

Abstract
Purpose
To examine changes in the position of the lower eyelid punctum and tear meniscus height (TMH) after correction of horizontal laxity of the lower eyelid in involutional lower eyelid entropion.
Methods
This prospective, observational study included 42 sides of 36 patients with involutional entropion who underwent a lateral tarsal strip procedure or transcanthal canthopexy (+ lower eyelid retractor advancement). The horizontal distance from the medial margin of the lower lacrimal punctum to the medial canthus was measured using ImageJ software. TMH was measured using anterior segment optical coherence tomography. All measurements were performed preoperatively, at postoperative 3-month and at postoperative 6-month.
Results
The lower lacrimal punctum significantly shifted laterally at 3-month follow-up and slightly returned toward its original position at 6-month follow-up (Friedman's test, P < 0.001). Although the differences did not reach statistical significance, TMH in the lower eyelid increased at 3-month follow-up and then slightly decreased at 6-month follow-up (Friedman's test, P = 0.076).
Conclusions
The results of this study imply that lateral shift of the lower lacrimal punctum prevents effective drainage of tears accumulated in the lacrimal lake, resulting in increased TMH after correction of horizontal laxity of the lower eyelid in involutional entropion.
1. Introduction
Involutional lower eyelid entropion (involutional entropion) is the most common type of entropion in which the lower eyelid turns inwardly [1]. Corneal abrasion by the cilia causes ocular pain, irritation, itching, burning sensation, tearing, photophobia, conjunctival injection, discharge, and vision loss [1–3].
The main etiologic factors for the development of involutional entropion are the vertical and horizontal laxities of the lower eyelid [1]. For addressing the vertical laxity, the lower eyelid retractor (LER) is advanced, while the horizontal laxity is corrected by horizontal tightening or shortening procedures of the lower eyelid, such as the lateral tarsal strip (LTS) procedure, transcanthal canthopexy (TCC), and wedge resection [1].
When the lower eyelid is horizontally tightened or shortened, the lower lacrimal punctum is shifted laterally [4]. A laterally shifted lower lacrimal punctum is away from the lacrimal lake, causing interruption of effective tear drainage. On the contrary, surgical correction of involutional entropion decreases reflex tear secretion and simultaneously corrects lower lacrimal punctum malposition. In addition, horizontal tightening/shortening may improve the lacrimal pump function [5–7]. None of the previous studies demonstrated postoperative changes in lacrimal punctum position and tear meniscus height (TMH) after surgical correction of the horizontal laxity in patients with involutional entropion.
In this study, we examined changes in the horizontal position of the lower lacrimal punctum and TMH after LTS or TCC for addressing the horizontal laxity in patients with involutional entropion.
2. Methods
2.1. Ethics Approval
The Institutional Review Board (IRB) of Aichi Medical University Hospital approved this study, which was conducted in accordance with the tenets of the Declaration of Helsinki and its later amendments (approval number, 2022-172). The IRB granted a waiver of informed consent for this study based on the ethical guidelines for medical and health research involving human subjects established by the Japanese Ministry of Education, Culture, Sports, Science, and Technology and by the Ministry of Health, Labour, and Welfare. The waiver was granted because the study was not an interventional study. Nevertheless, at the request of the IRB, an outline of the study was published on the Aichi Medical University website that was available for public viewing, which also gave the patients the option to refuse to participate in the study, although none did. Personal identifiers were removed from the records prior to data analysis.
2.2. Study Design and Patients
This prospective, observational study included Japanese patients in whom involutional lower eyelid entropion was corrected by one of the authors (YT) from October 2017 to January 2022. Patients with a previous history of eyelid or lacrimal surgery were excluded from this study. A patent lacrimal drainage system was confirmed before surgery in all patients.
2.3. Data Collection
The following data were collected: age, sex, affected side, results of the pinch test, and surgical procedures. The horizontal positions of the lower lacrimal punctum and TMH were measured preoperatively, at postoperative 3 months, and at postoperative 6 months.
To measure the horizontal position of the lacrimal punctum in the lower eyelid, slit-lamp photos were taken with the patients' heads and chins fixed and the eyes in the primary position. To avoid changes in the lower eyelid position vertically and horizontally, we gently turned the eyelid margin by a finger to expose the lower lacrimal punctum. A ruler was contained in the photos. The photos were captured, and the horizontal distance from the medial margin of the lacrimal punctum (white zone boundary [8]) to the medial canthus was measured using ImageJ software (National Institute of Health, Bethesda, MD) (Figure 1). The measurements were made by converting pixel numbers to distance based on the ruler contained in the same photo.
