

Key Points
Question
Are rapid-onset opioids noninferior to rapid-onset neuromuscular blockers for rapid sequence intubation in the operating room among adults at risk of aspiration?
Findings
In this noninferiority randomized clinical trial that included 1150 participants, the rate of tracheal intubation on first attempt without major complications was 66.1% in the remifentanil group and 71.6% in the neuromuscular blocker group, a difference that did not meet the prespecified noninferiority margin of −7% and was consistent with statistical inferiority of remifentanil.
Meaning
Among adults at risk of aspiration during rapid sequence intubation in the operating room, remifentanil did not meet the criterion for noninferiority and was statistically inferior to neuromuscular blockers with regard to the rate of successful tracheal intubation without major complications, although the wide confidence interval limits conclusions about the difference.
Abstract
Importance
It is uncertain whether a rapid-onset opioid is noninferior to a rapid-onset neuromuscular blocker during rapid sequence intubation when used in conjunction with a hypnotic agent.
Objective
To determine whether remifentanil is noninferior to rapid-onset neuromuscular blockers for rapid sequence intubation.
Design, Setting, and Participants
Multicenter, randomized, open-label, noninferiority trial among 1150 adults at risk of aspiration (fasting for <6 hours, bowel occlusion, recent trauma, or severe gastroesophageal reflux) who underwent tracheal intubation in the operating room at 15 hospitals in France from October 2019 to April 2021. Follow-up was completed on May 15, 2021.
Interventions
Patients were randomized to receive neuromuscular blockers (1 mg/kg of succinylcholine or rocuronium; n = 575) or remifentanil (3 to 4 μg/kg; n = 575) immediately after injection of a hypnotic.
Main Outcomes and Measures
The primary outcome was assessed in all randomized patients (as-randomized population) and in all eligible patients who received assigned treatment (per-protocol population). The primary outcome was successful tracheal intubation on the first attempt without major complications, defined as lung aspiration of digestive content, oxygen desaturation, major hemodynamic instability, sustained arrhythmia, cardiac arrest, and severe anaphylactic reaction. The prespecified noninferiority margin was 7.0%.
Results
Among 1150 randomized patients (mean age, 50.7 [SD, 17.4] years; 573 [50%] women), 1130 (98.3%) completed the trial. In the as-randomized population, tracheal intubation on the first attempt without major complications occurred in 374 of 575 patients (66.1%) in the remifentanil group and 408 of 575 (71.6%) in the neuromuscular blocker group (between-group difference adjusted for randomization strata and center, –6.1%; 95% CI, –11.6% to –0.5%; P = .37 for noninferiority), demonstrating inferiority. In the per-protocol population, 374 of 565 patients (66.2%) in the remifentanil group and 403 of 565 (71.3%) in the neuromuscular blocker group had successful intubation without major complications (adjusted difference, –5.7%; 2-sided 95% CI, –11.3% to –0.1%; P = .32 for noninferiority). An adverse event of hemodynamic instability was recorded in 19 of 575 patients (3.3%) with remifentanil and 3 of 575 (0.5%) with neuromuscular blockers (adjusted difference, 2.8%; 95% CI, 1.2%-4.4%).
Conclusions and Relevance
Among adults at risk of aspiration during rapid sequence intubation in the operating room, remifentanil, compared with neuromuscular blockers, did not meet the criterion for noninferiority with regard to successful intubation on first attempt without major complications. Although remifentanil was statistically inferior to neuromuscular blockers, the wide confidence interval around the effect estimate remains compatible with noninferiority and limits conclusions about the clinical relevance of the difference.
Trial Registration
ClinicalTrials.gov Identifier: NCT03960801
This randomized trial assesses the effect of remifentanil vs neuromuscular blockers on successful intubation without major complications among patients at risk of aspiration during rapid sequence intubation in the operating room.
Introduction
Aspiration of gastric contents is a rare but severe complication of general anesthesia, resulting in respiratory failure and increased risk of death.1 Tracheal intubation is an effective way to protect the lungs from aspiration, but this procedure can be performed only after induction of anesthesia. Rapid sequence intubation is the standard anesthetic procedure for the tracheal intubation of patients at risk of aspiration. It usually combines optimal preoxygenation with a hypnotic agent and rapid-onset neuromuscular blockers to rapidly achieve excellent intubation conditions. Succinylcholine and high-dose rocuronium are recommended to manage difficult airways because they enable myorelaxation in less than 90 seconds.2,3
High variability in the modalities of rapid sequence intubation has been reported in national surveys and randomized clinical trials published between 2015 and 2020.4,5,6,7,8 Rapid sequence intubation without neuromuscular blockers was performed in 25% to 75% of patients at risk of aspiration.4,5,6,7,8 This observation is possibly explained by concerns about potential severe adverse effects of neuromuscular blockers, including anaphylaxis,9 prolonged curarisation,10 metabolic disturbance,11 and postoperative respiratory complications.12 However, even if rapid sequence intubation without neuromuscular blockers is frequently performed in clinical practice, its noninferiority has not been demonstrated yet.13
In small studies, the combined use of hypnotic agents with remifentanil, a rapid-onset opioid, provides satisfactory tracheal intubation conditions in less than 90 seconds,14,15 suggesting that this combination may be a potential candidate for rapid sequence intubation without neuromuscular blockers. This study was therefore designed to test the hypothesis in a randomized clinical trial that the combined use of remifentanil with hypnotics is not inferior to the combination of rapid-onset neuromuscular blockers with hypnotics to achieve successful tracheal intubation on the first attempt without major complications in patients at risk of aspiration of gastric contents in the operating room.
Methods
Design
From October 2019 to May 2021, an investigator-initiated, multicenter, parallel-group, open-label, randomized noninferiority clinical trial was conducted to compare remifentanil vs rapid-onset neuromuscular blockers used in conjunction with a hypnotic agent during rapid sequence intubation of patients at risk of aspiration of gastric contents.
Ethical Review
The trial was conducted under the Declaration of Helsinki16 and was registered in May 2019. The trial protocol was approved in July 2019 by an institutional review board (Comité de Protection des Personnes Sud-Ouest et Outre-Mer II). All patients provided written informed consent before participation, either during the preoperative anesthetic medical consultation or immediately before entering the operating room. The study protocol and the statistical analysis plan (available in Supplement 1) were submitted before the first inclusion in the study and were published before the conclusion of enrollment.17
Study Oversight
The study sponsor (CHU Nantes) conducted the statistical analyses, coordinated the operational processes, and conducted data monitoring and quality checks. Investigators declared adverse events within 7 days. Patient safety was regularly monitored by an independent data and safety monitoring board, who analyzed adverse event reports in a blinded manner.
Trial Sites and Study Population
The study was conducted in 15 French private and university hospitals. Patients aged 18 to 80 years requiring orotracheal intubation during general anesthesia in the operating room were eligible for enrollment if they had 1 or more of the following risk factors for pulmonary aspiration18,19: a preoperative fasting period of less than 6 hours, bowel occlusion, a vomiting episode within the 12 hours prior to anesthesia, orthopedic trauma within the last 12 hours, or a medical history of severe symptomatic gastroesophageal reflux, hiatus hernia, gastroparesis, dysautonomia, or gastroesophageal surgery with sphincter dysfunction. Noninclusion criteria were pregnancy (legal obligation), guardianship (legal obligation), contraindication to use of succinylcholine and rocuronium (allergy, malignant hyperthermia, congenital muscular dystrophy, myasthenia gravis, congenital deficit in plasma pseudocholinesterase), predicted difficulty with tracheal intubation, preoperative hypoxemia (pulse oximetry oxygen saturation <95%) or hemodynamic shock (mean arterial pressure <65 mm Hg), cardiac arrest, or absence of insurance to cover health costs (legal obligation).
