

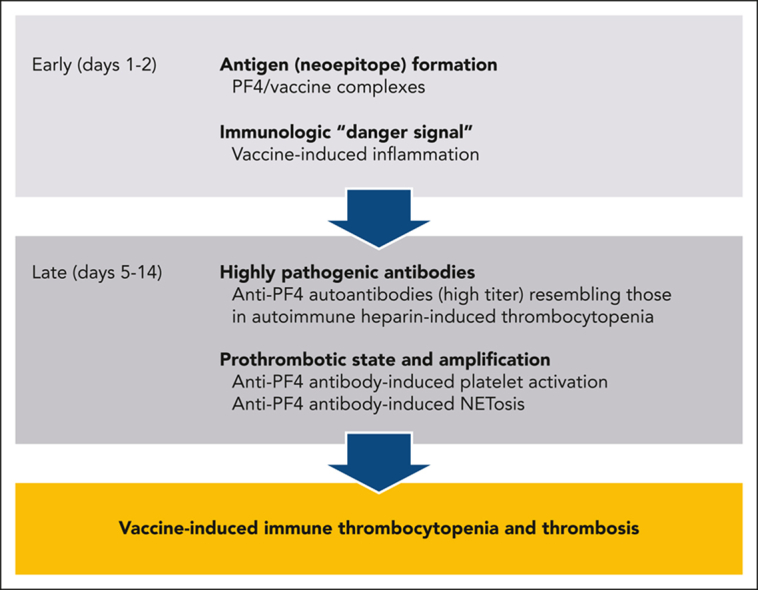
Visual Abstract
Abstract
Within the first months of the COVID-19 vaccination campaign, previously healthy recipients who developed severe thrombosis (often cerebral and/or splanchnic vasculature) and thrombocytopenia typically after adenoviral vector-based vaccination were identified. Similarities between this syndrome, vaccine-induced immune thrombotic thrombocytopenia (VITT), and heparin-induced thrombocytopenia prompted recognition of the role of antiplatelet factor 4 (PF4) antibodies and management strategies based on IV immunoglobulin and nonheparin anticoagulants, which improved outcome. We update current understanding of VITT and potential involvement of anti-PF4 antibodies in thrombotic disorders.
Cines and Greinacher provide a succinct Blood Spotlight review of current knowledge about COVID-19 and vaccine-induced immune thrombotic thrombocytopenia. This problem remains highly relevant in low- and middle-income countries that can only afford adenoviral vector-based vaccines for ongoing vaccination campaigns. It is also important to understand which vaccine constituent(s) triggers the immune response to the implicated platelet antigen, platelet factor 4, to design safer delivery systems for vaccinations against this and future emergent infectious diseases.
Introduction
Biotechnology and pharmaceutical companies responded to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic with unprecedented speed, generating adenovirus-based vaccines (ChAdOx1/nCoV-19 from AstraZeneca/Covishield and Ad26 COV2.S from Johnson and Johnson/Janssen) and mRNA-based vaccines (mRNA-1273 from Moderna and tozinameran/Comirnaty from Pfizer-BioNTech). Outside the European Union and the United States, SputnikV, Sinopharm, Sinovac-CoronaVac and Bharat Biotech BBV152 Covaxin vaccines are also used. However, by March 2021, safety signals concerning vaccines that use adenovirus-based vectors emerged involving previously healthy recipients who developed thromboses and thrombocytopenia, typically in the second week after initial vaccination.1, 2, 3, 4, 5
The term thrombosis and thrombocytopenia syndrome (TTS) refers to all thrombocytopenia and thrombotic complications after vaccination. Based on clinical similarities to “autoimmune” or “spontaneous” heparin-induced thrombocytopenia,6,7 Immunoglobulin G (IgG) antibodies cross-reacting with “unbound” platelet factor 4 (PF4) in assays for heparin-induced thrombocytopenia (HIT) were soon identified in a subgroup of patients with TTS. This syndrome, vaccine-induced immune thrombotic thrombocytopenia (VITT), was the subject of a Blood Spotlight in 20218; several national and international guidelines for diagnosis and management have been published,9, 10, 11, 12, 13, 14 which will be updated in 2023 by the World Health Organization.15 VITT remains highly relevant in low- and middle-income countries that can only afford adenoviral vector-based vaccines and where the vaccination campaign is ongoing. It is also important to understand which vaccine constituent(s) trigger(s) the immune response to PF4, in order to design safer delivery systems. Here we update our understanding of VITT based on recent findings.