Figure 1.
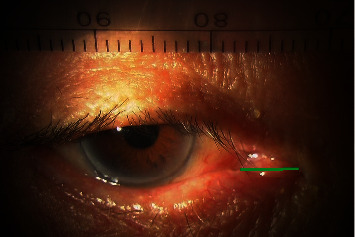
Measurement of the horizontal position of the lower lacrimal punctum. After exposure of the lower punctum, the horizontal distance from the medial margin of the lower lacrimal punctum to the medial canthus (green solid line) was measured.
TMH was measured on the sagittal plane through the centers of the upper and lower eyelids using an anterior segment optical coherence tomography (CASIA2, TOMEY Corporation, Aichi, Japan). Before surgery, an inverted lower eyelid was returned to the normal eyelid position by a digital push of the lower eyelid in the inferior direction. Patients were directed to blink several times, then stop blinking, and keep their eyes open to prevent another inward turn of the lower eyelid [9]. At that time, the TMH was measured. Postoperatively, the TMH was measured after blinking several times.
2.4. Surgical Procedure
The details of each surgical procedure are presented in our previous studies [10, 11].
2.4.1. LER Advancement
Under local anesthesia, the skin was incised 3 mm below the cilia. The layer under the orbicularis oculi muscle (OOM) was dissected toward the cilia. The anterior layer of the LER on the tarsus was detached inferiorly until the lower margin of the tarsus was exposed. The posterior layer of the LER was detached from the conjunctiva. The orbital septum was incised transversely just below the junction between the anterior layer of the LER and the orbital septum. The OOM in the eyelid margin was slightly debulked to facilitate outward rotation of the eyelid margin. Then, a site 2 mm below the edge of the posterior layer was fixed to the lower edge of the tarsus using a 6-0 Asflex® (Kono Seisakusho Co., Ltd., Tokyo, Japan) suture with simultaneous advancement of the anterior layer to reinforce the posterior layer. We added 2 additional sutures, and then the pretarsal OOM and the lower edge of the tarsus were secured at three points. Finally, the skin was sutured with 6-0 Asflex® sutures.
2.4.2. LTS
Under local anesthesia, a 10 mm skin incision was made along the lateral canthal rhytids. A lateral canthotomy was performed, and the inferior crus of the lateral canthal band and the Lockwood ligament were severed. A 7 mm incision through the conjunctiva and LERs was made immediately below the tarsus in the temporal portion of the eyelid to free the temporal tarsal attachment. The anterior and posterior lamellae of the temporal portion of the eyelid were separated. The skin and conjunctiva at the mucocutaneous junction were trimmed, and the conjunctiva on the tarsus was removed to fashion the tarsal strip. The tarsal strip was shortened by the appropriate amount and then fixed to the inside of the lateral orbital wall with a 5-0 Prolene® (Ethicon Inc., Bridgewater, NJ) suture. After a lateral canthoplasty, the OOM and skin were sutured with 6-0 Asflex® sutures.
2.4.3. TCC
Under local anesthesia, a 6 mm skin incision was made along the lateral canthal rhytids, just anterior to the lateral orbital rim. A stab incision was made at the lower eyelid margin, just medial to the commissure. Needles with a double-armed 5-0 Prolene® suture were inserted into the stab incision, passed through the hard lateral retinaculum or periosteum, and pulled out from the skin incision area. After a firm ligation of this suture, the skin was closed with 6-0 Asflex® sutures.
2.5. Statistical Analyses
Patient age and measurement results are expressed as the mean value ± standard deviation. The position of the lower lacrimal punctum and TMH were compared among 3 measurement periods using Friedman's test and Bonferroni correction because some of the measurement results did not have a normal distribution. In addition, the horizontal position of the lower lacrimal punctum and TMH were compared between patients who underwent LTS and TCC using the Mann–Whitney U test. Preoperative TMH was compared between the affected and unaffected sides in patients with unilateral involutional entropion using Student's t-test. All statistical analyses were performed using SPSS™ ver. 26 software (IBM Japan, Tokyo, Japan). A P value of <0.050 was considered statistically significant.
