

Abstract
Many adults express interest in e-cigarette cessation; however, there are few empirically tested interventions for quitting vaping. This study seeks to 1) to evaluate reasons for quitting e-cigarettes in treatment-seeking adults, and 2) to assess the feasibility and acceptability of nicotine replacement therapy (NRT) for e-cigarette cessation. Adult daily e-cigarette users completed qualitative interviews about quitting e-cigarettes, then were randomized to either 28-day supply of combination NRT (21mg patches, 4mg lozenges) + supportive booklet or Quitline referral. Primary aims were feasibility (number who enrolled) and acceptability (NRT use, adverse side effects). Exploratory aims evaluated abstinence (7-day point-prevalence) at end of treatment. Of the 30 participants who were enrolled, 50% (n=15) were dual users, and 50% (n=15) were mono-vapers, 26.6% (n=8) of whom were former smokers. Participants reported seeking treatment due to health concerns, dependence, stigma, and cost. Anticipated challenges of quitting vaping were withdrawal, negative mood, sensorimotor habits, and convenience. Most completed the end of treatment survey (n=24; 80%). Participants who received NRT reported using the patch M=10.89 days and lozenges M=6.39 days, with few days of adverse effects (M=2.67). At end of treatment, 6/18 (33.3%; 6 mono and 0 dual users) in the intervention group reported abstinence from vaping, compared to 0 in the control group (Fisher=5.00, p=.057). In conclusion, adults are interested in quitting e-cigarettes due to negative consequences of use and are willing to use pharmacotherapy. Future research should confirm these results in a larger trial, address cigarette smoking in dual users, and aim to disseminate treatments.
Keywords: e-cigarette, vaping, cessation, nicotine replacement therapy, qualitative, pilot study
1.0. INTRODUCTION
With the significant increase and proliferation of e-cigarettes in the tobacco marketplace1, prevalence of e-cigarette use is estimated to be 3.7% as of 20202. Among adults who vape, about 54% concurrently smoke cigarettes, 31% smoked in the past, and 15% never smoked cigarettes3. Nicotine is an addictive stimulant4, and many youth who use e-cigarettes report symptoms of dependence5, such as cravings, tolerance, habitual vaping, and inability to track consumption due to accessibility and convenience6,7. Dependence symptoms in adults are less well understood; however, many report perceived negative health effects8–15, cost concerns10,16–18, and withdrawal19. Individuals who use e-cigarettes may be prompted to consider cessation due to dependence and other negative consequences. Indeed, national survey data suggest that 60.7% of adults are interested in quitting e-cigarettes, with 15.7% endorsing a past year quit attempt3. Highest intention to quit is seen among those who smoked in the past, whereas highest prevalence of past year quit attempts is among those who never smoked.
Although many individuals report interest in quitting, there are very few empirically tested interventions to address e-cigarette cessation. One study of text-message support20, two using contingency management21,22, and one using counseling, nicotine replacement therapy (NRT), and nicotine tapering23 have shown promise for quitting vaping. The text-message program20,24 was the only fully-powered randomized controlled trial, which provided behavioral support via text to youth and young adults interested in quitting vaping and self-reported abstinence at the end of the program. Two case studies also show support for NRT for vaping cessation25,26. Importantly, the aforementioned studies were tailored for youth and young adults (ages 17–31). Limited research has been conducted evaluating methods for e-cigarette cessation among the general adult population. Additionally, there is a lack of treatment resources specifically addressing dual users of cigarettes and e-cigarettes, which is a common and troubling phenomenon given the health consequences of continued combustible cigarette smoking19,27. Finally, there is concern that quitting e-cigarettes may lead to increased smoking in dual users, or put individuals who used to smoke at risk of relapse28. No longitudinal research exists to examine these effects.
The purpose of the present study is to address these gaps through 1) a qualitative analysis of reasons for quitting e-cigarettes in treatment-seeking adults and 2) an investigation of the feasibility and acceptability of NRT plus supportive written materials for e-cigarette cessation through a preliminary clinical trial. The results of this study aim to inform e-cigarette interventions for the general adult population by evaluating motivators and barriers for quitting as well as gaining a preliminary appraisal into the application of an established smoking cessation treatment for vaping cessation.
2.0. METHODS
2.1. Participants
Participants were recruited to the study via online advertisements (Craigslist) across South Carolina. Advertisements were tailored explicitly for both e-cigarette-only (mono) users and dual-users interested in quitting such that equal numbers of mono- (n=15) and dual-users (n=15) were recruited. Participants were given a link to an online survey via REDCap29 to determine study eligibility, and all participants were screened over the phone to confirm. Randomization was stratified by cigarette smoking status (e-cigarette-only OR cigarette smoking ≥1x per week [dual user]).
Inclusion criteria included 1) age 18+; 2) daily nicotine-containing e-cigarette use (25+ days per month); 3) vaping 5+ times/day; 4) vaping ≥ 1 year; 5) interest in quitting vaping [and smoking, for dual users] within the next month (≥7 on 10-point scale); 6) willingness to try NRT; 7) able to receive text messages and to complete interviews over the phone or via video software; and 8) live in South Carolina. Exclusion criteria included participants who were pregnant or not using contraception, cognitively impaired, household members of study participants, used any other non-cigarette tobacco product or cessation medication, or endorsed a current medical condition that was contraindicated for NRT use.
2.2. Study Procedures
The study was approved by the Institutional Review Board. Participants who were eligible scheduled a video meeting with research staff where informed consent was obtained. All participants then completed a qualitative interview and baseline assessments. Finally, participants were randomized into study group at a target ~2:1 ratio; however, due to the small sample size, this exact ratio was not achieved: Intervention (n=18), Control (n=12).
Participants assigned to the Intervention condition were asked to pick a day to quit vaping (and smoking, if applicable) within 1 week. Participants were then mailed a 28-day supply of 21 mg nicotine patches, 4 mg lozenges, and a support booklet. The support booklet was developed by modifying the existing booklet utilized by the MUSC Tobacco Treatment Program which was based on cognitive-behavioral therapy skills30. For the present intervention, text was adapted to provide skills for e-cigarette cessation or dual product cessation, resulting in two separate booklets for each type of participant (one for mono-users detailing e-cigarette cessation, one for dual users detailing both smoking and e-cigarette cessation). On the specified quit day, participants received a supportive text message (“Today is your quit date! Make sure to use your medications and written materials to help you. You got this!”). After this, participants received daily surveys via text message over the course of 28 days.