Randomization
A secure web-based randomization system was used. Patients were randomized (1:1 ratio) immediately before the procedure in permuted blocks of size of 4 or 6, with stratification based on the device planned for the first laryngoscopy (direct laryngoscopy vs video laryngoscopy), which can affect the rate of tracheal intubation success on first attempt,20,21 and on bowel occlusion (yes vs no), which is a significant risk factor for lung aspiration.22 The randomization list was generated by a methodologist not involved in determining patient eligibility or outcome assessment.
Trial Intervention
For patients assigned to the remifentanil group, remifentanil (3 to 4 μg/kg) was intravenously injected immediately after administration of a hypnotic, and the tracheal intubation was initiated 30 to 60 seconds after administration of remifentanil without injecting neuromuscular blockers before the first intubation attempt (eFigure 1 in Supplement 2).
For patients assigned to the neuromuscular blocker group, a rapid-onset paralytic agent (1 mg/kg succinylcholine or 1 mg/kg rocuronium) was intravenously injected immediately after administering a hypnotic. The tracheal intubation was initiated 30 to 60 seconds after administration of the neuromuscular blocker without injecting morphine derivatives before the first intubation attempt. Succinylcholine was the first-choice neuromuscular blocker,23 and rocuronium was recommended in the case of contraindication of use of succinylcholine.
In the case of desaturation or unplanned difficult tracheal intubation, physicians could use remifentanil or a rapid-onset neuromuscular blocker as rescue therapy.
Standard Care for Intubation
The procedure was performed by senior anesthesiologists, anesthesiologist junior residents with more than 2 years of experience, or nurses specialized in anesthesiology. To avoid extremes in practice, investigators were asked to follow the French guidelines for neuromuscular blockers and reversal24 and recommendations for unplanned difficult tracheal intubation.2,3 In both groups, induction of general anesthesia was performed after 3 minutes of preoxygenation. The choice and the dose of the hypnotic depended on physicians’ preferences. The use of alternative airway procedures such as a stylet for tracheal intubation,25 applications of a Sellick maneuver,26 and bag-mask ventilation during the apneic period27 are not recommended in France and were not mandatory on the first tracheal intubation attempt. Rescue mask facial ventilation was recommended in the case of unplanned difficult intubation and oxygen saturation decreasing below 95%.2 To limit the risk of bias, the device used for the first laryngoscopy was a priori chosen before randomization and group attribution according to physicians’ preferences.
Outcomes
The primary outcome measure was successful tracheal intubation on the first attempt without any major complications.17 First-attempt intubation success was defined as successful endotracheal tube placement during the first laryngoscope insertion. The major complications were recorded up to 10 minutes after induction of anesthesia and were defined as lung aspiration of digestive content (defined as the visualization by an investigator of liquid or solid particles reaching the larynx during the intubation procedure), oxygen desaturation to less than 95%, major hemodynamic instability (duration and number of episodes of mean arterial pressure ≤50 mm Hg or ≥110 mm Hg), sustained arrhythmia (heart rate or rhythm alteration requiring pharmacological or electrical intervention, lasting more than 30 seconds, and not present at the time of study enrollment), cardiac arrest, and severe anaphylactic reaction (severity grade III-IV: hypotension, bronchospasm, cardiac arrhythmia, or cardiac arrest). A typing error in the primary outcome definition in the initial study protocol (version 1, June28, 2019; ≤2 laryngoscopic attempts) was corrected in version 2 of the study protocol (November 25, 2019; <2 laryngoscopic attempts, ie, intubation success on the first attempt) to align with the registration on ClinicalTrials.gov (May 23, 2019). Supplement 1 contains the history of protocol modifications and the study protocol summary published on August 4, 2020.17
The prespecified secondary outcomes included details of patient preoxygenation, patient position, presence of nasogastric tube, and use of gastric ultrasound prior to intubation. Secondary outcomes recorded within the first 10 minutes after anesthesia induction included Intubation Difficulty Score 3 (range, 0 [easy intubation] to infinity [intubation impossible]; a score between 0 and 5 indicates moderate to major difficulty); Cormack score, evaluated during direct laryngoscopy (a 4-grade score ranging from 1 [ full view of the glottis] to 4 [neither glottis nor epiglottis was seen]); percentage of glottic opening score during video laryngoscopy (percentile of the glottic opening view ranging from 0% to 100% of glottis visualization); delays between anesthetic induction and successful tracheal intubation (defined as sixth capnography curve); rates of use of alternative techniques for intubation; frequencies of moderate or severe desaturation (80%-95% and <80%, respectively); minimal pulse oximetry oxygen saturation value; rates of severe hemodynamic reaction (defined as heart rate <45/min or >110/min or systolic blood pressure <80 mm Hg or >160 mm Hg); proportions of patients with nonsevere anaphylactic reaction (grade I-II); and rates of patients with cough requiring sedation increase. The following secondary outcomes were recorded in the recovery room: rates of postoperative nausea and vomiting; postoperative sore throat immediately after tracheal extubation (postoperative laryngeal visual analog scale pain score ranging from 0 [no pain] to [unbearable pain]); percentage of patients with laryngeal dyspnea/stridor; rates of patients requiring postextubation mechanical ventilation support; rates of extubating failure; and rates of postoperative desaturation of 92% or less or less than 80%. The following secondary outcomes were also recorded up to day 7: rates of teeth and tracheal trauma, rates of postoperative pneumonia, rates of acute respiratory distress syndrome, and in-hospital mortality.
Post hoc outcomes included the rates of the primary outcome components (including intubation success on the first attempt), doses of vasopressors during the first 10 minutes after anesthesia induction, frequencies of neuromuscular blocker monitoring and reversal, and rates of postoperative aspiration and emergency admission in an intensive critical unit.
To limit missing data, a trained technician research assistant or an independent observer not involved in the intubation procedure prospectively collected outcome data on a standardized collection form from randomization until discharge from the recovery room. After discharge from the operating room, additional data were collected by intubating physicians or technician research assistants.
Sample Size Calculation
The proportion of rapid sequence intubations without major complications varied between 55% and 92% in recent studies.4,25,27,28,29 The intergroup difference used to power trials comparing successful intubation on the first attempt was between 5% and 9% in recent superiority trials.25,30 We thus deemed it reasonable that 80% of patients in the neuromuscular blocker group would have tracheal intubation without major complications and therefore set a noninferiority margin of 7 percentage points (ie, a relative difference of 8.75%), which was similar to that defined in a noninferiority trial comparing neuromuscular blockers for out-of-hospital tracheal intubation.23 With a 2.5% α risk, including 575 patients in each group (1150 in total) was required to provide 80% power to show noninferiority using the lower bound of the 2-sided 95% CI of the percentage difference in proportions of patients successfully intubated after the first attempt and free of major complications.
Statistical Analysis
Following international guidelines for interpretation of noninferiority trials,31,32 the primary outcome analysis was performed in the as-randomized population, and the data set for the per-protocol analysis was considered of equal importance to reach robust interpretation. The primary outcome analysis was thus undertaken in the as-randomized population analyzing all patients in the groups to which they were randomized, and under the per-protocol principle, analyzing all randomly assigned patients in the group to which they were randomized excluding those withdrawn consent, those who would not have been eligible for randomization according to the inclusion/noninclusion criteria, those who did not receive the assigned study treatment, and those without data for the primary outcome.
For the primary end point, the difference between the 2 study groups (with 2-sided 95% confidence interval) was estimated for the absolute proportion of successful tracheal intubations on the first attempt without major complications. The adjusted proportion and related confidence intervals in each group were estimated by a mixed-effects logistic regression model taking into account the randomization stratification factors (device for laryngoscopy and bowel occlusion) and accounting for centers as a random effect. The risk difference and related 95% confidence interval were then obtained using the Wald method.
