

This cohort study analyzes suicide rates among reproductive-aged women from 1974 to 2016 to determine their association with state-level legislative policies surrounding abortion and restricted access to reproductive care.
Key Points
Question
Are state-level legislative policies surrounding abortion or restricted access to reproductive care related to women’s suicide rates in the United States?
Findings
In this longitudinal ecologic study with a difference-in-differences analysis, the enforcement of laws restricting access to abortion and reproductive care from 1974 to 2016 was associated with suicide rates among reproductive-aged women but not women of postreproductive age.
Meaning
Restrictions to reproductive care represent a macro-level risk factor for suicide among reproductive-aged women, which may have implications for suicide prevention strategies in this population, particularly as the issue remains at the center of divisive debate in the United States.
Abstract
Importance
Many states in the United States enforce restrictions to reproductive care, with access to abortion remaining a highly divisive issue. Denial of abortion is linked with heightened stress and anxiety among reproductive-aged women. However, no studies have tested whether access to reproductive care is linked to suicide.
Objective
To evaluate whether state-level restrictions in access to reproductive care in the United States were associated with suicide rates among reproductive-aged women from 1974 to 2016.
Design, Setting, and Participants
A longitudinal ecologic study with a difference-in-differences analysis assessed whether annual changes in the enforcement of state-level restrictions to reproductive care were related to annual state-level suicide rates vs rates of death due to motor vehicle crashes. Duration of follow-up varied between different states (range, 4-40 years), contingent on the first year that restrictions were implemented. Models controlled for year and state fixed effects and other relevant demographic and economic factors. Analyses were conducted between December 2021 and January 2022.
Exposures
Targeted Regulation of Abortion Providers (TRAP) laws index measuring state-year–level restrictions to reproductive care.
Main Outcomes and Measures
Annual state-level suicide rates and motor vehicle crash death rates among reproductive-aged women (ages 20-34 years; target group) vs women of postreproductive age (ages 45-64 years; control group).
Results
Twenty-one US states enforced at least 1 TRAP law between 1974 and 2016. Annual rates of death by suicide ranged from 1.4 to 25.6 per 100 000 women of reproductive age to 2.7 to 33.2 per 100 000 women of postreproductive age during the study period (1974-2016). Annual motor vehicle crash death rates among women of reproductive age ranged from 2.4 to 42.9 per 100 000. Enforcement of TRAP laws was associated with higher suicide rates among reproductive-aged women (β = 0.17; 95% CI, 0.03 to 0.32; P = .02) but not women of postreproductive age (β = 0.06; 95% CI, –0.11 to 0.24; P = .47) nor to deaths due to motor vehicle crashes (β = 0.03, 95% CI, –0.04 to 0.11; P = .36). Among reproductive-aged women, the weighted average annual-state level suicide death rate when no TRAP laws were enforced was 5.5 per 100 000. Enforcement of a TRAP law was associated with a 5.81% higher annual rate of suicide than in pre-enforcement years. Findings remained significant when using alternative, broader indices of reproductive care access and different age categorizations.
Conclusions and Relevance
In this study with a difference-in-differences analysis of US women, restrictions on access to reproductive care from 1974 to 2016 were associated with suicide rates among reproductive-aged women. Given the limitations of the ecologic design of this study, further research is needed to assess whether current factors affecting access to reproductive care services are related to suicide risk among women of reproductive age and to inform suicide prevention strategies.
Introduction
Suicide is one of the 3 leading causes of death in young women.1 Theoretical models specify that biological and psychological factors predispose a person to suicidal behavior, which is precipitated further by environmental stressors.2 Environmental stressors operate proximally to an individual, including as interpersonal or health-related difficulties, and distally at the macro level, including through economic factors or media representations of suicide.3 Stressors that affect suicide risk vary across development, with different stressors being more prominent based on age,4 or among specific subpopulations.5 Identifying macro-level stressors associated with suicide risk can provide key insights for policy makers aiming to improve population health.6
Abortion and access to reproductive care represent divisive issues in the United States, with staggering health consequences for women. Since 1970, states have enacted more than 1300 abortion restrictions, including efforts to prohibit abortion after 6 weeks of gestational age.7 The dynamic nature of this legislation and its extensive media coverage have implications for the mental health of reproductive-aged women.8 Prior studies have tested whether receiving an abortion is related to negative mental health outcomes, including depression9 and suicide attempts,10 but provide disputed evidence of such associations. In contrast, in the Turnaway Study involving 1000 women, higher stress and anxiety were documented among women “turned away” and denied an abortion because they were outside the gestational limit of clinics, when compared with women who received an abortion because they were under the gestational limit.11 To date, however, no studies have tested whether access to reproductive care is associated with suicide rates among reproductive-aged women.
To address this knowledge gap, we investigated whether different measures of state-level legislation pertaining to access to reproductive care, including abortion, were associated with suicide rates of women from 1974 to 2016. We used state-year–level data in a difference-in-differences analytic approach to test whether annual changes in access to reproductive care were related to changes in suicide rates among women, while accounting for relevant macro-level factors. We hypothesized that restricted access to reproductive care would be specifically associated with higher suicide rates among reproductive-aged women but not with another leading cause of death among reproductive-aged women (motor vehicle crashes), nor with suicide rates among women of postreproductive age.
Methods
Study Design
We examined deidentified, state-level data made publicly available by the US Centers for Disease Control and Prevention (CDC). The study was exempt from full review by the institutional review board of the University of Pennsylvania (authorized by 45 CFR 46.104, category 4), and no informed consent was required. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies.
Exposures
Our exposure measures included indices of access to reproductive care. To ensure the robustness of our results, we used 3 different indices.