Participants in the Control condition were provided with information about how to contact the SC Quitline (call, text, online)31 and were encouraged to enroll in services within 1 week. Participants were told that the quitline offered pharmacotherapy, an e-cigarette cessation protocol32, and smoking cessation support if applicable. Given that the purpose of the study was to evaluate the feasibility and acceptability of the intervention described, the control group did not complete daily surveys.
At the end of treatment (EOT; Day 28) and follow-up (FU; Day 56), all participants received text message survey links to complete assessments. Participants were compensated $20 for each assessment completed (baseline, Day 28, Day 56; maximum $60). Participants in the Intervention condition were compensated an additional $60 for completing daily surveys, based on the number completed (i.e., 1 completed = $10, 14 = $40, 28 = $60). All payments were in the form of electronic gift cards.
2.3. Measures
2.3.1. Qualitative Interviews
Prior to trial onset, participants engaged in a brief interview over video software regarding their interest in the study. Participants were asked 1) “Tell me about why you are interested in quitting e-cigarettes (and cigarettes, if applicable).”; 2) “Have you talked to a medical professional about your e-cigarette use? What was that like/what do you think it would be like?”; and 3) “What do you think the challenges will be when quitting e-cigarettes (and smoking)?” Interviews were audio recorded.
2.3.2. Baseline and Follow-up Assessments
Participants completed questionnaires assessing demographics, current/past e-cigarette use characteristics, and current/past cigarette smoking characteristics (if applicable). E-cigarette dependence was measured with the Penn State Electronic Cigarette Dependence Inventory (ECDI; score range 0–20)33, current withdrawal symptoms was measured using the Brief Wisconsin Inventory of Smoking Dependence Motives (WISDM; total score range = 11–77) adapted to ask about e-cigarettes34, and reinforcing effects of e-cigarettes were measured using the Vaping Consequences Questionnaire (VCQ; Negative Consequences, Positive Reinforcement, Negative Reinforcement, and Weight Control subscales score range 0–9)35. At EOT and FU, measures related to e-cigarette use and cigarette smoking were readministered.
2.3.3. Daily Surveys
Daily surveys sent to participants randomized into the intervention group were asked to self-report (yes/no) e-cigarette use, cigarette use, quit attempts for either product, and NRT use. Finally, participants were able to report adverse events (e.g., common symptoms) of NRT use.
2.4. Outcomes
2.4.1. Feasibility and Acceptability
Feasibility was assessed by 1) the number of participants who reported interest in the study and enrolled; 2) the number of participants who completed the EOT and follow-up visits; and 3) the number of daily surveys completed. Acceptability was assessed by uptake of NRT use as well as reported adverse side effects.
2.4.2. Abstinence and Quit Attempts
Vaping and smoking abstinence at EOT and FU were determined by self-reported 7-day point prevalence abstinence. Vaping and smoking reduction were determined by subtracting the current days of use at EOT and FU from the baseline, and categorizing responses into 1) increased; 2) decreased; or 3) no change. Missing data were imputed as vaping/smoking (not abstinent) or no attempt to quit or reduce vaping36.
2.5. Analysis
2.5.1. Qualitative Analysis
Interview recordings were transcribed and the qualitative analysis was conducted using Taguette37. To begin, an initial set of codes were generated a priori based on the interview questions and a cursory review of transcripts. A subset (~20%) of transcripts were coded by three independent coders, and following completion, coders conferred to revise the codebook and discuss discrepancies. Once a final codebook was agreed upon, each transcript was coded by two coders. Tagged quotes were merged and compared for reliability among coders and discrepancies were discussed to obtain consensus.
2.5.2. Feasibility, Acceptability, and Outcomes
Descriptive statistics for sample characteristics, feasibility, and acceptability were computed. Fisher’s tests were used to determine differences in proportions of participants who were abstinent between treatment groups. Exploratory analyses included the comparison of mono- versus dual users as well as an evaluation of the daily survey data between those in the treatment group who quit and those who did not.
3.0. RESULTS
3.1. Participants
Figure 1 shows the CONSORT flow diagram. From June through December 2021, 196 participants expressed interest in the study which allowed for a final enrolled sample of 30 participants.
Figure 1.
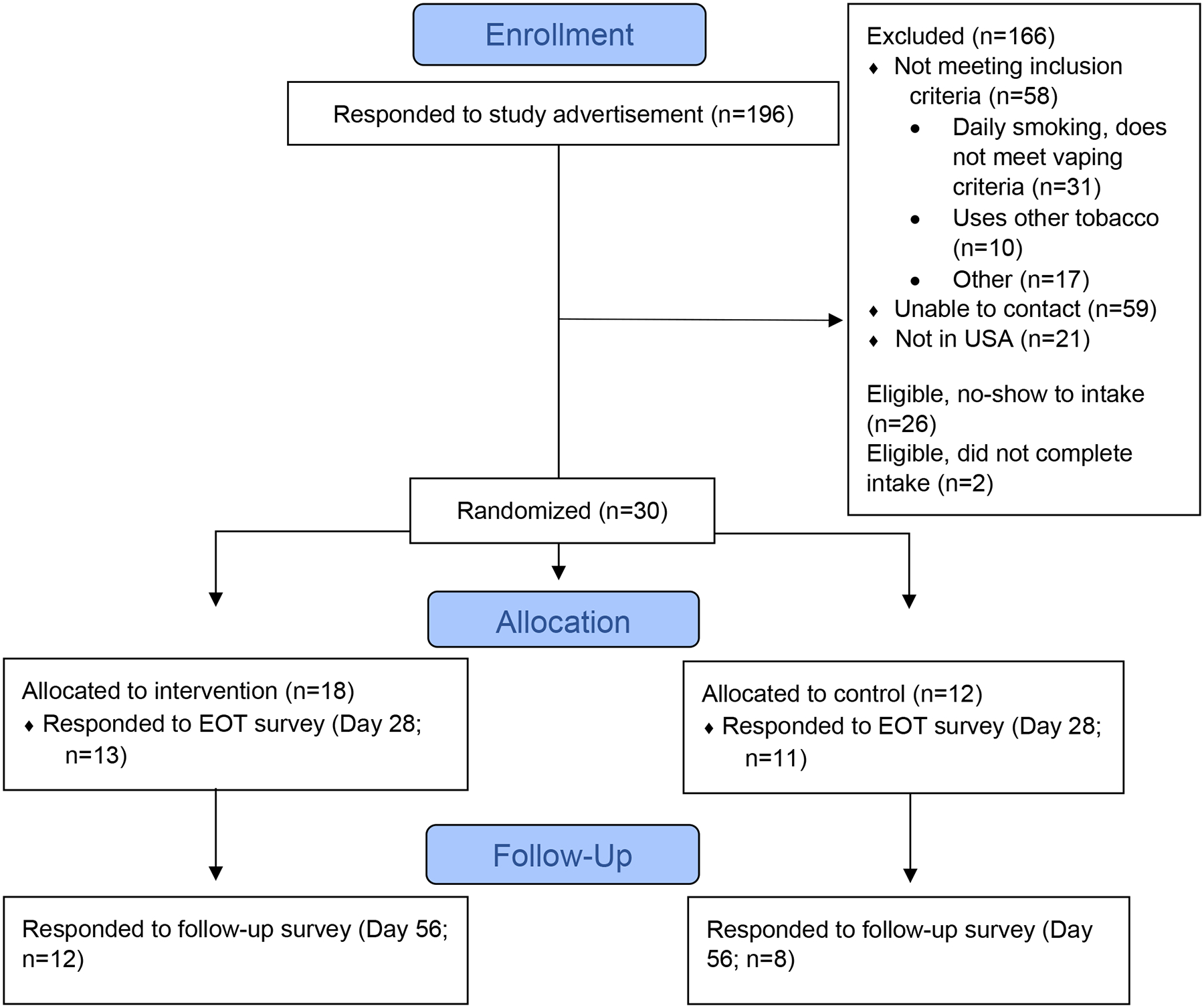
CONSORT flow diagram.