Clinical presentation
The incidence of VITT is estimated to be 3 to 15 cases per million initial vaccinations,16,17 depending on recognition and case definition. Fewer than 50 patients with VITT have been reported from Asia, Africa and Latin America combined. Potential under-recognition18 is worrisome, as early recognition and start of treatment can reduce mortality by nearly 90%. This has been demonstrated by the reduction in mortality from about 50% in the first 3 case series1,2,19 to about 5% to 6% in Australia where the vaccination campaign was combined with an educational program informing the public and especially physicians about symptoms of VITT and appropriate treatment.20
Patients typically present 4 to 30 days after first vaccination with an adenoviral vector-based vaccine (irrespective of whether another type of COVID-19 vaccine had been given before),19 with rare cases developing after a second vaccination with an adenovirus vector-based vaccine.18,21 There is a predilection for cerebral venous sinus thrombosis (CVST) and cerebral venous thrombosis, with ∼50% to 70% of patients presenting with persistent headache or other neurologic complaints, and for thrombi developing within the splanchnic and portal venous systems, with 10% to 20% of patients presenting with abdominal complaints; the remaining patients present with symptoms resulting from deep venous thrombosis, pulmonary embolism, and arterial thrombosis, including stroke and myocardial infarction. Thrombocytopenia is almost universal by the time of presentation, but occasionally precedes thromboembolism. An unexplained fall in platelet count >50% also indicates VITT independent of the absolute platelet count.17 A marked elevation in plasma D-dimers (>4000 fibrinogen equivalent units) is common, and so is a reduction in plasma fibrinogen,1,2,19 indicative of disseminated intravascular coagulation. Imaging reveals one or more sites of thrombosis in over 90% of patients, but neurovascular imaging may be negative initially in some who present on or after postvaccination day 4 with severe headache or with incipient microvascular CVST, necessitating treatment for presumed VITT and repeat imaging22 (“pre-VITT syndrome”23).
Diagnosis
VITT is a life-threatening condition, especially when CVST is present,21 and should be the foremost consideration in any patient who presents with severe headache and/or thrombosis with thrombocytopenia starting 4 to 30 days after adenoviral vector-based vaccination against SARS-CoV-2. Criteria have been published to help assess the likelihood of VITT (definite, probable, possible, unlikely) based on clinical features alone and along with the results of enzyme-linked immunosorbent assays (ELISAs) to detect anti-PF4 antibodies (Table 1).17,19 Routine postvaccine screening for PF4/heparin antibodies after vaccination is discouraged, as low levels of clinically irrelevant anti-PF4/heparin antibodies are detected in 5% to 10% of healthy recipients of adenoviral and mRNA-based vaccines.24 However, the clinical diagnosis of VITT should always be confirmed by PF4/heparin ELISA, as recent COVID-19 vaccination does not exclude coincidental thrombotic complications caused by HIT, cancer associated thrombosis, catastrophic antiphospholipid syndrome, HELLP syndrome in pregnancy, and thrombotic thrombocytopenic purpura, among others,25,26 especially if not all the clinical criteria presented in Table 1 are present.
Table 1.
The UK Haematology Expert Group developed consensus diagnostic criteria for VITT
| Case definition criteria |
| Onset of symptoms 5-30 days after COVID-19 vaccine (or up to 42 days if isolated DVT/PE) |
| Presence of thrombosis |
| Thrombocytopenia (platelet count <150 × 109/L) |
| D-dimer >4000 μg/mL (FEU) |
| Positive anti-PF4 Abs ELISA |
| Definite VITT |
| Meets all 5 criteria |
| Probable |
| D-dimer >4000 FEU but one criterion not fulfilled (timing, thrombosis, thrombocytopenia, anti-PF4 Abs), or |
| D-dimer unknown or 2000-4000 FEU with all other criteria present |
| Possible |
| D-dimer unknown or 2000-4000 FEU with one other criterion not fulfilled, or |
| Two other criteria not fulfilled (timing, thrombosis, thrombocytopenia, anti-PF4 Abs) |
| Unlikely |
| Platelet count <150 × 109/L without thrombosis with D-dimer <2000 FEU, or |
| Thrombosis with platelet count >150 × 109/L and D-dimer <2000 FEU, regardless of anti-PF4 Ab result, and/or |
Reproduced from “Vaccine induced immune thrombocytopenia and thrombosis: summary of NICE guidance,” Pavord S, Hunt BJ, Horner D, Bewley S, Karpusheff J; Guideline Committee. BMJ. 375:n2195, © 2021, with permission from BMJ Publishing Group Ltd.84
Microtiter plate ELISAs that measure antibodies to PF4/polyanion complexes used to diagnose HIT also detect anti-PF4 antibodies that cause VITT,17,19,27, 28, 29 most likely because noncomplexed PF4 is also coated on the solid phase.30 However, assays differ in sensitivity, and no single assay detects all possible cases. In case of strong clinical suspicion, treatment (see below) should be started immediately. Importantly most “rapid” and automated assays used to diagnose HIT give false negative results in VITT.19,28,30, 31, 32 The diagnosis can be confirmed with a functional assay showing PF4-dependent platelet activation by patient plasma or serum; activation is blocked by a monoclonal antibody to FcRγIIA and typically by high concentrations (100 IU/mL) of heparin. In contrast to HIT, low concentrations of heparin (0.2-1.0 IU) do not enhance, and indeed often inhibit, platelet activation by patient sera; instead, addition of PF4 (10 μg/mL) is needed to optimize platelet activation by VITT antibodies. The combination of a strongly positive PF4/heparin ELISA with PF4-dependent, heparin-independent platelet-activating antibodies has a sensitivity approaching 100% in the absence of recent administration of IVIG.33 In one study, the specificity of combined testing is ∼80% because of positive serology in patients with pre-VITT without documented thrombosis who might indeed have VITT.33 The sensitivity of the functional assay can be enhanced by testing undiluted and, if negative, diluted serum, which optimizes the stoichiometric ratio between PF4 and high titer antibodies that form pathogenic immune complexes.34 However, functional testing is not widely available in time for clinical decisions. The duration of antibody positivity is quite variable. Similar to HIT, platelet activating antibodies are generally no longer detected by 5 months, but positive ELISAs (albeit with falling optical densities) often persist.17,35, 36, 37 Rarely thrombocytopenia and high D-dimers do not resolve within 2-3 weeks after the onset of VITT, especially in patients with persistent high titer platelet-activating antibodies.35,36
Pathophysiology
VITT is the most recently described prothrombotic disorder mediated by anti-PF4 antibodies, ranging in decreasing frequency from “classic HIT,” to “persistent HIT” triggered by heparin that continues beyond drug exposure, to “autoimmune HIT” or “spontaneous HIT” that occurs without heparin exposure after orthopedic knee replacement surgery or after viral or bacterial infections.6,7,38
VITT antibodies recognize an epitope on PF4 that overlaps with the binding site for heparin, distinct from those recognized by HIT antibodies.39, 40, 41 This may enable VITT antibodies to bypass the template function served in HIT by heparin, DNA and polyphosphates42,43 by clustering PF4 directly.44 Binding of VITT antibodies is not restricted to this site,40 allowing them to also form immune complexes with PF4 bound to glycosaminoglycans expressed on cell surfaces. By analogy to the other anti-PF4 antibody-mediated disorders, the subsequent downstream prothrombotic cascade of VITT with activation of multiple cells including NETosis, is reasonably well understood and is summarized in Figure 1B.45
Figure 1.