Targeted Regulation of Abortion Providers (TRAP) Laws Index
The TRAP laws index maps 3 state-level TRAP laws as recorded by Austin and Harper12: ambulatory surgical center laws, admitting privileges, and transfer agreements (eTables 1 and 2 in the Supplement contain a detailed description of each law and its enforcement across US states during the study period). The index increases by 1 if a TRAP law is enforced and decreases by 1 if blocked. Thus, scores for any given year for a specific state range from 0 (ie, no laws in place) to 3 (ie, all 3 laws enforced). The index begins in 1974 (the first full year in which abortions were legal in the United States) and ends in 2016 (last full year for which complete TRAP laws data are available).12
Weighted and Unweighted Access Indices
These state-level indices measure restrictions and burdensome requirements to reproductive care services between 2006 and 2017.13 Both indices are derived from 17 categories defined by the National Abortion and Reproductive Rights Action League (NARAL) and reported in their annual “Who Decides?” reports,14 with higher scores representing lower access (the eMethods in the Supplement contain a detailed description). To create the weighted access index, consistent with the 2015 NARAL report, we weighted the categories according to their effectiveness in restricting or expanding access to reproductive care. The unweighted access index was obtained by summing the number of the restricting categories and subtracting the number of expanding categories at the state-year level. We focused on data from 2006 to 2017 because ambiguity in the language of laws prior to 2006 made identification of the 17 chosen categories inconclusive.
Outcome Measures
Our outcome measure was suicide rate from the CDC’s Wide-ranging Online Data for Epidemiologic Research (WONDER) database, which includes state-year–level data on causes of death.15 Overall, trends in suicide rates between 1974 and 2017 were similar among reproductive-aged women and women of postreproductive age (eFigure 1 in the Supplement). We refer to women based on the gender categorization (male/female) defined within the WONDER database.
To test our central hypothesis, we focused on how restrictions on reproductive care were related to suicide among women aged 20 to 34 years (ie, reproductive age, the target group) compared with women aged 45 to 64 years (ie, postreproductive age, the control group). As tests of robustness, we compared findings when the target group was aged 20 to 44 years and control group aged 45 to 74 years, as well as comparing suicide rates in all available age bins provided by the CDC (20-24, 25-34, 35-44, 45-54, 55-64, and 65-74 years). To generate suicide rates in each group, we added the annual number of deaths across the relevant age bins in a given state and divided it by the size of the corresponding population. Note that analyses only included available data from the CDC WONDER for deaths by suicide in our target age range in a given year for a given state, which included 1120 data points for ages 20 to 24 years and 1685 for ages 25 to 34 years (combined observations, 1115 for ages 20-34 years) (eTable 3 in the Supplement).
Finally, to test specificity of the findings to suicide, we also tested associations between restricted access to reproductive care and death rates of women due to another leading cause of death, motor vehicle crashes (eFigure 1 in the Supplement shows trends in motor vehicle crash death rates during the study period).
Other Explanatory Variables
Economic Factors
To account for macro-level economic characteristics that might affect suicide risk,16 we included (1) the annual, state-level, gross domestic product (GDP) growth reported by the Bureau of Economic Analysis and (2) the annual, state-level unemployment rates (available only from 1976) reported by the Bureau of Labor Statistics. Note that state-level data on unemployment rates were not available before 1976. Thus, as a robustness test, we also ran analyses without the unemployment rate covariate, including data from 1974 onwards.
Race and Ethnicity
The data we analyzed included women from all racial and ethnic groups. However, to account for racial and ethnic disparities in access to reproductive health, we included the state-year proportion of Black or African American residents as estimated by the US Census Bureau, Population Division, because this group has been historically most affected by restrictions, which could have confounded the results.17
Political Affiliation
To account for the confounding influence of political affiliation on TRAP law enactment, we controlled for the annual fraction of Republican senators representing the state at the US Senate, as reported on the Charles Stewart Congressional Data Page.18
Statistical Analyses
Analyses were performed using Stata version 16.1 and independently tested using R version 4.1.0. Data and code are publicly available.19 Analyses were conducted between December 2021 and January 2022. All dependent and independent variables were normalized by de-meaning and dividing them by their respective standard deviations to allow an intuitive interpretation of the coefficients.
First, we used a 2-way fixed effects dynamic difference-in-differences analysis using data from all 50 states.13,20 This method examined how access to reproductive care is linked to annual suicide rates after accounting for potential confounders and nonrelated, state-year–level changes in the rate. We examined the following weighted difference-in-differences fixed-effects regression:
| SuicideRates,t = αs + γt + βTRAPs,t + δZs,t + εs,t |
where subscript s indexes states, t indexes years, and β denotes the coefficient of interest. SuicideRates,t is the relevant, annual, state-level suicide rate, TRAPs,t is the state-year–level index, and Zs,t is a vector of covariates (GDP growth, unemployment rate, percentage of Black or African American individuals, and fraction of Republican senators). We also included state (αs) and year (γt) fixed effects (ie, 2-way fixed effects). The state fixed effects in the model allowed us to isolate rate changes after absorbing any fundamental average differences in the suicide rates between states. Similarly, the time fixed effects absorbed any unrelated time trends that could have biased our results. Standard errors were clustered at the state and year level, and the regression models were weighted by the annual number of residents in each state. To estimate the magnitude of the association (effect size), we divided the nonnormalized coefficient (β) of interest by the mean of the nontreated observations of the dependent variable. Namely, we calculated the change in suicide rate with each additional TRAP law enforced after absorbing potential confounders, including aggregate time trends and state-level, time-invariant heterogeneity that could potentially drive the results. Notably, the nonnormalized and normalized coefficients are derived using identical methods with the exception that the nonnormalized regressions use variables from the raw data and the normalized regressions use z-scored versions of the variables. We also examined the robustness of the model by replacing the TRAP laws index with both the weighted and unweighted access indices.
