

Abstract
BACKGROUND
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants has become a major concern contributing to increased morbidity and mortality worldwide.
OBJECTIVES
Here we describe the replacement of the Gamma variant of concern (VOC) with Delta in the western Brazilian Amazon.
METHODS
In this study, we analysed 540 SARS-CoV-2 positive samples determined by qualitative real-time RT-PCR selected in the state of Rondônia between June and December 2021. The positive cohort was sequenced through next-generation sequencing (NGS) and each sample was quantified using real-time RT-qPCR, the whole genome sequence was obtained, SARS-CoV-2 lineages were classified using the system Pango and the maximum likelihood (ML) method was used to conduct phylogenetic analyses.
FINDINGS
A total of 540 high-quality genomes were obtained, where the Delta VOC showed the highest prevalence making up 72%, with strain AY.43 being the most abundant, while the Gamma VOC was present in 28%, where the P.1 strain was the most frequent. In this study population, only 32.96% (178/540) had completed the vaccination schedule.
MAIN CONCLUSIONS
This study highlighted the presence of Gamma and Delta variants of SARS-CoV-2 in RO. Furthermore, we observed the replacement of the Gamma VOC with the Delta VOC and its lineages.
Key words: SARS CoV-2, variant of concern, Gamma, Delta, genomic surveillance
Coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and remains a worldwide concern nearly 2 years after a pandemic was declared. 1 This virus presents a high rate of transmissibility, thus acquiring many mutations that favour the emergence of variants of concern (VOC), which in turn may be characterised by increased infectivity and/or the potential for immune evasion, especially that of neutralising anti-SARS-CoV-2 antibodies. The Gamma (P.1), Delta (B.1.617.2 and AY.*), Alpha (B.1.1.7 and Q.*), Beta (B.1.351) and, recently, Omicron (B.1.1.529 and BA.*) VOCs have shown the highest impact on public health to date. 2
The Gamma VOC was detected in December 2020 in northern Brazil, more precisely in Manaus, which has been identified as the beginning of the second wave of COVID-19 in the country. 3 The Delta VOC was first described in India, in October 2020, and was identified in April 2021 when the first case occurred in southern Brazil, linked to a person who had travelled to Asia. 4 , 5 ) Since then, the high rate of transmissibility of these variants has permitted the appearance of new sublineages, which is a phenomenon that is an integral part of viral evolution. 6 - 8
As has happened in other countries, the North Region of Brazil has shown a high incidence and cumulative mortality rate since these VOCs were originally detected. The state of Rondônia (RO) presented the highest mortality rate in the region, according to the Ministry of Health, which highlights the importance of implementing genomic surveillance. 9 The objective of this study was to describe the profile of SARS-CoV-2 variants in the western Brazilian Amazon region between June and December 2021.
MATERIALS AND METHODS
Ethical aspects and study site - This study was conducted at Fiocruz/RO, under the authorisation of the FIOCRUZ COVID-19 Genomics Surveillance Network of the Brazilian Ministry of Health and was approved by the Research Ethics Committee of the Centro de Pesquisa em Medicina Tropical de Rondônia (protocol 4.000.086). All experiments were performed in accordance with relevant guidelines and regulations and was exempted from informed consent requirements owing to its retrospective design.
Biological samples and epidemiological data - SARS-CoV-2 positive individuals were conveniently sampled in primary health units and reference centres in different municipalities of RO. Laboratory diagnosis was performed by RT-qPCR at Laboratório Central de Saúde Pública de Rondônia (LACEN/RO) using the One Step/COVID-19 Kit [Instituto de Biologia Molecular do Paraná (IBMP), Curitiba, Brazil], and a total of 540 samples with cycle threshold (Ct) values < 25 for the viral target were selected for the study. Epidemiological data and vaccination status were collected from medical records in Gerenciador de Ambiente Laboratorial (GAL/RO), Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe) and E-SUS databases.
Complete genome sequencing of SARS-CoV-2 - Complete genome sequencing of SARS-CoV-2 samples with Ct values < 25, based on qualitative assays, were selected to allow for high genomic coverage. Nucleotide sequencing was performed using Illumina MiSeq or NextSeq platforms and the COVIDSEQ Kit (Illumina, San Diego, USA). 10
Data acquisition and maximum likelihood (ML) phylogeny - High-quality (< 1% of N) complete genomes (> 29 kb) of SARS-CoV-2 (n = 544, corresponding to two representatives for each states of Brazil and lineage found) were retrieved from the GISAID EpiCoV database 11 on December 22, 2021 and the sequences were aligned using MAFFT v.7.487. 12 The ML method was adopted using IQ-TREE v.2.1.3 13 and the best-fitting nucleotide substitution model was GTR+G+I using the ModelFinder tool. 14 Ultrafast bootstrap with 1,000 replicates was used to obtain branch support values. The tree was visualised and edited with FigTree v.1.4.4. 15 SARS-CoV-2 genomes were classified into lineages using the available software Pangolin 7 and mutations were analysed with Nextclade Beta. 16
Nucleic acid isolation and RT-qPCR - Sample quantification was performed in the Laboratório de Virologia Molecular (Fiocruz/RO) where viral RNA was extracted from 140 µL of pooled swab samples using a QIAamp® Viral RNA Mini Kit (QIAGEN, Hilden, Germany), according to the manufacturer’s instructions. Viral load was determined using 5 μL of this extracted viral RNA using the Multiplex One-Step RT-qPCR assay for detection of SARS-CoV-2, as developed by Queiroz et al. 17
Statistical analysis - Descriptive analyses were represented through central tendency and dispersion measurements. The chi-square test was used for statistical inference with a significance level of 5% (p < 0.05). Statistical analysis was performed and graphics were generated using the software R v4.0.3.