Participant demographics, vaping characteristics, and smoking characteristics can be seen in Table 1. The average age of participants was 32; 50% male; 33.3% identified as a racial or ethnic minority. A majority of participants endorsed vaping continuously all day (76.6%) and using a nicotine content of 50mg/ml/5% or higher (66.6%). Among mono users, 53.3% endorsed a history of regular cigarette smoking. Most current dual users (80%) reported smoking 10 cigarettes or less per day. Participants reported moderate nicotine dependence as evidenced by Brief WISDM total score (M=48.06) and ECDI score (M=13.83).
Table 1.
Participant demographics, vaping characteristics, and smoking characteristics.
| Intervention (N=18) | Control (N=12) | Full Sample | |||
|---|---|---|---|---|---|
| E-cigarette only (N=10) | Dual User (N=8) | E-cigarette only (N=5) | Dual User (N=7) | ||
| Age (mean, SD) | 28 (7) | 33 (11) | 32 (11) | 37 (15) | 32 (11) |
| Range: 20–59 | |||||
| Gender identity (N, %) | |||||
| Male | 3 (30%) | 6 (75%) | 4 (80%) | 2 (28.5%) | 15 (50%) |
| Female | 7 (70%) | 2 (25%) | 1 (20%) | 5 (71.4%) | 15 (50%) |
| Race or Ethnicity (N, %) | |||||
| Native American/Alaskan Native | 1 (10%) | 0 | 0 | 0 | 1 (3.3%) |
| Black/African American | 2 (20%) | 0 | 1 (20%) | 3 (42.8%) | 6 (20%) |
| Hispanic | 1 (10%) | 1 (12.5%) | 0 | 0 | 2 (6.6%) |
| South Asian | 0 | 0 | 1 (20%) | 0 | 1 (3.3%) |
| White | 6 (60%) | 7 (87.5%) | 3 (60%) | 4 (57.1%) | 20 (66.6%) |
| Marital Status (N, %) | |||||
| Single, never married | 6 (60%) | 5 (62.5%) | 3 (60%) | 4 (57.1%) | 18 (60%) |
| Married/Partnered | 3 (30%) | 1 (12.5%) | 1 (20%) | 0 | 5 (16.6%) |
| Divorced/Widowed | 1 (10%) | 2 (25%) | 1 (20%) | 3 (42.8%) | 7 (23.3%) |
| Highest Education (N, %) | |||||
| High School or less | 3 (30%) | 4 (50%) | 0 | 3 (42.8%) | 10 (33.3%) |
| Beyond high school | 7 (70%) | 4 (50%) | 5 (100%) | 4 (57.1%) | 20 (66.6%) |
| Household Income (N, %) | |||||
| <$50,000 | 9 (90%) | 8 (100%) | 2 (40%) | 4 (57.1%) | 23 (76.6%) |
| ≥$50,000 | 1 (10%) | 0 | 3 (60%) | 3 (42.8%) | 7 (23.3%) |
| # E-cig uses/day (M, SD) | 29.30 (24.21) | 72.88 (80.64) | 29.00 (15.17) | 23.57 (34.51) | 39.53 (49.53) |
| Vape continuously all day (N,%) | 6 (60%) | 7 (87.5%) | 4 (80%) | 6 (85.7%) | 23 (76.6%) |
| Disposable device (N, %) | 4 (40%) | 3 (37.5%) | 1 (20%) | 3 (42.8%) | 11 (36.6%) |
| Nicotine Content (N, %)a | |||||
| <50mg/ml, 5% | 2 (20%) | 4 (50%) | 1 (20%) | 3 (42.8%) | 10 (33.3%) |
| ≥50mg/ml, 5% | 7 (70%) | 4 (50%) | 4 (80%) | 4 (57.1%) | 20 (66.6%) |
| Flavor (N, %) | |||||
| Tobacco/Menthol | 5 (50%) | 3 (37.5%) | 2 (40%) | 5 (71.4%) | 15 (50%) |
| Fruit/Other | 5 (60%) | 5 (62.5%) | 3 (60%) | 2 (28.5%) | 15 (50%) |
| Past e-cig quit attempt (N,%) | 6 (60%) | 3 (37.5%) | 3 (60%) | 6 (85.7%) | 18 (60%) |
| Former Smokers (N, %) | 6 (60%) | - | 2 (40%) | - | 8/15 (53.3%) |
| # Smoking days/week (M, SD)b | 6 (2) | 4 (3) | 6 (2) | 5 (3) | - |
| Cigarettes per day (N, %)b | - | ||||
| 0–10 | 3 (50%) | 7 (87.5%) | 1 (50%) | 5 (71.4%) | |
| 11–20 | 2 (33.3%) | 0 | 1 (50%) | 1 (14.2%) | |
| 21+ | 1 (16.6%) | 1 (12.5%) | 0 | 1 (14.2%) | |
| Time to first cigarette (N, %)b | - | ||||
| ≤5 minutes | 2 (33.3%) | 3 (37.5%) | 0 | 4 (57.1%) | |
| >6 minutes | 4 (66.6%) | 5 (62.5%) | 2 (100%) | 3 (42.8%) | |
| WISDM total score (M, SD) | 50.10 (12.89) | 52.81 (8.14) | 37.93 (15.19) | 46.93 (15.04) | 48.06 (13.11) |
| ECDI total score (M, SD) | 14.40 (4.48) | 14.88 (3.64) | 11.60 (5.37) | 13.43 (3.74) | 13.83 (4.19) |
| VCQ (M, SD) | |||||
| Negative Consequences | 5.59 (1.96) | 5.72 (2.80) | 4.40 (2.71) | 5.93 (1.72) | 5.51 (2.23) |
| Positive Reinforcement | 5.36 (1.91) | 5.85 (2.06) | 3.56 (2.51) | 5.89 (1.94) | 5.31 (2.12) |
| Negative Reinforcement | 6.16 (1.87) | 6.20 (1.82) | 5.00 (1.82) | 6.27 (1.78) | 6.00 (1.79) |
| Weight Control | 6.56 (1.27) | 2.00 (4.80) | 4.80 (2.33) | 5.97 (1.63) | 5.95 (1.77) |
Notes:
missing data due to response of “don’t know.”
