

Key Points
Question
What is the cost-effectiveness of laparoscopic compared with open gastrectomy in a multicenter randomized clinical trial?
Findings
In this cost-effectiveness analysis alongside a randomized clinical trial of 227 patients with gastric cancer, although the laparoscopic gastrectomy itself was more expensive, after 1-year follow-up, differences in both total costs and effectiveness were limited between laparoscopic and open gastrectomy.
Meaning
Findings suggest that the comparable costs and cost-effectiveness support centers’ choosing, based on their own preference, whether to (de)implement laparoscopic gastrectomy as an alternative to open gastrectomy.
Abstract
Importance
Laparoscopic gastrectomy is rapidly being adopted worldwide as an alternative to open gastrectomy to treat gastric cancer. However, laparoscopic gastrectomy might be more expensive as a result of longer operating times and more expensive surgical materials. To date, the cost-effectiveness of both procedures has not been prospectively evaluated in a randomized clinical trial.
Objective
To evaluate the cost-effectiveness of laparoscopic compared with open gastrectomy.
Design, Setting, and Participants
In this multicenter randomized clinical trial of patients undergoing total or distal gastrectomy in 10 Dutch tertiary referral centers, cost-effectiveness data were collected alongside a multicenter randomized clinical trial on laparoscopic vs open gastrectomy for resectable gastric adenocarcinoma (cT1-4aN0-3bM0). A modified societal perspective and 1-year time horizon were used. Costs were calculated on the individual patient level by using hospital registry data and medical consumption and productivity loss questionnaires. The unit costs of laparoscopic and open gastrectomy were calculated bottom-up. Quality-adjusted life-years (QALYs) were calculated with the EuroQol 5-dimension questionnaire, in which a value of 0 indicates death and 1 indicates perfect health. Missing questionnaire data were imputed with multiple imputation. Bootstrapping was performed to estimate the uncertainty surrounding the cost-effectiveness. The study was conducted from March 17, 2015, to August 20, 2018. Data analyses were performed between September 1, 2020, and November 17, 2021.
Interventions
Laparoscopic vs open gastrectomy.
Main Outcomes and Measures
Evaluations in this cost-effectiveness analysis included total costs and QALYs.
Results
Between 2015 and 2018, 227 patients were included. Mean (SD) age was 67.5 (11.7) years, and 140 were male (61.7%). Unit costs for initial surgery were calculated to be €8124 (US $8087) for laparoscopic total gastrectomy, €7353 (US $7320) for laparoscopic distal gastrectomy, €6584 (US $6554) for open total gastrectomy, and €5893 (US $5866) for open distal gastrectomy. Mean total costs after 1-year follow-up were €26 084 (US $25 965) in the laparoscopic group and €25 332 (US $25 216) in the open group (difference, €752 [US $749; 3.0%]). Mean (SD) QALY contributions during 1 year were 0.665 (0.298) in the laparoscopic group and 0.686 (0.288) in the open group (difference, −0.021). Bootstrapping showed that these differences between treatment groups were relatively small compared with the uncertainty of the analysis.
Conclusions and Relevance
Although the laparoscopic gastrectomy itself was more expensive, after 1-year follow-up, results suggest that differences in both total costs and effectiveness were limited between laparoscopic and open gastrectomy. These results support centers’ choosing, based on their own preference, whether to (de)implement laparoscopic gastrectomy as an alternative to open gastrectomy.
This cost-effectiveness analysis of a randomized clinical trial investigates the cost-effectiveness of laparoscopic compared with open gastrectomy for gastric cancer.
Introduction
Gastric cancer is the sixth most prevalent cancer and the third most common cause of cancer-related death worldwide.1 Gastrectomy with lymphadenectomy is the cornerstone of multimodality curative treatment.2 Open gastrectomy has long been the criterion standard worldwide. However, application of laparoscopic gastrectomy for advanced gastric cancer is estimated to have increased in the Netherlands from 5% in 2012 to 80% in 2019 and worldwide from between 6% and 9% in 2014 to between 33% and 39% in 2020.3,4,5
The recent western Laparoscopic vs Open Gastrectomy for Gastric Cancer (LOGICA) trial on laparoscopic vs open gastrectomy for predominantly advanced gastric cancer reported similar results regarding the safety and oncologic efficacy for both procedures, in concordance with previous trials from the east.6,7,8,9,10 Costs of the laparoscopic operation itself (the unit costs) are expected to be higher compared with open gastrectomy owing to longer operating times and surgical materials or disposables.6,7,8,9,11 On initiation of the LOGICA trial, it was hypothesized that these higher unit costs would be compensated for by reduced hospital stays and reduced postoperative complications.3,11,12,13,14 However, these benefits were not demonstrated in the LOGICA trial and the majority of other randomized clinical trials on advanced gastric cancer.6,7,8,9 Hence, the clinical benefit of laparoscopic gastrectomy has not been proven so far, whereas its unit costs might be higher, which necessitates a dedicated randomized cost-effectiveness analysis between both procedures.
To date, the costs and cost-effectiveness of laparoscopic gastrectomy have been analyzed in 3 observational cohort studies.11,15,16 Furthermore, a model-based study was recently performed, using input from eastern randomized clinical trials and western retrospective studies on laparoscopic distal gastrectomy only.17 Hence, it remains difficult to draw conclusions on the costs and cost-effectiveness of laparoscopic total and distal gastrectomy, especially for the western population.10
Cost-effectiveness data were prospectively collected during the multicenter LOGICA randomized clinical trial on laparoscopic vs open gastrectomy.6,13 The cost-effectiveness results are reported here.
Methods
In this economic evaluation alongside a randomized clinical trial, the costs and quality-adjusted life-years (QALYs) of patients undergoing total or distal gastrectomy were compared as a prospective cost-effectiveness analysis between the open and laparoscopic approach as part of the multicenter randomized LOGICA trial.6 A modified societal perspective was used with a 1-year time horizon, starting on the day of surgery and corresponding to the LOGICA trial follow-up period.18 Hence, results are not discounted.
