

Abstract
Introduction
Research participants have a growing expectation for transparency with their collected information; however, there is little guidance on participant preferences for receiving health information and how researchers should return this information to participants.
Methods
We conducted a cross-sectional online survey with a representative sample of 502 participants in the United States. Participants were asked about their preferences for receiving, sharing, and the formatting of health information collected for research purposes.
Results
Most participants wanted their health information returned (84%) to use it for their own knowledge and to manage their own health. Email was the most preferred format for receiving health data (67%), followed by online website (44%), and/or paper copy (32%). Data format preferences varied by age, education, financial resources, subjective numeracy, and health literacy. Around one third of Generation Z (25%), Millennials (30%), and Generation X (29%) participants preferred to receive their health information with a mobile app. In contrast, very few Baby Boomers (12%) and none from the Silent Generation preferred the mobile app format. Having a paper copy of the data was preferred by 38% of participants without a college degree compared to those with a college degree. Preferences were highest for sharing all health information with doctors and nurses (77%), and some information with friends and family (66%).
Conclusion
Study findings support returning research information to participants in multiple formats, including email, online websites, and paper copy. Preferences for whom to share information with varied by stakeholders and by sociodemographic characteristics. Researchers should offer multiple formats to participants and tailor data sharing options to participants’ preferences. Future research should further explore combinations of individual characteristics that may further influence data sharing and format preferences.
Keywords: Transparency, Trust, Patient-reported outcomes, Health informatics, Recruitment
1. INTRODUCTION
People have access to thousands of mobile health applications and health tracking devices worldwide.1 With on-demand access to personal health data through mobile devices, there is a growing expectation for transparency with health data in other domains, such as in healthcare and health research. Health informatics researchers frequently use mobile health technologies to collect health data with the intention of developing health-related interventions. However, there is no standardized approach to return collected health data to research participants, despite participants’ willingness to have it returned.2,3 Researchers face an ongoing challenge to understand what information people want returned to them, how to return collected health information, and how to ensure privacy and trust when sharing collected health information.3–5
International mandates have been developed in response to user expectations for data access and transparency, but policies, laws, and implementation vary widely by country and by state. In the European Union, the General Data Protection Regulation (GDPR) protects data access rights and privacy for individuals.6 The GDPR also outlines key principles to protect the rights of personal data for research participants, particularly when sharing data for research purposes.7 Likewise, in Canada, users have the Personal Information Protection and Electronic Documents Act (PIPEDA) which allows users to obtain access to, correct, and report the mis-management of personal information from private sector organizations.8 In the United States (US), initiatives such as HIPAA, OpenNotes, and the 21st Century Cures Act promote patient access to electronic health information.9,10 The recent Information Blocking Rule of the Cures Act goes a step further by enacting consequences to ‘information blockers’ who restrict access to health information.11,12 Despite substantive efforts to improve data access and sharing in healthcare in the US, researchers are still trying to determine the best practices around returning and sharing research data with participants.13,14
Research participants prefer to have access to their collected health information,15–17 yet most research studies do not return participant information. If data is returned it is typically not in an accessible format.15,18 Among studies that do return health information, it is most frequently genetic information or lab results that require a genetic counselor or conversation with a specialist to interpret sensitive information.19,20 Other large-scale studies, such as the All of Us, offer an online research portal for access to their information.21 There is wide variation in how health information is communicated, and that the format can impact health behaviors, communication with clinicians, and comprehension of the information.22–24
Overall, there is a lack of standardization for returning health information to research participants in ways that respect participants’ privacy and transparency. In this study, we evaluated public perceptions among a representative US sample of participants to explore the reasons for participants wanting data returned to them, preferences on the format of data return, and actions taken with their data, including data sharing preferences.
2. MATERIALS AND METHODS
2.1. Study design
In March 2021, we recruited 502 participants representative of the US population using Prolific, an online survey recruitment platform.25 Prolific uses an algorithm to select participants based on population proportions from US Census data. Prolific consists of verified users who are willing to participate in research studies and facilitates the recruitment and compensation for participating. Participants were directed to complete a cross-sectional survey that included questions on socio-demographic information, preferences on the return of research information, preferences for the format to receive collected health information, and preferences on how much health information to share with key stakeholder groups. This study received ethical approval from the Institutional Review Board at Weill Cornell Medicine.
2.2. Participants
Participants were over 18 years of age and representative of the US population by age, sex, and race. All participants provided informed consent and were compensated $15 per hour.
2.3. Data collection
The survey included socio-demographic information and validated instruments to measure health literacy26, subjective numeracy27, and graph literacy28. The survey included questions including: 1) ranking how importance of having their collected health research information returned to them, 2) selecting all of their preferred formats for receiving their data from a list including: e-mail, text message, online website, mobile app, paper copy, and other, 3) rating how much of their collected health information they would share with various stakeholder groups, 4) indicating what actions they would take with their collected health information, and 5) indicating whether or not they should be compensated for sharing their health information with health tech companies. Full questions and response options are detailed in Figure 1.
Figure 1.