Current concept of the pathogenesis of VITT. The schematic presentation shown in A is speculative and in large part inferred from experiments in HIT. The schematic presentation of the downstream prothrombotic process shown in Panel B is largely substantiated by experimental data, some performed with VITT antibodies, others with HIT antibodies. Modified from Greinacher et al.45 (A) After vaccination, PF4 comes in contact with vaccine constituents and activates B-cells. Left side: It has been proposed that a direct inadvertent breach in the microvasculature at the vaccination site by IV injection or by disruption of vascular endothelial-cadherin tight junctions by EDTA in ChAdOx1, allows vaccine constituents to enter the circulation.45 Within the circulation, adenovirus particles can bind to platelets and can also bind PF4 released by activated platelets or from the matrix coating the microvascular endothelium.46,47 Platelets may become activated by vessel injury caused by injection of vaccine, after binding of the virions to the cell surface, or by immune complexes formed between contaminating host cell-line proteins in the vaccine and natural IgG antibodies against these proteins. Whether the virions themselves or another yet unknown constituent in the vaccine causes a conformational change in PF4 is unknown. Middle: once complexes with PF4 have formed, natural IgM antibodies activate complement (as it has been shown for PF4/heparin complexes),48 which enhances their proximity to B-cell receptors. In a mouse model, IV injection of ChAdOx-1, platelet-bound adenoviral particles are transported to the marginal zone of the spleen where B-cells are activated upon direct contact.49 However, electron microscopy and super resolution microscopy revealed complexes between PF4 and anti-PF4 VITT antibodies with amorphous constituents of the vaccine rather than virus particles.50 Beside the virions, other potential partners for PF4 include unassembled hexons51 and host cell-line proteins, although there is little overlap in the proteins contaminating ChAdOx1 and Ad26.COV2 vaccines.51 Right side: eventually, complexes of PF4 and vaccine (constituents) come in contact with B-cells expressing a cognate Ig receptors for PF4, either as fluid phase complexes, as virion-PF4 complexes, or the complexes are presented by platelets. (B) From right to left. After clonal expansion and isotype switching of one or a few B-cell clones, high titer IgG anti-PF4 antibodies are released into the circulation.52,53 Immune complexes containing PF4 and anti-PF4 IgG cluster and signal through FcRγIIA,50,54 which generates procoagulant platelets, induces platelet/neutrophil aggregates,55 and stimulates NETosis by neutrophils.50,54,56 DNA released by NETosis amplifies immune injury and activates complement, which deposits on the endothelium.57,58 Endothelial cells become activated, expressing tissue factor and releasing von Willebrand factor (VWF). VWF binds PF4 and subsequently anti-PF4 antibodies, which in turn further activates neutrophils and further propagates thrombin generation.59 Professional illustration by Patrick Lane, ScEYEnce Studios.
It is less clear how the anti-PF4 response is initiated. VITT appears to be a class effect of adenovirus vector-based vaccines. The few cases of platelet activating PF4-dependent antibodies attributed to mRNA vaccines probably reflect the background rate of spontaneous or autoimmune HIT.34 However, which constituent(s) in the vaccines might cause(s) conformational changes in PF4 through electrostatic interactions to trigger the immune response46,50,51 is unresolved. The observation of a VITT-like syndrome after human-papilloma virus 60 vaccination suggests a range of factors may trigger conformational changes in PF4, similar to the HIT antigen that can be induced by diverse polyanions.61 Figure 1A summarizes some of the current hypotheses on the generation of VITT antibodies.