In prespecified subgroup analyses, we compared the proportions of patients achieving the primary outcome using an adjusted logistic regression with the same adjustment variables as the primary outcome analysis (device for laryngoscopy, bowel obstruction, and centers as random effects, except when they define a subgroup): direct laryngoscopy vs video laryngoscopy, digestive occlusion vs other risk factors of aspiration, age (18-39, 40-59, or 60-80 years), Mallampati score ((I-II: the palate and uvula are visible; III-IV: only the base of the uvula or the hard palate are visible), urgent vs nonurgent procedure, body mass index (≤30 or >30; calculated as weight in kilograms divided by height in meters squared), American Society of Anesthesiologists Physical Status Classification System (ASA) score (I-II vs III-IV), and choice of hypnotic (propofol vs others). The interactions between the treatment effect and subgroup covariates were tested with mixed-effects logistic regression models adjusted with the same factors as the primary analysis. As exploratory post hoc analyses, the rates of the primary outcome in the study groups were compared across participating hospitals, and a time-series analysis using a linear regression model evaluated the secular trend during the inclusion period. The rates of primary outcomes in patients receiving low (<3.5 μg/kg) vs high (≥3.5 μg/kg) doses of remifentanil were also compared a posteriori.
To manage missing data, analysis of the primary outcome in the as-randomized population was performed by multiple imputation methods (10 imputations; relative efficiency of the imputation >99%). χ2 and t tests were performed to include all the variables statistically associated with the primary outcome or the treatment group in the multiple imputation model. P < .05 was considered statistically significant. The final multiple imputation model was based on age; body mass index; medical history of ischemic cardiomyopathy, arterial hypertension, chronic pulmonary obstructive disease, asthma, or stroke; ASA score; and urgent surgery (yes vs no).
Secondary end points were compared between the 2 study groups using mixed-effects logistic regression models for binary data (eg, postoperative pneumonia, postoperative respiratory distress) and mixed-effects linear regression models for continuous data (eg, time to successful intubation, intubation difficulty scores). For secondary end points, all analyses were performed with superiority testing with a 2-sided α = .05 and were adjusted for stratification factors and account centers as a random effect. Because of the potential for type I error due to multiple comparisons, findings of secondary end points should be interpreted as exploratory. All analyses were conducted using SAS version 9.4 (SAS Institute Inc).
Continuous variables are presented as mean and standard deviations or median and interquartile ranges. Categorical data are presented as exact counts and percentages.
Results
Trial Population
From October 2019 to April 2021, 1150 patients underwent randomization (575 patients in the remifentanil group and 575 in the neuromuscular blocker group). Among the 1150 randomized patients, 20 (1.7%) were excluded from the per-protocol analyses: 16 patients met noninclusion criteria, 3 did not receive the allocated treatment, and 1 had missing data for the primary outcome (Figure 1). Patient characteristics at baseline are reported in Table 1. Digestive occlusion, ileus, or vomiting were recorded in 613 (54.1%) patients, and digestive procedures were the most frequent reason for intubation.
Figure 1. Participant Flow.

Data collection of the number of patients assessed for eligibility was not planned during the trial and these data are not available.
aMultiple imputation model based on age, body mass index, medical history of ischemic cardiomyopathy, arterial hypertension, chronic pulmonary obstructive disease, asthma, or stroke, American Society of Anesthesiology Physical Status Classification System score, and urgent surgery (yes vs no).
bDid not require general anesthesia (inclusion criterion) (n = 1), did not require orotracheal intubation (inclusion criterion) (n = 2), or did not undergo surgery (n = 2).
cDid not require orotracheal intubation (inclusion criterion) (n = 1), preoperative hypoxemia (noninclusion criterion) (n = 1), or patient enrolled twice in the study (n = 2).
Table 1. Baseline Participant Characteristics.
| Characteristics | Remifentanil group (n = 575) | Neuromuscular blocker group (n = 575) |
|---|---|---|
| Age, mean (SD), y | 49.6 (17.9) [n = 573] | 51.7 (16.9) [n = 572] |
| Sex, No./total (%) | ||
| Female | 282/573 (49.2) | 291/572 (50.9) |
| Male | 291/573 (50.8) | 281/572 (49.1) |
| Weight, mean (SD), kg | 77.2 (19.8) | 75.6 (19.0) |
| Body mass index, mean (SD)a | 26.7 (6.7) | 26.4 (6.4) |
| Medical history, No./total (%) | ||
| Smoking | 137/561 (24.4) | 112/556 (20.1) |
| Arterial hypertension | 133/571 (23.3) | 131/570 (23.0) |
| Diabetes | 58/572 (10.1) | 59/570 (10.4) |
| Obstructive sleep apnea | 48/566 (8.5) | 39/567 (6.9) |
| Asthma | 41/572 (7.2) | 32/570 (5.6) |
| Stroke | 26/572 (4.5) | 18/572 (3.1) |
| Ischemic cardiomyopathy | 21/571 (3.7) | 29/572 (5.1) |
| Chronic obstructive pulmonary disease | 21/571 (3.7) | 20/570 (3.5) |
| Chronic kidney failure | 19/572 (3.3) | 19/572 (3.3) |
| Cardiac rhythm abnormality | 18/571 (3.2) | 31/571 (5.4) |
| Liver cirrhosis | 13/571 (2.3) | 11/571 (1.9) |
| Cardiac insufficiency | 8/572 (1.4) | 8/572 (1.4) |
| Suspected or confirmed COVID-19 infection, No./total (%) | 2/400 (0.5) | 3/401 (0.7) |
| American Society of Anesthesiologists Physical Status Classification System score, No./total (%) | ||
| I (healthy) | 196/573 (34.2) | 186/572 (32.5) |
| II (mild systemic disease without significant functional limitation) | 265/573 (46.2) | 275/572 (48.1) |
| III (severe systemic disease with significant functional limitation) | 104/573 (18.2) | 107/572 (18.7) |
| IV (severe systemic disease with constant threat to life) | 8/573 (1.4) | 4/572 (0.7) |
| Timing of surgery, No./total (%) | ||
| Urgent or semiurgent | 343/573 (59.9) | 349/572 (61.0) |
| Scheduled | 230/573 (40.1) | 223/572 (39.0) |
| Type of surgery, No./total (%) | ||
| Digestive | 296/573 (51.7) | 284/572 (49.7) |
| Endoscopy or radiointerventional | 117/573 (20.4) | 112/572 (19.6) |
| Orthopedic | 39/573 (6.8) | 64/572 (11.2) |
| Severe trauma/burns | 38/573 (6.6) | 35/572 (6.1) |
| Urological | 34/573 (5.9) | 34/572 (5.9) |
| Ear, nose, and throat | 8/573 (1.4) | 4/572 (0.7) |
| Otherb | 41/573 (7.2) | 39/572 (6.8) |
| Risk factors for pulmonary aspiration, No./total (%) | ||
| Digestive intake, h | ||
| <6 | 54/527 (10.2) | 48/530 (9.1) |
| 6-12 | 129/527 (24.5) | 149/530 (28.1) |