Second, we tested the parallel trends assumption (ie, absence of a pre-trend, which is critical to ensure the internal validity of differences-in-differences models20) focusing on the 21 states that enforced at least 1 TRAP law across the study period (TRAP law states). Thus, we split the original difference-in-differences analysis by years and performed a visual confirmation of parallel trends of the target and control groups’ coefficients in the pretreatment (ie, pre-TRAP laws) years. The absence of pre-trends suggests no other state-level trend accounts for the results. In contrast, a positive regression coefficient in the target group (ie, increasing suicide rate) in the 2 years before TRAP law enforcement would suggest the existence of a pre-trend, thus undermining the validity of the results. Similarly, a positive regression coefficient in the control group 2 years after the enforcement would suggest a broader trend among women, undermining the validity of the results. We examined the following weighted 2-way fixed-effects difference-in-differences regression:
| SuicideRates,t = αs + γt + β−LRTRAPs,n ≤ −3 + ∑2j = −2; j ≠ −1 βjTRAPs,n + j + βLRTRAPs,n ≥ 3 + δZs,t + εs,t |
where n indexes the year at which the first TRAP law was enforced in a state s, j indexes the year relative to the enforcement year, −LR indexes the period of time that ends 3 years before the enforcement, and LR indexes the long-run effect 3 years after the enforcement onward. TRAPs,n+j is a binary variable (ie, change from 0 to 1) only in year j after the enforcement, TRAPs,n≤3 is a binary variable (ie, change from 0 to 1) 3 years before the enforcement, and TRAPs,n≥3 is a binary variable (ie, change from 0 to 1) 3 years or more after the enforcement.
Sensitivity Analysis
To address the possibility that our age-range choice in the main analyses (ie, 20-34 years and 45-64 years for the target and control groups, respectively) influenced the results, we reran all models using wider age ranges for the target (20-44 years) and control groups (45-74 years), as well as in all the available age bins provided by the CDC (20-24, 25-34, 35-44, 45-54, 55-64, and 65-74 years).
Results
Twenty-one US states enforced at least 1 TRAP law from 1974 to 2016 (Figure 1; eTable 2 and eFigure 2 in the Supplement). All US states introduced legislation that promoted or restricted access to reproductive care, generating variability in our weighted and unweighted access indices (eFigures 3 and 4 in the Supplement show the annual index level for all US states across the study period). Change in access over time based on the weighted and unweighted access scores is visualized in Figure 2 for 4 states chosen as examples.
Figure 1. Targeted Regulation of Abortion Providers (TRAP) Laws Enforced in the United States From 1974 to 2016.

Figure 2. Access Index for 4 Representative US States From 2006 to 2017.
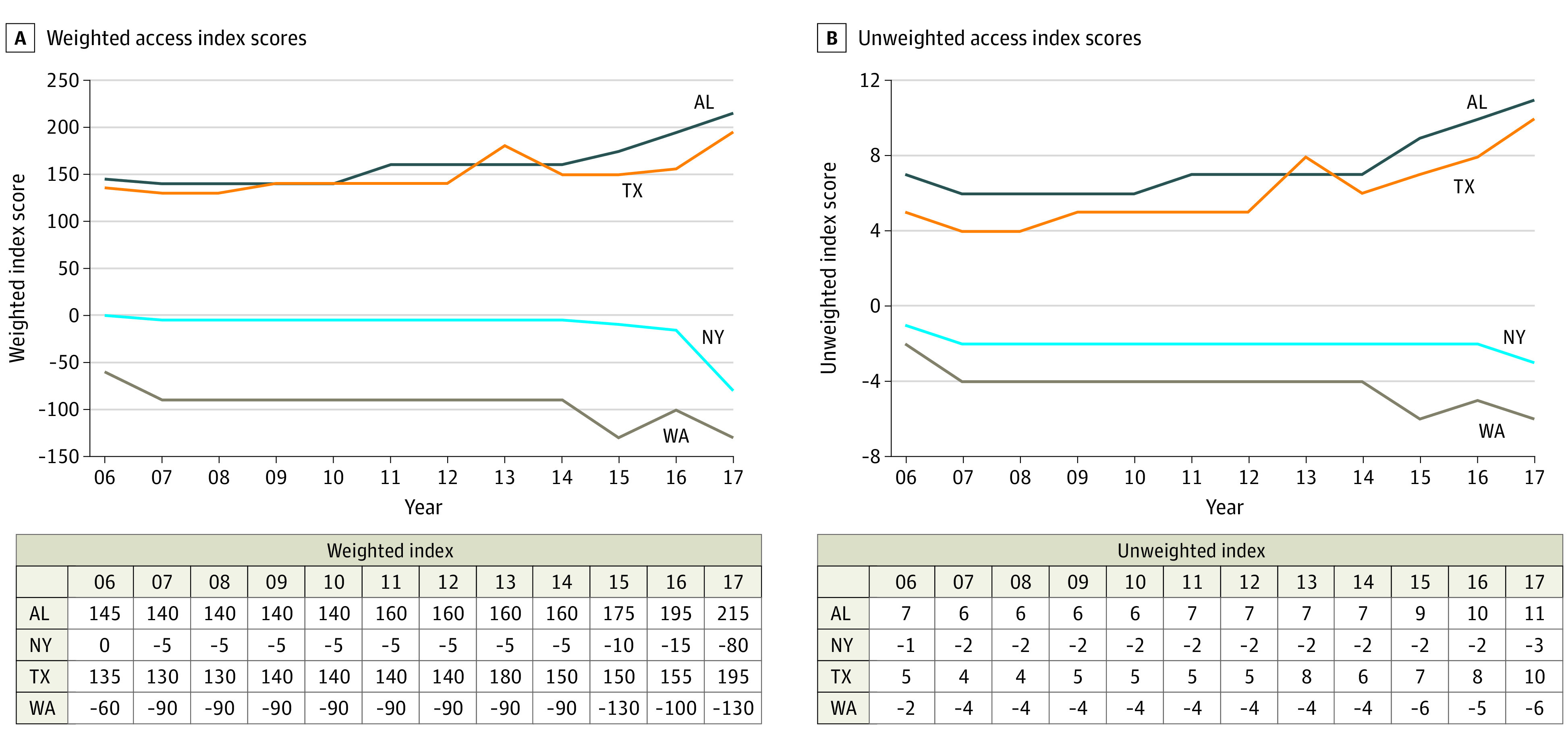
Weighted (A) and unweighted (B) access index scores derived from 17 categories defined by the National Abortion and Reproductive Rights Action League (NARAL),14 with higher scores on the index representing lower access (also see the eMethods in the Supplement). We chose Alabama (AL), New York (NY), Texas (TX), and Washington (WA) semirandomly to provide a visual presentation of the dynamics of the access index over time. Note that year labels are abbreviated due to space constraints.