Anti-PF4 antibodies in VITT do not cross-react with spike protein,62,63 nor does COVID-19 infection increase anti-PF4 antibody titers,64 although high titer anti-PF4 antibodies have also been observed in patients with COVID-19.65 The development of high avidity isotype-switched IgG antibodies by day 5 postvaccination, also seen in HIT, suggests activation of preexisting PF4-reactive marginal zone memory B-cells in the spleen and elsewhere posited to be involved in the innate immune response to microbial infection50,66 in the setting of inflammatory costimulatory signals.50,56
At least some VITT antibodies are oligoclonal52 (in contrast to HIT antibodies) and the reported skewing in the expression of the genes that encode the hypervariable region of the immunoglobulin light chain53 might point to a genetic predisposition to respond to vaccination by generating anti-PF4 antibodies. Few individuals have preexisting antibodies against ChAdOx-1 and or Ad26 COV2.S before vaccination.67,68 Neutralizing antibodies to adenoviral proteins that develop after the initial vaccination may thereafter limit exposure to viral proteins entering the circulation or inhibit formation of viral protein-PF4 complexes, reducing the risk of developing VITT after subsequent vaccinations. VITT-like antibodies are not restricted to COVID-19 vaccination. In one patient with monoclonal gammopathy and recurrent venous and arterial thromboses, PF4-dependent platelet activating antibodies binding to the same binding site on PF4 as VITT antibodies were identified.34 The frequency of such VITT-like antibodies in patients with recurrent thrombosis is currently unresolved as is the predilection for thrombosis involving the cerebral and splanchnic-portal vasculatures.69
Treatment
Treatment should be initiated with IVIG (1 mg/kg IV × 2 days),70 which inhibits FcRγIIA-mediated platelet activation70, 71, 72 and a nonheparin anticoagulant (direct thrombin inhibitors, oral anti-Xa agents, fondaparinux). Although >95% of patients with VITT develop thrombotic complications, in a few patients, clinical symptoms, especially headache, can precede thrombosis, so-called pre-VITT. In case of strong clinical suspicion, treatment with IVIG and therapeutic dose anticoagulation should be started immediately, even in the absence of overt thrombosis. Heparin appears to be safe and effective in most patients and may be the only anticoagulant available in some jurisdictions.4,9,73 However, nonheparin anticoagulants are preferred as concurrent heparin-dependent antibodies might be present in a small subset of patients. Vitamin K antagonists should be avoided during the acute phase of VITT, as the induced protein C deficiency can worsen microvascular thrombosis in severe prothrombotic disorders.74 In patients with extensive CVST, anticoagulation after IVIG is generally indicated,75 but timing and intensity depends on severity of thrombocytopenia and presence of extensive intracerebral hemorrhage. Prophylactic platelet transfusions are discouraged; however, supplementation with fibrinogen17 and transfusion of platelets may be indicated for bleeding especially during surgical procedures.76 Patients with platelet counts <30 × 109/L and CVST may benefit from plasma exchange.17,19,77,78 The role of corticosteroids19 and inhibition of complement79,80 in nonresponsive or critically ill patients remains to be established. The potential of blocking FcRγIIA-mediated procoagulant pathways with inhibitors of the Bruton kinase pathway81 has not been tested clinically. Platelet inhibitors may have a role in long term secondary prophylaxis in patients with arterial thrombosis. However, in acute VITT, inhibition of thrombin generation is more important and dual anticoagulation may enhance the bleeding risk.
The platelet count and D-dimer levels should be used to guide duration of therapeutic dose anticoagulation rather than the results of anti-PF4 antibody tests. If platelet counts decrease and D-dimer levels increase after stopping anticoagulation, treatment should be resumed as recurrences of thrombocytopenia/thrombosis requiring retreatment with IVIG have been reported.17,19,35,71 The optimal duration of thromboprophylaxis is uncertain, but generally guided by the location and severity of the initial thrombotic complication(s).17 Revaccination using mRNA-based vaccines is safe and has not led to a recrudescence of platelet activating anti-PF4 antibodies.64,82
Conclusions, unknowns and future directions
Fortunately, VITT is very rare. However, it can be life-threatening, especially if the diagnosis and treatment are delayed. Adenovirus vectors provide an affordable framework for highly effective vaccines. Unravelling the mechanisms of the anti-PF4 response in VITT has the potential to provide the basis for a more rational approach to developing safer vaccine delivery systems. The finding of VITT-like antibodies in patients with recurrent thrombosis raises the possibility that platelet-activating anti-PF4 antibodies might contribute to as yet unexplained recurrent venous and arterial thrombotic disorders. This question can be addressed once assays that distinguish HIT-like and VITT-like anti-PF4 antibodies are developed.83
Conflict-of-interest disclosure: A.G.'s employer, Universitätsmedizin Greifswald, holds a patent for a laboratory assay detecting VITT-like anti-PF4 antibodies. D.B.C. declares no competing financial interests.
Acknowledgments
This work was supported by National Institutes of Health, National Heart, Lung, and Blood Institute grants HL151730 and HL142122 (D.B.C.).
Authorship
Contribution: D.B.C. and A.G. contributed equally to this work, from conceptualization through the development of the manuscript.