| >12 | 344/568 (65.3) | 333/566 (62.8) |
| Ileus, bowel occlusion, vomiting | 309/571 (54.4) | 304/571 (53.7) |
| Orthopedic trauma <12 h | 34/571 (6.0) | 55/571 (9.6) |
| Severe chronic gastric dysfunctionc | 276/571 (48.3) | 256/671 (44.8) |
| Risk factors for difficult tracheal intubation, No./total (%) | ||
| History of difficult tracheal intubation | 12/552 (2.2) | 8/561 (1.4) |
| Mallampati score | ||
| I (soft palate, uvula, pillars visible) | 302/561 (53.8) | 306/557 (54.9) |
| II (soft palate, major part of uvula visible) | 205/561 (36.5) | 201/557 (36.1) |
| III (soft palate, base of uvula visible) | 45/561 (8.0) | 46/557 (8.3) |
| IV (only hard palate visible) | 9/561 (1.6) | 4/557 (0.7) |
| Thyroid-chin distance <65 mm | 10/567 (1.8) | 9/560 (1.6) |
| Buccal opening <35 mm | 16/565 (2.8) | 6/561 (1.1) |
| Cervical mobility ≤35° | 15/563 (2.7) | 9/558 (1.6) |
| Risk factors for difficult mask ventilation, No./total (%) | ||
| Self-perceived snoring | 90/491 (18.3) | 89/509 (17.5) |
| Has beard | 54/572 (9.4) | 42/571 (7.4) |
| Missing dentition | 46/573 (8.0) | 67/570 (11.8) |
| Retrognathia | 5/567 (0.9) | 12/564 (2.1) |
| Baseline vital signs | ||
| Pulse oximetry oxygen saturation, mean (SD), % | 97.8 (2.2) | 97.8 (2.2) |
| Systolic blood pressure, mean (SD), mm Hg | 135 (21) | 136 (22) |
| Diastolic blood pressure, mean (SD), mm Hg | 77 (13) | 78 (13) |
| Blood pressure, mean (SD), mm Hg | 94 (15) | 95 (16) |
| Heart rate, /min | ||
| Mean (SD) | 82 (16) | 81 (17) |
| >100, No./total (%) | 68/562 (12.1) | 73/564 (12.9) |
| <65, No./total (%) | 32/562 (5.7) | 42/564 (7.5) |
| Hypertension (systolic blood pressure >140 mm Hg), No./total (%) | 196/561 (34.9) | 222/562 (39.5) |
| Hypotension (systolic blood pressure <100 mm Hg), No./total (%) | 19/561 (3.4) | 13/562 (2.3) |
| Nasogastric tube placement before intubation, No./total (%) | 90/567 (15.9) | 79/568 (13.9) |
| Medications in the preceding hour, No./total (%) | ||
| Midazolam | 40/570 (7.0) | 30/571 (5.3) |
| Gastric acid–reducing agent | 39/570 (6.8) | 35/571 (6.1) |
| Morphine | 38/570 (6.7) | 42/571 (7.4) |
| Ketamine | 12/570 (2.1) | 19/571 (3.3) |
Calculated as weight in kilograms divided by height in meters squared.
Bariatric surgery, neurosurgery, vascular surgery, or gynecological surgery.
Severe chronic gastric dysfunction was defined as severe gastroesophageal reflux, hiatal hernia, and dysautonomia-induced gastroparesis.
Characteristics of the Intubation Procedure
The characteristics of the intubation procedure are reported in Table 2. Preoxygenation by a bag-valve mask was used in 1024 patients (91%) (Table 2). Propofol, the most frequently used hypnotic, was given to 1118 of 1145 patients (98%) in the entire study population. Succinylcholine and rocuronium were respectively used in 408 of 570 patients (71.6%) and 156 of 570 patients (27.4%) in the neuromuscular blocker group, and 574 of 575 patients (99.8%) randomized to the remifentanil group received the allocated treatment.
Table 2. Characteristics of Intubation Procedures.
| Characteristics | Remifentanil group (n = 575) | Neuromuscular blocker group (n = 575) | Adjusted difference (95% CI)a |
|---|---|---|---|
| Preoxygenation method, No./total (%) | |||
| Bag-mask device | 510/562 (90.7) | 514/568 (90.5) | –0.9 (–4.6 to 2.9) |
| Bilevel positive airway pressure | 52/562 (9.3) | 54/568 (9.5) | |
| O2 expiratory fraction at the end of preoxygenation, mean (SD), % | 85.3 (8.8) | 85.8 (8.3) | –0.4 (–1.4 to 0.6) |
| Operator on first attempt, No./total (%) | |||
| Nurse specializing in anesthesiology (>2 y) | 446/528 (78.7) | 456/535 (80.1) | 0.5 (–1.5 to 2.5) |
| Anesthesiologist junior resident (postgraduate year 2-5) | 69/528 (12.2) | 67/535 (11.8) | |
| Senior anesthesiologist (MD) | 44/528 (7.8) | 41/535 (7.2) | |
| Other | 8/528 (1.4) | 5/535 (0.9) | |
| Patient position for intubation, No./total (%) | |||
| Neutral cervical spine | 351/566 (62.0) | 353/566 (62.4) | 0.1 (–4.4 to 4.7) |
| Sniffing position (Jackson)b | 149/566 (26.3) | 142/566 (25.1) | |
| Cervical spine extension without sniffing position | 60/566 (10.6) | 59/566 (10.4) | |
| Cervical spine flexion | 6/566 (1.1) | 12/566 (2.1) | |
| Laryngoscopy on first attempt, No./total (%) | |||
| Direct laryngoscopy | 479/567 (84.5) | 484/570 (84.9) | 0.0 (–2.6 to 2.7) |
| Video laryngoscopy | 88/567 (15.5) | 86/570 (15.1) | |
| Use of a stylet or bougie on first attempt, No./total (%) | 63/567 (11.1) | 90/570 (15.8) | –2.5 (–5.1 to 0.1) |
| Bag-mask ventilation during apneic period, No./total (%) | 6/565 (1.1) | 4/565 (0.7) | 0.2 (–0.5 to 0.8) |
| Rapid-onset neuromuscular blocker, No./total (%) | |||
| Succinylcholine | 408/570 (71.6) | ||
| Dose, mean (SD), mg/kg | 76 (17) | ||
| Rocuronium | 156/570 (27.4) | ||
| Dose, mean (SD), mg/kg | 74 (18) | ||
| Morphine derivative, No./total (%) | |||
| Remifentanil | 574/575 (99.8) | ||
| Dose, mean (SD), μg | 241 (93) | ||
| Other | 30/566 (5.3) | ||
| Hypnotic used for tracheal intubation, No./total (%)c | |||
| Propofol | 557/573 (97.2) | 561/572 (98.1) | –0.3 (–1.3 to 0.8) |
| Dose, mean (SD), mg/kg | 246 (75) | 236 (80) | |
| Ketamine | 94/573 (16.4) | 115/572 (20.1) | –2.2 (–6.0 to 1.7) |
| Thiopental | 5/573 (0.9) | 5/572 (0.9) | –0.01 (–0.2 to 0.2) |
The confidence interval was calculated by mixed-effects logistic regression adjusted for stratification factors and center as a random effect.
Extension of the head in relation to the cervical spine and flexion of the neck in relation to the chest to provide optimal exposure of the vocal cords.
Combined use of several hypnotics was possible.
Primary Outcome
In the as-randomized population, successful tracheal intubation on the first attempt without major complications occurred in 374 patients (66.1%) in the remifentanil group and 408 patients (71.6%) in the neuromuscular blocker group (adjusted difference for randomization strata and center, –6.1%; 2-sided 95% CI, –11.6% to –0.5%; P = .37 for noninferiority) (Figure 2). In the per-protocol analysis, the primary outcome occurred in 374 patients (66.2%) in the remifentanil group and 403 patients (71.3%) in the neuromuscular blocker group (adjusted difference, –5.7%; 2-sided 95% CI, –11.3% to –0.1%; P = .32 for noninferiority). In both the as-randomized and per-protocol populations, the lower limit of the 2-sided 95% CI (–11.6% and –11.3%, respectively) exceeded the noninferiority margin of –7.0%, thus not demonstrating noninferiority, and the upper limits were lower than 0 (–0.5% and –0.1%, respectively), thus demonstrating inferiority.
Figure 2. Primary Outcome of Successful Intubation on the First Attempt Without Major Complications in the Randomized and Per-Protocol Populations, and Preplanned Subgroup Analyses in the Randomized Population.