LOGICA Trial
This was a multicenter, open-label, superiority randomized clinical trial comparing laparoscopic with open gastrectomy in 10 Dutch hospitals. The trial protocol was approved by the institutional review board at each participating hospital (University Medical Center Utrecht, Utrecht; Catharina Hospital, Eindhoven; Zuyderland Medical Center, Heerlen and Sittard-Geleen; Erasmus University Medical Center, Rotterdam; Leiden University Medical Center, Leiden; ZGT Hospitals, Almelo; Gelre Hospitals, Apeldoorn; Meander Medical Center, Amersfoort; Amsterdam UMC, location AMC, Amsterdam; Amsterdam UMC, location VUmc, Amsterdam [all locations in the Netherlands]), registered at ClinicalTrials.gov (NCT02248519), and published at the start of the trial (trial protocol in Supplement 1).13 The study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline. In brief, after providing written informed consent, patients with surgically resectable (cT1-4aN0-3bM0) gastric cancer were randomly assigned to laparoscopic or open surgery (stratified by total or distal gastrectomy and hospital). Surgical procedures included total or distal gastrectomy with D2 lymphadenectomy. Multiple surgical and pathologic quality control measures were in place.6 Alongside this trial, the EuroQol 5-dimension questionnaire (EQ-5D), iMedical Consumption Questionnaire, and Short Form–Health and Labour questionnaire were sent to the patients at baseline (only EQ-5D), 6 weeks, 3 months, 6 months, 9 months, and 12 months.19,20,21
The clinical results were published recently.6 Between 2015 and 2018, 227 patients were included and randomly assigned to laparoscopic (n = 115) or open gastrectomy (n = 112) (Figure 1).22 In the laparoscopic group, the mean (SD) operating time was longer (216 [68.8] vs 182 [53.7] minutes). Neither group differed regarding the mean (SD) initial hospital stay (9.5 [10.8] vs 9.2 [8.2] days), the R0 resection rate (95% vs 95%), the median (IQR) lymph node yield (29 [21.1-37.0] vs 29 [22.0-39.0] nodes), postoperative complications (44% vs 42%), or 1-year overall survival.
Figure 1. Trial Flowchart.
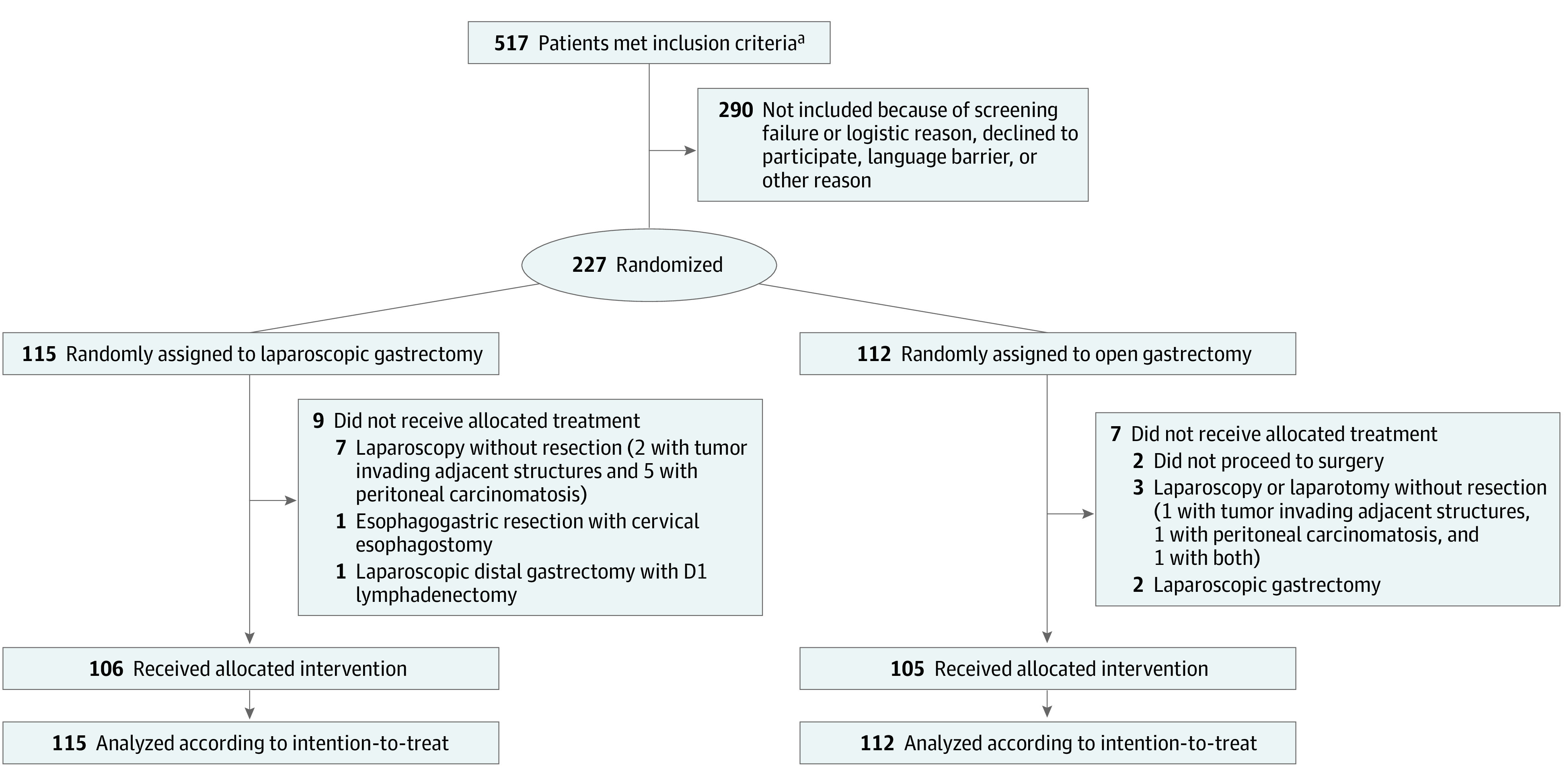
All 227 patients who underwent random assignment were included in the intention-to-treat analysis, 115 in the laparoscopic gastrectomy group and 112 in the open gastrectomy group. A total of 211 patients underwent their allocated treatment according to the protocol, 106 in the laparoscopic gastrectomy group and 105 in the open gastrectomy group.