We also performed a post hoc analysis of the validity of the sample size in this study. The effect size was calculated based on the mean values and standard deviations of TMH in the lower eyelid. The α error was set as 0.05, and the power of the test (=1 − β error) was calculated using G∗Power software version 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany).
3. Results
Data on demography and measurement results are shown in Table 1. This study included 42 sides from 36 patients. Bilateral involutional entropion was seen in 6 patients. The pinch test was positive (8 mm anterior displacement from the globe) before surgery on 36 sides. LTS and TCC were performed on 15 and 27 sides, respectively. None of the patients had any disease affecting wound healing or took medications, which could also affect the recovery of the surgical site. The power of the test (=1 − β error) was 1.000, indicating the validity of the sample size in this study.
Table 1.
Demographic data and results of measurements and statistical comparison.
| Patient number/sides | 36/42 |
|
| |
| M/F | 18/18 |
| R/L | 19/23 |
| Patient age (years) | 75.9 ± 8.1 |
| Positive pinch test (sides) | |
| Preoperative | 36 |
| Postoperative 6 months | 4 |
| Surgical procedure | |
| LER advancement + LTS | 15 |
| LER advancement + TCC | 27 |
| Horizontal position of lower lacrimal punctum (mm) | |
| Preoperative | 3.95 ± 0.24 |
| Postoperative 3 months | 4.79 ± 0.23 |
| Postoperative 6 months | 4.56 ± 0.23 |
| P value | <0.001 |
| TMH (μm) upper eyelid | |
| Preoperative | 196.8 ± 14.9 |
| Postoperative 3 months | 195.1 ± 14.3 |
| Postoperative 6 months | 194.2 ± 13.6 |
| P value | 0.801 |
| Lower eyelid | |
| Preoperative | 276.0 ± 29.4 |
| Postoperative 3 months | 311.1 ± 29.6 |
| Postoperative 6 months | 303.2 ± 25.3 |
| P value | 0.076 |
M, male; F, female; R, right; L, left; LER, lower eyelid retractor; LTS, lateral tarsal strip; TCC, transcanthal canthopexy; TMH, tear meniscus height.
The results of the statistical comparison are shown in Tables 1to 4. The horizontal distance from the lower punctum to the medial canthus got longer at the 3-month follow-up period. At the 6-month follow-up period, the distance got shorter from the baseline measured at 3-month follow-up, but it was still longer than that measured preoperatively. The distance measured at 3-month follow-up was significantly longer than that measured preoperatively (P = 0.035). The difference in the distances measured preoperatively and at 6-month follow-up did not reach statistical significance (P = 0.194). Similarly, the distances measured at 3- and 6-month follow-up were also not significantly different (P = 1.000).
Table 4.
Comparison of preoperative tear meniscus height (TMH) between the affected and unaffected sides in patients with unilateral involutional entropion.
| Affected side | Unaffected side | P value | |
|---|---|---|---|
| Preoperative upper TMH (μm) | 202.8 ± 104.7 | 210.3 ± 81.9 | 0.759 |
| Preoperative lower TMH (μm) | 270.5 ± 203.0 | 238.7 ± 113.7 | 0.456 |
The TMH in the upper eyelid did not change significantly after surgery (P = 0.801). TMH in the lower eyelid increased once at the 3-month follow-up period and then slightly decreased at the 6-month follow-up period. But these changes did not reach statistical significance (P = 0.076).
The lower punctum position and TMH measured at each measurement period were not different between patients who underwent LTS and TCC (P > 0.050). Preoperative TMH was not different between the affected and unaffected sides in patients with unilateral involutional entropion (P > 0.050).
Involutional entropion was successfully treated, and none of the patients experienced recurrence until 6-month follow-up. None of the patients had apparent lower eyelid retraction and ectropion after the surgeries performed. Although all patients obtained horizontal tightness after surgery once, 4 patients showed a positive pinch test at the 6-month follow-up period (after LTS in 2 cases and after TCC in 2 cases).
4. Discussion
This study examined changes in the position of the lower lacrimal punctum and TMH after correction of horizontal laxity of the lower eyelid in patients with involutional entropion. We found out that the lower lacrimal punctum shifted laterally significantly. Although the differences did not reach statistical significance, TMH in the lower eyelid increased after the surgeries. The lacrimal lake is located adjacent to the lacrimal caruncle and is vertically aligned with the lacrimal papilla [12]. A laterally shifted lower lacrimal punctum is, therefore, away from the lacrimal lake, which may interfere with the effective drainage of tears accumulated in the lacrimal lake. This may be reflected in the measurement results of this study.