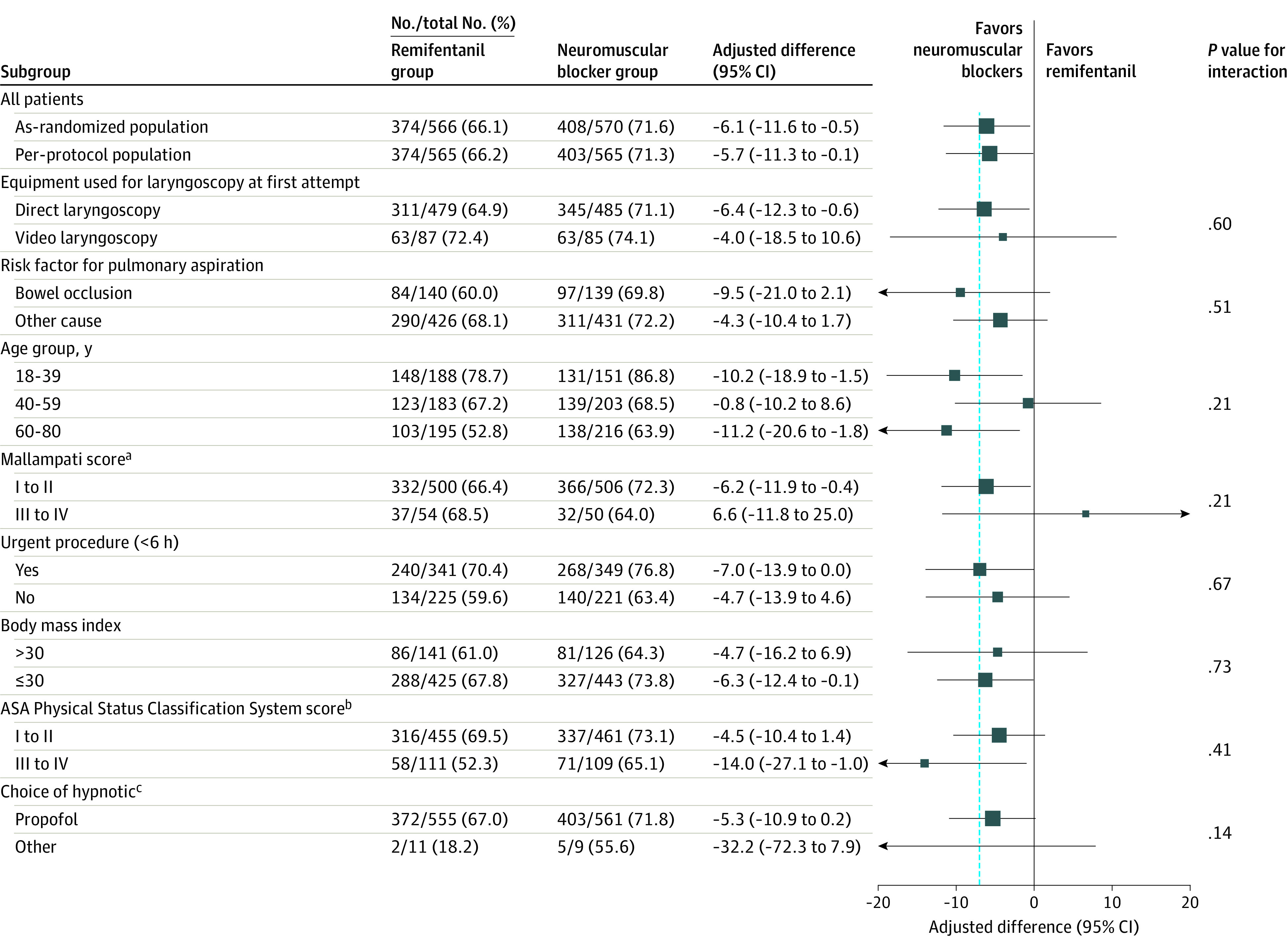
ASA indicates American Society of Anesthesiology. The vertical dashed line indicates the noninferiority margin of 7%. Body mass index is calculated as weight in kilograms divided by height in meters squared.
aScore of I to II, major part of the uvula is visible; score of III to IV, the base of the uvula or less is visible.
bScore of I to II, healthy or mild systemic disease without significant functional limitation; score of III to IV, significant functional limitation with potential constant threat to life.
cOther hypnotics: thiopental or etomidate.
In the randomization stratum of patients, the adjusted differences in the primary outcome rates were –4.0% (95% CI, −18.5% to 10.6%) among the 172 patients intubated with video laryngoscopy vs –6.4% (95% CI, −12.3% to –0.6%) among the 964 patients with direct laryngoscopy (P = .60 for interaction), and –9.5% (95% CI, −21.0% to 2.1%) in the 279 patients with digestive occlusion vs −4.3% (95% CI, −10.4% to 1.7%) in the 857 patients with other risk factors (P = .51 for interaction) (Figure 2). Considering the prespecified subgroup analyses, none of the characteristics significantly modified the effect of remifentanil on the primary outcome (see Figure 2 for the as-randomized population and eFigure 2 in Supplement 2 for the per-protocol population). Exploratory post hoc analyses found that the intervention effect varied significantly across centers (P < .001 for interaction) (eFigure 3 in Supplement 2). We found no secular trend during the inclusion period (eFigure 4 in Supplement 2). In the intervention group, the primary outcome was observed in 229 of 356 patients (64.3%) receiving low-dose remifentanil (<3.5 μg/kg) and in 142 of 206 patients (68.9%) receiving high-dose remifentanil (≥3.5 μg/kg) (adjusted difference, –4.6; 95% CI, –12.7% to 3.4%).
Secondary Outcomes
Secondary outcomes in the as-randomized population are reported in Table 3 and eTable 1 in Supplement 2 (and see eTable 2 in Supplement 2 for the results in the per-protocol population). The time from induction to successful intubation was 2.5 minutes (SD, 1.0 minute) in the remifentanil group and 2.5 minutes (SD, 1.2 minutes) with neuromuscular blockers (mean adjusted difference, 0.0 minutes; 95% CI, –0.1 to 0.2 minutes). The rates of postoperative pneumonia at day 7 were 0.5% in the remifentanil group and 0.4% in the neuromuscular blocker group (adjusted difference, 0.1%; 95% CI, –0.5% to 0.7%) (Table 2). The alternative methods used for the second and subsequent attempts are described in eTable 3 in Supplement 2.
Table 3. Outcomes in the As-Randomized Population.