aThe Dutch Upper GI Cancer Audit (DUCA) is a mandatory registration that contains information about every patient who underwent a gastrectomy for gastric cancer, including open-close procedures.22 DUCA data were used to calculate the total number of patients who met the study inclusion criteria during the inclusion period of each trial center.
Resource Use and Costs
Unit Costs of Surgery
No standardized unit costs were available for laparoscopic or open gastrectomy and were therefore calculated bottom-up for laparoscopic total and distal gastrectomy and open total and distal gastrectomy. Costs for laparoscopy or laparotomy without resection and gastroesophageal resection without anastomosis were also calculated bottom-up for the intention-to-treat analysis, but they were not reported as unit costs. The unit cost included costs of the operation room (including the room itself, personnel, and overhead), disposable materials, laparoscopic equipment, and epidural anesthesia. Furthermore, reoperation unit costs were calculated with a simple approach that included only the operation room costs. Operation room costs were estimated by multiplying the operating time of each patient by a minute price of the operation room, which was recently calculated in 1 of the participating centers of the LOGICA trial.23
Of the disposable materials, vessel sealers, staplers, barbed sutures, and wound-protecting retractor ports were categorized as expensive and the remaining materials as inexpensive (eTable 1 in Supplement 2). The amount of used expensive disposable materials was estimated per patient according to the materials used during normal practice at each of the 10 participating hospitals (as supplied by a trial surgeon from each hospital) for each type of operation (laparoscopic vs open gastrectomy, distal vs total gastrectomy, or other) and type of anastomosis (circular stapled, linear stapled, or hand sewn). Prices were obtained from the purchase department of 1 of the participating hospitals.
Other costs were calculated as a standard price per laparoscopic or open gastrectomy (not per patient). Inexpensive disposable materials costs were based on the materials used during normal practice at 1 of the participating hospitals. Laparoscopic equipment costs per gastrectomy were calculated with depreciation and service costs at 1 of the participating hospitals (eAppendix 1 and eTable 2 in Supplement 2).
Other Direct and Indirect Costs
All data on hospital procedures, registered for reimbursement purposes, were collected from each of the 10 participating hospital registries. In addition, data on extramural care, such as general practitioner consultations, home care, and family care, were available from the iMedical Consumption Questionnaire.24 Costs were calculated per patient by multiplying the number of procedures by the unit costs of every procedure. Unit costs were based on the Dutch guideline on costing research in health care and the Dutch Healthcare Authority.18,25 Furthermore, indirect costs to society associated with productivity losses were estimated with the Short Form–Health and Labour questionnaires by using the friction cost method.21
Quality-Adjusted Life-Years
Quality-adjusted life-years were calculated with the EQ-5D, in which a value of 0 indicates death and 1 indicates perfect health.19 The Dutch EQ-5D tariff was applied.26 The QALY contribution during 1 year was calculated for each patient by using an area under the curve approach with linear interpolation between time points. From the day a patient died, his or her EQ-5D was assumed to be zero. The QALY contributions were corrected for baseline EQ-5D scores and stratification factors by linear regression.
Cost-effectiveness and Sensitivity Analysis
Statistical analysis was performed with R (R Foundation for Statistical Computing), version 4.0.3. Data analyses were performed between September 1, 2020, and November 17, 2021. Missing values were imputed with multiple imputing with the R MICE package, using baseline characteristics, treatment outcomes, available questionnaires at other time points, and hospital costs. Aside from 2 patients with missing data on duration of operation (1 laparoscopic distal gastrectomy, 1 surgery without resection), data on costs from all 10 participating hospitals were complete. The EQ-5D questionnaire values were available for 79% of alive patients (138 of 174) to 83% of alive patients (187 of 225) at each time point. Therefore, 20 imputed data sets were created.
Cost-effectiveness was then evaluated via standard health economics statistics.27 The total costs and the QALY contribution of the laparoscopic and open gastrectomy groups were estimated and compared with each other. To estimate the uncertainty of the costs and QALY outcomes, bootstrapping was used with 100 iterations for each of the 20 imputed data sets. Finally, a cost-effectiveness plane was constructed in which each dot represented the costs and QALY of laparoscopic gastrectomy compared with open gastrectomy of 1 iteration.27 As prespecified, analyses were performed according to intention to treat, and subgroup analyses were performed for patients who underwent total or distal gastrectomy.13
Results
Unit Costs of Gastrectomy
A total of 227 patients were included in the analysis; 140 (61.7%) were male, 87 (38.3%) were female, and mean (SD) age was 67.5 (11.7) years. Approximately 92% of patients were White, as determined by investigator or clinician observation, without a uniform definition. Mean unit costs of the initial surgery were €8124 (US $8087) for laparoscopic total gastrectomy, €7353 (US $7320) for laparoscopic distal gastrectomy, €6584 (US $6554) for open total gastrectomy, and €5893 (US $5866) for open distal gastrectomy (Table 1). The majority of costs were for the operation room itself, personnel, and overhead (€5236 [US $5212], €4687 [US $4666], €4274 [US $4255], and €3938 [US $3920], respectively), followed by disposable material costs (€2814 [US $2801], €2592 [US $2580], €2200 [US $2190], and €1877 [US $1868], respectively), whereas epidural anesthesia costs and laparoscopic equipment costs contributed little to total costs (Table 1 and Table 2). Additional details on the laparoscopic equipment cost calculation, anastomotic technique, and expensive disposable material costs are provided in eAppendix 1, eAppendix 2, eTable 2, and eTable 3 in Supplement 2.