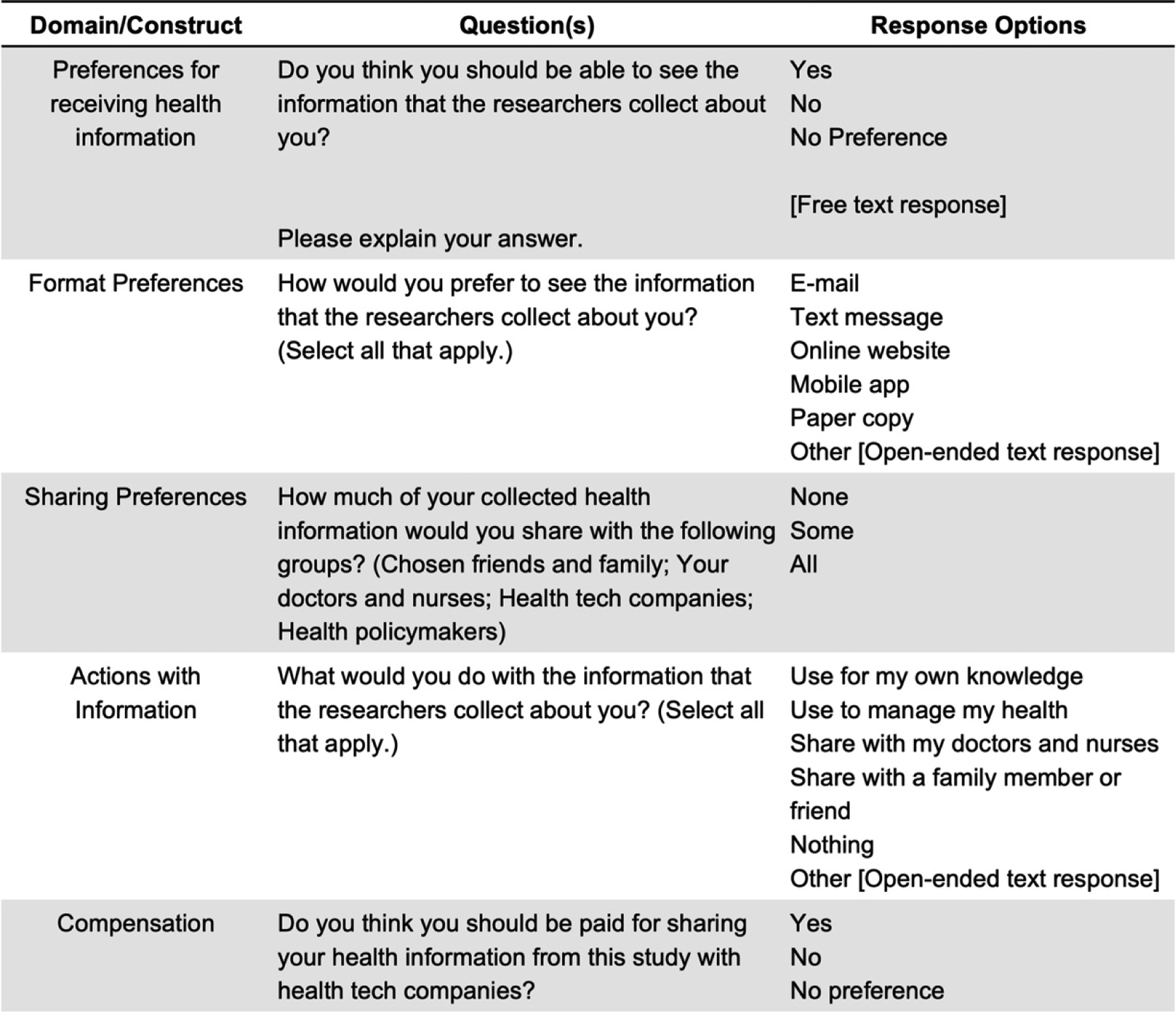
Questions asked in the survey to explore data format and sharing preferences
2.4. Statistical analysis
Descriptive and summary statistics on sociodemographic variables, literacy, numeracy, data access responses, data format preferences, actions taken with collected data, data sharing desires, and data compensation preferences were calculated. Differences in the respondents’ selections to questions regarding actions with collected data, and data format preferences were assessed with Cochran’s Q test. Comparisons of proportions of each preferred format of data delivery differed when stratified by various sociodemographic variables – including age, race, gender, ethnicity, education, health literacy, graph literacy, and subjective numeracy. Age was grouped by generation: Generation Z (18–24), Millennials (25–40), Generation X (41–56), Baby Boomers (57–75), Silent Generation (76–93) as defined by the Pew Research Center.29 Differences across groups were assessed with the Chi-squared test or Fisher’s exact test.
2.5. Qualitative Analysis
Responses from the free text response question asking preference to receive health information were compiled in a single file using Microsoft Excel. Two members of the research team reviewed 10% of responses together and established relevant categories for analysis. Two reviewers then independently double-coded the next 10% of responses into previously established categories to establish inter-rater reliability.30 A Cohen’s kappa statistic was calculated to measure inter-rater reliability. The remaining responses were independently coded, and consensus was reached through dialogue with the rest of the team.
3. RESULTS
Among the 502 participants who completed the survey, about half (51%) were female, 74% were White, 13% were Black or African American, 7% were Asian, and 7% were of Hispanic or Latino origin (Table 1). The average age of the sample was 46 years (SD: 16), and participants mainly comprised Millennials (32%), Generation X (26%) and Baby Boomers (32%). Fifty-eight percent reported having at least a college degree, and 25% reported financial instability or not having enough to make ends meet. Overall, subjective numeracy was moderate (41%) or low (33%), health literacy was adequate (72%), and graph literacy was good or fair (77%).
Table 1.
Demographic characteristics of the survey sample
| Variable | Overall (n=502) |
|---|---|
| Demographics | |
| Age (mean, SD)* | 46.6 (±16.0) |
| Generation Z | 44 (9) |
| Milennials | 158 (32) |
| Generation X | 132 (26) |
| Baby Boomers | 162 (32) |
| Silent Generation | 6 (1) |
| Gender (n, %) | |
| Female | 254 (51) |
| Male | 243 (48) |
| Non-binary or gender diverse | 5 (1.0) |
| Race (n, %) | |
| Asian | 36 (7) |
| Black or African American | 65 (13) |
| Multi-Race | 19 (4) |
| Native American or Alaska Native | 5 (1) |
| Native Hawaiian or Pacific Islander | 1 (0.2) |
| White | 370 (74) |
| Identifies as race not listed | 6 (1) |
| Hispanic or Latino Origin (n, %) | 34 (7) |
| Socioeconomic Status | |
| Education (n, %) | |
| High school graduate or less | 47 (9) |
| Some college or Bachelor’s | 345 (69) |
| Graduate degree | 110 (22) |
| Financial resources (n, %) | |
| Not enough | 126 (25) |
| Enough | 297 (59) |
| More than enough | 79 (16) |
| Disability status (n, %) | |
| Physical disability | 39 (8) |
| Hearing-related disability | 10 (2) |
| Eyesight-related disability | 19 (4) |
| Other disability | 104 (21) |
| No disability | 430 (86) |
| Literacy and Numeracy | |
| Health Literacy25 (n %) | |
| Adequate | 363 (72) |
| Limited/Marginal | 139 (28) |
| Subjective Numeracy26 (n %) | |
| Low (3–12) | 165 (33) |
| Medium (13–15) | 208 (41) |
| High (16–18) | 129 (26) |
| Graph Literacy27 n (%) | |
| Good/Fair | 388 (77) |
| Poor/Very Poor | 114 (23) |
The generational age ranges include: Generation Z (18–24), Millennials (25–40), Generation X (41–56), Baby Boomers (57–75), Silent Generation (76–93) as defined by the Pew Research Center.29
3.1. Format preferences for receiving data
Most participants (84%) want their health information returned, 15% had no preference, and only 1% did not want their collected health information returned to them. The most preferred format for receiving health information was email (67%), online website (44%) and paper copy (32%) (Figure 2). Participants selected an average of 1.8 formats for the return of their health information.