During the study period, annual rates of death due to suicide among women of reproductive age (ages 20-34 years; target group) ranged from 1.4 to 25.6 per 100 000 (annual rates of death due to suicide across 50 states for the entire study period are detailed in eTable 3 in the Supplement). Annual rates of death due to suicide in the control group (women postreproductive age, ages 45-64 years) ranged from 2.7 to 33.2 per 100 000 during the study period. Annual motor vehicle crash death rates among women of reproductive age ranged from 2.4 to 42.9 per 100 000.
Among reproductive-aged women, the weighted average annual-state level suicide rate when no TRAP laws were enforced was 5.5 per 100 000 deaths. We found that the enforcement of a TRAP law was related to higher suicide rates among reproductive-aged women (β = 0.17; 95% CI, 0.03 to 0.32; P = .02) but not to suicide rates among women of postreproductive age (β = 0.06; 95% CI, –0.11 to 0.24; P = .47) (Table 1). Examining the nonnormalized β (β = 0.32; 95% CI, 0.06 to 0.58; P = .02) implies that the enforcement of a TRAP law was associated with a 5.81% higher suicide rate among reproductive-aged women compared with the pre-enforcement years’ mean (ie, 0.32 divided by 5.5, the average suicide death rate for 100 000 women when no TRAP laws were enforced).
Table 1. Multivariate Regression Analysis With State and Year Fixed Effects for TRAP Law Enforcement, Suicide Rates, and Motor Vehicle Crash Death Rates From 1976 to 2016a.
| Variableb | Suicide rate | Motor vehicle crash death rate for those aged 20-34 y | ||||
|---|---|---|---|---|---|---|
| Age 20-34 y | Age 45-64 y | |||||
| β (95% CI) | P value | β (95% CI) | P value | β (95% CI) | P value | |
| TRAP law index | 0.17 (0.03 to 0.32) | .02 | 0.06 (–0.11 to 0.24) | .47 | 0.03 (–0.04 to 0.11) | .36 |
| Black or African Americanc | 1.12 (–0.59 to 2.83) | .19 | 0.87 (–0.83 to 2.58) | .31 | 0.23 (–0.35 to 0.80) | .43 |
| Fraction Republicand | 0.04 (–0.07 to 0.15) | .44 | 0.02 (–0.10 to 0.15) | .72 | 0.07 (–0.01 to 0.15) | .08 |
| State GDP growthe | 0.08 (–0.05 to 0.20) | .22 | –0.00 (–0.07 to 0.06) | .92 | 0.06 (–0.01 to 0.13) | .10 |
| State unemployment ratef | 0.09 (–0.07 to 0.25) | .26 | 0.08 (–0.02 to 0.18) | .10 | –0.12 (–0.20 to –0.04) | .005 |
| No. of observations | 1022 | 1467 | 1631 | |||
| R2 | 0.69 | 0.75 | 0.83 | |||
Abbreviations: GDP, gross domestic product; TRAP, Targeted Regulation of Abortion Providers.
Three weighted least-square regression models weighted by state population. Standard errors are clustered at the state and year level.
All independent variables (first 5 rows) were z scored.
Percentage of state residents who are Black or African American.
Fraction of senators representing the state in the US Senate who are Republican.
Annual state-level GDP growth rate.
Annual state-level unemployment rate.
In terms of specificity, TRAP law enforcement was not associated with death rates due to motor vehicle crashes in reproductive-aged women (β = 0.03; 95% CI, –0.04 to 0.11; P = .36) (Table 1). In terms of sensitivity, results were similar when age groups were defined less narrowly (ie, ages 20-44 years and 45-74 years for the target and control groups, respectively) and using all available age bins (eTables 4 and 5 in the Supplement). Finally, a model that used all available data on TRAP law enforcement and suicide rates from 1974 to 2016 but did not account for unemployment rate (ie, available only from 1976) revealed similar findings to the main analysis (eTable 6 in the Supplement).
In terms of robustness, restricted access to reproductive care based on scores on the weighted access index was also associated with higher suicide rates among reproductive-aged women (β = 0.41; 95% CI, 0.08 to 0.74; P = .02) but not among women of postreproductive age (β = 0.21; 95% CI, –0.18 to 0.60; P = .26) (Table 221). This association was not observed with motor vehicle crash death rates among reproductive-aged women (β = 0.01; 95% CI, –0.19 to 0.21; P = .90) (Table 2). Results were similar when age groups were defined less narrowly (ie, ages 20-44 years and 45-74 years) and using the unweighted access index (eTables 7 and 8 in the Supplement).