References
- 1.Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med. 2021;384(22):2092–2101. doi: 10.1056/NEJMoa2104840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schultz NH, Sorvoll IH, Michelsen AE, et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med. 2021;384(22):2124–2130. doi: 10.1056/NEJMoa2104882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Scully M, Singh D, Lown R, et al. Pathologic antibodies to platelet factor 4 after ChAdOx1 nCoV-19 vaccination. N Engl J Med. 2021;384(23):2202–2211. doi: 10.1056/NEJMoa2105385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization Coronavirus disease (COVID-19): vaccines. 2022. https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines? [PubMed]
- 5.Herrera-Comoglio R, Lane S. Vaccine-induced immune thrombocytopenia and thrombosis after the Sputnik V vaccine. N Engl J Med. 2022;387(15):1431–1432. doi: 10.1056/NEJMc2210813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Warkentin TE, Greinacher A. Spontaneous HIT syndrome: knee replacement, infection, and parallels with vaccine-induced immune thrombotic thrombocytopenia. Thromb Res. 2021;204:40–51. doi: 10.1016/j.thromres.2021.05.018. [DOI] [PubMed] [Google Scholar]
- 7.Warkentin TE. Platelet-activating anti-PF4 disorders: an overview. Semin Hematol. 2022;59(2):59–71. doi: 10.1053/j.seminhematol.2022.02.005. [DOI] [PubMed] [Google Scholar]
- 8.Arepally GM, Ortel TL. Vaccine-induced immune thrombotic thrombocytopenia: what we know and do not know. Blood. 2021;138(4):293–298. doi: 10.1182/blood.2021012152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Greinacher A, Langer F, Makris M, et al. Vaccine-induced immune thrombotic thrombocytopenia (VITT) – update on diagnosis and management considering different resources: response to comment from Yamada et al. J Thromb Haemost. 2022;20(2):542–543. doi: 10.1111/jth.15619. [DOI] [PubMed] [Google Scholar]
- 10.Oldenburg J, Klamroth R, Langer F, et al. Diagnosis and management of vaccine-related thrombosis following AstraZeneca COVID-19 vaccination: guidance statement from the GTH. Hamostaseologie. 2021;41(3):184–189. doi: 10.1055/a-1469-7481. [DOI] [PubMed] [Google Scholar]
- 11.Nazy I, Sachs UJ, Arnold DM, et al. Recommendations for the clinical and laboratory diagnosis of VITT against COVID-19: Communication from the ISTH SSC Subcommittee on Platelet Immunology. J Thromb Haemost. 2021;19(6):1585–1588. doi: 10.1111/jth.15341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chen RT. Interim case definition of thrombosis with thrombocytopenia syndrome (TTS) 2021. https:brightoncollaborationus/thrombosis-with-thrombocytopenia-interim-case definition
- 13.American Society of Hematology Vaccine-induced immune thrombotic thrombocytopenia. https://www.hematology.org/covid-19/vaccine-induced-immune-thrombotic-thrombocytopenia
- 14.Guidance produced by the Expert Haematology Panel (EHP) focussed on Vaccine induced Thrombosis and Thrombocytopenia (VITT) https://b-s-h.org.uk/about-us/news/guidance-produced-by-the-expert-haematology-panel-ehp-focused-on-vaccine-induced-thrombosis and thrombocytopenia-vitt
- 15.WHO Updated guidance for clinical case management of thrombosis with thrombocytopenia syndrome (TTS) following vaccination to prevent coronavirus disease (COVID-19).Updated guidance. 2023. Forthcoming. [PubMed] [Google Scholar]
- 16.See I, Lale A, Marquez P, et al. Case series of thrombosis with thrombocytopenia syndrome after COVID-19 vaccination-United States, December 2020 to August 2021. Ann Intern Med. 2022;175(4):513–522. doi: 10.7326/M21-4502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Craven B, Lester W, Boyce S, et al. Natural history of PF4 antibodies in vaccine-induced immune thrombocytopenia and thrombosis. Blood. 2022;139(16):2553–2560. doi: 10.1182/blood.2021014684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Paez-Alacron ME, Greinacher A. Vaccine-induced immune thrombotic thrombocytopenia (VITT)-Update on diagnosis and management considering different resources: comment. J Thromb Haemost. 2022;20(11):2707–2708. doi: 10.1111/jth.15853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pavord S, Scully M, Hunt BJ, et al. Clinical features of vaccine-induced immune thrombocytopenia and thrombosis. N Engl J Med. 2021;385(18):1680–1689. doi: 10.1056/NEJMoa2109908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Australian Government, Department of Health and Aged Care. https://www.tga.gov.au/periodic/covid-19-vaccine-weekly-safety-report-23-09-2021