Table 1. Unit Costs of Laparoscopic and Open Gastrectomy as Calculated With a Bottom-up Approacha.
| Units | Cost per unit, €b | Total gastrectomy | Distal gastrectomy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Laparoscopic gastrectomy (n = 48) | Open gastrectomy (n = 43) | Laparoscopic gastrectomy (n = 58)c | Open gastrectomy (n = 64) | ||||||
| Mean No. of units | Mean costs, €b | Mean No. of units | Mean costs, €b | Mean No. of units | Mean costs, €b | Mean No. of units | Mean costs, €b | ||
| Minute price of operation (including operation room, personnel, and overhead) | 22.00 | 238 | 5236 | 194 | 4274 | 213 | 4687 | 179 | 3938 |
| Expensive disposable materials (vessel sealer, staplers, barbed sutures, and extraction ports) | Variable | 48 | 2432 | 43 | 2042 | 58 | 2210 | 64 | 1729 |
| Inexpensive laparoscopic disposable materials | 234.09 | 48 | 235 | 2 | 11 | 58 | 235 | 0 | 0 |
| Inexpensive other disposable materials | 147.46 | 48 | 147 | 43 | 147 | 58 | 147 | 64 | 147 |
| Use of laparoscope | 51.00 | 48 | 51 | 2 | 2 | 58 | 51 | 0 | 0 |
| Epidural anesthesia | 136.00 | 8 | 23 | 34 | 108 | 4 | 9 | 37 | 79 |
| Total surgery costs (without imputation) | NA | NA | 8124 | NA | 6584 | NA | 7340c | NA | 5893 |
Abbreviation: NA, not applicable.
Including costs for the operating room, personnel, laparoscope, staplers, vessel sealer, other disposable materials, and epidural anesthesia.
Current exchange rate: €1 = $0.99545.
Operation duration was missing in 1 patient who underwent laparoscopic distal gastrectomy. With imputation of this patient, total surgery costs in the laparoscopic distal gastrectomy group were €7353 (US $7320).
Table 2. Number of Procedures, Costs, and QALYs of Patients Undergoing Either Laparoscopic or Open Gastrectomy During 1-Year Follow-upa.
| Type of procedure | Laparoscopic gastrectomy (n = 115) | Open gastrectomy (n = 112) | ||||
|---|---|---|---|---|---|---|
| No. of individuals with procedure | Mean No. of procedures, d | Mean costs, €b | No. of individuals with procedure | Mean No. of procedures, d | Mean costs, €b | |
| Surgery | ||||||
| Initial surgery | 115 | 1.0 | 7380 | 112 | 1.0 | 5972 |
| Reoperation | 11 | 0.1 | 317 | 17 | 0.2 | 308 |
| Admissionsc | ||||||
| Hospital stay | 115 | 14.6 | 8518 | 112 | 13.3 | 7738 |
| ICU stay | 16 | 0.7 | 1775 | 18 | 1.2 | 2958 |
| Rehabilitation center or nursing home | 12 | 3.3 | 1118 | 14 | 7.3 | 2194 |
| Care | ||||||
| Home care or informal care | 75 | 73.8 | 1697 | 64 | 51.7 | 1188 |
| Diagnostics | ||||||
| Endoscopy | 45 | 0.7 | 128 | 30 | 0.6 | 124 |
| Imaging | 79 | 4.0 | 552 | 76 | 3.9 | 567 |
| Laboratory | 45 | 191.4 | 1736 | 30 | 182.2 | 1756 |
| Other | 49 | 2.0 | 135 | 45 | 1.6 | 91 |
| Consultations | ||||||
| Outpatient visits | 109 | 23.4 | 1737 | 110 | 24.2 | 1717 |
| General practitioner | 104 | 6.6 | 218 | 95 | 4.6 | 153 |
| Chemotherapy | 32 | NA | 455 | 21 | NA | 249 |
| Work absence | 34 | NA | 169 | 31 | NA | 195 |
| Other | 75 | 14.4 | 151 | 64 | 10.4 | 121 |
| Total | 115 | NA | 26 084 | 112 | NA | 25 332 |
| Mean QALYs | ||||||
| Baseline EQ-5D value | 0.819 (0.182) | 0.829 (0.161) | ||||
| During 1 yd | 0.665 (0.298) | 0.686 (0.288) | ||||
Abbreviations: EQ-5D, EuroQol 5-dimension questionnaire; ICU, intensive care unit; NA, not applicable; QALY, quality-adjusted life-year.
Number of procedures and costs of patients receiving either laparoscopic or open gastrectomy during 1-year follow-up, subdivided into surgery costs, admission costs, care costs, costs for diagnostics, consultations, work absence and other costs, and the baseline EQ-5D value and QALYs during 1 year.
Different procedures have different costs; hence, the mean number of procedures is not linearly related to the mean costs. Current exchange rate: €1 = $0.99545.
Mean number of procedures represents mean number of days.
Adjusted for baseline QALYs and stratification factors (total or distal gastrectomy and hospital).
Costs in the Laparoscopic and Open Groups
Costs of Surgery
Mean initial surgery costs were €7380 (US $7346) in the laparoscopic group and €5972 (US $5945) in the open group (Table 2). These costs were somewhat lower than the gastrectomy unit costs because some patients did not undergo surgery or underwent surgery without resection. Mean total reoperation costs were €317 (US $316) in the laparoscopic group and €308 (US $307) in the open group.