Ns/% in “e-cigarette only” columns reflect former smokers, who were asked about the past.
3.2. Qualitative Interviews
Table 2 provides themes and sample quotations from interviews (n=28; two interviews were unable to be transcribed). In response to “Tell me about why you are interested in quitting e-cigarettes (and cigarettes, if applicable)”, major themes emerged surrounding health, cost, perceptions of friends and family, negative consequences of dependence, and stigma. All (n=28) participants acknowledged that there were detrimental effects of vaping on health, largely related to nicotine exposure and unknown long-term effects. Dual users had substantial health concerns regarding the known effects of cigarette smoking and the potential additive effects of vaping. Many (n=19) also noted that cost was a motivating factor to quit, and some participants suggested the financial costs were comparable to cigarette smoking. Disapproval from friends and family were also highly motivating for participants (n=17). Many discussed feeling the need to hide their e-cigarette use from others and negative consequences once loved ones found out. Many (n=19) participants endorsed discontent with being dependent on e-cigarettes, noting that they find themselves using more than desired and not being in control of their vaping. Finally, n=22 participants discussed repercussions from stigma associated with vaping. Some individuals (n=8) endorsed problems at work as a result of continued e-cigarette use.
Table 2.
Interview themes and sample quotes
| Prompt | Theme | Quotes |
|---|---|---|
| “Tell me about why you are interested in quitting e-cigarettes (and cigarettes, if applicable)” | Health |
“I’m interested in quitting because of health concerns that I know that it is damaging to my body. The area where I notice it the most is my lung capacity and my ability to exercise is limited. And I think that would benefit hugely from finding a way to quit.” 28-year-old white male, mono user “Just the concept of like sucking out a device and blowing it. And I’m the same way. I mean it’s just gross. And you’re inhaling it, and I know what’s in it. And I just know that it’s unhealthy. And I’m in the medical field, so I know how bad it is. I tell my patients not to do it, and I go and do it…I have acne from it. I have a sensitivity to the propylene glycol, and so I get like cystic acne. I’ve been having hair loss since I started it. Obviously with COVID, the susceptibility and the whole popcorn lung and everything. I just know that it’s really bad, and then obviously like the flavorings and stuff.”28-year-old white female, former smoker “I thought it was an alternative to try to quit smoking as much nicotine, but they make me cough a lot. It’s like they make my chest hurt sometimes.” 28-year-old white female dual user |
| Cost |
“I thought it was gonna be cheaper, but in all actuality I’m still spending - so it’s $20.00 for my refills, and I’m still spending that four times a week sometimes. That’s a lot; it’s not cheaper” 37-year-old white female, former smoker
“And the financial aspect, you know, it’s a pretty useless thing to be spending money on.”26-year-old white male, former smoker |
|
| Family/Friends |
“And if my family knew that I did it, they’d be like ashamed. And I know that my husband hates it, and he’s thrown out my device several times. And we have arguments about it. And so I have to do it in like private, so it’s like a shameful thing for me to do.” 28-year-old white female, former smoker
“My parents begged, begged, begged me to quit” 22-year-old white female, mono user |
|
| Dependence |
“[After quitting smoking], instead of like what you’re supposed to do, go down in nicotine and try to wean yourself off, I literally stayed at the same one…I think I vape more than I smoked cigarettes” 32-year-old white female, former smoker
“I don’t want to be dependent on any cigarettes or e-cigarettes.” 49-year-old Hispanic male, dual user |
|
| Stigma | “And that’s kind of what got me in trouble at work. I kind of hide the JUUL, but I was puffing away on that and there’s a lot more smoke with it and the boss saw it and he wasn’t too happy. You know, I said, ‘I don’t want to lose this job. It’s a beautiful job,’ and it’s like, ‘Why do I keep doing that?’” 58-year-old white female, dual user | |
| “Have you talked to a medical professional about your e-cigarette use? What was that like/what do you think it would be like?” | Stigma |
“They just didn’t really like – they didn’t care as much which was what made me feel weird about it. They didn’t really want to refer any hotlines or anything… they didn’t really provide any help, they just said you should quit.” 23-year-old Hispanic female, mono user
“I kind of like didn’t tell them how much I was smoking… the doctor was really hard on me about the vape. He said that they are really worse than cigarettes, like, cigarettes are bad too, but he was telling me that a vape is really, really bad.”28-year-old white female, dual user |
| Support |
“She’s not a fan of any kind of nicotine use at all but at least this was a start headed in the right direction, so she kind of basically left it right there. She was like ‘Oh, I’m glad. I’m glad you’ve taken a pathway to want to quit completely.’ So, that’s how she left it”. 50-year-old Black male, former smoker
“The doctor that I talked to when I asked about Chantix, she was very understanding. She wasn’t judgmental. I felt comfortable. I imagine I wouldn’t with all doctors, but she was pretty chill.” 33-year-old South Asian male, former smoker |
|
| Ambivalence | “They all ask you when you first go in, you know, ‘Do you drink? Do you smoke? Do you do this or that?’ And I mean it really doesn’t go farther than just telling that I used to smoke and now I vape. It really hasn’t gone farther, and honestly I really haven’t had any health concerns that would make me need anyone’s guidance on that.”30 year-old Native American female, former smoker | |