Figure 2.
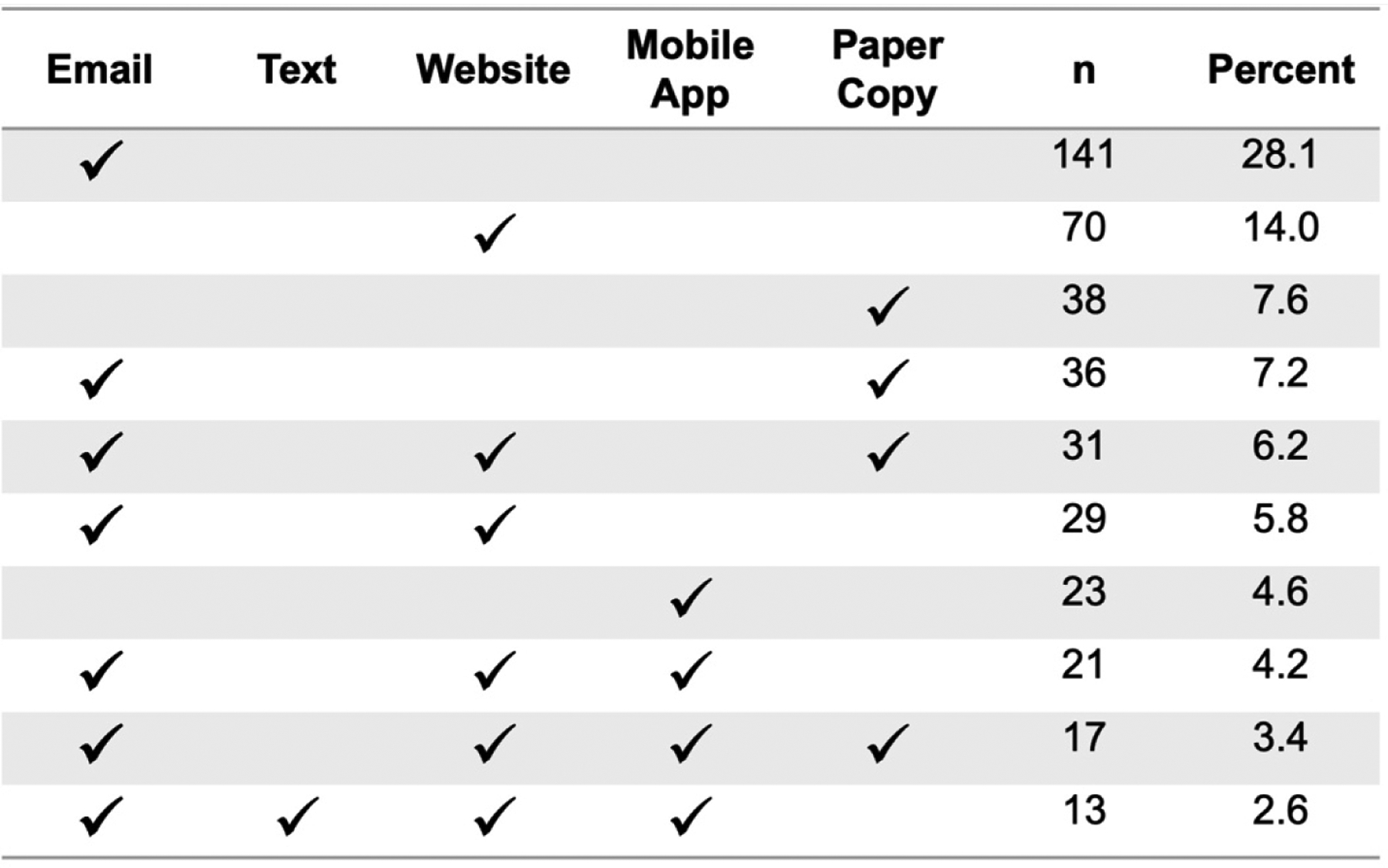
Participant preferences for format of receiving health information. This figure displays the top ten most common selections and combinations of participant format preferences based on responses to a ‘select all that apply’ question asking: How would you prefer to see the information that the researchers collect about you?.
Email and online website were the most preferred ways to receive health information returned across all age groups. Preferences for receiving health information using a mobile app differed by age. Almost one third of Generation Z (25%), Millennials (30%), and Generation X (29%) preferred to receive their health information through a mobile app, whereas less than a quarter of Baby Boomers (12%) and no one in the Silent Generation (0%) preferred the mobile app format (p < 0.01). Figure 3 shows participant data preferences by generation.
Figure 3.