- 21.Krzywicka K, van de Munckhof A, Zimmermann J, et al. Cerebral venous thrombosis due to vaccine-induced immune thrombotic thrombocytopenia after a second ChAdOx1 nCoV-19 dose. Blood. 2022;139(17):2720–2724. doi: 10.1182/blood.2021015329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Salih F, Schonborn L, Kohler S, et al. Vaccine-induced thrombocytopenia with severe headache. N Engl J Med. 2021;385(22):2103–2105. doi: 10.1056/NEJMc2112974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Salih F, Kohler S, Schonborn L, Thiele T, Greinacher A, Endres M. Early recognition and treatment of pre-VITT syndrome after adenoviral vector-based SARS-CoV-2 vaccination may prevent from thrombotic complications: review of published cases and clinical pathway. Eur Heart J Open. 2022;2(3) doi: 10.1093/ehjopen/oeac036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Thiele T, Ulm L, Holtfreter S, et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood. 2021;138(4):299–303. doi: 10.1182/blood.2021012217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bissola AL, Daka M, Arnold DM, et al. The clinical and laboratory diagnosis of vaccine-induced immune thrombotic thrombocytopenia. Blood Adv. 2022;6(14):4228–4235. doi: 10.1182/bloodadvances.2022007766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lee AYY, Al Moosawi M, Peterson EA, et al. Clinical care pathway for the evaluation of patients with suspected VITT after ChAdOx1 nCoV-19 vaccination. Blood Adv. 2022;6(11):3315–3320. doi: 10.1182/bloodadvances.2021006862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vayne C, Rollin J, Gruel Y, et al. PF4 Immunoassays in vaccine-induced thrombotic thrombocytopenia. N Engl J Med. 2021;385(4):376–378. doi: 10.1056/NEJMc2106383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Platton S, Bartlett A, MacCallum P, et al. Evaluation of laboratory assays for anti-platelet factor 4 antibodies after ChAdOx1 nCOV-19 vaccination. J Thromb Haemost. 2021;19(8):2007–2013. doi: 10.1111/jth.15362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Reilly-Stitt C, Kitchen S, Jennings I, et al. Anti-PF4 testing for vaccine-induced immune thrombocytopenia and thrombosis and heparin induced thrombocytopenia: results from a UK National External Quality Assessment Scheme exercise April 2021. J Thromb Haemost. 2021;19(9):2263–2267. doi: 10.1111/jth.15423. [DOI] [PubMed] [Google Scholar]
- 30.Warkentin TE, Greinacher A. Laboratory testing for VITT antibodies. Semin Hematol. 2022;59(2):80–88. doi: 10.1053/j.seminhematol.2022.03.003. [DOI] [PubMed] [Google Scholar]
- 31.Sachs UJ, Cooper N, Czwalinna A, et al. PF4-dependent immunoassays in patients with vaccine-induced immune thrombotic thrombocytopenia: results of an interlaboratory comparison. Thromb Haemost. 2021;121(12):1622–1627. doi: 10.1055/a-1535-9002. [DOI] [PubMed] [Google Scholar]
- 32.Gabarin N, Arnold DM, Nazy I, Warkentin TE. Treatment of vaccine-induced immune thrombotic thrombocytopenia (VITT) Semin Hematol. 2022;59(2):89–96. doi: 10.1053/j.seminhematol.2022.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Thiele T, Weisser K, Schonborn L, et al. Laboratory confirmed vaccine-induced immune thrombotic thrombocytopenia: retrospective analysis of reported cases after vaccination with ChAdOx-1 nCoV-19 in Germany. Lancet Reg Health Eur. 2022;12 doi: 10.1016/j.lanepe.2021.100270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Greinacher A, Langer F, Schonborn L, et al. Platelet-activating anti-PF4 antibodies mimic VITT antibodies in an unvaccinated patient with monoclonal gammopathy. Haematologica. 2022;107(5):1219–1221. doi: 10.3324/haematol.2021.280366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Schonborn L, Thiele T, Kaderali L, Greinacher A. Decline in pathogenic antibodies over time in VITT. N Engl J Med. 2021;385(19):1815–1816. doi: 10.1056/NEJMc2112760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Schonborn L, Thiele T, Kaderali L, et al. Most anti-PF4 antibodies in vaccine-induced immune thrombotic thrombocytopenia are transient. Blood. 2022;139(12):1903–1907. doi: 10.1182/blood.2021014214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kanack AJ, Singh B, George G, et al. Persistence of Ad26.COV2.S-associated vaccine-induced immune thrombotic thrombocytopenia (VITT) and specific detection of VITT antibodies. Am J Hematol. 2022;97(5):519–526. doi: 10.1002/ajh.26488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Greinacher A, Selleng K, Warkentin TE. Autoimmune heparin-induced thrombocytopenia. J Thromb Haemost. 2017;15(11):2099–2114. doi: 10.1111/jth.13813. [DOI] [PubMed] [Google Scholar]
- 39.Huynh A, Kelton JG, Arnold DM, Daka M, Nazy I. Antibody epitopes in vaccine-induced immune thrombotic thrombocytopaenia. Nature. 2021;596(7873):565–569. doi: 10.1038/s41586-021-03744-4. [DOI] [PubMed] [Google Scholar]
- 40.Huynh A, Arnold DM, Michael JV, et al. Characteristics of VITT antibodies in patients vaccinated with Ad26.COV2.S. Blood Adv. 2023;7(2):246–250. doi: 10.1182/bloodadvances.2022007336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Huynh A, Arnold DM, Kelton JG, et al. Characterization of platelet factor 4 amino acids that bind pathogenic antibodies in heparin-induced thrombocytopenia. J Thromb Haemost. 2019;17(2):389–399. doi: 10.1111/jth.14369. [DOI] [PubMed] [Google Scholar]
- 42.Brandt S, Krauel K, Jaax M, et al. Polyphosphates form antigenic complexes with platelet factor 4 (PF4) and enhance PF4-binding to bacteria. Thromb Haemost. 2015;114(6):1189–1198. doi: 10.1160/TH15-01-0062. [DOI] [PubMed] [Google Scholar]