| “What do you think the challenges will be when quitting e-cigarettes (and smoking)?” | Accessibility | “The cost and the convenience. I save a lot of money using this as opposed to smoking cigarettes. This is really affordable…This is accepted in restaurants or in stores. I can just vape away and nothing is said. So, I’m not breaking any laws.” 50-year-old Black male, former smoker |
| Social situations | “I believe the biggest challenge will probably be just having to not be around [my girlfriend] when she does it. I’ll let her know, ‘If you’re going to do it, make sure you’re away from me and I don’t see you do it, because I don’t want to watch you do something that I really want to do.’” 20-year-old white male, former smoker | |
| Mood | “Just the thought of not having it. It’s been such a crutch my whole life. Whenever I’m stressed out or anxious, even if it doesn’t really make me feel better, I guess I’m tricking myself, like a placebo type effect. It’s just like a security blanket to me.” 27-year-old white male, dual user | |
| Sensorimotor/Habit | “I think I kind of have less of a nicotine problem and more of a mouth fixation problem…Like, I go to hit something all of the time. It’s like something I do in between activities, like, I feel like it’s going to be hard for me to like shake that.”21-year-old white female, dual user | |
| Withdrawal | “[When I’ve stopped vaping in the past] I was ungodly agitated and irritable. And everything bothered me. And my mood was just really bad. And I was tired, and I had body aches. I was sweating at night. It was really bad.” 28-year-old white female, mono user |
When asked “Have you talked to a medical professional about your e-cigarette use? What was that like/what do you think it would be like?”, participants reported mixed feelings about the encounters. Some (n=13) reported that their healthcare providers had negative viewpoints about e-cigarette use and felt admonished after disclosing their vaping. On the other hand, others (n=9) reported that their doctors were supportive of their e-cigarette use if it was a means to reduce cigarette smoking.
Participants were asked “What do you think the challenges will be when quitting e-cigarettes (and smoking)?” Major themes that emerged included habitual and sensorimotor factors, social situations, nicotine withdrawal, mood symptoms, and convenience. Many participants (n=17) endorsed that e-cigarette use was a habit embedded into their everyday activities, noting that the sensorimotor aspects of vaping felt automatic. Participants described feeling discomfort when being without their e-cigarette (n=17), some (n=15) endorsing mood symptoms such as anxiety or stress. Participants (n=18) also reported that being around others who vape would pose a challenge when trying to quit. Some individuals (n=17) described withdrawal symptoms from previous times when they were without e-cigarettes or had tried to quit vaping, similar to cigarette withdrawal: headaches, nausea, irritability, anxiety, and sleep disturbance. Dual users reported a similar concern regarding their dependence on nicotine from both products. Finally, participants (n=10) noted that the ease of accessibility and use of e-cigarettes would make it hard to break the habit.
3.3. Feasibility and Acceptability
Participants in the intervention group completed, on average, 19.61 daily surveys (SD = 8.63) throughout the 28-day treatment (70.0%). Within these survey responses, participants reported using NRT an average of 12.78 days (SD=10.14; patch M = 10.89 days [SD=9.98]; lozenges M= 6.39 days [SD=7.11]; combined use M = 4.50 days [SD=6.40]). Participants reported few days with adverse side effects from the NRT (M=2.67, SD=4.99). A majority of participants completed the EOT survey (80%) and a large number completed the FU survey (66.6%). Those with missing data had vaping and smoking status imputed as not abstinent. These results are shown by intervention group in Table 3.
Table 3.
Abstinence outcomes
| Intervention (N=18) | Control (N=12) | Intervention vs Control Fisher, p, φ |
|||||
|---|---|---|---|---|---|---|---|
| E-cigarette only (N=10) | Dual Use (N=8) | Overall | E-cigarette only (N=5) | Dual User (N=7) | Overall | ||
| End of Treatment (Day 28) | |||||||
| Completed survey | 8 (80%) | 5 (62.5%) | 13 (72.2%) | 4 (90%) | 7 (100%) | 11 (91.6%) | - |
| E-cigarette abstinencea | 4 (40%) | 2 (25%) | 6 (33.33%) | 0 | 0 | 0 | 5.00, .057, −.408 |
| Increased | 0 | 0 | 0 | 0 | 0 | 0 | |
| Smoking abstinencea | - | 0 | 0 | - | 0 | 0 | - |
| Increased | 0 | 0 | 0 | 0 | 1 (14.2%) | 1 (6.7%) | |
| Intervention Group b | |||||||
| # surveys completed | 21.00 (6.15) | 17.88 (11.23) | 19.61 (8.63) | - | - | - | - |
| # days vapingc | 6.50 (8.29) | 6.88 (8.32) | 6.67 (8.06) | - | - | - | - |
| # days smokingc | .10 (.32) | 6.63 (10.53) | 3.00 (7.54) | - | - | - | - |
| # days attempting to quit vapingc | 18.10 (8.43) | 12.25 (10.42) | 9.30 (10.64) | - | - | - | - |
| # days attempting to quit smokingc | - | 3.75 (7.42) | 1.03 (4.01) | - | - | - | - |
| # days using any NRTc | 15.20 (9.58) | 9.75 (10.63) | 12.78 (10.14) | - | - | - | - |
| # days using NRT patchc | 12.50 (9.37) | 8.87 (10.99) | 10.89 (9.98) | - | - | - | - |
| # days using NRT lozengec | 7.20 (9.37) | 8.87 (10.99) | 6.39 (7.11) | - | - | - | - |
| # days using combined NRTc | 4.50 (5.16) | 4.50 (8.07) | 4.50 (6.40) | - | - | - | - |
| # days endorsing AEc | 4.50 (6.20) | .38 (.52) | 2.67 (4.99) | - | - | - | - |
| Follow-up (Day 56) | |||||||
| Completed survey | 8 (80%) | 4 (50%) | 12 (66.6%) | 3 (60%) | 5 (71.4%) | 8 (66.6%) | - |
| E-cigarette abstinencea | 3 (30%) | 2 (25%) | 5 (27.78%) | 1 (20%) | 1 (14.2%) | 2 (16.66%) | .49, .669, −.129 |
| Increased | 0 | 0 | 0 | 0 | 0 | 0 | |
| Smoking abstinencea | - | 0 | 0 | - | 0 | 0 | - |
| Increased | 0 | 0 | 0 | 0 | 1 (14.2%) | 1 (6.7%) | |
Notes:
7-day point-prevalence via self-report.