Table 2. Multivariate Regression Analysis With State and Year Fixed Effects for the Weighted Access Index, Suicide Rates, and Motor Vehicle Crash Death Rates From 2006 to 2017a.
| Variableb | Suicide rate | Motor vehicle crash death rate for those aged 20-34 y | ||||
|---|---|---|---|---|---|---|
| Age 20-34 y | Age 45-64 y | |||||
| β (95% CI) | P value | β (95% CI) | P value | β (95% CI) | P value | |
| Weighted access indexc | 0.41 (0.08 to 0.74) | .02 | 0.21 (–0.18 to 0.60) | .26 | 0.01 (–0.19 to 0.21) | .90 |
| Black or African Americand | 0.57 (–2.27 to 3.40) | .67 | 1.26 (–2.82 to 5.33) | .51 | –2.07 (–3.83 to –0.31) | .03 |
| Fraction Republicane | –0.05 (–0.29 to 0.18) | .62 | 0.04 (–0.17 to 0.24) | .70 | –0.00 (–0.08 to 0.07) | .93 |
| State GDP growthf | –0.11 (–0.23 to 0.01) | .06 | –0.05 (–0.12 to 0.02) | .12 | –0.03 (–0.11 to 0.05) | .47 |
| State unemployment rateg | 0.00 (–0.34 to 0.34) | .98 | 0.14 (–0.05 to 0.33) | .14 | –0.11 (–0.29 to 0.08) | .22 |
| No. of observations | 220 | 415 | 337 | |||
| R2 | 0.84 | 0.87 | 0.91 | |||
Abbreviation: GDP, gross domestic product.
Three weighted least-square regression models weighted by state population. Standard errors are clustered at the state and year level.
All independent variables (first 5 rows) were z scored.
Measuring accessibility to a broad set of reproductive health services in each state.21
Percentage of state residents who are Black or African American.
Fraction of senators representing the state in the US Senate who are Republican.
Annual state-level GDP growth rate.
Annual state-level unemployment rate.
Lastly, we tested for pre-trends in suicide rates in the 21 states that enforced at least 1 TRAP law. We visualized the significant association between TRAP law enforcement and increased suicide rate in Figure 3, which was documented among reproductive-aged women (Figure 3A) but not among postreproductive-aged women (Figure 3B). This analysis showed no pre-trends in suicide rates in the years before enforcement of TRAP laws among women included in the study. In addition, this analysis, conducted within TRAP law states, suggests that TRAP law enforcement was associated with increased suicide rates beyond any other fundamental differences that could exist between the TRAP law states vs those states that have never enacted such laws. Visualization of the nonsignificant association between TRAP law enforcement and motor vehicle crash death rates is included in eFigure 5 in the Supplement.
Figure 3. Dynamic Difference-in-Differences in Suicide Rates Around a Targeted Regulation of Abortion Providers (TRAP) Law Enforcement Split by Relative Years of Enforcement.
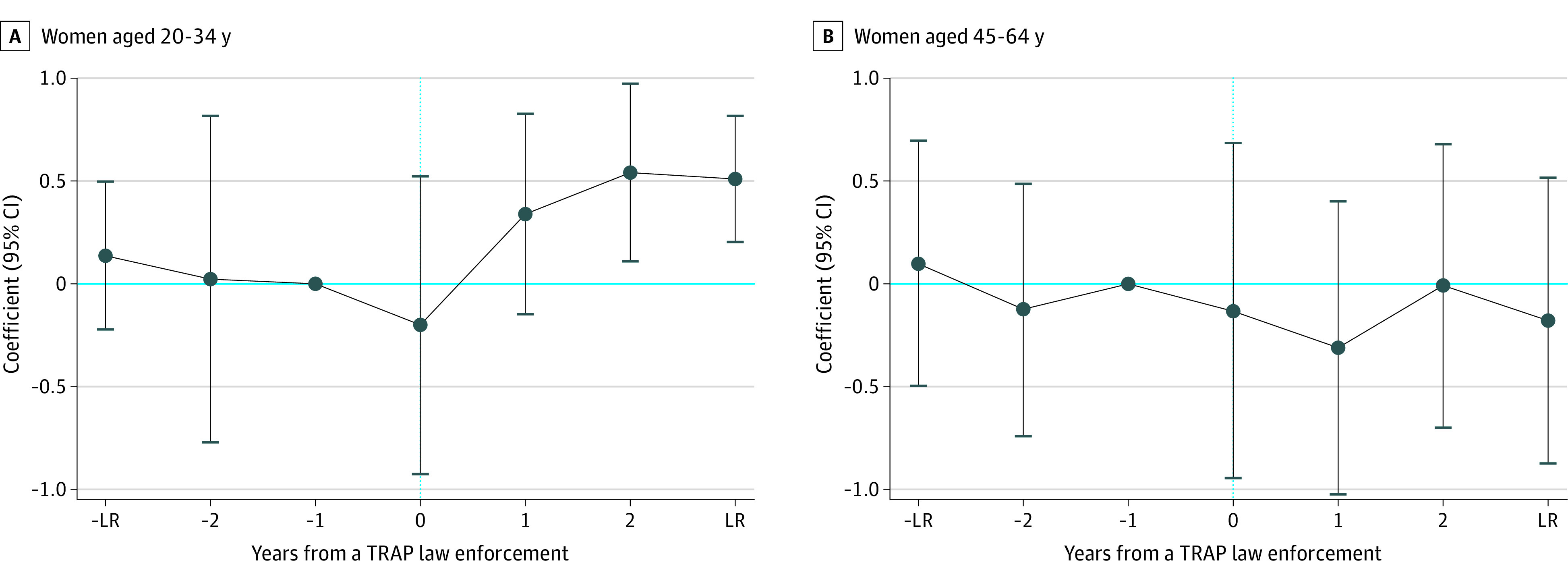
The coefficients and 95% CI of a dynamic difference-in-differences analysis regressed on the target group of women aged 20 to 34 years (A) and on the control group, which is women aged 45 to 64 years (B). −LR is a dummy variable turning one 3 years before the enforcement and earlier, and LR is a dummy variable turning one 3 years after the enforcement onward.