Admission Costs
Mean total costs of admissions (including initial and readmissions) were €11 411 (US $11 359) in the laparoscopic group and €12 890 (US $12 831) in the open group (Table 2), which included mean costs for hospital stay (€8518 [US $8479] vs €7738 [US $7703]), intensive care unit stay (€1775 [US $1767] vs €2958 [US $2945]), and rehabilitation center or nursing home stay (€1118 [US $1113] vs €2194 [US $2184]). The violin plots show that the distribution of admission and home care costs for individual patients was similar in both treatment groups (Figure 2). Further details on lengths of admission are given in Table 2.
Figure 2. Distributions of Per-Patient Costs.

A, Distribution of the per-patient total costs during 1-year follow-up for patients undergoing either laparoscopic or open gastrectomy. B, Distribution of the per-patient costs during 1-year follow-up for patients undergoing either laparoscopic or open gastrectomy for hospital admissions, intensive care unit (ICU), rehabilitation center or nursing home, and home care. Hospital admission and ICU costs were the observed costs because there were no missing values. Rehabilitation center, nursing home, and home care costs also included imputations of missing values. The transparent body of the violin plot displays the estimated density of the data: costs on the y-axis and the corresponding number of individuals on the x-axis (ie, the broader the shape, the more individuals). The circles indicate individual outliers. A standard box plot is displayed within the transparent body of the violin plot for total costs, hospital admissions, and home care. The box plot displays the median (horizontal line), IQRs (box), and the minimum and maximum excluding outliers (central black line). Current exchange rate: €1 = $0.99545.
Direct Costs
Mean costs for home care or informal care were €1697 (US $1689) in the laparoscopic group and €1188 (US $1183) in the open group. Mean total costs for diagnostics and consultations were €4505 (US $4485) in the laparoscopic group and €4409 (US $4389) in the open group (Table 2). Furthermore, mean costs were €455 (US $452) vs €249 (US $248) for chemotherapy and €151 (US $150) vs €121 (US $120) for other for the laparoscopic vs open group, respectively (Table 2).
Indirect and Total Costs
Mean total costs for work productivity losses (absenteeism and presenteeism) were €169 (US $168) in the laparoscopic group and €195 (US $194) in the open group (Table 2). Mean total costs up to 1 year postoperatively were €26 084 (US $25 965) in the laparoscopic group and €25 332 (US $25 217) in the open group (difference, €752 [US $749; 3.0%]) (Table 2). The violin plots show that the distribution of costs for individual patients was similar in both treatment groups (Figure 2).
Quality-Adjusted Life-Years (EQ-5D)
At baseline, mean (SD) EQ-5D values were 0.819 (0.182) in the laparoscopic group and 0.829 (0.161) in the open group. Mean (SD) QALY contributions during 1 year postoperatively, adjusted for baseline QALYs and stratification factors, were 0.665 (0.298) in the laparoscopic group and 0.686 (0.288) in the open group (difference, −0.021 [corresponding to 7.7 days in perfect health]).
Sensitivity Analysis
The 2000 bootstrap iterations are displayed in the cost-effectiveness plane, illustrating the uncertainty regarding the difference in costs and QALYs between treatment groups (Figure 3). Of all iterations, 13% represented lower costs and higher effectiveness for the laparoscopic group, 14% represented higher costs and higher effectiveness, 32% represented lower costs and lower effectiveness, and 41% represented higher costs and lower effectiveness.
Figure 3. Cost-effectiveness Plane.

Costs and quality-adjusted life-years (QALYs) gained of the laparoscopic group compared with the open group for 2000 bootstrap iterations displayed in a cost-effectiveness plane. Of all bootstrap iterations, 13% (260 of 2000) were in the bottom right quadrant (lower costs and higher effectiveness for the laparoscopic group), 14% (280) in the upper right quadrant (higher costs and higher effectiveness), 32% (640) in the bottom left quadrant (lower costs and lower effectiveness), and 41% (820) in the upper left quadrant (higher costs and lower effectiveness). Each dot indicates the difference in costs and QALYs between laparoscopic and open gastrectomy, of 1 bootstrap iteration. Blue, purple, and red colors indicate overlapping dots (bootstrap iterations) in increasing densities (with red indicating the highest density).
Total and Distal Subgroup Analyses
For total gastrectomy (n = 91), mean total costs and adjusted QALY contributions during 1 year were €32 297 (US $32 150) and 0.617 (SD, 0.288) in the laparoscopic group compared with €30 787 (US $30 647) and 0.626 (SD, 0.295) in the open group, respectively (difference in mean costs, €1503 [US $1496]; difference in mean QALYs, −0.009) (eTable 4 in Supplement 2). For distal gastrectomy (n = 123), these mean outcomes were €21 999 (US $21 899) and 0.750 (SD, 0.261) in the laparoscopic group compared with €21 884 (US $21 784) and 0.761 (SD, 0.243) in the open group, respectively (difference in mean costs, €115 [US $114]; difference in mean QALYs, −0.011) (eTable 5 in Supplement 2). For total and distal gastrectomy, the bootstrap iterations were clearly divided over all 4 quadrants of the cost-effectiveness plane (eFigure 1 and eFigure 2 in Supplement 2).
Discussion
To our knowledge, this was the first time that the cost-effectiveness of laparoscopic vs open gastrectomy for gastric cancer was prospectively evaluated in a multicenter randomized clinical trial. A detailed bottom-up calculation showed that the unit costs for the initial surgery were €8124 (US $8087) for laparoscopic total gastrectomy, €7353 (US $7320) for laparoscopic distal gastrectomy, €6584 (US $6554) for open total gastrectomy, and €5893 (US $5866) for open distal gastrectomy. The difference in mean total costs after 1-year follow-up was smaller, at 3.0% (€752; US $749): €26 084 (US $25 965) in the laparoscopic group and €25 332 (US $25 217) in the open group. Uncertainty of this difference was estimated in the bootstrap analysis, in which 45% of the iterations (900 of 2000) indicated lower total costs for the laparoscopic group and 55% (1100 of 2000) indicated higher total costs. Hence, the difference in total costs was limited between laparoscopic and open gastrectomy.
