2362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pichet Binette A, Franzmeier N, Spotorno N, et al. Amyloid-associated increases in soluble tau is a key driver in accumulation aggregates and cognitive decline in early Alzheimer. medRxiv. Printed posted online January 8, 2022. doi: 10.1101/2022.01.07.22268767 [DOI]
- 13.Janelidze S, Stomrud E, Smith R, et al. Cerebrospinal fluid p-tau217 performs better than p-tau181 as a biomarker of Alzheimer’s disease. Nat Commun. 2020;11(1):1683. doi: 10.1038/s41467-020-15436-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mielke MM, Hagen CE, Xu J, et al. Plasma phospho-tau181 increases with Alzheimer’s disease clinical severity and is associated with tau- and amyloid-positron emission tomography. Alzheimers Dement. 2018;14(8):989-997. doi: 10.1016/j.jalz.2018.02.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barthélemy NR, Li Y, Joseph-Mathurin N, et al. ; Dominantly Inherited Alzheimer Network . A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzheimer’s disease. Nat Med. 2020;26(3):398-407. doi: 10.1038/s41591-020-0781-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mattsson-Carlgren N, Andersson E, Janelidze S, et al. Aβ deposition is associated with increases in soluble and phosphorylated tau that precede a positive Tau PET in Alzheimer’s disease. Sci Adv. 2020;6(16):eaaz2387. doi: 10.1126/sciadv.aaz2387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hansson O. Biomarkers for neurodegenerative diseases. Nat Med. 2021;27(6):954-963. doi: 10.1038/s41591-021-01382-x [DOI] [PubMed] [Google Scholar]
- 18.Ashton NJ, Benedet AL, Pascoal TA, et al. Cerebrospinal fluid p-tau231 as an early indicator of emerging pathology in Alzheimer’s disease. EBioMedicine. 2022;76:103836. doi: 10.1016/j.ebiom.2022.103836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Therriault J, Benedet AL, Pascoal TA, et al. Association of apolipoprotein E ε4 with medial temporal tau independent of amyloid-β. JAMA Neurol. 2020;77(4):470-479. doi: 10.1001/jamaneurol.2019.4421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183-194. doi: 10.1111/j.1365-2796.2004.01388.x [DOI] [PubMed] [Google Scholar]
- 21.Mattsson-Carlgren N, Leuzy A, Janelidze S, et al. The implications of different approaches to define AT(N) in Alzheimer disease. Neurology. 2020;94(21):e2233-e2244. doi: 10.1212/WNL.0000000000009485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Alzheimer’s Disease Neuroimaging Initiative . Alzheimer’s Disease Neuroimaging Initiative home page. Accessed February 7, 2022. https://adni.loni.usc.edu/
- 23.Diedenhofen B, Musch J. Cocor: a comprehensive solution for the statistical comparison of correlations. PLoS One. 2015;10(3):e0121945. doi: 10.1371/journal.pone.0121945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Palmqvist S, Schöll M, Strandberg O, et al. Earliest accumulation of β-amyloid occurs within the default-mode network and concurrently affects brain connectivity. Nat Commun. 2017;8(1):1214-1226. doi: 10.1038/s41467-017-01150-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sperling RA, Mormino EC, Schultz AP, et al. The impact of amyloid-beta and tau on prospective cognitive decline in older individuals. Ann Neurol. 2019;85(2):181-193. doi: 10.1002/ana.25395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hanseeuw BJ, Betensky RA, Jacobs HIL, et al. Association of amyloid and tau with cognition in preclinical Alzheimer disease: a longitudinal study. JAMA Neurol. 2019;76(8):915-924. doi: 10.1001/jamaneurol.2019.1424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Quiroz YT, Sperling RA, Norton DJ, et al. Association between amyloid and tau accumulation in young adults with autosomal dominant Alzheimer disease. JAMA Neurol. 2018;75(5):548-556. doi: 10.1001/jamaneurol.2017.4907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ossenkoppele R, Reimand J, Smith R, et al. ; Alzheimer’s Disease Neuroimaging Initiative . Tau PET correlates with different Alzheimer’s disease-related features compared to CSF and plasma p-tau biomarkers. EMBO Mol Med. 2021;13(8):e14398. doi: 10.15252/emmm.202114398 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Schindler SE, Li Y, Todd KW, et al. ; Dominantly Inherited Alzheimer Network . Emerging cerebrospinal fluid biomarkers in autosomal dominant Alzheimer’s disease. Alzheimers Dement. 