RESULTS
A total of 540 samples from 36 municipalities in RO were selected and sequenced (< 1% N, or nucleotides not identified). The Delta variant was prevalent, accounting for 72% (390/540) of the characterised sequences, while the Gamma variant was found in 28% (150/540) of cases (Fig. 1).
Fig. 1: temporal substitution of the Gamma variant of concern (VOC) for the Delta VOC from July to December 2021 in municipalities of the state of Rondônia. A) July: absence of Delta VOC detection; B) August-September: insertion of the Delta VOC followed by reduction of the Gamma VOC; C) October-November: increase in the Delta VOC, indicating the overlap profile in relation to the Gamma VOC; D) December: only Delta VOC was detected. Brazilian states: Acre (AC), Amazonas (AM), Pará (PA), Mato Grosso (MT).
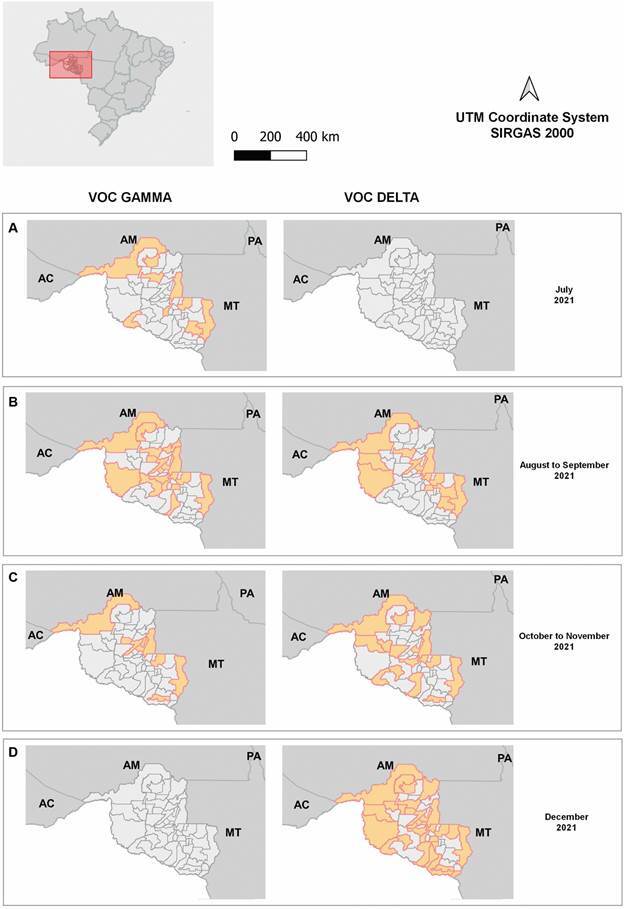
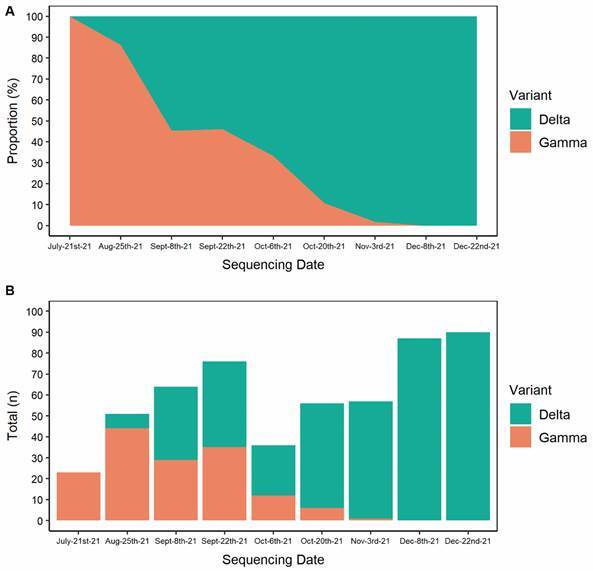
Fig. 2 represents the temporal dynamics of infections for the identified variants, where it is possible to observe the increase in the proportion of the Delta variant in relation to Gamma.