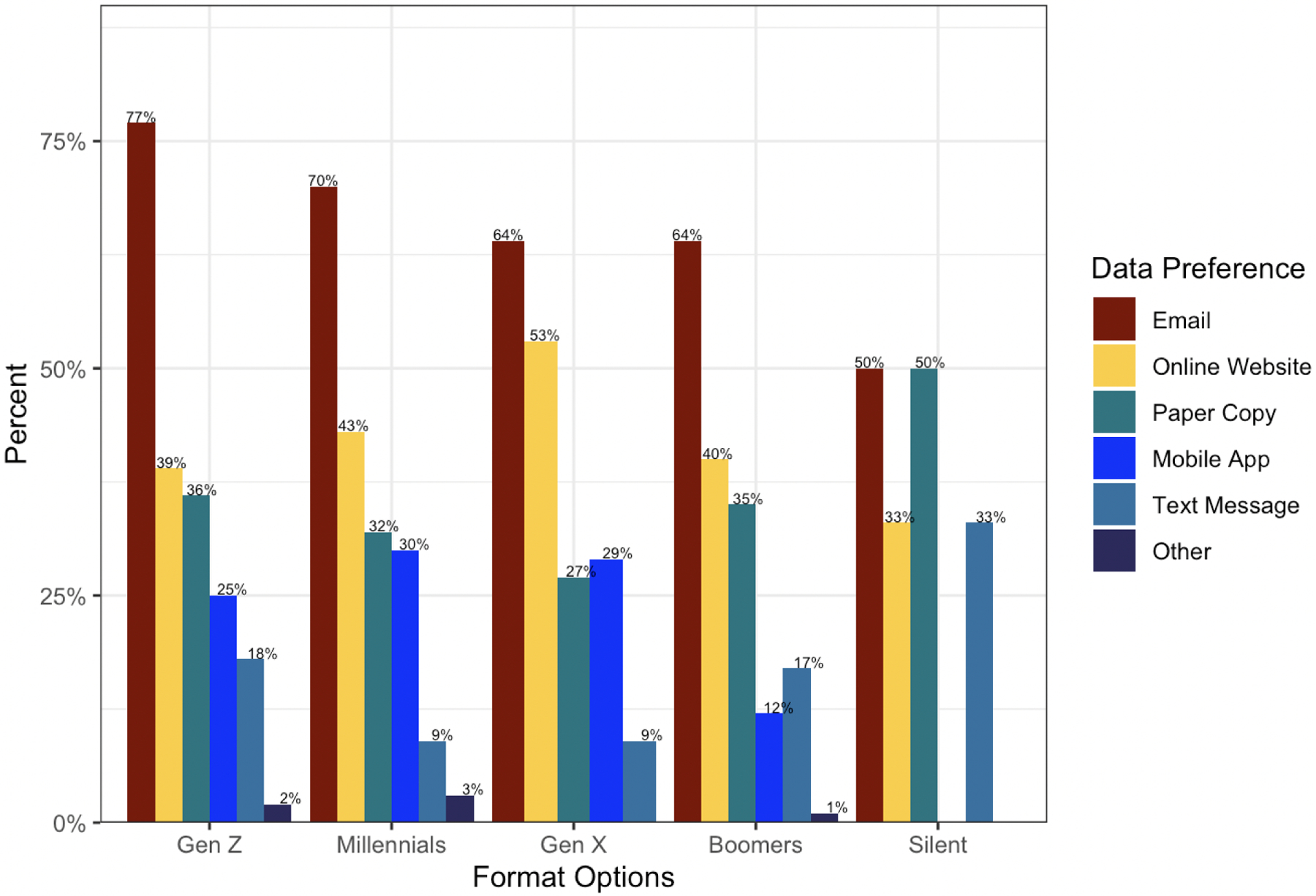
Distribution of format preferences by age generation. This figure shows the percentage of respondents who preferred each format, broken down by age. The percentages are based on responses to a ‘select all that apply’ question asking: How would you prefer to see the information that the researchers collect about you?.
There were also differences in format preference by education, health literacy, subjective numeracy, and financial resources (Figure 4). A higher proportion of participants without a college degree preferred to receive their health information through text message (19%) and paper copy (38%) compared to participants with a college degree or higher (text message: 8%, p < 0.001; paper copy: 27%, p = 0.013). A higher proportion of participants with inadequate health literacy preferred to receive their health information through an online website (52%) compared to those with adequate health literacy (41%, p = 0.034). A higher proportion of participants reporting insufficient financial resources (41%) preferred to receive a paper copy of their health information compared to those with more than enough (23%) and enough financial resources (30%, p = 0.015). Fewer participants with low subjective numeracy (13%) preferred to receive their health information through an online website, compared to those with medium (46%) and high subjective numeracy (47%, p < 0.001). There were no differences in format preferences by race, gender, or ethnicity.
Figure 4.
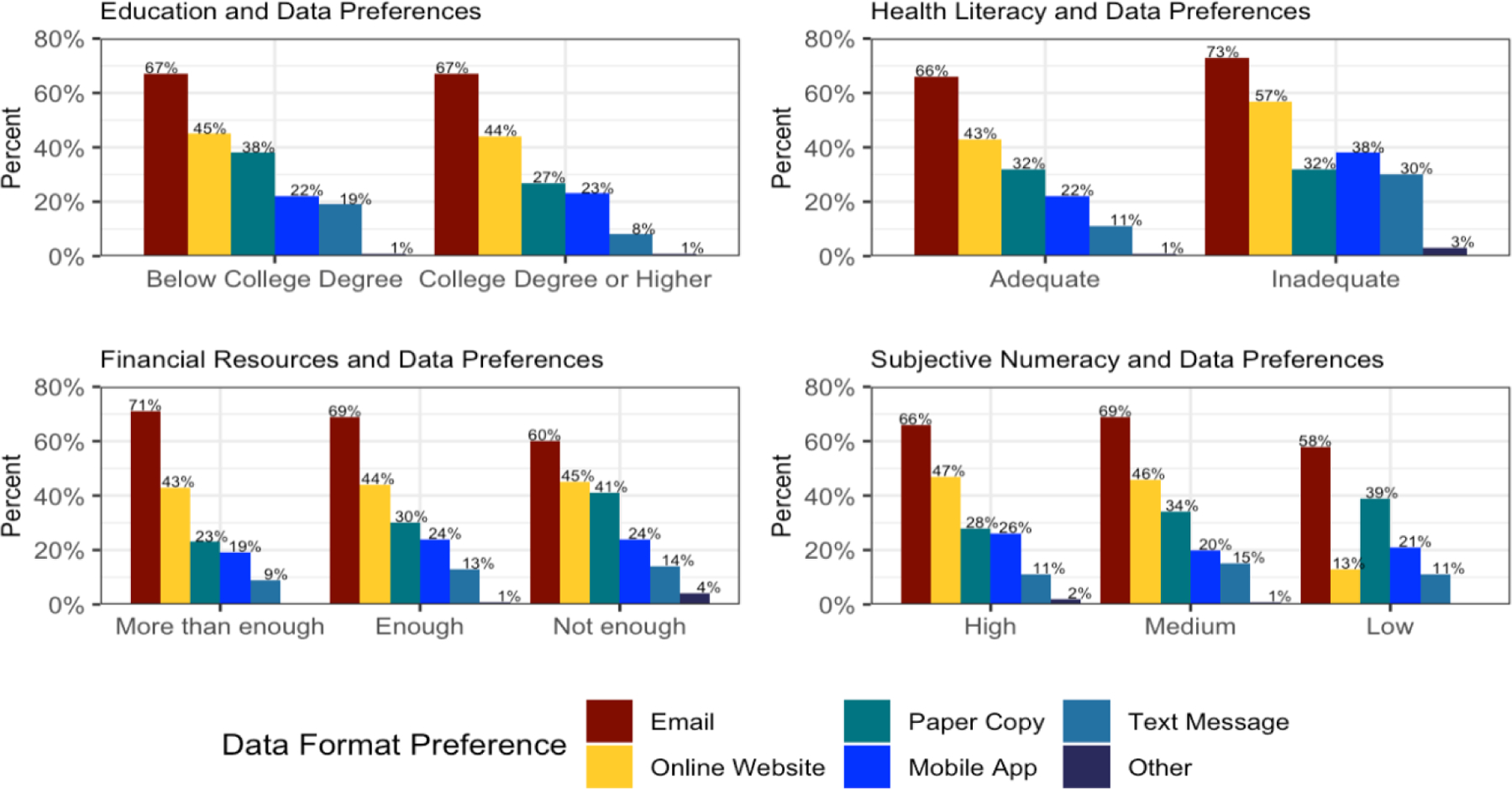
Differences in format preferences to receive collected health information by key sociodemographic characteristics
3.3. Actions with the Data
Most participants (81%) would use their returned health information for their own knowledge or to would use it to manage their health (70%). Less than half of the participants (42%) would share it with their doctors and nurses and less than a quarter would share it with chosen friends and family (20%).