No significant differences were found between smoking status on these variables.
Among responders only.
3.4. Abstinence Outcomes
Table 3 shows abstinence outcomes by group, with non-responders imputed as not abstinent. Among those in the intervention group, 6 (33.3%) reported abstinence from vaping at EOT, whereas 0 participants in the control group endorsed abstinence (Fisher statistic = 5.00, p=.057, φ = −.408). At FU, 5 participants (27.7%; 4/6 that were abstinent at EOT) in the intervention group remained abstinent from vaping whereas 2 (16.66%) in the control group endorsed quitting vaping. Within those who continued to vape at EOT and FU, 5 participants in the treatment group (5/12; 41.67%) and 4 participants in the control group (33.33%) endorsed reducing e-cigarette use. Among dual users, no participants in either treatment group reported abstinence from cigarettes at either endpoint. At EOT, 2 participants had reduced smoking (13.3%) and 1 increased (6.6%). At follow-up, 4 reduced smoking (26.67%) and 1 increased (6.67%). Importantly, no mono users endorsed initiating or returning to cigarette smoking.
Table 4 shows differences in self-reported treatment engagement and outcomes between those who quit vaping and those who did not. Participants in the intervention group who quit vaping reported making an active quit attempt on significantly more days (M=23.17, SD=3.31) than those who did not quit (M=5.83, SD=8.81, t=−7.70, p<.001). Those who quit also reported significantly more days using NRT (M=22.66, SD=2.87; patches [M=19.50, SD=4.76]; lozenges [M=11.33, SD=7.06] than those who did not quit (NRT days M=7.83, SD=8.67, t=−5.36, p<.001; patch days M=6.58, SD=9.11, t=−3.23, p<.001; lozenge days M=3.91, SD=5.96, t=−2.34, p<.05). Table 4 also shows vaping outcomes crossed with smoking outcomes among those with dual use, former smoking, and never smoking histories. No dual users who quit e-cigarettes had increased their smoking at either EOT or FU.
Table 4.
Smoking outcomes and treatment effects by e-cigarette abstinence
| E-cigarette Abstinence | |||
|---|---|---|---|
| EOT (Day 28) | Abstinent (N=6) | Not abstinent (N=24) | Abstinent vs Not T or Fisher, p, d or φ |
| Smoking change | 2.01, .501, .217 | ||
| Reduced | 1 | 1 | |
| No change | 5 | 22 | |
| Increased | 0 | 1 | |
| Intervention (N=18) | Abstinent (N=6) | Not abstinent (N=12) | |
| # e-cigarette quit attempt daysa | 23.16 (3.31) | 11.66 (9.37) | −3.8, <.001, −1.44 |
| # days using any NRTa | 22.67 (2.88) | 7.83 (8.67) | −5.36, <.001, −2.01 |
| # days using NRT patcha | 19.50 (4.76) | 6.58 (4.76) | −3.23, <.01, −1.61 |
| # days using NRT lozengea | 11.33 (7.06) | 3.91 (5.96) | −2.35, <.05, −1.17 |
| # days using combined NRTa | 8.16 (6.49) | 2.66 (5.75) | −1.83, .08, −0.92 |
| Follow-up (Day 56) | Abstinent (N=7) | Not abstinent (23) | |
| Smoking change | 2.27, .416, .261 | ||
| Reduced | 2 | 2 | |
| No change | 5 | 20 | |
| Increased | 0 | 1 | |
| E-cigarette Change | ||||
|---|---|---|---|---|
| Smoking Change Categorized by Smoking History | Quit | Reduced | No change | Increased |
| Dual Use | ||||
| Reduced | 1 | 3 | 0 | 0 |
| No change | 1 | 2 | 7 | 0 |
| Increased | 0 | 1 | 0 | 0 |
| Former Smoking | ||||
| Reduced | 0 | 0 | 0 | 0 |
| No change | 2 | 1 | 5 | 0 |
| Increased | 0 | 0 | 0 | 0 |
| Never Smoking | ||||
| Reduced | 0 | 0 | 0 | 0 |
| No change | 2 | 2 | 3 | 0 |
| Increased | 0 | 0 | 0 | 0 |
Notes:
Among responders only.
4.0. DISCUSSION
This preliminary clinical trial sought to evaluate 1) interest and motivations for vaping cessation among adults, and 2) the feasibility and acceptability of NRT alongside a supportive booklet for e-cigarette cessation among mono- and dual-user adults motivated to quit. The small sample recruited for this pilot study presents clear limitations that reduce the generalizability and interpretability of the results. However, given the lack of empirically supported interventions for e-cigarette cessations, especially among adults and dual users, these data represent an important exploratory contribution that can guide future treatment interventions.
As a measure of feasibility, a large number of individuals in the community expressed interest in the study over the short course of study duration. This is especially significant in that equal numbers of dual users and e-cigarette only users, including former cigarette smokers, were recruited. This demonstrates that these individuals are in need of treatment interventions to support nicotine cessation. The remote procedures were an advantage for recruitment, allowing participants to complete all study visits from where they were located, which increased reach and representativeness in the sample. Once enrolled, a majority engaged in the treatment and completed the follow-up surveys. Overall, these findings add support to the nascent body of work being conducted to develop, test, and disseminate effective e-cigarette cessation treatments. On the other hand, results are somewhat suggestive of survey response burden for those in the intervention group. At EOT 92% (11/12) of control participants responded to the survey, whereas only 72.2% (13/18) of intervention participants responded. It should be noted that these measures may better represent feasibility of a cessation trial and may not fully capture feasibility of engaging in the intervention. Future trials should be designed with more rigorous feasibility assessment in mind, which will aid dissemination of treatments.