Fig. 2: area plot (A) and bar plot (B) representing the relative and absolute proportion of the Gamma and Delta variants of concern (VOCs) over time, respectively.
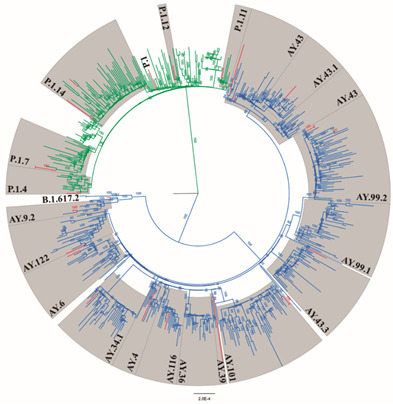
The ML phylogeny regarding the classification and distribution of the major clades of Delta and Gamma variants is shown in Fig. 3. In addition to the parent variant B.1.617.2 (45/390), other Delta lineages were found, the most prevalent being AY.43 (179/390), followed by AY.99.2 (139/390), AY.9.2 (10/390), AY.101 (4/390), AY.4 (3/390), AY.122 (2/390), AY.6 (1/390), AY.34.1.1 (1/390), AY.36 (1/390), AY.39 (1/390), AY.43.1 (1/390), AY.46.3 (1/390), AY.99.1 (1/390) and AY.116 (1/390). Among the Gamma variants, the P.1 line of origin was most frequently encountered (78/150), followed by the subvariants P.1.4 (41/150), P.1.7 (21/150), P.1.14 (8/150), P.1.11 (1/150) and P.1.12 (1/150).
Fig. 3: maximum likelihood phylogenetic tree including representatives isolated from the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Delta and Gamma variant study and 544 full genome sequences retrieved from GISAID. Samples are in the red branches. Delta and Gamma variants are in blue and green clades, respectively. Bootstrap values are in the branches.
Individuals infected with the Delta VOC showed a median age of 37 years old [standard deviation (SD) 16.96], with ages ranging from 6 to 86 years old and 51% (200/390) were female while 49% (190/390) were male. The Gamma VOC population showed a median age of 34 years old (SD 18.6), ranging from 7 to 90 years old, and 56% (84/150) were female while 44% (66/150) were male.
In this cohort, 32.96% (178/540) were considered to be fully vaccinated (at least 15 days after the second or third dose of the vaccine at the time of sample collection), 41.66% (225/540) were partially immunised (at least 15 days after the first dose of the vaccine at the time of sample collection), and 25.37% (137/540) were unvaccinated (Table). The complete immunisation rate among individuals over 50 years of age was 46.62% (83/178), 39.88% (71/178) among individuals aged 30-50 years and 13.48% (24/178) in individuals under 30 years of age.
TABLE. Distribution of identified lineages in relation to the immunisation profile of the study population.
| Variant | Lineage | Complete immunisation (n = 178) | % | Partial immunisation (n = 225) | % | No immunisation (n = 137) | % | Total (n = 540) |
| Delta (n = 390) | B.1.617.2 | 9 | 5.1 | 24 | 10.7 | 12 | 8.8 | 45 |
| AY.4 | 1 | 0.6 | 2 | 0.9 | 0 | 0.0 | 3 | |
| AY.6 | 0 | 0.0 | 0 | 0.0 | 1 | 0.7 | 1 | |
| AY.9.2 | 6 | 3.4 | 2 | 0.9 | 2 | 1.5 | 10 | |
| AY.34.1.1 | 1 | 0.6 | 0 | 0.0 | 0 | 0.0 | 1 | |
| AY.36 | 0 | 0.0 | 0 | 0.0 | 1 | 0.7 | 1 | |
| AY.39 | 0 | 0.0 | 0 | 0.0 | 1 | 0.7 | 1 | |
| AY.43 | 59 | 33.1 | 75 | 33.3 | 45 | 32.8 | 179 | |
| AY.43.1 | 0 | 0.0 | 1 | 0.4 | 0 | 0.0 | 1 | |
| AY.46.3 | 1 | 0.6 | 0 | 0.0 | 0 | 0.0 | 1 | |
| AY.99.1 | 1 | 0.6 | 0 | 0.0 | 0 | 0.0 | 1 | |
| AY.99.2 | 74 | 41.6 | 36 | 16.0 | 29 | 21.2 | 139 | |
| AY.101 | 0 | 0.0 | 1 | 0.4 | 3 | 2.2 | 4 | |
| AY.116 | 0 | 0.0 | 1 | 0.4 | 0 | 0.0 | 1 | |
| AY.122 | 0 | 0.0 | 0 | 0.0 | 2 | 1.5 | 2 | |
| Gamma (n = 150) | P.1 | 11 | 6.2 | 42 | 18.7 | 25 | 18.2 | 78 |
| P.1.4 | 6 | 3.4 | 25 | 11.1 | 10 | 7.3 | 41 | |
| P.1.7 | 5 | 2.8 | 12 | 5.3 | 4 | 2.9 | 21 | |
| P.1.11 | 0 | 0.0 | 1 | 0.4 | 0 | 0.0 | 1 | |
| P.1.12 | 0 | 0.0 | 0 | 0.0 | 1 | 0.7 | 1 | |
| P.1.14 | 4 | 2.2 | 3 | 1.3 | 1 | 0.7 | 8 | |
| Hospitalisation (n = 5) | B.1.617.2 | 0 | 0.0 | 1 | 0.5 | 0 | 0.0 | 1 |
| P.1 | 0 | 0.0 | 1 | 0.5 | 0 | 0.0 | 1 | |
| P.1.4 | 1 | 1.0 | 0 | 0.0 | 2 | 1.7 | 3 | |
| Death (n = 4) | AY.43 | 0 | 0.6 | 1 | 0.0 | 0 | 0.0 | 1 |
| P.1 | 0 | 0.0 | 2 | 1.0 | 1 | 0.8 | 3 |
Percentage of Delta (AY.*+B.1.617.2) and Gamma (P.1.*+P.1) strains identified in relation to the immunisation profile of the study population. Individuals were classified into three distinct groups: complete immunisation (after receiving the second or third dose of the vaccine), partial immunisation (after receiving the first dose of the vaccine) or no immunisation.