3.4. Sharing Data
When asked how much of their collected health information they would share with stakeholder groups, 72% of respondents would share “all” of their health information with their doctors and nurses, 66% would share “some” of their information with chosen friends and family, and roughly half would share “some” of their health information with health policy makers (53%) and health tech companies (49%). About one-third of respondents would share “none” of their health information with health tech companies (36%) and health policy makers (30%) (Figure 5).
Figure 5.
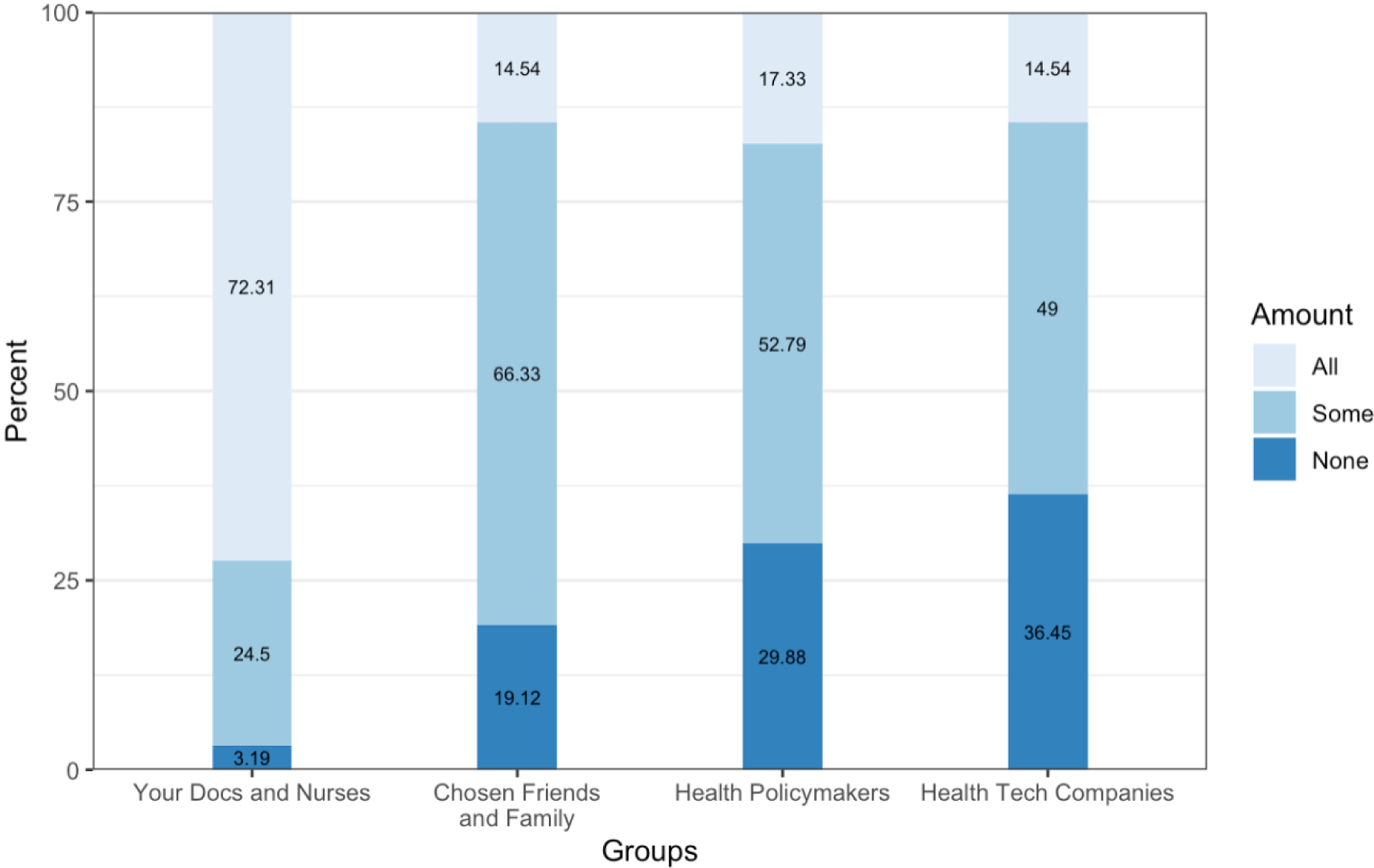
Amount of health information participants would share with stakeholder groups
3.5. Data Compensation
Most participants (72%) indicated that they should be paid for sharing their health information with health tech companies, 21% had no preference, and 8% indicated that they should not be paid.
3.6. Qualitative Data
For the qualitative analysis, the Cohen’s kappa score was 0.87, indicating excellent agreement. The top three reasons for wanting to have access to health information, (among the 84% who preferred their collected health information) were: 1) endorsement of an obligation of researchers to return health information to participants, 2) self-management and to use for own health, and 3) fact checking of the accuracy of the information researchers collected. Among participants who did not want access to their health information, most participants found that it would be too much information without benefit to them. Lastly, participants who had no preference to receive their health information: 1) would not know what to do with that information, 2) mentioned that it depends on the type of information collected, and 3) said that they would not mind if the researchers did not return the results, understanding that it may compromise the integrity of the study. A summary of responses and example quotes can be found in Table 2.
Table 2.