Discussion
We provide evidence that restricted access to reproductive care based on state-level data from 1974 to 2016 was associated with suicide rates among reproductive-aged women. Specifically, enforcement of a TRAP law was associated with a 5.81% higher annual rate of suicide than in pre-enforcement years. The average rate of suicide, which is among the 3 leading causes of death in the study population, was 5.5 per 100 000 deaths in the pre-enforcement years. There was specificity in the association since we found no link between restricted access to reproductive care and suicide rates among women of postreproductive age and no link between restricted access to reproductive care and death rates due to another leading cause of death among young women, namely motor vehicle crashes. The associations were robust across 3 different measures of access to reproductive care: a TRAP laws index, a weighted access index, and an unweighted access index. We leveraged a difference-in-differences design that allowed us to establish that associations were robust to the inclusion of potential confounders, including macro-level economic, demographic, and political factors, fixed effects at the time and state level, and across different categorizations for our age bins. Our findings galvanize a growing interest in the macro-level determinants of mental health22,23 and point to a potential modifiable risk factor that policy makers could address to mitigate suicide risk among reproductive-aged women.
The findings are significant for several reasons, especially given that suicide represents the second (ages 20-24 years) and third (ages 25-34 years) leading cause of death among reproductive-aged women.1 First, our finding that restricted access to reproductive care may represent a risk factor for suicide specifically among reproductive-aged women has vital clinical implications. Clinicians should be cognizant of the additional stresses that restricted access to reproductive care engenders as it pertains to clinical care and suicide prevention for women of reproductive age. Second, the findings inform ethical considerations surrounding access to abortions and reproductive care more broadly,24,25 even as the issue remains at the center of a divisive debate in the United States following the recent ruling on Roe v Wade.26 Third, our findings contribute to a “multilevel” approach for suicide prevention that relies on integrating individual- and population-level factors.27,28,29 Indeed, a growing body of literature has documented associations between state-level factors and suicide risk, for example, same-sex marriage policies.5 Third, our findings highlight the need for studies to identify mechanisms through which restricted access to reproductive care could affect risk for suicide among reproductive-aged women, including by amplifying stress and anxiety,30,31 which are established risk factors for suicidal ideation and behavior,2,3 or by eliminating autonomy in decision-making around childbirth and reproductive care.
Limitations
Our study design was ecologic and relied on state-level data, which entails important limitations. We did not have individual-level data and therefore could not assess the association between restrictions to reproductive care and reports of anxiety, stress, or suicidal ideation among reproductive-aged women, nor did we have individual-level data on the proportion of suicides that specifically occurred among pregnant women. Thus, our interpretation of the findings is based on prior studies conducted at the individual level establishing links between restricted access to reproductive care and adverse mental health outcomes among reproductive-aged women.31,32 Prospective clinical and observational studies are needed to assess individual-level mental health outcomes, including death due to suicide, following restrictions to reproductive care. In addition, we do not have higher-resolution data on the dynamic changes in actual access to reproductive care within a state, including distance to a neighboring state with access to abortion.33 Moreover, a key design decision was to define our exposure variable based on restrictions to abortion (ie, an exogenous, macro-level factor), rather than actual abortion rate. This decision was motivated by the fact that the association between abortion rates and suicide could be driven by opposite forces that are impossible to disentangle using population-level data, including the possibility that higher rates of unplanned pregnancy among women experiencing mental health symptoms might lead to a positive correlation between abortion and suicide rates.34 Additionally, although models accounted for the proportion of the population who identified as Black individuals at the state-year level, we did not analyze other racial and ethnic categories and we did not have granular data on race differences in access to reproductive care within states, nor did we have sufficient data on race differences in state-level suicide rates. These are important limitations in the context of established racial and ethnic disparities in access to reproductive care17,35 and differences in suicide rates in the United States on the basis of race and ethnicity.36
Other study limitations also warrant consideration. First, we used observational data, limiting our ability to draw causal inferences. However, our implementation of a difference-in-differences approach represents a preferred approach to analyzing observational data for inferring causality.21 Second, although challenging to quantify, at least some deaths by suicide occur through motor vehicle crashes.37 Thus, deaths due to suicide may have been underestimated, while deaths due to actual motor vehicle crashes may have been overestimated. Accordingly, the true magnitude of the association between restrictions to reproductive care and suicide may be greater than we report. Moreover, the misclassification of suicides more generally38 could have resulted in an underestimation in the reported estimates. Third, our theoretical framework and hypotheses were premised on prior literature examining how restricted access to reproductive care specifically affects suicide risk among women.8,11 Future studies are warranted at both an individual and population level to investigate how changes in access to reproductive care are related to mental health outcomes among other groups (eg, men, children). Fourth, we relied on data on annual suicide rates released by the CDC. Accordingly, some data were not available, which could have led to an ascertainment bias. Nevertheless, data from which our findings were derived included 1115 observations from across 50 states, recorded between 1974 and 2016, and encompassing the full range of TRAP law enforcement from 0 to 3. Fifth, data were only available up to 2016, and findings may not generalize to the current context or recent laws surrounding abortion access. Finally, the nature of the abortion debate in the United States is unique. Thus, the finding of an association between restricted access to reproductive care and increased suicide rates among reproductive-aged women may not generalize to other countries.