Among the nine hospitalised individuals, two children under 10 years of age (7 and 8 years old) were not vaccinated and did not present comorbidities, one of whom evolved to death.
The other three individuals that died were elderly, partially immunised and presented comorbidities. There were no recorded deaths among fully immunised individuals.
The symptoms were similar in the two groups, with 61% (329/540) of individuals presenting cough, 54% (297/540) fever, 54% (299/540) headache, 36% (196/540) sore throat and 35% (190/540) runny nose. The least frequently reported symptoms among the individuals were 18% (98/540) presenting olfactory disorders, 16% (86/540) reporting taste disorders and 12% exhibiting (63/540) dyspnoea; 2% (10/540) of patients were asymptomatic.
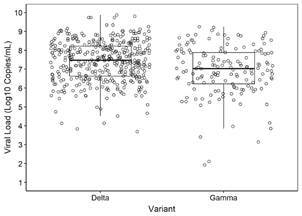
We observed no difference regarding the viral load when individuals with Gamma or Delta infections were compared; an interquartile median of 7.47 Log10 copies/mL (min:3.68 max:9.87) for the Delta VOC and 7.03 Log10 copies/mL (min:1.92 max:9.24) for the Gamma VOC (Fig. 4).
Fig. 4: viral load profile of samples characterised as positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Delta or Gamma variants based on RT-qPCR.
DISCUSSION
In this study, we analysed socio-demographic data, viral load and SARS-CoV-2 circulating lineages in the second half of 2021 in RO, located in the northern region of Brazil. Our analyses revealed that the Gamma VOC and its subvariants were predominant between July and August 2021, the period preceding the entry of the Delta VOC and its subvariants.
The Gamma VOC was responsible for rapidly spreading waves of infections in Brazil, making it the most prevalent variant from January through August 2021, 18 , 19 possibly justified by its high transmissibility and partial immune evasion, as shown by reinfection cases. 20 However, this scenario changed after the introduction of the Delta VOC with the first confirmed case in RO on August 3, 2021, leading to a gradual increase in cases as described in this study. The incidence of SARS-CoV-2 in the state decreased between June and October, from 237.8 to 22.8 cases per 100,000 inhabitants; however, in November and December, there was a significant increase where the incidence rates recorded were 80.7 and 126.7, respectively, with the highest numbers in relation to the other states in the northern region of the country. 9 , 21 - 27
Published data demonstrate rapid growth and dissemination of this variant on a global scale, 28 - 31 being about two times more transmissible than the original Wuhan SARS-CoV-2 strain. 32 - 34 Furthermore, a comparative study suggests a clear competitive advantage of the Delta variant over the Alpha, Beta and Gamma variants, showing an estimated increase in the number of effective replications by about 55, 60 and 34%, respectively. 33
Mutations in the viral genome allowed for the emergence of sublineages relative to the original strain. The Delta subvariant AY.99.2 was predominant in Brazil between August and December 2021 35 ; however, in this study a higher prevalence of AY.43 was observed during the same period. Studies have shown that the posterior division of this lineage into AY.43.1 and AY.43.2 originated in Brazil. 36 In addition, the subvariants AY.4.2 and AY.1, also described as “Delta plus”, both associated with an increased number of Delta cases in several countries, were not detected. 37 Regarding the Gamma lineage, we observed a higher proportion of P.1.4 than P.1.7, different from previously published data in the country, which show a higher prevalence of P.1.7 compared to P.1.4. 10 The subvariant profile was different than that of the state of Amazonas, where besides P.1.4, there was also a predominance in the P.1.3 and P.1.6 lineages during this same time period; both states are located in the northern region of the country. 10
On the other hand, vaccination in children between 5 and 11 years of age has been widely recommended by health agencies 38 , 39 and has been demonstrated to be safe, immunogenic and effective against COVID-19. 40 We report two cases of children in this age group, who were not vaccinated, required hospitalisation and one of whom died.