- 43.Cines DB, Yarovoi SV, Zaitsev SV, et al. Polyphosphate/platelet factor 4 complexes can mediate heparin-independent platelet activation in heparin-induced thrombocytopenia. Blood Adv. 2016;1(1):62–74. doi: 10.1182/bloodadvances.2016000877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sachais BS, Litvinov RI, Yarovoi SV, et al. Dynamic antibody-binding properties in the pathogenesis of HIT. Blood. 2012;120(5):1137–1142. doi: 10.1182/blood-2012-01-407262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Greinacher A, Schonborn L, Siegerist F, et al. Pathogenesis of vaccine-induced immune thrombotic thrombocytopenia (VITT) Semin Hematol. 2022;59(2):97–107. doi: 10.1053/j.seminhematol.2022.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Baker AT, Boyd RJ, Sarkar D, et al. ChAdOx1 interacts with CAR and PF4 with implications for thrombosis with thrombocytopenia syndrome. Sci Adv. 2021;7(49) doi: 10.1126/sciadv.abl8213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Othman M, Labelle A, Mazzetti I, Elbatarny HS, Lillicrap D. Adenovirus-induced thrombocytopenia: the role of von Willebrand factor and P-selectin in mediating accelerated platelet clearance. Blood. 2007;109(7):2832–2839. doi: 10.1182/blood-2006-06-032524. [DOI] [PubMed] [Google Scholar]
- 48.Khandelwal S, Barnes A, Rauova L, et al. Complement mediates binding and procoagulant effects of ultralarge HIT immune complexes. Blood. 2021;138(21):2106–2116. doi: 10.1182/blood.2020009487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Nicolai L, Leunig A, Pekayvaz K, et al. Thrombocytopenia and splenic platelet-directed immune responses after IV ChAdOx1 nCov-19 administration. Blood. 2022;140(5):478–490. doi: 10.1182/blood.2021014712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Greinacher A, Selleng K, Palankar R, et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood. 2021;138(22):2256–2268. doi: 10.1182/blood.2021013231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Michalik S, Siegerist F, Palankar R, et al. Comparative analysis of ChAdOx1 nCoV-19 and Ad26.COV2.S SARS-CoV-2 vector vaccines. Haematologica. 2022;107(4):947–957. doi: 10.3324/haematol.2021.280154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kanack AJ, Bayas A, George G, et al. Monoclonal and oligoclonal anti-platelet factor 4 antibodies mediate VITT. Blood. 2022;140(1):73–77. doi: 10.1182/blood.2021014588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Wang JJ, Armour BL, Chataway T, et al. Vaccine-induced immune thrombotic thrombocytopenia (VITT) is mediated by a stereotyped clonotypic antibody. Blood. 2022;140(15):1738–1742. doi: 10.1182/blood.2022016474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Leung HHL, Perdomo J, Ahmadi Z, et al. NETosis and thrombosis in vaccine-induced immune thrombotic thrombocytopenia. Nat Commun. 2022;13(1):5206. doi: 10.1038/s41467-022-32946-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Althaus K, Moller P, Uzun G, et al. Antibody-mediated procoagulant platelets in SARS-CoV-2-vaccination associated immune thrombotic thrombocytopenia. Haematologica. 2021;106(8):2170–2179. doi: 10.3324/haematol.2021.279000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Holm S, Kared H, Michelsen AE, et al. Immune complexes, innate immunity, and NETosis in ChAdOx1 vaccine-induced thrombocytopenia. Eur Heart J. 2021;42(39):4064–4072. doi: 10.1093/eurheartj/ehab506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Pomara C, Sessa F, Ciaccio M, et al. Post-mortem findings in vaccine-induced thrombotic thrombocytopenia. Haematologica. 2021;106(8):2291–2293. doi: 10.3324/haematol.2021.279075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Pitkanen HH, Jouppila A, Helin T, et al. COVID-19 adenovirus vaccine triggers antibodies against PF4 complexes to activate complement and platelets. Thromb Res. 2021;208:129–137. doi: 10.1016/j.thromres.2021.10.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Johnston I, Sarkar A, Hayes V, et al. Recognition of PF4-VWF complexes by heparin-induced thrombocytopenia antibodies contributes to thrombus propagation. Blood. 2020;135(15):1270–1280. doi: 10.1182/blood.2018881607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Kanack AJ, Laegreid IJ, Johansen S, Reikvam H, Ahlen MT, Padmanabhan A. Human papilloma virus vaccine and VITT antibody induction. Am J Hematol. 2022;97(10):E363–E364. doi: 10.1002/ajh.26659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Greinacher A, Michels I, Mueller-Eckhardt C. Heparin-associated thrombocytopenia: the antibody is not heparin specific. Thromb Haemost. 1992;67(5):545–549. [PubMed] [Google Scholar]