The mean QALY contributions up to 1 year postoperatively were 0.021 lower in the laparoscopic group compared with the open group, corresponding to 7.7 days in perfect health. In the bootstrap analysis, 27% of iterations (540 of 2000) indicated higher QALY contributions and 73% (1460 of 2000) indicated lower ones for the laparoscopic group, showing that either laparoscopic or open gastrectomy could be effective. This outcome aligns with the postoperative complications, 1-year survival, and disease-specific European Organisation for Research and Treatment of Cancer quality-of-life questionnaire outcomes, which did not differ between treatment groups in the current trial.6,28,29 Likewise, the recent western Surgical Techniques, Open Versus Minimally Invasive Gastrectomy After Chemotherapy (STOMACH) trial also showed no difference between laparoscopic and open gastrectomy regarding postoperative complications and 1-year survival.7
The total €752 (US $749; €26 084 [US $25 965] in the laparoscopic group and €25 332 [US $25 217] in the open group, or 3.0%) higher costs in the laparoscopic group were mainly due to higher unit costs of initial surgery owing to longer operating time and higher disposable material costs. The disposable material costs were higher in the laparoscopic group despite that expensive laparoscopy-compatible staplers were also used for two-thirds of patients in the open group. Surgeons using laparoscopy-compatible staplers in open surgery did so because they prefer the triple row of staples and longer arm with increased maneuverability. The higher costs of initial surgery were only partly compensated by cost savings in the laparoscopic group in admission costs. The mean total admission costs were lower in the laparoscopic group because of the shorter intensive care unit stays and rehabilitation and nursing home stays, even though the hospital stays were longer. The longer hospital stays in the laparoscopic group were due to longer readmissions that occurred after 30 days postoperatively, which could be due to chance. The initial postoperative admission length and number of readmissions within 30 days did not differ between treatment groups.6 The shorter mean intensive care unit stay was mainly a result of a shorter stay for patients with anastomotic leakage in the laparoscopic group (n = 10) compared with the open group (n = 11). We believe this was most likely due to chance because the anastomotic technique and leakage severity did not significantly differ between laparoscopic and open gastrectomy.6 Furthermore, rehabilitation center and nursing home costs were lower in the laparoscopic group (€1118 [US $1113] vs €2194 [US $2184]), mainly because of 1 patient who stayed in such care for the entire 1-year follow-up period after open distal gastrectomy. Last, home care and informal care costs were higher in the laparoscopic group (€1697 [US $1689] vs €1188 [US $1183]). All other costs were similar between treatment groups.
In the prespecified total and distal laparoscopic gastrectomy subgroups, mean QALY contributions were only 0.009 to 0.011 lower compared with that in the open subgroups (corresponding to 3-4 days in perfect health).13 However, mean costs were €1510 (US $1503) higher in the laparoscopic total subgroup and only €115 (US $114) higher in the laparoscopic distal subgroup compared with the open subgroups. This was mainly due to the aforementioned patient with high rehabilitation center and nursing home costs, who happened to be in the open distal gastrectomy subgroup. It is important that the bootstrapping also demonstrated in the total and distal subgroup that, compared with the uncertainty of the analysis, the differences between laparoscopic and open gastrectomy were relatively small.
Three nonrandomized studies with observed patient data on costs for laparoscopic vs open gastrectomy are available, performed in a Japanese nationwide database ($21 510 vs $21 024),15 a US academic medical centers database ($40 633 vs $41 326),16 and a single Dutch center (€8187 [US $8150] vs €7673 [US $7638]).11 Unfortunately, data on QALYs were not included, and details on costs were limited in the multicenter studies.15,16 Most important, because of the lack of randomization, these studies are likely subject to historical, hospital, and selection bias.
Recently, a model-based cost-effectiveness study reported laparoscopic distal gastrectomy to be cost-effective compared with open distal gastrectomy.17 Cost-effectiveness was contrived by combining costs from a retrospective Canadian data set, QALYs from 2 clinical studies performed between 2000 and 2005, and complication probabilities from eastern randomized clinical trials and western retrospective studies on laparoscopic vs open distal gastrectomy.17,30,31 Hence, it is likely more representative for early gastric cancer in the eastern population than for advanced cancer or the western population.10,17 Moreover, the increased cost-effectiveness of laparoscopic distal gastrectomy in western populations was based on a mean hospital stay reduction of 3.2 days from nonrandomized retrospective studies, whereas the current trial and the STOMACH trial were randomized and found no difference in hospital stay between laparoscopic and open gastrectomy.6,7
Strengths and Limitations
The strengths and limitations of the clinical results of the current trial have been discussed previously.6 Further strengths of the cost-effectiveness analysis include the unprecedented level of detail in which surgical costs were calculated bottom-up and the inclusion of extramural costs, such as nursing homes, home care, consultations with the general practitioner, and (work) productivity losses. An additional strength is the completeness of resource use derived from all 227 included patients in 10 hospital registries in which surgical follow-up was performed. Cost components that contributed most to total costs (surgery, hospital and intensive care unit stays, and diagnostics) were derived from these hospital registries and thus were not influenced by imputed missing questionnaires. However, because surgical treatment of gastric cancer is centralized in the Netherlands, the 10 participating hospitals are tertiary referral centers, and the main limitation of the current study is that costs were not available from the referring hospitals or other centers where the patients could have been treated.22 For instance, postoperative chemotherapy, follow-up by the medical oncologist, and diagnostics and treatment of nonsurgical complications are often performed at the referring hospital and thus not included in the current intramural costs. Accordingly, the current study is not able to provide a detailed comparison of postoperative chemotherapy costs. Therefore, the absolute costs after 1-year follow-up involving patients who underwent gastrectomy patients could be an underestimation of the actual costs. Nevertheless, because the current trial was randomized, the comparison of laparoscopic vs open gastrectomy is expected to remain unaffected.