Infection of fully vaccinated individuals is a reality in COVID-19, mainly due to the emergence of new variants and mutations that may favour immune escape. 41 - 44 Even with the possibility of infection after vaccination, vaccinated individuals are less likely to develop the severe form of the disease or die. 43 Furthermore, due to the emergence of new variants, booster doses of immunisations are essential as a measure to protect against and combat the disease. 45 - 47 In our study, the three adults who died were not fully vaccinated.
During June and December 2021, RO went from having 7.2 to 55.2% of the population fully immunised, and 12.6 to 67.7% of the population being partially immunised. 48 ) However, the profile of the study population demonstrated a low immunisation rate of individuals aged around 30 years old, which may reflect hesitancy towards vaccination, previously observed in the working-age population in other countries, 49 , 50 as well as in Brazil. 41
Infection of fully vaccinated individuals is a reality in COVID-19, mainly due to the emergence of new variants and mutations that may favour immune escape. 43 , 44 , 51 , 52 Even with the possibility of infection after vaccination, vaccinated individuals are less likely to develop severe disease or die. 53 In this population, only one death was observed, whose individual had only one dose of the vaccine, besides advanced age and comorbidities, not being reported cases of death in fully vaccinated individuals.
Most patients had the same triad of symptoms, including cough, fever, headache, supporting studies that report no divergent aspects of symptoms with the progressive introduction of new strains and VOCs in other countries. 54 , 55 Olfactory and gustatory disturbances were observed at the start of the pandemic as the most frequent symptoms; however, in our study, these symptoms were not frequent. 56
The constant emergence of new variants suggests the need to maintain preventive measures, such as the use of adequate masks, prioritisation of professional and educational activities, as well as avoiding unnecessary social agglomerations, in order to reduce the probability of SARS-CoV-2 evolution; we encourage vaccination, since severe cases were not seen in fully vaccinated patients within the two VOCs analysed. 48 , 49
In conclusion, this study showed the replacement of the Gamma VOC with Delta and its sublineages in RO, western Brazilian Amazon, and analysed both socio-demographic and laboratorial data that may have contributed to this phenomenon. Our study further emphasises the importance of local genomic surveillance in large countries like Brazil.
Data availability - All the SARS-CoV-2 genomes generated and analysed in this study are available in the EpiCov database in GISAID under the following ID numbers: EPI_ISL_11112665-11112674, EPI_ISL_5030021, EPI_ISL_6575689-6575706, EPI_ISL_6575708, EPI_ISL_6575710-6575739, EPI_ISL_8623163-8623164, EPI_ISL_8623166-8623256, EPI_ISL_8623258-8623269, EPI_ISL_9414682-9414748, EPI_ISL_9414750-9414760, EPI_ISL_9414773-9414774, EPI_ISL_9636798-9636802 and EPI_ISL_9636805-9636877.
The list of accession IDs may be found in the attached file in the Supplementary data (157.9KB, pdf) .
ACKNOWLEDGEMENTS
The present study was developed by a group of researchers from Laboratório de Virologia Molecular, Fiocruz/RO, with financial support from the Genomic Coronavirus Fiocruz Network, Departamento de Ciência e Tecnologia (DECIT), Fundação para o Desenvolvimento das Ações Científicas e Tecnológicas da Pesquisa do Estado de Rondônia (FAPERO), Programa de Pesquisa para o SUS (PPSUS), as well as Instituto Nacional de Ciência e Tecnologia de Epidemiologia da Amazônia Ocidental (INCT-EpiAmo), important contributors to scientific development in the Amazon region, Coordenação de Aperfeiçoamento Pessoal de Nível Superior (CAPES), from which some authors received financial aid (scholarships) during the production of this study, the vice president of Vigilância em Saúde and Laboratórios de Referências of Fiocruz, IBMP and LACEN/RO, essential for the development of the study, US/CDC and OPAS, Brazilian office. FGN is a CNPq fellow. The authors declare no conflict of interest.
Footnotes
Financial support: FIOCRUZ/RO (PROEP 2021 process: VPGDI-008-FIO-21-2-17), DECIT, FAPERO (process: 01133100038-0000.72/2016; Public bid invitation: 012/2016 PRO-RONDÔNIA, PPSUS 001/2021 process: 350.095.442.048.526.000.000), INCT EpiAmO.