- 62.Greinacher A, Selleng K, Mayerle J, et al. Anti-platelet factor 4 antibodies causing VITT do not cross-react with SARS-CoV-2 spike protein. Blood. 2021;138(14):1269–1277. doi: 10.1182/blood.2021012938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Uzun G, Althaus K, Bakchoul T. No correlation between anti-PF4 and anti-SARS-CoV-2 antibodies after ChAdOx1 nCoV-19 vaccination. N Engl J Med. 2021;385(14):1334–1336. doi: 10.1056/NEJMc2111305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Schonborn L, Seck SE, Thiele T, Warkentin TE, Greinacher A. SARS-CoV-2 infection in patients with a history of VITT. N Engl J Med. 2022;387(1):88–90. doi: 10.1056/NEJMc2206601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Brodard J, Kremer Hovinga JA, Fontana P, Studt JD, Gruel Y, Greinacher A. COVID-19 patients often show high-titer non-platelet-activating anti-PF4/heparin IgG antibodies. J Thromb Haemost. 2021;19(5):1294–1298. doi: 10.1111/jth.15262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Zheng Y, Wang AW, Yu M, et al. B-cell tolerance regulates production of antibodies causing heparin-induced thrombocytopenia. Blood. 2014;123(6):931–934. doi: 10.1182/blood-2013-11-540781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Barouch DH, Kik SV, Weverling GJ, et al. International seroepidemiology of adenovirus serotypes 5, 26, 35, and 48 in pediatric and adult populations. Vaccine. 2011;29(32):5203–5209. doi: 10.1016/j.vaccine.2011.05.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Dicks MDJ, Spencer AJ, Edwards NJ, et al. A novel chimpanzee adenovirus vector with low human seroprevalence: improved systems for vector derivation and comparative immunogenicity. PLoS One. 2012;7(7) doi: 10.1371/journal.pone.0040385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.McGonagle D, De Marco G, Bridgewood C. Mechanisms of immunothrombosis in vaccine-induced thrombotic thrombocytopenia (VITT) compared to natural SARS-CoV-2 infection. J Autoimmun. 2021;121 doi: 10.1016/j.jaut.2021.102662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Uzun G, Althaus K, Singh A, et al. The use of IV immunoglobulin in the treatment of vaccine-induced immune thrombotic thrombocytopenia. Blood. 2021;138(11):992–996. doi: 10.1182/blood.2021012479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Bourguignon A, Arnold DM, Warkentin TE, et al. Adjunct immune globulin for vaccine-induced immune thrombotic thrombocytopenia. N Engl J Med. 2021;385(8):720–728. doi: 10.1056/NEJMoa2107051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.McFadyen JD, Sharma P, Moon MJ, et al. Activation of circulating platelets in vaccine-induced thrombotic thrombocytopenia and its reversal by intravenous immunoglobulin. Br J Haematol. 2022;196(1):234–237. doi: 10.1111/bjh.17750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Greinacher A, Eichler P, Lietz T, Warkentin TE. Replacement of unfractionated heparin by low-molecular-weight heparin for postorthopedic surgery antithrombotic prophylaxis lowers the overall risk of symptomatic thrombosis because of a lower frequency of heparin-induced thrombocytopenia. Blood. 2005;106(8):2921–2922. doi: 10.1182/blood-2005-05-1824. [DOI] [PubMed] [Google Scholar]
- 74.Warkentin TE. Ischemic limb gangrene with pulses. N Engl J Med. 2015;373(24):2386–2388. doi: 10.1056/NEJMc1511750. [DOI] [PubMed] [Google Scholar]
- 75.Rizk JG, Gupta A, Sardar P, et al. Clinical characteristics and pharmacological management of COVID-19 vaccine-induced immune thrombotic thrombocytopenia with cerebral venous sinus thrombosis: a review. JAMA Cardiol. 2021;6(12):1451–1460. doi: 10.1001/jamacardio.2021.3444. [DOI] [PubMed] [Google Scholar]
- 76.Pavord S, Lester W, Hunt BJ. Clinical features of VITT. Reply. N Engl J Med. 2022;386(1):95–96. doi: 10.1056/NEJMc2118473. [DOI] [PubMed] [Google Scholar]
- 77.Patriquin CJ, Laroche V, Selby R, et al. Therapeutic plasma exchange in vaccine-induced immune thrombotic thrombocytopenia. N Engl J Med. 2021;385(9):857–859. doi: 10.1056/NEJMc2109465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Major A, Carll T, Chan CW, et al. Refractory vaccine-induced immune thrombotic thrombocytopenia (VITT) managed with delayed therapeutic plasma exchange (TPE) J Clin Apher. 2022;37(1):117–121. doi: 10.1002/jca.21945. [DOI] [PubMed] [Google Scholar]
- 79.Tiede A, Sachs UJ, Czwalinna A, et al. Prothrombotic immune thrombocytopenia after COVID-19 vaccination. Blood. 2021;138(4):350–353. doi: 10.1182/blood.2021011958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Panagiota V, Dobbelstein C, Werwitzke S, et al. Long-term outcomes after vaccine-induced thrombotic thrombocytopenia. Viruses. 2022;14(8) doi: 10.3390/v14081702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.von Hundelshausen P, Lorenz R, Siess W, Weber C. Vaccine-induced immune thrombotic thrombocytopenia (VITT): targeting pathomechanisms with Bruton tyrosine Kinase inhibitors. Thromb Haemost. 2021;121(11):1395–1399. doi: 10.1055/a-1481-3039. [DOI] [PubMed] [Google Scholar]
- 82.Lacy J, Pavord S, Brown KE. VITT and second doses of Covid-19 vaccine. N Engl J Med. 2022;386(1):95. doi: 10.1056/NEJMc2118507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Favaloro EJ, Pasalic L, Henry B, Lippi G. Laboratory testing for platelet factor 4 antibodies: differential utility for diagnosis/exclusion of heparin induced thrombocytopenia versus suspected vaccine induced thrombotic thrombocytopenia. Pathology. 2022;54(3):254–261. doi: 10.1016/j.pathol.2021.10.008. [DOI] [PubMed] [Google Scholar]
- 84.Pavord S, Hunt BJ, Horner D, Bewley S, Karpusheff J. Vaccine induced immune thrombocytopenia and thrombosis: summary of NICE guidance. BMJ. 2021;375:n2195. doi: 10.1136/bmj.n2195. [DOI] [PubMed] [Google Scholar]