2019;15(5):655-665. doi: 10.1016/j.jalz.2018.12.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Palmqvist S, Insel PS, Stomrud E, et al. Cerebrospinal fluid and plasma biomarker trajectories with increasing amyloid deposition in Alzheimer’s disease. EMBO Mol Med. 2019;11(12):e11170. doi: 10.15252/emmm.201911170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Salvadó G, Ossenkoppele R, Ashton NJ, Beach TG. Specific associations between plasma biomarkers and postmortem amyloid plaque and neurofibrillary tau tangle loads. medRxiv. Preprint posted online August 22, 2022. doi: 10.1101/2022.08.22.22279052 [DOI] [PMC free article] [PubMed]
- 32.Karikari TK, Pascoal TA, Ashton NJ, et al. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol. 2020;19(5):422-433. doi: 10.1016/S1474-4422(20)30071-5 [DOI] [PubMed] [Google Scholar]
- 33.Janelidze S, Berron D, Smith R, et al. Associations of plasma phospho-tau217 levels with tau positron emission tomography in early Alzheimer disease. JAMA Neurol. 2021;78(2):149-156. doi: 10.1001/jamaneurol.2020.4201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.O’Connor A, Karikari TK, Poole T, et al. Plasma phospho-tau181 in presymptomatic and symptomatic familial Alzheimer’s disease: a longitudinal cohort study. Mol Psychiatry. 2021;26(10):5967-5976. doi: 10.1038/s41380-020-0838-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Therriault J, Pascoal TA, Lussier FZ, et al. Biomarker modeling of Alzheimer’s disease using PET-based Braak staging. Nat Aging. 2022;2:526-535. doi: 10.1038/s43587-022-00204-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bridel C, Somers C, Sieben A, et al. Associating Alzheimer’s disease pathology with its cerebrospinal fluid biomarkers. Brain. Published online January 13, 2022. doi: 10.1093/brain/awac013 [DOI] [PubMed] [Google Scholar]
- 37.Venkatramani A, Panda D. Regulation of neuronal microtubule dynamics by tau: implications for tauopathies. Int J Biol Macromol. 2019;133:473-483. doi: 10.1016/j.ijbiomac.2019.04.120 [DOI] [PubMed] [Google Scholar]
- 38.Zhang F, Gannon M, Chen Y, et al. β-amyloid redirects norepinephrine signaling to activate the pathogenic GSK3β/tau cascade. Sci Transl Med. 2020;12(526):eaay6931. doi: 10.1126/scitranslmed.aay6931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.He Z, Guo JL, McBride JD, et al. Amyloid-β plaques enhance Alzheimer’s brain tau-seeded pathologies by facilitating neuritic plaque tau aggregation. Nat Med. 2018;24(1):29-38. doi: 10.1038/nm.4443 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Maia LF, Kaeser SA, Reichwald J, et al. Changes in amyloid-β and Tau in the cerebrospinal fluid of transgenic mice overexpressing amyloid precursor protein. Sci Transl Med. 2013;5(194):194re2. doi: 10.1126/scitranslmed.3006446 [DOI] [PubMed] [Google Scholar]
- 41.Choi SH, Kim YH, Hebisch M, et al. A 3-dimensional human neural cell culture model of Alzheimer’s disease. Nature. 2014;515(7526):274-278. doi: 10.1038/nature13800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Sato C, Barthélemy NR, Mawuenyega KG, et al. Tau kinetics in neurons and the human central nervous system. Neuron. 2018;97(6):1284-1298.e7. doi: 10.1016/j.neuron.2018.02.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Therriault J, Zimmer ER, Benedet AL, Pascoal TA, Gauthier S, Rosa-Neto P. Staging of Alzheimer’s disease: past, present, and future perspectives. Trends Mol Med. 2022;28(9):726-741. doi: 10.1016/j.molmed.2022.05.008 [DOI] [PubMed] [Google Scholar]
- 44.Wang JZ, Xia YY, Grundke-Iqbal I, Iqbal K. Abnormal hyperphosphorylation of tau: sites, regulation, and molecular mechanism of neurofibrillary degeneration. J Alzheimers Dis. 2013;33(suppl 1):S123-S139. doi: 10.3233/JAD-2012-129031 [DOI] [PubMed] [Google Scholar]
- 45.Wegmann S, Biernat J, Mandelkow E. A current view on tau protein phosphorylation in Alzheimer’s disease. Curr Opin Neurobiol. 2021;69:131-138. doi: 10.1016/j.conb.2021.03.003 [DOI] [PubMed] [Google Scholar]