REFERENCES
- 1.WHO WHO Coronavirus (COVID-19) Dashboard. Dashboard with vaccination data [Internet] 2021. https://covid19.who.int/
- 2.WHO Tracking SARS-CoV-2 variants [Internet] 2022. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
- 3.Naveca F, Souza V, Corado A, Nascimento F, Silva G, Costa Á, et al. COVID-19 epidemic in the Brazilian state of Amazonas was driven by long-term persistence of endemic SARS-CoV-2 lineages and the recent emergence of the new variant of concern P.1. 2021. https://www.researchsquare.com
- 4.Kumar S. Second wave of COVID-19: emergency situation in India. J Travel Med. 2021 doi: 10.1093/jtm/taab082. https://academic.oup.com/jtm/article/28/7/taab082/6284095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Arantes I, Gomes Naveca F, Gräf T, Genomic F, Network S, Miyajima F, et al. Emergence and spread of the SARS-CoV-2 variant of concern Delta across different Brazilian regions. medRxiv. 2022 doi: 10.1128/spectrum.02641-21. https://www.medrxiv.org/content/10.1101/2021.11.25.21266251v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.de Souza UJB, dos Santos RN, Campos FS, Lourenço KL, da Fonseca FG, Spilki FR. High rate of mutational events in SARS-CoV-2 genomes across Brazilian geographical regions, February 2020 to June 2021. Viruses. 2021 doi: 10.3390/v13091806. https://pmc/articles/PMC8473193/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rambaut A, Holmes EC. O'Toole Á.Hill V.McCrone JT.Ruis C A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat Microbiol. 2020;5(11):1403–1407. doi: 10.1038/s41564-020-0770-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.O'Toole Á, Scher E, Underwood A, Jackson B, Hill V, McCrone JT, et al. Assignment of epidemiological lineages in an emerging pandemic using the pangolin tool. Virus Evol. 2022 doi: 10.1093/ve/veab064. https://academic.oup.com/ve/article/7/2/veab064/6315289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ministério da Saúde Brasil Boletim Epidemiológico Nº 92. Boletim COE Coronavírus. 2021 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/boletins-epidemiologicos-covid-19/2021/boletim_epidemiologico_covid_92_10dez21.pdf/view [Google Scholar]
- 10.Gomes Naveca F, Nascimento V, Souza V, de Lima Corado A, Nascimento F, Silva G, et al. Spread of Gamma (P.1) sub-lineages carrying spike mutations close to the furin cleavage site and deletions in the N-terminal domain drives ongoing transmission of SARS-CoV-2 in Amazonas, Brazil. 2022. [DOI] [PMC free article] [PubMed]
- 11.Global Influenza Surveillance and Response System GISAID Initiative. 2021. https://www.gisaid.org/
- 12.Katoh K, Standley DM. MAFFT Multiple Sequence Alignment Software Version 7 improvements in performance and usability. Mol Biol Evol. 2013;30(4):772–780. doi: 10.1093/molbev/mst010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Minh BQ, Schmidt HA, Chernomor O, Schrempf D, Woodhams MD, von Haeseler A. IQ-TREE 2 new models and efficient methods for phylogenetic inference in the genomic era. Mol Biol Evol. 2020;37(5):1530–1534. doi: 10.1093/molbev/msaa015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kalyaanamoorthy S, Minh BQ, Wong TKF, von Haeseler A, Jermiin LS. ModelFinder fast model selection for accurate phylogenetic estimates. Nat Methods. 2017;14(6):587–589. doi: 10.1038/nmeth.4285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.FigTree 2021. http://tree.bio.ed.ac.uk/software/figtree/
- 16.Hadfield J, Megill C, Bell SM, Huddleston J, Potter B, Callender C. NextStrain Real-time tracking of pathogen evolution. Bioinformatics. 2018;34(23):4121–4123. doi: 10.1093/bioinformatics/bty407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Queiroz JA da S.Rampazzo R de CP.Filho EB da S.Oliveira GS.Oliveira S da C.Souza LFB Development of a quantitative one-step multiplex RT-qPCR assay for the detection of SARS-CoV-2 in a biological matrix. Int J Infect Dis. 2021;104:373–378. doi: 10.1016/j.ijid.2021.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Naveca FG, Nascimento V, de Souza VC, Corado A de L, Nascimento F, Silva G, et al. COVID-19 in Amazonas, Brazil, was driven by the persistence of endemic lineages and P.1 emergence. Nat Med. 2021 doi: 10.1038/s41591-021-01378-7. https://www.nature.com/articles/s41591-021-01378-7 [DOI] [PubMed] [Google Scholar]
- 19.Faria NR, Morales Claro I, Candido D, Franco LAM, Andrade PS, Coletti TM, et al. Genomic characterisation of an emergent SARS-CoV-2 lineage in Manaus: preliminary findings [Internet] 2021. https://virological.org/t/genomic-characterisation-of-an-emergent-sars-cov-2-lineage-in-manaus-preliminary-findings/586