Consistent with previous literature4,5,8–18, participants discussed several negative consequences of vaping that motivated them to seek treatment. Namely, acute and distal health concerns, dependence, social stigma, and cost. Many of these factors overlap with negative consequences of cigarette smoking. This evidence is encouraging in that the overlap of motivational factors for quitting smoking may also be applied to e-cigarette and dual use cessation treatments. The combined negative consequences from dual product use may be especially salient to encourage users to completely quit nicotine. Finally, motivational enhancement strategies might be able to capitalize on these negative outcomes to promote e-cigarette cessation among those who may be experiencing some of these consequences of vaping.
Another important finding from the qualitative analysis was that participants reported mixed messages from healthcare providers about quitting vaping. This might be a result of the different smoking histories that participants presented to their providers with. That is, there is no standard set of recommendations available to providers who are presented with patients at various stages of the tobacco use spectrum. Participants also discussed a number of barriers and challenges related to quitting vaping, including withdrawal symptoms, changes in mood, sensorimotor habits, and convenience. Overall, these results show that there are several treatment gaps to be filled. To begin, treatment interventions and consistent cessation guidelines should be rapidly disseminated to a variety of providers in the healthcare system, as this is a typical starting point for many seeking assistance with tobacco use. Future intervention studies should attempt to mitigate some of the barriers to quitting by addressing physiological and habitual factors that maintain continued e-cigarette use.
This preliminary intervention trial provides further insight into the effectiveness of NRT to promote e-cigarette cessation23,25,26. In the sample recruited, a substantial proportion of e-cigarette only users who endorsed use of the provided NRT were able to quit mono-vaping. This suggests that NRT might be sufficient to mitigate nicotine withdrawal symptoms in e-cigarette users quitting, which is a bit surprising given the relative inefficiency of NRT to deliver nicotine as compared to e-cigarettes. However, when considering NRT’s efficacy for combustible tobacco cessation, these results are consistent. NRT was clearly insufficient for dual users seeking to quit both vaping and smoking, suggesting that dual users have unique pharmacologic needs and/or non-pharmacologic constructs should be addressed more substantially. More research is needed to determine 1) pharmacotherapy recommendations for e-cigarette cessation and 2) the most effective treatment protocol for dual users. Importantly, individuals who quit vaping did not increase or initiate cigarette smoking at follow-up, which helps to alleviate concerns regarding relapse or increases in smoking during e-cigarette cessation. Although some participants in the dual use group reduced smoking alongside vaping, most did not change their smoking. Given the high disease burden of combustible tobacco use, quitting smoking should remain a top priority.
4.1. Limitations
Results should be interpreted with caution given the pilot nature of the study, minimal intervention, single variable tests, and short-term follow-up period. The NRT dose was not tailored for each individual, and thus, may have been insufficient to address those with greater dependence, including dual users. Additionally, engagement with the treatment outside from NRT (e.g., support booklet, quitline) was not evaluated and should be a priority for future research studies. Survey contact may have also augmented quit intentions in the intervention group. Because the purpose of the study was to evaluate the feasibility and acceptability of NRT alongside a supportive booklet, the control group did not complete daily surveys. Therefore, important information regarding the nature of the quit attempts in this group is lacking. Finally, reliance on self-reported abstinence and imputing missing data has limitations36, although biochemical verification of e-cigarette use separate from NRT is challenging39.
4.2. Conclusions
Recruitment for the present study supports that many adults are interested in e-cigarette or dual use cessation. Participants reported experiencing negative consequences from vaping that motivated them to quit but received minimal support for overcoming challenges associated with quitting. This preliminary trial of NRT + a self-help booklet for e-cigarette cessation showed encouraging evidence of effectiveness for those who use e-cigarettes only. Future research should confirm these results through larger, more rigorous trials, and explore ways to improve outcomes for dual users. Effective interventions should be rapidly disseminated to treatment providers to assist the growing number of e-cigarette users who wish to quit.
Highlights.
Many adults who use e-cigarettes are interested in quitting
Interventions for e-cigarette cessation are not well studied
Participants were interested in quitting due to negative effects of dependence
Nicotine replacement therapy for vaping cessation was feasible and acceptable
Larger trials should evaluate nicotine replacement therapy for vaping cessation
Acknowledgements:
The authors would like to thank Megan Stover for her assistance with this project, and the participants for their contributions to the study.
Funding:
This study has been funded by NIH Institutional Postdoctoral Training Grant NIH-T32-HL144470 and the MUSC Hollings Cancer Center P30 CA138313. This funding source had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest in the past 3 years: Dr. Toll has testified on behalf of plaintiffs who have filed litigation against the tobacco industry.
References
- 1.Zhu S-H, Zhuang Y-L, Wong S, Cummins SE, Tedeschi GJ. E-cigarette use and associated changes in population smoking cessation: evidence from US current population surveys. BMJ 2017;358:j3262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cornelius ME, Loretan CG, Wang TW, Jamal A, Homa DM. Tobacco Product Use Among Adults—United States, 2020. Morbidity and Mortality Weekly Report 2022;71:397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Palmer AM, Smith TT, Nahhas GJ, et al. Interest in quitting e-cigarettes among adult e-cigarette users with and without cigarette smoking history. JAMA Network Open 2021;4:e214146–e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Parrott AC. The psychobiological problems of continued nicotine dependency in e-cigarette ‘vapers’. Commentary:“Electronic cigarettes”. Frontiers in Psychiatry 2015;6:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Amato MS, Bottcher MM, Cha S, Jacobs MA, Pearson JL, Graham AL. “It’s really addictive and I’m trapped:” A qualitative analysis of the reasons for quitting vaping among treatment-seeking young people. Addictive Behaviors 2021;112:106599. [DOI] [PubMed] [Google Scholar]