| Outcomes | Remifentanil group (n = 575) | Neuromuscular blocker group (n = 575) | Adjusted difference (95% CI)a |
|---|---|---|---|
| Primary outcome | |||
| Successful intubation on the first attempt without major complications, No./total (%) | 374/575 (66.1) | 408/575 (71.6) | –6.1 (–11.6 to –0.5) |
| Components of the primary outcome, No./total (%) | |||
| Successful intubation on the first attempt | 502/567 (88.5) | 533/570 (93.5) | –4.9 (–8.2 to –1.6) |
| Operator-reported aspiration | 4/567 (0.7) | 2/570 (0.4) | 0.5 (–0.5 to 1.5) |
| Hypoxemia (oxygen saturation <95%) | 42/567 (7.4) | 38/570 (6.7) | 0.7 (–2.4 to 3.7) |
| Lowest saturation if severe, mean (SD), % | 87.0 (7.6) | 88.8 (5.7) | 0.7 (–2.2 to 3.6) |
| Episode of saturation <80% | 8/567 (1.4 | 3/570 (0.5) | 0.6 (–0.3 to 1.6) |
| Episode of major hemodynamic instability, prolonged arrhythmia >30 s, and/or cardiac arrestb | 118/567 (20.8) | 111/570 (19.5) | 1.1 (–3.7 to 5.9) |
| Episode of major hemodynamic instabilityb | 113/567 (19.1) | 110/570 (19.3) | –0.3 (–5.0 to 4.5) |
| Prolonged arrhythmia >30 s | 5/568 (0.9) | 1/570 (0.2) | 0.9 (–0.1 to 1.8) |
| Cardiac arrest | 0 | 0 | |
| Severe anaphylactic reaction (grade III or IV)c | 1/567 (0.2) | 0 | 0.0 (0.0 to 0.0) |
| Secondary outcomes | |||
| No esophageal intubation, No./total (%) | 558/567 (98.4) | 564/570 (98.9) | 0.0 (–0.02 to 0.02) |
| Time from induction to apnea, mean (SD), mind | 1.6 (0.8) | 1.5 (0.7) | 0.1 (0.0 to 0.2) |
| Time from induction to successful intubation, mean (SD), mind,e | 2.5 (1.0) | 2.5 (1.2) | 0.0 (–0.1 to 0.2) |
| Rescue therapy in cases of difficult intubation, No./total (%) | |||
| Neuromuscular blocker | 19/568 (3.3) | 8/570 (1.4) | 0.9 (–0.2 to 2.1) |
| Opioid | 6/568 (1.1) | 25/570 (4.4) | –3.6 (–5.6 to –1.7) |
| Hypnotic | 29/568 (5.1) | 20/570 (3.5) | 1.7 (–0.6 to 3.9) |
| Cormack-Lehane grade if direct laryngoscopy, No./total (%) | |||
| 1: Full glottis view | 388/478 (81.2) | 410/482 (85.1) | –4.0 (–8.8 to 0.8) |
| 2: Partial view of the glottis | 70/478 (14.6) | 53/482 (11.0) | |
| 3: Only epiglottis seen, no view of the glottis seen | 19/478 (4.0) | 15/482 (3.1) | |
| 4: Neither glottis nor epiglottis seen | 1/478 (0.2) | 4/482 (0.8) | |
| Percentage of glottic opening view if indirect laryngoscopy, mean (SD), %f | 92.6 (19.7) | 91.8 (18.7) | 0.7 (–4.9 to 6.4) |
| Sellick maneuver, No./total (%) | 19/567 (3.4) | 12/570 (2.1) | 1.5 (–0.6 to 3.5) |
| Intubation Difficulty Scale score, mean (SD)g | 3.0 (1.6) | 2.7 (1.3) | 0.4 (0.2 to 0.6) |
| Mechanical complications, No./total (%) | |||
| Dental injury | 0 | 0 | |
| Tracheal injuries | 1/567 (0.2) | 0 | 0.0 (0.0 to 0.0) |
| Cough requiring sedation increase | 63/567 (11.1) | 42/570 (7.4) | 3.6 (0.3 to 6.9) |
| Complications in the recovery room | |||
| Postextubation laryngeal dyspnea | 6/561 (1.2) | 4/561 (0.7) | 0.3 (–0.7 to 1.2) |
| Postoperative desaturation ≤92% | 58/566 (10.3) | 56/567 (9.9) | 0.6 (–2.7 to 3.9) |
| Postoperative nurse-reported aspiration | 2/562 (0.4) | 1/561 (0.2) | 0.3 (–0.5 to 1.0) |
| Laryngeal visual analog pain scale score, mean (SD)h | 8.6 (17.1) | 7.3 (15.5) | 1.3 (–0.6 to 3.3) |
| Admission to intensive care unit on day 7, No./total (%) | 35/569 (6.2) | 30/571 (5.3) | 0.4 (–2.2 to 3.0) |
| Postoperative pneumonia on day 7, No./total (%) | 3/569 (0.5) | 2/571 (0.4) | 0.1 (–0.5 to 0.7) |
| Acute respiratory distress syndrome on day 7, No./total (%) | 5/569 (0.9) | 4/571 (0.7) | 0.2 (–0.9 to 1.3) |
| In-hospital mortality, No./total (%) | 1/569 (0.2) | 1/571 (0.2) | 0.0 (–0.6 to 0.6) |
Confidence intervals were calculated by a mixed-effects logistic regression adjusted on stratification factors and centers as a random effect. No adjustment was made for multiplicity in the analysis of secondary outcomes. The confidence intervals around adjusted differences for secondary outcomes should not be used to infer definitive treatment effects.
Episode of major hemodynamic instability defined as mean arterial pressure ≤50 mm Hg or ≥110 mm Hg for more than 3 minutes.
Allergy severity grade I, cutaneous rash; grade II, moderate clinical signification requiring medical intervention; grade III, life-threatening symptoms: collapse, tachycardia or bradycardia, arrhythmias, bronchospasm; grade IV, cardiac and respiratory arrest.
Measured by an independent observer.
Time between administration of hypnotic (start of anesthetic induction) and tracheal intubation (defined as the sixth capnography curve).
Percentage of glottic opening ranges from 0% to 100% of glottis visualization.
The Intubation Difficulty Scale ranges from 0 (easy intubation) to infinity (impossible intubation). A score strictly superior to 0 but inferior to 5 indicates moderate difficulty; a score superior to 5 indicates major difficulty.
The laryngeal visual analog pain scale ranges from 0 (no pain) to 10 (unbearable pain).
Post Hoc Outcomes
The primary outcome components are described in Table 3. Successful intubation on the first attempt was observed in 502 patients (88.5%) in the remifentanil group vs 533 patients (93.5%) in the neuromuscular blocker group (adjusted difference, –4.9%; 95% CI, –8.2% to –1.6%).
Adverse Events
The rates of severe adverse events were 2.1% in the remifentanil group and 0.5% in the neuromuscular blocker group (adjusted difference, 1.8%; 95% CI, 0.4%-3.2%) (eTable 4 and the eAppendix [data safety report] in Supplement 2). Hemodynamic instability was recorded in 19 of 575 patients (3.3%) with remifentanil and 3 of 575 patients (0.5%) with neuromuscular blockers (adjusted difference, 2.8%; 95% CI, 1.2%-4.4%).
Discussion
In this multicenter randomized clinical trial that involved patients at risk of aspiration, remifentanil, compared with neuromuscular blocking agents, did not meet the criterion for noninferiority with regard to successful intubation on first attempt without major complications. Additionally, remifentanil was statistically inferior to neuromuscular blockers, although the wide confidence interval around the effect estimate remains compatible with noninferiority, thus limiting conclusions about the clinical relevance of the difference.
Morphine derivatives can be used in addition to neuromuscular blockers to facilitate tracheal intubation,33 and many advocate for their use as an alternative therapy to neuromuscular blockers.14,15,34 The results of this study do not support this approach, but this does not define the role of morphine derivatives as part of the intubation process.
The type and dose of morphine derivatives and neuromuscular blockers are critical to consider in the setting of rapid sequence intubation. Only alfentanil and remifentanil, which have rapid-onset effects, appear of potential interest in enabling rapid intubation success. Remifentanil was tested because of its shorter half-life, which can reduce apnea duration in the case of unplanned difficult intubation.35 Moreover, pilot studies have already set the optimal dose of remifentanil for intubation without a neuromuscular blocker. Notably, the rates of excellent intubation conditions increased with the dose of remifentanil up to a plateau at 4 μg/kg.14,15,36 Still, the risk of arterial hypotension also increases with the dose. The range of 3 to 4 μg/kg of remifentanil enabled clinicians to adapt to the individual benefit-risk balance and limits the risk of arterial hypotension.