Conclusions
In the current study, total costs were €752 (US $749; €26 084 [US $25 965] vs €25 332 [US $25 217], or 3.0%) higher in the laparoscopic group compared with the open group. Bootstrapping showed that this difference was relatively small compared with the uncertainty of the analysis. The comparable cost-effectiveness between treatment groups in the current study supports centers’ choosing, based on their own preference, whether to (de)implement laparoscopic gastrectomy as an alternative to open gastrectomy.
In conclusion, to our knowledge, this was the first cost-effectiveness analysis alongside a multicenter randomized clinical trial on laparoscopic vs open gastrectomy for gastric cancer. Although laparoscopic gastrectomy unit costs were higher, differences in both total costs and cost-effectiveness up to 1 year postoperatively were limited between laparoscopic and open gastrectomy.
Trial Protocol
eTable 1. Disposable Materials
eAppendix 1. Laparoscopic Equipment Costs Calculation
eTable 2. Laparoscopic Equipment Costs Per Laparoscopic Gastrectomy
eTable 3. Type of Anastomosis
eAppendix 2. Details on Stapler Usage
eTable 4. Subgroup Analyses on Patients With Total Resection
eFigure 1. Subgroup Analyses on Patients With Total Gastrectomy
eTable 5. Subgroup Analyses on Patients With Distal Resection
eFigure 2. Subgroup Analyses on Patients With Distal Gastrectomy
Nonauthor Collaborators
Data Sharing Statement
References
- 1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi: 10.3322/caac.21492 [DOI] [PubMed] [Google Scholar]
- 2.Al-Batran SE, Homann N, Pauligk C, et al. ; FLOT4-AIO Investigators . Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957. doi: 10.1016/S0140-6736(18)32557-1 [DOI] [PubMed] [Google Scholar]
- 3.Brenkman HJF, Ruurda JP, Verhoeven RHA, van Hillegersberg R. Safety and feasibility of minimally invasive gastrectomy during the early introduction in the Netherlands: short-term oncological outcomes comparable to open gastrectomy. Gastric Cancer. 2017;20(5):853-860. doi: 10.1007/s10120-017-0695-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gertsen EC, Brenkman HJF, Haverkamp L, Read M, Ruurda JP, van Hillegersberg R. Worldwide practice in gastric cancer surgery: a 6-year update. Dig Surg. 2021;38(4):266-274. doi: 10.1159/000515768 [DOI] [PubMed] [Google Scholar]
- 5.Dutch Upper GI Cancer Audit (DUCA) annual report 2019. Article in Dutch. DICA. Accessed August 24, 2021. https://dica.nl/jaarrapportage-2019/duca
- 6.van der Veen A, Brenkman HJF, Seesing MFJ, et al. ; LOGICA Study Group . Laparoscopic Versus Open Gastrectomy for Gastric Cancer (LOGICA): a multicenter randomized clinical trial. J Clin Oncol. 2021;39(9):978-989. doi: 10.1200/JCO.20.01540 [DOI] [PubMed] [Google Scholar]
- 7.van der Wielen N, Straatman J, Daams F, et al. Open versus minimally invasive total gastrectomy after neoadjuvant chemotherapy: results of a European randomized trial. Gastric Cancer. 2021;24(1):258-271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Beyer K, Baukloh AK, Kamphues C, et al. Laparoscopic versus open gastrectomy for locally advanced gastric cancer: a systematic review and meta-analysis of randomized controlled studies. World J Surg Oncol. 2019;17(1):68. doi: 10.1186/s12957-019-1600-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lee HJ, Hyung WJ, Yang HK, et al. ; Korean Laparo-endoscopic Gastrointestinal Surgery Study (KLASS) Group . Short-term Outcomes of a Multicenter Randomized Controlled Trial Comparing Laparoscopic Distal Gastrectomy With D2 Lymphadenectomy to Open Distal Gastrectomy for Locally Advanced Gastric Cancer (KLASS-02-RCT). Ann Surg. 2019;270(6):983-991. doi: 10.1097/SLA.0000000000003217 [DOI] [PubMed] [Google Scholar]
- 10.Russo A, Li P, Strong VE. Differences in the multimodal treatment of gastric cancer: east versus west. J Surg Oncol. 2017;115(5):603-614. doi: 10.1002/jso.24517 [DOI] [PubMed] [Google Scholar]
- 11.Tegels JJ, Silvius CE, Spauwen FE, Hulsewé KW, Hoofwijk AG, Stoot JH. Introduction of laparoscopic gastrectomy for gastric cancer in a western tertiary referral centre: a prospective cost analysis during the learning curve. World J Gastrointest Oncol. 2017;9(5):228-234. doi: 10.4251/wjgo.v9.i5.228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haverkamp L, Weijs TJ, van der Sluis PC, van der Tweel I, Ruurda JP, van Hillegersberg R. Laparoscopic total gastrectomy versus open total gastrectomy for cancer: a systematic review and meta-analysis. Surg Endosc. 2013;27(5):1509-1520. doi: 10.1007/s00464-012-2661-1 [DOI] [PubMed] [Google Scholar]