- 6.Simpson KA, Kechter A, Schiff SJ, et al. Characterizing symptoms of e-cigarette dependence: a qualitative study of young adults. BMC Public Health 2021;21:959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kong G, Bold KW, Cavallo DA, Davis DR, Jackson A, Krishnan-Sarin S. Informing the development of adolescent e-cigarette cessation interventions: A qualitative study. Addictive Behaviors 2021;114:106720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abdel-Qader DH, Al Meslamani AZ. Knowledge and Beliefs of Jordanian Community Toward E-cigarettes: A National Survey. J Community Health 2021;46:577–86. [DOI] [PubMed] [Google Scholar]
- 9.Kelly BC, Pawson M, Vuolo M. Beliefs on COVID-19 Among Electronic Cigarette Users: Behavioral Responses and Implications for COVID Prevention and E-Cigarette Interventions. Journal of Drug Issues 2020;51:284–300. [Google Scholar]
- 10.Klemperer EM, Villanti AC. Why and how do dual users quit vaping? Survey findings from adults who use electronic and combustible cigarettes. Tob Induc Dis 2021;19:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lin W, Martinez SA, Ding K, Beebe LA. Knowledge and Perceptions of Tobacco-Related Harm Associated with Intention to Quit among Cigarette Smokers, e-Cigarette Users, and Dual Users: Findings from the US Population Assessment of Tobacco and Health (PATH) Wave 1. Subst Use Misuse 2021;56:464–70. [DOI] [PubMed] [Google Scholar]
- 12.Mendel JR, Hall MG, Baig SA, Jeong M, Brewer NT. Placing Health Warnings on E-Cigarettes: A Standardized Protocol. Int J Environ Res Public Health 2018;15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Powers JM, LaRowe LR, Garey L, Zvolensky MJ, Ditre JW. Pain intensity, e-cigarette dependence, and cessation-related outcomes: The moderating role of pain-related anxiety. Addict Behav 2020;111:106548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Volesky KD, Maki A, Scherf C, Watson LM, Cassol E, Villeneuve PJ. Characteristics of e-cigarette users and their perceptions of the benefits, harms and risks of e-cigarette use: survey results from a convenience sample in Ottawa, Canada. Health Promot Chronic Dis Prev Can 2016;36:130–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Brewer NT, Jeong M, Hall MG, et al. Impact of e-cigarette health warnings on motivation to vape and smoke. Tob Control 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Minami H, Teo TK. The impact of e-cigarette price changes on vaping and smoking behaviors. Subst Use Misuse 2019;54:1599–610. [DOI] [PubMed] [Google Scholar]
- 17.Pepper JK, Ribisl KM, Emery SL, Brewer NT. Reasons for starting and stopping electronic cigarette use. Int J Environ Res Public Health 2014;11:10345–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wong LP, Mohamad Shakir SM, Alias H, Aghamohammadi N, Hoe VC. Reasons for Using Electronic Cigarettes and Intentions to Quit Among Electronic Cigarette Users in Malaysia. J Community Health 2016;41:1101–9. [DOI] [PubMed] [Google Scholar]
- 19.Klemperer EM, Villanti AC. Motivations and methods of dual users to quit vaping: Survey findings from adults who use electronic and combustible cigarettes. Tobacco induced diseases 2021;19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Graham AL, Amato MS, Cha S, Jacobs MA, Bottcher MM, Papandonatos GD. Effectiveness of a vaping cessation text message program among young adult e-cigarette users: a randomized clinical trial. JAMA internal medicine 2021;181:923–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Palmer AM, Tomko RL, Squeglia LM, et al. A pilot feasibility study of a behavioral intervention for nicotine vaping cessation among young adults delivered via telehealth. Drug and Alcohol Dependence 2022:109311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Raiff BR, Newman ST, Upton CR, Burrows CA. The feasibility, acceptability, and initial efficacy of a remotely delivered, financial-incentive intervention to initiate vaping abstinence in young adults. Experimental and clinical psychopharmacology 2021. [DOI] [PubMed] [Google Scholar]
- 23.Sahr M, Kelsh S, Blower N, Sohn M. Pilot study of electronic nicotine delivery systems (ENDS) cessation methods. Pharmacy 2021;9:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Graham AL, Jacobs MA, Amato MS. Engagement and 3-month outcomes from a digital e-cigarette cessation program in a cohort of 27 000 teens and young adults. Nicotine and Tobacco Research 2020;22:859–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sikka G, Oluyinka M, Schreiber R, Galiatsatos P. Electronic Cigarette Cessation in Youth and Young Adults: A Case Series. Tobacco use insights 2021;14:1179173X211026676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Silver B, Ripley Moffitt C, Greyber J, Goldstein AO. Successful use of nicotine breplacement therapy to quit e cigarettes: lack of treatment protocol highlights need for guidelines. Clinical case reports 2016;4:409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cornelius ME, Wang TW, Jamal A, Loretan CG, Neff LJ. Tobacco Product Use Among Adults - United States, 2019. MMWR Morb Mortal Wkly Rep 2020;69:1736–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Etter JF. Are long term vapers interested in vaping cessation support? Addiction 2019;114:1473–7. [DOI] [PubMed] [Google Scholar]
- 29.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of biomedical informatics 2009;42:377–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Palmer AM, Rojewski AM, Chen L-s, et al. Tobacco treatment program models in US hospitals and outpatient centers on behalf of the SRNT treatment network. Chest 2021;159:1652–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.South Carolina Tobacco Quitline. (Accessed 05/2022, at https://www.quitnowsc.org/.)
- 32.Live Vape Free Program. 2022. (Accessed 05, 2022, at https://www.rallyhealth.com/live-vape-free.)
- 33.Foulds J, Veldheer S, Yingst J, et al. Development of a Questionnaire for Assessing Dependence on Electronic Cigarettes Among a Large Sample of Ex-Smoking E-cigarette Users. Nicotine & Tobacco Research 2014;17:186–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Piper ME, McCarthy DE, Bolt DM, et al. Assessing dimensions of nicotine dependence: an evaluation of the Nicotine Dependence Syndrome Scale (NDSS) and the Wisconsin Inventory of Smoking Dependence Motives (WISDM). Nicotine & Tobacco Research 2008;10:1009–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Morean ME, L’Insalata A. The Short Form Vaping Consequences Questionnaire: Psychometric Properties of a Measure of Vaping Expectancies for Use With Adult E-cigarette Users. Nicotine & Tobacco Research 2016;19:215–21. [DOI] [PubMed] [Google Scholar]
- 36.Tompsett D, Sutton S, Seaman SR, White IR. A general method for elicitation, imputation, and sensitivity analysis for incomplete repeated binary data. Statistics in Medicine 2020;39:2921–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rampin R, Rampin V. Taguette: open-source qualitative data analysis. Journal of Open Source Software 2021;6:3522. [Google Scholar]
- 39.Shahab L, Goniewicz ML, Blount BC, et al. Nicotine, Carcinogen, and Toxin Exposure in Long-Term E-Cigarette and Nicotine Replacement Therapy Users. Annals of Internal Medicine 2017;166:390–400. [DOI] [PMC free article] [PubMed] [Google Scholar]