- 46.Mielke MM, Frank RD, Dage JL, et al. Comparison of plasma phosphorylated tau species with amyloid and tau positron emission tomography, neurodegeneration, vascular pathology, and cognitive outcomes. JAMA Neurol. 2021;78(9):1108-1117. doi: 10.1001/jamaneurol.2021.2293 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Dujardin S, Commins C, Lathuiliere A, et al. Tau molecular diversity contributes to clinical heterogeneity in Alzheimer’s disease. Nat Med. 2020;26(8):1256-1263. doi: 10.1038/s41591-020-0938-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Mielke MM, Dage JL, Frank RD, et al. Performance of plasma phosphorylated tau 181 and 217 in the community. Nat Med. 2022;28(7):1398-1405. doi: 10.1038/s41591-022-01822-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Meyer PF, Pichet Binette A, Gonneaud J, Breitner JCS, Villeneuve S. Characterization of Alzheimer disease biomarker discrepancies using cerebrospinal fluid phosphorylated tau and AV1451 positron emission tomography. JAMA Neurol. 2020;77(4):508-516. doi: 10.1001/jamaneurol.2019.4749 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Groot C, Smith R, Stomrud E, et al. Phospho-tau with subthreshold tau-PET predicts increased tau accumulation rates in amyloid-positive individuals. Brain. Published online September 9, 2022. doi: 10.1093/brain/awac329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Villemagne VL, Doré V, Burnham SC, Masters CL, Rowe CC. Imaging tau and amyloid-β proteinopathies in Alzheimer disease and other conditions. Nat Rev Neurol. 2018;14(4):225-236. doi: 10.1038/nrneurol.2018.9 [DOI] [PubMed] [Google Scholar]
- 52.Shi Y, Murzin AG, Falcon B, et al. Cryo-EM structures of tau filaments from Alzheimer’s disease with PET ligand APN-1607. Acta Neuropathol. 2021;141(5):697-708. doi: 10.1007/s00401-021-02294-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ossenkoppele R, Pichet Binette A, Groot C, et al. Amyloid and tau PET positive cognitively unimpaired individuals: destined to decline? medRxiv. Preprint posted online May 25, 2022. doi: 10.1101/2022.05.23.22275241 [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods 1. Positron Emission Tomography Image Acquisition and Processing
eMethods 2. CSF and Plasma Sample Handling and Assays
eResults. Sensitivity Analyses
eFigure 1. Relationship Between CSF p-Tau Biomarkers and Early PET ROIs
eFigure 2. Relationship Between CSF p-Tau Biomarkers and CSF Aβ42/40 and Tau-PET
eFigure 3. Relationship of CSF Aβ42/40 Ratio With Amyloid-PET and Tau-PET
eTable 1. Statistical Comparison of Correlation Between CSF p-Tau Biomarkers and Summary Amyloid- and Tau-PET Biomarkers in TRIAD
eTable 2. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers With CSF Aβ42/40 and Tau-PET Biomarkers in TRIAD
eTable 3. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in CU Individuals in TRIAD
eTable 4. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in CI Individuals in TRIAD
eTable 5. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Early Amyloid- and Tau-PET Biomarkers in TRIAD
eTable 6. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Whole-Cortex Amyloid-PET and Whole-Cortex Tau-PET in TRIAD
eTable 7. Statistical Comparison of Correlations Between CSF p-Tau Biomarkers and Summary Amyloid-PET and Braak I-II Tau-PET Biomarkers in TRIAD
eTable 8. Statistical Comparison of Partial Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in TRIAD Correcting for Each Other
eTable 9. Statistical Comparison of Partial Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in TRIAD Correcting for Age
eTable 10. Statistical Comparison of CSF p-Tau Associations With Amyloid-PET and Tau-PET in TRIAD Correcting for Sex
eTable 11. Statistical Comparison of Correlations Between CSF p-Tau With Amyloid-PET and Tau-PET in ADNI
eTable 12. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers and Summary Amyloid-PET and Tau-PET Biomarkers in TRIAD
eTable 13. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers With Amyloid-PET and Tau-PET in TRIAD Correcting for Each Other
eTable 14. Statistical Comparison of Correlations Between Plasma p-Tau Biomarkers With Amyloid-PET and Tau-PET in TRIAD Correcting for Age
References