Open ended responses categorized by individual preferences for receiving health information
| Emergent theme or category N (%) | Description | Example responses | ||
|---|---|---|---|---|
| Participants who want access to health information (N = 425)* | ||||
| Personal right n = 189 (41%) | Participants saw having access to their collected health information as an obligation of researchers. This perspective asserted that having access to health information is a right because it is coming from them as the research participant. | “It is my right to see the information that is collected about my health” “If it deals with my body and my health, I should be able to know” |
||
| Personal knowledge and self-management n = 125 (27%) | Participants wanted their information to supplement their management of their health and use their information as a means of communication with clinicians if there were any concerning findings. | “The research findings could help me (or my doctors) better choose any necessary treatments or more finely tuned wellness plans” “That information could steer me to make better health choices, follow up on something that was not positive.” “I am my own health advocate. My information may not always be useful to me or my doctors, but sometimes it will be.” |
||
| Fact-checking and accountability n = 125 (27%) | Participants wanted access to their health information 1) as a means to verify the accuracy of the information that was collected about them, 2) to ensure that there was transparency from the researchers to offer access to their data, and 3) because transparency with researchers would increase their trust and willingness to participate in future research. | 1) “It is important to see any information that would be collected on a person’s behalf to make sure it is accurate” 2) “I think it is important that researchers are transparent about what information they are collecting” 3) “I should be able to see the information that the researchers collected about me because that will give me more confidence to trust in them” |
||
| No specified reason n = 17 (4%) | Some participants did not specify an explicit reason for wanting their health information returned to them. | “Yes, we should have that option” | ||
| Participants who do not want access to their health information (N = 4) | ||||
| Too much information or unnecessary concern | Few patients think that they might not understand their data returned to them, and that receiving their data would cause unnecessary concerns about their health. | “I wouldn’t necessarily have the context to understand what they collected and why. I wouldn’t want to cause myself unnecessary concern” | ||
| Participants who have no preference on receiving their health information (N = 73) | ||||
| Generally, no preference for receiving information or not n = 35 (48%) | Participants did not mind receiving their information, but it also did not matter to them if they did not receive it. | “It would be nice to see that information, but still fine if I’m not able to see it.” | ||
| Would not know what to do with information n = 15 (21%) | Participants had no preference on receiving their health information because they would not know what to do with their information. Sometimes, these participants expressed that it was not necessary to receive this information because they were already aware of their responses. | “I don’t think I’m knowledgeable enough to do anything with that information except make myself worry or something.” “I think I have a decent idea of what information they’re collecting based on what they ask me, so I don’t feel it’s necessary.” |
||
| Depends on the type of data n = 17 (23%) | Participants expressed that it depended on the type of research and the data collected for them to be interested in seeing their data. | “For some studies, I’d like to see the information but in others, I really couldn’t care less.” “Most surveys do not ask about things that I’d care about knowing or having records of. But, if there was a long-term study about fatigue or some other health issue that I would like to have recorded, then perhaps it would be helpful to see some sort of summary.” |
||
| To preserve integrity of the study n = 6 (8%) | Some participants believed receiving their health information could negatively affect the integrity of the study therefore were not sure if it was okay to receive it. | “In some cases, I could see how knowing what type of information the researchers are collecting about you could make you a biased subject in their study.” | ||
For participants who selected “yes”, some participants (n = 31, 7%) indicated responses with multiple categories, making the total overall N who responded ‘yes’ (N = 425) smaller than the total count of responses (N = 456). The percentages are calculated with 456 as the denominator.
4. DISCUSSION
These study findings provide insight for academic and applied consumer health informaticists on meeting research participant expectations for data access, format of data return, and data sharing preferences. In a representative US sample, the preferred formats for the return of research information were by email, online website, and paper copy. Compared with those with a college degree or higher, participants without a college degree were more likely to prefer text message and paper copy. Participants with low health literacy preferred mobile app or text message more than those with high health literacy, and participants with insufficient financial resources preferred paper copy more than those with enough financial resources. Participants wanted their research results returned for several reasons including increased transparency, accountability from researchers, and for self-management of health. In addition to using information for their own knowledge, many participants would share most of their information with their doctors and nurses, some information with friends and family, and little to no information with health tech companies and health policymakers.
Participants preferred email, online, and paper formats of information return, which echoes existing approaches involving participant preferences on the return of health information collected for research.31 Most existing studies that return health data to participants involve the return of genetic or lab result data that may be sensitive or have implications for personal or familial health.32 Various formats are in use to return health information, including an online platform plus paper copy to bring to clinical encounters,31 consultation with a genetic specialist to interpret findings,33 online platform alone21 and paper copy alone mailed to participants following the study.34 There is no current consensus on the optimal way to return health information to research participants in the US, but efforts are focused towards providing clarity, and are particularly driven by the unclear regulations on when and how to return genetic information to participants.35,36
Individual-level factors may play a role in what format research participants prefer to receive their information. While the most preferred format in our study was by email, patient-level factors, including education, subjective numeracy, health literacy, and financial resources were associated with differences in format preference from the majority. For instance, more individuals with inadequate health literacy preferred to receive their information via a mobile application or text message than those with adequate health literacy, and those with insufficient financial resources preferred a paper copy over those with enough and more than enough resources. This finding is consistent with current research about the impact of social determinants of health on engagement with healthcare and healthcare research.37–39
The format of information return can impact how research participants are able to obtain and interact with their own information. Prior qualitative work also found that research participants prefer to have an individualized choice on the format, content, and timing to receive research results and that participants should be considered stakeholders in the research design process.31 Our findings highlight the need for researchers to tailor the return of health information to the needs of the target population as not to extend inequities experienced by those with lower literacy, numeracy, and financial stability.
Most participants endorsed the return of health information from research studies, consistent with prior work.16 Participants would use this information to ensure its accuracy, for self-management, and to share with clinicians and select groups. There is also an ethical responsibility to return health information, particularly when research results may be concerning, abnormal, or diagnostic.33,40 In addition to the ethical expectation for researchers to return information, participants also wanted to verify that their health information was collected and portrayed accurately.
Participants’ preferences for how much information they would share with different groups varied (e.g., most would share all information with clinicians, but only some information with chosen family and friends). Currently, existing policies such as OpenNotes and the 21st Century Cures Act promote access to health information but do not address how users can verify the accuracy of information or control the type or amount of information shared.9,11 This is important for future consideration, as adding patients as collaborators in sharing clinical notes and health information have been shown to be preferred by patients and improve accuracy.41,42 Notably, most participants preferred to have agency with the amount of information shared to different groups.43,44 Researchers should consider these nuanced preferences to control the amount of information shared and the expectation for transparency when designing research studies that involve the return of collected health information.