- 20.Naveca FG, Alves Nascimento V, Nascimento F, Ogrzewalska M, Pauvolid-Corrêa A, Ferreira Araujo M, et al. A case series of SARS-CoV-2 reinfections caused by the variant of concern Gamma in Brazil. medRxiv. 2022 https://www.medrxiv.org/content/10.1101/2021.11.29.21266109v1 [Google Scholar]
- 21.Ministério da Saúde Brasil Boletim Epidemiológico Nº 88. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_88_23nov21_fig37nova.pdf/view [Google Scholar]
- 22.Ministério da Saúde Brasil Boletim Epidemiológico Nº 83. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_83.pdf/view [Google Scholar]
- 23.Ministério da Saúde Brasil Boletim Epidemiológico Nº 75. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_75-final-13ago_15h40.pdf/view [Google Scholar]
- 24.Ministério da Saúde Brasil Boletim Epidemiológico Nº 70. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_70-1.pdf/view [Google Scholar]
- 25.Ministério da Saúde Brasil Boletim Epidemiológico Nº 66. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_66-final_-11-junho.pdf/view [Google Scholar]
- 26.Ministério da Saúde Brasil Boletim Epidemiológico Nº 61. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_61_final.pdf/view [Google Scholar]
- 27.Ministério da Saúde Brasil Boletim Epidemiológico Nº 57. Boletim COE Coronavírus. 2022 https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_57.pdf/view [Google Scholar]
- 28.Hwang H, Lim JS, Song SA, Achangwa C, Sim W, Kim G, et al. Transmission dynamics of the Delta variant of SARS-CoV-2 infections in South Korea. J Infect Dis. 2022 doi: 10.1093/infdis/jiab586. https://academic.oup.com/jid/advance-article/doi/10.1093/infdis/jiab586/6448309 [DOI] [PubMed] [Google Scholar]
- 29.Mishra S, Mindermann S, Sharma M, Whittaker C, Mellan TA, Wilton T, et al. Changing composition of SARS-CoV-2 lineages and rise of Delta variant in England. EClinicalMedicine. 2021 doi: 10.1016/j.eclinm.2021.101064. https://pubmed.ncbi.nlm.nih.gov/34401689/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tian D, Sun Y, Zhou J, Ye Q. The global epidemic of the SARS-CoV-2 Delta variant, key spike mutations and immune escape. Front Immunol. 2021 doi: 10.3389/fimmu.2021.751778. https://pubmed.ncbi.nlm.nih.gov/34917076/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Earnest R, Uddin R, Matluk N, Renzette N, Siddle KJ, Loreth C, et al. Comparative transmissibility of SARS-CoV-2 variants Delta and Alpha in New England, USA. medRxiv. 2021 doi: 10.1016/j.xcrm.2022.100583. https://pmc/articles/PMC8509091/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Moghaddar M, Radman R, Macreadie I. Severity, pathogenicity and transmissibility of Delta and Lambda variants of SARS-CoV-2, toxicity of spike protein and possibilities for future prevention of COVID-19. Microorganisms. 2021. https://pmc/articles/PMC8540532/ [DOI] [PMC free article] [PubMed]
- 33.Campbell F, Archer B, Laurenson-Schafer H, Jinnai Y, Konings F, Batra N, et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance. 2021 doi: 10.2807/1560-7917.ES.2021.26.24.2100509. https://pmc/articles/PMC8212592/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yang W, Shaman J. COVID-19 pandemic dynamics in India, the SARS-CoV-2 Delta variant, and implications for vaccination. medRxiv. 2022 doi: 10.1098/rsif.2021.0900. https://www.medrxiv.org/content/10.1101/2021.06.21.21259268v2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fundação Oswaldo Cruz Dashboard Rede Genômica - Genomahcov [Internet] 2021. http://www.genomahcov.fiocruz.br/dashboard/
- 36.Lima ARJ, Ribeiro G, Viala VL, Lima LPO de, Martins AJ, Barros CR dos S, et al. SARS-CoV-2 genomic monitoring in the São Paulo state unveils new sublineages of the AY.43 strain. medRxiv. 2022 https://www.medrxiv.org/content/10.1101/2021.11.29.21266819v1 [Google Scholar]
- 37.Kannan SR, Spratt AN, Cohen AR, Naqvi SH, Chand HS, Quinn TP, et al. Evolutionary analysis of the Delta and Delta plus variants of the SARS-CoV-2 viruses. J Autoimmun. 2022 doi: 10.1016/j.jaut.2021.102715. https://pubmed.ncbi.nlm.nih.gov/34399188/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.WHO COVID-19 vaccines advice [Internet] 2022. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
- 39.Centers for Disease Control and Prevention COVID-19 vaccines for children and teens [Internet] 2022. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/children-teens.html