Conclusions
In this longitudinal ecologic study with a difference-in-differences analysis of US women, restrictions on access to reproductive care from 1974 to 2016 were associated with suicide rates among reproductive-aged women. Thus, access to reproductive care may represent a potentially modifiable population-level suicide risk factor for reproductive-aged women. The results may have important implications for clinicians and policy makers in the United States. However, given the limitations of the design of this study, further research is needed to assess whether current factors affecting access to reproductive care services are related to suicide risk among women of reproductive age and to inform suicide prevention strategies.
eMethods. Access index scoring scheme
eTable 1. Detailed description of the Targeted Regulation of Abortion Providers (TRAP) laws in the United States
eTable 2. TRAP laws dynamics in the United States during the study period
eTable 3. Rates of death due to suicide (per 100,000) among women of reproductive age (20-34) from 1974-2016
eTable 4. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1976 and 2016 examining wider age ranges.
eTable 5. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1976 and 2016 examining all age bins.
eTable 6. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1974 and 2016 excluding unemployment rate.
eTable 7. Multivariate regression analysis with state and year fixed effects for the weighted access index, suicide rates, and motor vehicle crashes deaths between 2006 and 2017 examining wider age ranges.
eTable 8. Multivariate regression analysis with state and year fixed effects for the unweighted access index, suicide rates, and motor vehicle crashes deaths between 2006 and 2017.
eFigure 1. Suicide death rates (left panel) and motor vehicle crashes death rates of women ages 20-34 and 45-64 in the United States during the study period.
eFigure 2. Total number of enforced TRAP laws at the state- and year-level
eFigure 3. Unweighted Access Index by year from 2006-2017
eFigure 4. Weighted Access Index by year from 2006-2017
eFigure 5. Dynamic difference-in-differences in motor vehicle accident death rates around a TRAP law enforcement split by relative years of enforcement
References
- 1.Centers for Disease Control and Prevention, National Vital Statistics System . Leading causes of death. Accessed May 13, 2022. https://www.cdc.gov/nchs/nvss/leading-causes-of-death.htm
- 2.Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156(2):181-189. doi: 10.1176/ajp.156.2.181 [DOI] [PubMed] [Google Scholar]
- 3.Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227-1239. doi: 10.1016/S0140-6736(15)00234-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gunnell D, Lewis G. Studying suicide from the life course perspective: implications for prevention. Br J Psychiatry. 2005;187:206-208. doi: 10.1192/bjp.187.3.206 [DOI] [PubMed] [Google Scholar]
- 5.Raifman J, Moscoe E, Austin SB, McConnell M. Difference-in-differences analysis of the association between state same-sex marriage policies and adolescent suicide attempts. JAMA Pediatr. 2017;171(4):350-356. doi: 10.1001/jamapediatrics.2016.4529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Occhipinti JA, Skinner A, Doraiswamy PM, et al. Mental health: build predictive models to steer policy. Nature. 2021;597(7878): 633-636. doi: 10.1038/d41586-021-02581-9 [DOI] [PubMed] [Google Scholar]
- 7.Cohen IG, Adashi EY, Gostin LO. The Supreme Court, the Texas abortion law (SB8), and the beginning of the end of Roe v Wade? JAMA. 2021;326(15):1473-1474. doi: 10.1001/jama.2021.17639 [DOI] [PubMed] [Google Scholar]
- 8.Stotland NL. Update on reproductive rights and women’s mental health. Med Clin North Am. 2019;103(4):751-766. doi: 10.1016/j.mcna.2019.02.006 [DOI] [PubMed] [Google Scholar]
- 9.Major B, Cozzarelli C, Cooper ML, et al. Psychological responses of women after first-trimester abortion. Arch Gen Psychiatry. 2000;57(8):777-784. doi: 10.1001/archpsyc.57.8.777 [DOI] [PubMed] [Google Scholar]
- 10.Steinberg JR, Laursen TM, Adler NE, Gasse C, Agerbo E, Munk-Olsen T. The association between first abortion and first-time non-fatal suicide attempt: a longitudinal cohort study of Danish population registries. Lancet Psychiatry. 2019;6(12):1031-1038. doi: 10.1016/S2215-0366(19)30400-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Foster DG. The Turnaway Study: Ten Years, a Thousand Women, and the Consequences of Having—or Being Denied—an Abortion. Simon & Schuster; 2021. [Google Scholar]
- 12.Austin N, Harper S. Constructing a longitudinal database of targeted regulation of abortion providers laws. Health Serv Res. 2019;54(5):1084-1089. doi: 10.1111/1475-6773.13185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zandberg J. Family comes first: reproductive health and the gender gap in entrepreneurship. J Financ Econ. 2021;140:838-864. doi: 10.1016/j.jfineco.2020.06.020 [DOI] [Google Scholar]
- 14.NARAL Pro-Choice America . 2017 Who decides? the status of women’s reproductive rights in the United States. Accessed January 4, 2022. https://www.prochoiceamerica.org/report/2017-decides-status-womens-reproductive-rights-united-states/
- 15.Centers for Disease Control and Prevention . CDC Wide-ranging Online Data for Epidemiologic Research (WONDER) [database]. Accessed January 4, 2022. https://wonder.cdc.gov/
- 16.Hawton K, Haw C. Economic recession and suicide. BMJ. 2013;347:f5612. doi: 10.1136/bmj.f5612 [DOI] [PubMed] [Google Scholar]
- 17.Sutton MY, Anachebe NF, Lee R, Skanes H. Racial and ethnic disparities in reproductive health services and outcomes, 2020. Obstet Gynecol. 2021;137(2):225-233. doi: 10.1097/AOG.0000000000004224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Harvard Dataverse . Charles Stewart’s congressional data dataverse. Accessed November 23, 2022. https://dataverse.harvard.edu/dataverse/congdata
- 19.GitHub , Barzilay R. Data and analysis: abortion laws and suicide. Accessed November 29, 2022. https://github.com/barzilab1/abortion-laws-and-suicide