Over a quarter of participants did not want any of their health information shared with health tech companies or health policymakers. This finding is consistent with widespread reticence to share and commercialize data, which is driven by a lack of transparency and trust in large corporations and organizations.45 The Sync for Science initiative demonstrates an early attempt in the US to operationalize data sharing in research, which grants individuals the ability to authorize electronic health record information sharing to researchers through third-party applications.46 Sync for Science shared pilot testing results in 2020, demonstrating willingness for interoperability between multiple key stakeholders; however, little is known about patients’ experiences.46
We also found that over 70% of participants would like to be compensated for sharing their information with health tech companies. Mechanisms for compensation are in development in other countries such as through the digital services tax in Canada, where profits are cycled back to users for using services and sharing data with large corporations.47 Our findings reinforce the need for more engagement and compensation from large organizations and companies as a way to increase willingness to share data. Transparency with information and intent and providing participants with control over where their information is going, are some approaches to addressing this issue, but more work is needed.
4.1. Limitations
We acknowledge the limitations of using an online research platform to collect data about preferences on research. The participants in this study may represent the opinions of individuals who are receptive to research and have participated in research in the past. Our results are intended to be a first step toward understanding data access, format, and sharing preferences among research study participants. The high preference toward receiving research information back through an online platform or email could be explained by our use of an online platform to conduct the study. Nonetheless, there were a range of participants that preferred an additional paper copy of their health information, and access through text message or mobile apps. Moreover, our survey was limited to English-speaking individuals with higher levels of health literacy, graph literacy, and subjective numeracy than the public. We also acknowledge limitations in the representation of the population through select categorizations for sociodemographic characteristics. Further, due to our limitations in representing socioeconomic status and having a sample that is familiar with research and use of technology, further efforts should be taken in research recruitment to obtain perspectives from diverse groups to minimize bias.
5. CONCLUSION
Overall, participants want their collected research information returned to them to manage their own health conditions, to ensure researcher accountability, and to ensure their information is accurate. Participants overall prefer to receive their information back through email, online website, and paper copy. Moreover, sociodemographic characteristics drove differences in format preferences. Future research should further explore factors that drive participant preferences for receiving and sharing research information, including type of data collected and combinations of individual sociodemographic characteristics.
Summary Table.
| What was already known on the topic | What this study added to our knowledge |
|---|---|
|
|
Highlights.
Respondents want their data back through combinations of email, website, and paper.
Format preferences for data vary by age, education, numeracy, and health literacy.
Respondents see access to their personal data as a right and expectation.
Respondents want to use their data for their own reference or to manage health.
Funding Statement
This work was supported by the National Institute of Nursing Research, Grant number R00NR016275-05S1, PI: Masterson Creber; T32NR016913, PIs: Heitkemper, Thompson
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest Statement
MRT has the following conflicts to disclose: Boston Scientific Corp. (consulting); Iris OB Health Inc. (equity ownership).
CrediT Author Statement
Mangal S.: Conceptualization, Methodology, Investigation, Writing – Original draft, Writing – Review and editing, Visualization; Niño de Rivera S.: Writing – Original draft, Writing – Review and editing, Visualization; Choi J.: Methodology, Formal Analysis, Data Curation, Writing – Review and editing, Visualization; Reading Turchioe M.: Conceptualization, Methodology, Investigation, Writing – Original draft, Writing – Review and editing, Visualization; Benda N.: Writing – Review and editing; Sharko M.: Writing – Review and editing; Myers A.: Writing – Review and editing; Goyal P.: Writing – Review and editing; Dugdale L.: Writing – Review and editing; Masterson Creber R.: Conceptualization, Methodology, Investigation, Writing – Original draft, Writing – Review and editing, Supervision, Project administration, Funding acquisition
REFERENCES
- 1.Kao CK, Liebovitz DM. Consumer Mobile Health Apps: Current State, Barriers, and Future Directions. PM R. 2017;9(5S):S106–S115. [DOI] [PubMed] [Google Scholar]
- 2.McElfish PA, Purvis RS, Long CR. Researchers’ experiences with and perceptions of returning results to participants: Study protocol. Contemp Clin Trials Commun. 2018;11:95–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Health Sciences Policy, et al. Advancing Practices for Returning Individual Research Results. National Academies Press (US); 2018. [PubMed] [Google Scholar]
- 4.Hulsen T Sharing Is Caring-Data Sharing Initiatives in Healthcare. Int J Environ Res Public Health. 2020;17(9). doi: 10.3390/ijerph17093046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Seltzer E, Goldshear J, Guntuku SC, et al. Patients’ willingness to share digital health and non-health data for research: a cross-sectional study. BMC Med Inform Decis Mak. 2019;19(1):157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.General Data Protection Regulation (GDPR) – Official Legal Text. General Data Protection Regulation (GDPR). Published July 13, 2016. Accessed March 30, 2022. https://gdpr-info.eu/
- 7.Staunton C, Slokenberga S, Mascalzoni D. The GDPR and the research exemption: considerations on the necessary safeguards for research biobanks. Eur J Hum Genet. 2019;27(8):1159–1167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Office of the Privacy Commissioner of Canada. PIPEDA in brief. Accessed April 18, 2022. https://www.priv.gc.ca/en/privacy-topics/privacy-laws-in-canada/the-personal-information-protection-and-electronic-documents-act-pipeda/pipeda_brief/
- 9.Federal Rules Mandating Open Notes. Accessed May 11, 2022. https://www.opennotes.org/onc-federal-rule/
- 10.Health Information Privacy Division. Individuals’ Right under HIPAA to Access their Health Information. Accessed April 5, 2022. https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/access/index.html
- 11.ONC’s Cures Act Final Rule. Accessed April 18, 2022. https://www.healthit.gov/curesrule/
- 12.Information Blocking. Accessed April 18, 2022. https://www.healthit.gov/topic/information-blocking
- 13.Committee on Strategies for Responsible Sharing of Clinical Trial Data, Board on Health Sciences Policy, Institute of Medicine. Guiding Principles for Sharing Clinical Trial Data. National Academies Press (US); 2015. [PubMed] [Google Scholar]