Regarding the choice of neuromuscular blockers as the comparator, even if rocuronium was not demonstrated to be noninferior to succinylcholine for tracheal intubation success rate in patients undergoing out-of-hospital rapid sequence intubation,23 it was not excluded as a possible therapy in patients with a medical contraindication to succinylcholine, as proposed by French guidelines on neuromuscular blockade.24
The interpretation of the intervention effect on the primary composite outcome could be challenging, notably because of the severity range of its components. The difference between the study groups in the primary composite outcome was mainly driven by a higher rate of tracheal intubation failure on first attempt in the remifentanil group, an event that can be particularly damaging in patients at risk of aspiration.
Using a bougie25 or video laryngoscopy37 increases the likelihood of first-attempt success, but application rates of these techniques were low in this study. Even if the rates of successful intubation on the first attempt were high, these low rates potentially limit the extrapolation of the findings to other settings. There were no differences in their use rates between the study groups, suggesting that they did not bias the study results.
Limitations
This study has several limitations. First, this trial was open label. It was impossible to blind the procedure since succinylcholine, the most frequently used neuromuscular blocker during rapid sequence intubation, induces muscle fasciculations that clinicians easily observe. Second, the study aimed to include patients at risk of aspiration of gastric contents during the intubation procedure, yet there is no international consensus to define and quantify these risk factors to our knowledge. Patients with 1 or more risk factors were thus included, and some may have been considered at intermediate risk. However, the investigators deemed rapid sequence intubation necessary for all of these patients, and the subgroup analyses did not suggest heterogeneity of the intervention effect according to the baseline characteristics. Third, these results were obtained with doses of neuromuscular blockers appropriate for patients undergoing general anesthesia for surgical or interventional procedures and may not be generalizable to situations outside of operating rooms, such as obstetrical settings, intensive care units, or out-of-hospital or emergency department settings. Fourth, the low rate of stylet use, which increases the rate of success intubation on first attempt,25,30 could limit the generalization of the study results. However, all investigators were highly trained in tracheal intubation, as demonstrated by the 93.5% rate of first-attempt intubation success in the neuromuscular blocker group, which is higher than what is routinely described in areas where intubations are less frequently performed.20,38,39 Fifth, the learning curve of investigators not familiar with the use of remifentanil for rapid sequence intubation at the beginning of the study could have affected the estimation of the intervention effect. However, a secular trend in the rates of the primary outcome was not observed during the inclusion period.
Conclusions
Among adults at risk of aspiration during rapid sequence intubation in the operating room, remifentanil, compared with neuromuscular blockers, did not meet the criterion for noninferiority with regard to successful intubation on first attempt without major complications. Although remifentanil was statistically inferior to neuromuscular blockers, the wide confidence interval around the effect estimate remains compatible with noninferiority and limits conclusions about the clinical relevance of the difference.
Trial Protocol and Statistical Analyses Plan
eFigure 1. Study Intervention Timeline
eFigure 2. Preplanned Subgroup Analyses in the Per-Protocol Population
eFigure 3. Adjusted Difference of the Primary Outcome Across Participating Hospitals
eFigure 4. Temporal Trends of the Rates of Successful Intubation Without Major Complication
eTable 1. Secondary Outcomes in the As-Randomized Population
eTable 2. Secondary Outcomes in the Per-Protocol Population
eTable 3. Successful Technique After Failed First Attempt
eTable 4. Safety
eAppendix. Data Safety Report
Nonauthor Collaborators. Atlanrea Study Group and Société Française d’Anesthésie Réanimation (SFAR) Research Network
Data Sharing Statement
References
- 1.Michel P, Quenon JL, Djihoud A, Tricaud-Vialle S, de Sarasqueta AM. French national survey of inpatient adverse events prospectively assessed with ward staff. Qual Saf Health Care. 2007;16(5):369-377. doi: 10.1136/qshc.2005.016964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Langeron O, Bourgain JL, Francon D, et al. Difficult intubation and extubation in adult anaesthesia. Anaesth Crit Care Pain Med. 2018;37(6):639-651. doi: 10.1016/j.accpm.2018.03.013 [DOI] [PubMed] [Google Scholar]
- 3.Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022;136(1):31-81. doi: 10.1097/ALN.0000000000004002 [DOI] [PubMed] [Google Scholar]
- 4.Russotto V, Myatra SN, Laffey JG, et al. ; INTUBE Study Investigators . Intubation practices and adverse peri-intubation events in critically ill patients from 29 countries. JAMA. 2021;325(12):1164-1172. doi: 10.1001/jama.2021.1727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wong DJN, El-Boghdadly K, Owen R, et al. Emergency airway management in patients with COVID-19: a prospective international multicenter cohort study. Anesthesiology. 2021;135(2):292-303. doi: 10.1097/ALN.0000000000003791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Parida S, Varadharajan R, Bidkar PU, et al. A survey of a population of anaesthesiologists from South India regarding practices for rapid sequence intubation in patients with head injury. Indian J Anaesth. 2016;60(4):258-263. doi: 10.4103/0019-5049.179463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Botha JC, Lourens A, Stassen W. Rapid sequence intubation: a survey of current practice in the South African pre-hospital setting. Int J Emerg Med. 2021;14(1):45. doi: 10.1186/s12245-021-00368-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pillay L, Hardcastle T. Collective review of the status of rapid sequence intubation drugs of choice in trauma in low- and middle-income settings (prehospital, emergency department and operating room setting). World J Surg. 2017;41(5):1184-1192. doi: 10.1007/s00268-016-3712-x [DOI] [PubMed] [Google Scholar]
- 9.Petitpain N, Argoullon L, Masmoudi K, et al. ; French Network of Regional Pharmacovigilance Centres . Neuromuscular blocking agents induced anaphylaxis: results and trends of a French pharmacovigilance survey from 2000 to 2012. Allergy. 2018;73(11):2224-2233. doi: 10.1111/all.13456 [DOI] [PubMed] [Google Scholar]
- 10.Kaufman SE, Donnell RW, Aiken DC, Magee C. Prolonged neuromuscular paralysis following rapid-sequence intubation with succinylcholine. Ann Pharmacother. 2011;45(4):e21. doi: 10.1345/aph.1P753 [DOI] [PubMed] [Google Scholar]
- 11.Martyn JAJ, Richtsfeld M, Warner DO. Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms. Anesthesiology. 2006;104(1):158-169. doi: 10.1097/00000542-200601000-00022 [DOI] [PubMed] [Google Scholar]
- 12.Kirmeier E, Eriksson LI, Lewald H, et al. ; POPULAR Contributors . Post-anaesthesia Pulmonary Complications After Use of Muscle Relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7(2):129-140. doi: 10.1016/S2213-2600(18)30294-7 [DOI] [PubMed] [Google Scholar]
- 13.Lundstrøm LH, Duez CHV, Nørskov AK, et al. Effects of avoidance or use of neuromuscular blocking agents on outcomes in tracheal intubation: a Cochrane systematic review. Br J Anaesth. 2018;120(6):1381-1393. doi: 10.1016/j.bja.2017.11.106 [DOI] [PubMed] [Google Scholar]