- 20.Columbia Public Health . Difference-in-difference estimation. Accessed January 4, 2022. https://www.publichealth.columbia.edu/research/population-health-methods/difference-difference-estimation
- 21.Bind MA. Causal modeling in environmental health. Annu Rev Public Health. 2019;40:23-43. doi: 10.1146/annurev-publhealth-040218-044048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rose-Clarke K, Gurung D, Brooke-Sumner C, et al. Rethinking research on the social determinants of global mental health. Lancet Psychiatry. 2020;7(8):659-662. doi: 10.1016/S2215-0366(20)30134-6 [DOI] [PubMed] [Google Scholar]
- 23.Davidson KW, Krist AH, Tseng CW, et al. Incorporation of social risk in US Preventive Services Task Force recommendations and identification of key challenges for primary care. JAMA. 2021;326(14):1410-1415. doi: 10.1001/jama.2021.12833 [DOI] [PubMed] [Google Scholar]
- 24.Maxmen A. Why hundreds of scientists are weighing in on a high-stakes US abortion case. Nature. 2021;599(7884):187-189. doi: 10.1038/d41586-021-02834-7 [DOI] [PubMed] [Google Scholar]
- 25.The Lancet . Why Roe v. Wade must be defended. 2022;399(10338):1845. doi: 10.1016/S0140-6736(22)00870-4 [DOI] [PubMed] [Google Scholar]
- 26.Cohen IG, Murray M, Gostin LO. The end of Roe v Wade and new legal frontiers on the constitutional right to abortion. JAMA. 2022;328(4):325-326. doi: 10.1001/jama.2022.12397 [DOI] [PubMed] [Google Scholar]
- 27.Christensen H, Cuijpers P, Reynolds CF III. Changing the direction of suicide prevention research: a necessity for true population impact. JAMA Psychiatry. 2016;73(5):435-436. doi: 10.1001/jamapsychiatry.2016.0001 [DOI] [PubMed] [Google Scholar]
- 28.van der Feltz-Cornelis CM, Sarchiapone M, Postuvan V, et al. Best practice elements of multilevel suicide prevention strategies: a review of systematic reviews. Crisis. 2011;32(6):319-333. doi: 10.1027/0227-5910/a000109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Barzilay R, Moore TM, Calkins ME, et al. Deconstructing the role of the exposome in youth suicidal ideation: trauma, neighborhood environment, developmental and gender effects. Neurobiol Stress. 2021;14:100314. doi: 10.1016/j.ynstr.2021.100314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Biggs MA, Gould H, Barar RE, Foster DG. Five-year suicidal ideation trajectories among women receiving or being denied an abortion. Am J Psychiatry. 2018;175(9):845-852. doi: 10.1176/appi.ajp.2018.18010091 [DOI] [PubMed] [Google Scholar]
- 31.Biggs MA, Upadhyay UD, McCulloch CE, Foster DG. Women’s mental health and well-being 5 years after receiving or being denied an abortion: a prospective, longitudinal cohort study. JAMA Psychiatry. 2017;74(2):169-178. doi: 10.1001/jamapsychiatry.2016.3478 [DOI] [PubMed] [Google Scholar]
- 32.Foster DG, Steinberg JR, Roberts SCM, Neuhaus J, Biggs MA. A comparison of depression and anxiety symptom trajectories between women who had an abortion and women denied one. Psychol Med. 2015;45(10):2073-2082. doi: 10.1017/S0033291714003213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Thompson KMJ, Sturrock HJW, Foster DG, Upadhyay UD. Association of travel distance to nearest abortion facility with rates of abortion. JAMA Netw Open. 2021;4(7):e2115530-e2115530. doi: 10.1001/jamanetworkopen.2021.15530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hall KS, Kusunoki Y, Gatny H, Barber J. The risk of unintended pregnancy among young women with mental health symptoms. Soc Sci Med. 2014;100:62-71. doi: 10.1016/j.socscimed.2013.10.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Prather C, Fuller TR, Jeffries WL IV, et al. Racism, African American women, and their sexual and reproductive health: a review of historical and contemporary evidence and implications for health equity. Health Equity. 2018;2(1):249-259. doi: 10.1089/heq.2017.0045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ramchand R, Gordon JA, Pearson JL. Trends in suicide rates by race and ethnicity in the United States. JAMA Netw Open. 2021;4(5):e2111563. doi: 10.1001/jamanetworkopen.2021.11563 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Radun I, Radun J, Kaistinen J, et al. Suicide by crashing into a heavy vehicle: professional drivers’ views. Traffic Inj Prev. 2019;20:826-831. doi: 10.1080/15389588.2019.1679796 [DOI] [PubMed] [Google Scholar]
- 38.Kapusta ND, Tran US, Rockett IRH, et al. Declining autopsy rates and suicide misclassification: a cross-national analysis of 35 countries. Arch Gen Psychiatry. 2011;68(10):1050-1057. doi: 10.1001/archgenpsychiatry.2011.66 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods. Access index scoring scheme
eTable 1. Detailed description of the Targeted Regulation of Abortion Providers (TRAP) laws in the United States
eTable 2. TRAP laws dynamics in the United States during the study period
eTable 3. Rates of death due to suicide (per 100,000) among women of reproductive age (20-34) from 1974-2016
eTable 4. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1976 and 2016 examining wider age ranges.
eTable 5. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1976 and 2016 examining all age bins.
eTable 6. Multivariate regression analysis with state and year fixed effects for TRAP laws’ enforcement, suicide rates, and motor vehicle crashes deaths between 1974 and 2016 excluding unemployment rate.
eTable 7. Multivariate regression analysis with state and year fixed effects for the weighted access index, suicide rates, and motor vehicle crashes deaths between 2006 and 2017 examining wider age ranges.
eTable 8. Multivariate regression analysis with state and year fixed effects for the unweighted access index, suicide rates, and motor vehicle crashes deaths between 2006 and 2017.
eFigure 1. Suicide death rates (left panel) and motor vehicle crashes death rates of women ages 20-34 and 45-64 in the United States during the study period.
eFigure 2. Total number of enforced TRAP laws at the state- and year-level
eFigure 3. Unweighted Access Index by year from 2006-2017
eFigure 4. Weighted Access Index by year from 2006-2017
eFigure 5. Dynamic difference-in-differences in motor vehicle accident death rates around a TRAP law enforcement split by relative years of enforcement