- 13.Haverkamp L, Brenkman HJF, Seesing MFJ, et al. ; LOGICA Study Group . Laparoscopic versus open gastrectomy for gastric cancer: a multicenter prospectively randomized controlled trial (LOGICA-trial). BMC Cancer. 2015;15(1):556. doi: 10.1186/s12885-015-1551-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brenkman HJF, Gisbertz SS, Slaman AE, et al. ; Dutch Upper Gastrointestinal Cancer Audit (DUCA) group . Postoperative outcomes of minimally invasive gastrectomy versus open gastrectomy during the early introduction of minimally invasive gastrectomy in the Netherlands: a population-based cohort study. Ann Surg. 2017;266(5):831-838. doi: 10.1097/SLA.0000000000002391 [DOI] [PubMed] [Google Scholar]
- 15.Yasunaga H, Horiguchi H, Kuwabara K, et al. Outcomes after laparoscopic or open distal gastrectomy for early-stage gastric cancer: a propensity-matched analysis. Ann Surg. 2013;257(4):640-646. doi: 10.1097/SLA.0b013e31826fd541 [DOI] [PubMed] [Google Scholar]
- 16.Glenn JA, Turaga KK, Gamblin TC, Hohmann SF, Johnston FM. Minimally invasive gastrectomy for cancer: current utilization in US academic medical centers. Surg Endosc. 2015;29(12):3768-3775. doi: 10.1007/s00464-015-4152-7 [DOI] [PubMed] [Google Scholar]
- 17.Gosselin-Tardif A, Abou-Khalil M, Mata J, et al. Laparoscopic versus open subtotal gastrectomy for gastric adenocarcinoma: cost-effectiveness analysis. BJS Open. 2020;4(5):830-839. doi: 10.1002/bjs5.50327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.National Health Care Institute (Zorginstituut Nederland) . Guideline for conducting economic evaluations in healthcare. Zorginstituut Nederland. Published June 16, 2016. Accessed August 18, 2021. https://english.zorginstituutnederland.nl/publications/reports/2016/06/16/guideline-for-economic-evaluations-in-healthcare
- 19.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. doi: 10.1007/s11136-011-9903-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kobayashi N, Kohno T, Haruta S, et al. Pulmonary metastasectomy secondary to esophageal carcinoma: long-term survival and prognostic factors. Ann Surg Oncol. 2014;21(suppl 3):S365-S369. doi: 10.1245/s10434-014-3677-7 [DOI] [PubMed] [Google Scholar]
- 21.Hakkaart-van Roijen L, Essink-Bot ML. The Health and Labour Questionnaire manual. Accessed August 18, 2021. https://www.researchgate.net/publication/254804594_The_Health_and_Labour_Questionnaire_Manual [Google Scholar]
- 22.Busweiler LAD, Wijnhoven BPL, van Berge Henegouwen MI, et al. ; Dutch Upper Gastrointestinal Cancer Audit (DUCA) Group . Early outcomes from the Dutch Upper Gastrointestinal Cancer Audit. Br J Surg. 2016;103(13):1855-1863. doi: 10.1002/bjs.10303 [DOI] [PubMed] [Google Scholar]
- 23.Bolkenstein HE, de Wit GA, Consten ECJ, Van de Wall BJM, Broeders IAMJ, Draaisma WA. Cost-effectiveness analysis of a multicentre randomized clinical trial comparing surgery with conservative management for recurrent and ongoing diverticulitis (DIRECT trial). Br J Surg. 2019;106(4):448-457. doi: 10.1002/bjs.11024 [DOI] [PubMed] [Google Scholar]
- 24.iMTA Medical Consumption Questionnaire. Institute for Medical Technology Assessment. Accessed February 1, 2020. https://www.imta.nl/questionnaires/imcq/
- 25.Performance and tariffs specialist medical care. Article in Dutch. Nederlandse Zorgauthoriteit. Accessed December 1, 2019. https://www.nza.nl/zorgsectoren/medisch-specialistische-zorg
- 26.Versteegh MM, Vermeulen KM, Evers SMAA, de Wit GA, Prenger R, Stolk EA. Dutch tariff for the five-level version of EQ-5D. Value Health. 2016;19(4):343-352. doi: 10.1016/j.jval.2016.01.003 [DOI] [PubMed] [Google Scholar]
- 27.Mutubuki EN, El Alili M, Bosmans JE, et al. The statistical approach in trial-based economic evaluations matters: get your statistics together! BMC Health Serv Res. 2021;21(1):475. doi: 10.1186/s12913-021-06513-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. doi: 10.1093/jnci/85.5.365 [DOI] [PubMed] [Google Scholar]
- 29.Blazeby JM, Conroy T, Bottomley A, et al. ; European Organisation for Research and Treatment of Cancer Gastrointestinal and Quality of Life Groups . Clinical and psychometric validation of a questionnaire module, the EORTC QLQ-STO 22, to assess quality of life in patients with gastric cancer. Eur J Cancer. 2004;40(15):2260-2268. doi: 10.1016/j.ejca.2004.05.023 [DOI] [PubMed] [Google Scholar]
- 30.Kim YW, Baik YH, Yun YH, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008;248(5):721-727. doi: 10.1097/SLA.0b013e318185e62e [DOI] [PubMed] [Google Scholar]
- 31.Avery KNL, Metcalfe C, Nicklin J, et al. Satisfaction with care: an independent outcome measure in surgical oncology. Ann Surg Oncol. 2006;13(6):817-822. doi: 10.1245/ASO.2006.08.019 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eTable 1. Disposable Materials
eAppendix 1. Laparoscopic Equipment Costs Calculation
eTable 2. Laparoscopic Equipment Costs Per Laparoscopic Gastrectomy
eTable 3. Type of Anastomosis
eAppendix 2. Details on Stapler Usage
eTable 4. Subgroup Analyses on Patients With Total Resection
eFigure 1. Subgroup Analyses on Patients With Total Gastrectomy
eTable 5. Subgroup Analyses on Patients With Distal Resection
eFigure 2. Subgroup Analyses on Patients With Distal Gastrectomy
Nonauthor Collaborators
Data Sharing Statement