- 40.Walter EB, Talaat KR, Sabharwal C, Gurtman A, Lockhart S, Paulsen GC, et al. Evaluation of the BNT162b2 covid-19 vaccine in children 5 to 11 years of age. N Engl J Med. 2022 doi: 10.1056/NEJMoa2116298. https://www.nejm.org/doi/full/10.1056/nejmoa2116298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Paschoalotto MAC, Costa EPPA, Almeida SV de, Cima J, Costa JG da, Santos JV, et al. Running away from the jab: factors associated with COVID-19 vaccine hesitancy in Brazil. Rev Saude Publica. 2022 doi: 10.11606/s1518-8787.2021055003903. https://www.revistas.usp.br/rsp/article/view/193416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Moore DCBC, Nehab MF, Camacho KG, Reis AT. Junqueira-Marinho M de F.Abramov DM Low COVID-19 vaccine hesitancy in Brazil. Vaccine. 2021;39(42):6262–6268. doi: 10.1016/j.vaccine.2021.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Harvey WT, Carabelli AM, Jackson B, Gupta RK, Thomson EC, Harrison EM, et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat Rev Microbiol. 2021. https://www.nature.com/articles/s41579-021-00573-0 [DOI] [PMC free article] [PubMed]
- 44.Weisblum Y, Schmidt F, Zhang F, DaSilva J, Poston D, Lorenzi JCC, et al. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. Elife. 2022 doi: 10.7554/eLife.61312. https://pubmed.ncbi.nlm.nih.gov/33112236/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Abbasi J. Studies suggest COVID-19 vaccine boosters save lives. JAMA. 2022 doi: 10.1001/jama.2021.23455. https://jamanetwork.com/journals/jama/fullarticle/2787929 [DOI] [PubMed] [Google Scholar]
- 46.Avivi I, Luttwak E, Saiag E, Halperin T, Haberman S, Sarig A, et al. BNT162b2 mRNA COVID-19 vaccine booster induces seroconversion in patients with B-cell non-Hodgkin lymphoma who failed to respond to two prior vaccine doses. Br J Haematol. 2022 doi: 10.1111/bjh.18029. https://onlinelibrary.wiley.com/doi/full/10.1111/bjh.18029 [DOI] [PubMed] [Google Scholar]
- 47.Mattiuzzi C, Lippi G. Efficacy of COVID-19 vaccine booster doses in older people. Eur Geriatr Med. 2022 doi: 10.1007/s41999-022-00615-7. https://pubmed.ncbi.nlm.nih.gov/35067909/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Governo do Estado de Rondônia 2022. https://rondonia.ro.gov.br/covid-19/
- 49.Schwarzinger M, Watson V, Arwidson P, Alla F, Luchini S. COVID-19 vaccine hesitancy in a representative working-age population in France: a survey experiment based on vaccine characteristics. Lancet Public Health. 2021 doi: 10.1016/S2468-2667(21)00012-8. http://www.thelancet.com/article/S2468266721000128/fulltext [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Al-Mulla R, Abu-Madi M, Talafha QM, Tayyem RF, Abdallah AM. COVID-19 vaccine hesitancy in a representative education sector population in Qatar. Vaccines. 2022 doi: 10.3390/vaccines9060665. https://www.mdpi.com/2076-393X/9/6/665/htm [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Greaney AJ, Loes AN, Crawford KHD, Starr TN, Malone KD, Chu HY, et al. Comprehensive mapping of mutations in the SARS-CoV-2 receptor-binding domain that affect recognition by polyclonal human plasma antibodies. Cell Host Microbe. 2022 doi: 10.1016/j.chom.2021.02.003. https://pubmed.ncbi.nlm.nih.gov/33592168/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Starr TN, Greaney AJ, Hilton SK, Ellis D, Crawford KHD, Dingens AS, et al. Deep mutational scanning of SARS-CoV-2 receptor binding domain reveals constraints on folding and ACE2 binding. Cell. 2022 doi: 10.1016/j.cell.2020.08.012. https://pubmed.ncbi.nlm.nih.gov/32841599/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Centers for Disease Control and Prevention Vaccine breakthrough infections: the possibility of getting COVID-19 after getting vaccinated [Internet] 2022. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/why-measure-effectiveness/breakthrough-cases.html
- 54.Pan Y, Zhang D, Yang P, Poon LLM, Wang Q. Viral load of SARS-CoV-2 in clinical samples. Lancet Infect Dis. 2020;20(4):411–412. doi: 10.1016/S1473-3099(20)30113-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sun P, Qie S, Liu Z, Ren J, Li K, Xi J. Clinical characteristics of hospitalized patients with SARS-CoV-2 infection: a single arm meta-analysis. J Med Virol. 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/jmv.25735 [DOI] [PMC free article] [PubMed]
- 56.Galmiche S, Bruel T, Madec Y, Tondeur L, Grzelak L, Staropoli I, et al. Characteristics associated with olfactory and taste disorders in COVID-19. 2021. https://www.karger.com/Article/FullText/517066 [DOI] [PMC free article] [PubMed]