- 14.Keerie C, Tuck C, Milne G, Eldridge S, Wright N, Lewis SC. Data sharing in clinical trials - practical guidance on anonymising trial datasets. Trials. 2018;19(1):25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Long CR, Stewart MK, Cunningham TV, Warmack TS, McElfish PA. Health research participants’ preferences for receiving research results. Clin Trials. 2016;13(6):582–591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sayeed S, Califf R, Green R, et al. Return of individual research results: What do participants prefer and expect? PLoS One. 2021;16(7):e0254153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wilkins CH, Mapes BM, Jerome RN, Villalta-Gil V, Pulley JM, Harris PA. Understanding What Information Is Valued By Research Participants, And Why. Health Aff. 2019;38(3):399–407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wong CA, Hernandez AF, Califf RM. Return of Research Results to Study Participants: Uncharted and Untested. JAMA. 2018;320(5):435–436. [DOI] [PubMed] [Google Scholar]
- 19.Roberts JS, Shalowitz DI, Christensen KD, et al. Returning individual research results: development of a cancer genetics education and risk communication protocol. J Empir Res Hum Res Ethics. 2010;5(3):17–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gaieski JB, Patrick-Miller L, Egleston BL, et al. Research participants’ experiences with return of genetic research results and preferences for web-based alternatives. Mol Genet Genomic Med. 2019;7(9):e898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.All of Us Research Program Investigators, Denny JC, Rutter JL, et al. The “All of Us” Research Program. N Engl J Med. 2019;381(7):668–676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Haddock G, Foad C, Saul V, Brown W, Thompson R. The medium can influence the message: Print-based versus digital reading influences how people process different types of written information. Br J Psychol. 2020;111(3):443–459. [DOI] [PubMed] [Google Scholar]
- 23.Luo Y, Oh CY, Jean BS, Choe EK. Interrelationships Between Patients’ Data Tracking Practices, Data Sharing Practices, and Health Literacy: Onsite Survey Study. J Med Internet Res. 2020;22(12):e18937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nebeker C, Leow AD, Moore RC. From Return of Information to Return of Value: Ethical Considerations when Sharing Individual-Level Research Data. J Alzheimers Dis. 2019;71(4):1081–1088. [DOI] [PubMed] [Google Scholar]
- 25.Prolific. Accessed December 13, 2021. https://www.prolific.co/
- 26.Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with inadequate health literacy. Fam Med. 2004;36(8):588–594. [PubMed] [Google Scholar]
- 27.McNaughton CD, Cavanaugh KL, Kripalani S, Rothman RL, Wallston KA. Validation of a Short, 3-Item Version of the Subjective Numeracy Scale. Med Decis Making. 2015;35(8):932–936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Okan Y, Janssen E, Galesic M, Waters EA. Using the Short Graph Literacy Scale to Predict Precursors of Health Behavior Change. Med Decis Making. 2019;39(3):183–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Defining generations: Where Millennials end and Generation Z begins. Published January 17, 2019. Accessed December 13, 2021. https://www.pewresearch.org/fact-tank/2019/01/17/where-millennials-end-and-generation-z-begins/
- 30.O’Connor C, Joffe H. Intercoder Reliability in Qualitative Research: Debates and Practical Guidelines. International Journal of Qualitative Methods. 2020;19:1609406919899220. [Google Scholar]
- 31.Cook S, Mayers S, Goggins K, et al. Assessing research participant preferences for receiving study results. J Clin Transl Sci. 2019;4(3):243–249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Christensen KD, Savage SK, Huntington NL, et al. Preferences for the Return of Individual Results From Research on Pediatric Biobank Samples. J Empir Res Hum Res Ethics. 2017;12(2):97–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bradbury AR, Patrick-Miller L, Egleston BL, et al. Returning Individual Genetic Research Results to Research Participants: Uptake and Outcomes Among Patients With Breast Cancer. JCO Precis Oncol. 2018;2. doi: 10.1200/po.17.00250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bonilla J, Alhomsi A, Santoyo-Olsson J, et al. Sharing research results with Latina breast cancer survivors who participated in a community-engaged behavioral RCT study: a descriptive cross-sectional survey study. Trials. 2022;23(1):25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Health Sciences Policy, Committee on the Return of Individual-Specific Research Results Generated in Research Laboratories. Returning Individual Research Results to Participants: Guidance for a New Research Paradigm. National Academies Press; 2018. [PubMed] [Google Scholar]
- 36.Return of Research Results. Genome.gov. Accessed May 11, 2022. https://www.genome.gov/about-genomics/policy-issues/Human-Subjects-Research-in-Genomics/Return-of-Research-Results
- 37.Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband Internet Access Is a Social Determinant of Health! Am J Public Health. 2020;110(8):1123–1125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Jackson CS, Gracia JN. Addressing health and health-care disparities: the role of a diverse workforce and the social determinants of health. Public Health Rep. 2014;129 Suppl 2:57–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Nutbeam D, Lloyd JE. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu Rev Public Health. 2021;42:159–173. [DOI] [PubMed] [Google Scholar]
- 40.Lewis KL, Turbitt E, Chan PA, et al. Engagement and return of results preferences among a primarily African American genomic sequencing research cohort. Am J Hum Genet. 2021;108(5):894–902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Blease CR, Bell SK. Patients as diagnostic collaborators: sharing visit notes to promote accuracy and safety. Diagnosis (Berl). 2019;6(3):213–221. [DOI] [PubMed] [Google Scholar]
- 42.Bell SK, Mejilla R, Anselmo M, et al. When doctors share visit notes with patients: a study of patient and doctor perceptions of documentation errors, safety opportunities and the patient-doctor relationship. BMJ Qual Saf. 2017;26(4):262–270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Grande D, Mitra N, Shah A, Wan F, Asch DA. The importance of purpose: moving beyond consent in the societal use of personal health information. Ann Intern Med. 2014;161(12):855–862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Grande D, Asch DA, Wan F, Bradbury AR, Jagsi R, Mitra N. Are Patients With Cancer Less Willing to Share Their Health Information? Privacy, Sensitivity, and Social Purpose. J Oncol Pract. 2015;11(5):378–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Esmaeilzadeh P The Impacts of the Perceived Transparency of Privacy Policies and Trust in Providers for Building Trust in Health Information Exchange: Empirical Study. JMIR Med Inform. 2019;7(4):e14050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sync for Science. Accessed May 10, 2022. https://www.healthit.gov/topic/sync-science
- 47.Ljunggren D Canada plans digital tax in 2022 on global tech giants such as Facebook, Google. Reuters. https://www.reuters.com/article/us-canada-budget-tax-idUSKBN28A2ZM. Published November 30, 2020. Accessed December 23, 2021.