- 14.Hanna SF, Ahmad F, Pappas ALS, et al. The effect of propofol/remifentanil rapid-induction technique without muscle relaxants on intraocular pressure. J Clin Anesth. 2010;22(6):437-442. doi: 10.1016/j.jclinane.2009.12.004 [DOI] [PubMed] [Google Scholar]
- 15.Erhan E, Ugur G, Alper I, Gunusen I, Ozyar B. Tracheal intubation without muscle relaxants: remifentanil or alfentanil in combination with propofol. Eur J Anaesthesiol. 2003;20(1):37-43. doi: 10.1097/00003643-200301000-00007 [DOI] [PubMed] [Google Scholar]
- 16.World Medical Association . World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- 17.Grillot N, Garot M, Lasocki S, et al. Assessment of remifentanil for rapid sequence induction and intubation in patients at risk of pulmonary aspiration of gastric contents compared to rapid-onset paralytic agents: study protocol for a non-inferiority simple blind randomized controlled trial (the REMICRUSH study). Trials. 2021;22(1):237. doi: 10.1186/s13063-021-05192-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ng A, Smith G. Gastroesophageal reflux and aspiration of gastric contents in anesthetic practice. Anesth Analg. 2001;93(2):494-513. doi: 10.1213/00000539-200108000-00050 [DOI] [PubMed] [Google Scholar]
- 19.Neelakanta G, Chikyarappa A. A review of patients with pulmonary aspiration of gastric contents during anesthesia reported to the Departmental Quality Assurance Committee. J Clin Anesth. 2006;18(2):102-107. doi: 10.1016/j.jclinane.2005.07.002 [DOI] [PubMed] [Google Scholar]
- 20.Lascarrou JB, Boisrame-Helms J, Bailly A, et al. ; Clinical Research in Intensive Care and Sepsis (CRICS) Group . Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among icu patients: a randomized clinical trial. JAMA. 2017;317(5):483-493. doi: 10.1001/jama.2016.20603 [DOI] [PubMed] [Google Scholar]
- 21.de Carvalho CC, da Silva DM, Lemos VM, et al. Videolaryngoscopy vs direct Macintosh laryngoscopy in tracheal intubation in adults: a ranking systematic review and network meta-analysis. Anaesthesia. 2022;77(3):326-338. doi: 10.1111/anae.15626 [DOI] [PubMed] [Google Scholar]
- 22.Landreau B, Odin I, Nathan N. Pulmonary aspiration: epidemiology and risk factors. Ann Fr Anesth Reanim. 2009;28(3):206-210. doi: 10.1016/j.annfar.2009.01.020 [DOI] [PubMed] [Google Scholar]
- 23.Guihard B, Chollet-Xémard C, Lakhnati P, et al. Effect of rocuronium vs succinylcholine on endotracheal intubation success rate among patients undergoing out-of-hospital rapid sequence intubation: a randomized clinical trial. JAMA. 2019;322(23):2303-2312. doi: 10.1001/jama.2019.18254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Plaud B, Baillard C, Bourgain JL, et al. Guidelines on muscle relaxants and reversal in anaesthesia. Anaesth Crit Care Pain Med. 2020;39(1):125-142. doi: 10.1016/j.accpm.2020.01.005 [DOI] [PubMed] [Google Scholar]
- 25.Driver BE, Prekker ME, Klein LR, et al. Effect of use of a bougie vs endotracheal tube and stylet on first-attempt intubation success among patients with difficult airways undergoing emergency intubation: a randomized clinical Trial. JAMA. 2018;319(21):2179-2189. doi: 10.1001/jama.2018.6496 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Birenbaum A, Hajage D, Roche S, et al. ; IRIS Investigators Group . Effect of cricoid pressure compared with a sham procedure in the rapid sequence induction of anesthesia: the IRIS randomized clinical trial. JAMA Surg. 2019;154(1):9-17. doi: 10.1001/jamasurg.2018.3577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Casey JD, Janz DR, Russell DW, et al. ; PreVent Investigators and the Pragmatic Critical Care Research Group . Bag-mask ventilation during tracheal intubation of critically ill adults. N Engl J Med. 2019;380(9):811-821. doi: 10.1056/NEJMoa1812405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Vourc’h M, Asfar P, Volteau C, et al. High-flow nasal cannula oxygen during endotracheal intubation in hypoxemic patients: a randomized controlled clinical trial. Intensive Care Med. 2015;41(9):1538-1548. doi: 10.1007/s00134-015-3796-z [DOI] [PubMed] [Google Scholar]
- 29.De Jong A, Molinari N, Terzi N, et al. ; AzuRéa Network for the Frida-Réa Study Group . Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187(8):832-839. doi: 10.1164/rccm.201210-1851OC [DOI] [PubMed] [Google Scholar]
- 30.Driver BE, Semler MW, Self WH, et al. ; BOUGIE Investigators and the Pragmatic Critical Care Research Group . Effect of use of a bougie vs endotracheal tube with stylet on successful intubation on the first attempt among critically ill patients undergoing tracheal intubation: a randomized clinical trial. JAMA. 2021;326(24):2488-2497. doi: 10.1001/jama.2021.22002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Piaggio G, Elbourne DR, Pocock SJ, Evans SJW, Altman DG; CONSORT Group . Reporting of noninferiority and equivalence randomized trials: extension of the CONSORT 2010 statement. JAMA. 2012;308(24):2594-2604. doi: 10.1001/jama.2012.87802 [DOI] [PubMed] [Google Scholar]
- 32.Mauri L Sr, D’Agostino RB Sr. Challenges in the design and interpretation of noninferiority trials. N Engl J Med. 2017;377(14):1357-1367. doi: 10.1056/NEJMra1510063 [DOI] [PubMed] [Google Scholar]
- 33.Chaumeron A, Castanie J, Fortier LP, et al. Efficacy and safety of remifentanil in a rapid sequence induction in elderly patients: a three-arm parallel, double blind, randomised controlled trial. Anaesth Crit Care Pain Med. 2020;39(2):215-220. doi: 10.1016/j.accpm.2019.09.010 [DOI] [PubMed] [Google Scholar]
- 34.Dolsan A, Bruneteau L, Roche C, et al. Comparison of intubating conditions after induction with propofol and remifentanil or sufentanil: randomized controlled REMIDENT trial for surgical tooth extraction. Anaesthesist. 2020;69(4):262-269. doi: 10.1007/s00101-020-00739-0 [DOI] [PubMed] [Google Scholar]
- 35.Egan TD, Minto CF, Hermann DJ, Barr J, Muir KT, Shafer SL. Remifentanil versus alfentanil: comparative pharmacokinetics and pharmacodynamics in healthy adult male volunteers. Anesthesiology. 1996;84(4):821-833. doi: 10.1097/00000542-199604000-00009 [DOI] [PubMed] [Google Scholar]
- 36.Alexander R, Booth J, Olufolabi AJ, El-Moalem HE, Glass PS. Comparison of remifentanil with alfentanil or suxamethonium following propofol anaesthesia for tracheal intubation. Anaesthesia. 1999;54(11):1032-1036. doi: 10.1046/j.1365-2044.1999.01070.x [DOI] [PubMed] [Google Scholar]
- 37.Garcia-Marcinkiewicz AG, Kovatsis PG, Hunyady AI, et al. ; PeDI Collaborative Investigators . First-attempt success rate of video laryngoscopy in small infants (VISI): a multicentre, randomised controlled trial. Lancet. 2020;396(10266):1905-1913. doi: 10.1016/S0140-6736(20)32532-0 [DOI] [PubMed] [Google Scholar]
- 38.Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010;36(2):248-255. doi: 10.1007/s00134-009-1717-8 [DOI] [PubMed] [Google Scholar]
- 39.Park L, Zeng I, Brainard A. Systematic review and meta-analysis of first-pass success rates in emergency department intubation: creating a benchmark for emergency airway care. Emerg Med Australas. 2017;29(1):40-47. doi: 10.1111/1742-6723.12704 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol and Statistical Analyses Plan
eFigure 1. Study Intervention Timeline
eFigure 2. Preplanned Subgroup Analyses in the Per-Protocol Population
eFigure 3. Adjusted Difference of the Primary Outcome Across Participating Hospitals
eFigure 4. Temporal Trends of the Rates of Successful Intubation Without Major Complication
eTable 1. Secondary Outcomes in the As-Randomized Population
eTable 2. Secondary Outcomes in the Per-Protocol Population
eTable 3. Successful Technique After Failed First Attempt
eTable 4. Safety
eAppendix. Data Safety Report
Nonauthor Collaborators. Atlanrea Study Group and Société Française d’Anesthésie Réanimation (SFAR) Research Network
Data Sharing Statement