Preoperative TMH was not different between the affected and unaffected sides in patients with unilateral involutional entropion. Although involutional entropion can cause reflex tear secretion by cilia-induced ocular surface abrasion [3], decreased corneal sensitivity in old patients may not increase the amount of reflex tear secretion [13]. In addition, malposition of the lower lacrimal punctum may also not affect the function of tear drainage.
Horizontal tightening/shortening of the lower eyelid may improve the function of the lacrimal pump [5–7]. However, TMH tended to increase after LTS or TCC in this study. One of the possible reasons was that horizontal tightening/shortening does not always cure lacrimal pump failure. Previous studies showed that 41.2–87% of patients experienced complete or nearly complete relief of epiphora after horizontal tightening/shortening [5–7]. Another possible reason was that the degree of TMH elevation by the lateral shift of the lower lacrimal punctum surpassed the degree of TMH reduction by the effectiveness of horizontal tightening/shortening.
Although the differences did not reach statistical significance, the horizontal distance between the lower lacrimal punctum and the medial canthus and TMH in the lower eyelid measured at 6-month follow-up decreased slightly from the baseline measured at 3-month follow-up. Since the scar gradually softens during the scar remodeling phase within a several weeks to a few years [14, 15], this may be caused by mild improvement of cicatricial contracture in the lateral canthus.
We supposed that LTS secures a tighter fixation, resulting in a more lateral shift of the lower lacrimal punctum and no return of the lower punctum position at 6-month follow-up, compared to TCC. However, the measurement results were not different between patients who underwent LTS and TCC. Our previous reports showed no recurrence of involutional entropion after both LER advancement + LTS and LER advancement + TCC [10, 11]. These imply that even TCC provides a horizontal tightness equivalent to LTS.
In LTS and TCC, the lower eyelid is drawn laterally in one direction. On the contrary, in the Kuhnt–Szymanowski procedure [16], the lower eyelid is drawn both medially and laterally [4]. This may induce a less lateral shift of the lower lacrimal punctum [4]. Although we did not evaluate medial and lateral canthal laxities using lateral and medial distraction tests, the Kuhnt–Szymanowski procedure may be a better option to prevent excess lateral shift of the lower lacrimal punctum and following epiphora, particularly in patients with severe laxity of the medial canthus.
There are a few limitations to this study. First, this study included only Japanese patients. Since there are known racial differences in eyelid anatomy [17], the results may not be applicable to other races. Second, all the measurements were performed by a single examiner, which could affect the reliability of this study. Third, quantification of the results of the pinch test may provide more information for this study.
In conclusion, the lower lacrimal punctum shifted laterally, and TMH in the lower eyelid tended to increase after correcting horizontal laxity of the lower eyelid in patients with involutional entropion. These results indicate that a laterally shifted lower lacrimal punctum was unable to effectively drain tears accumulated in the lacrimal lake, resulting in increased TMH after surgery.
Table 2.
The results of Bonferroni correction.
| Lower punctum position | Postoperative 3 months | Postoperative 6 months |
|---|---|---|
| Preoperative | 0.035 | 0.194 |
| Postoperative 3 months | — | 1.000 |
Table 3.
Comparison of measurement results between patients who underwent lateral tarsal strip (LTS) procedure and transcanthal canthopexy (TCC).
| LTS | TCC | P value | |
|---|---|---|---|
| Horizontal position of lower lacrimal punctum (mm) | |||
| Preoperative | 3.57 ± 1.42 | 4.16 ± 1.64 | 0.232 |
| Postoperative 3 months | 4.81 ± 1.62 | 4.77 ± 1.42 | 0.783 |
| Postoperative 6 months | 4.36 ± 1.64 | 4.67 ± 1.40 | 0.896 |
| TMH (μm) | |||
| Upper eyelid | |||
| Preoperative | 173.2 ± 88.2 | 210.0 ± 100.3 | 0.242 |
| Postoperative 3 months | 205.3 ± 98.1 | 189.5 ± 90.9 | 0.646 |
| Postoperative 6 months | 172.3 ± 79.3 | 206.3 ± 92.2 | 0.372 |
| Lower eyelid | |||
| Preoperative | 248.9 ± 199.4 | 291.0 ± 188.1 | 0.416 |
| Postoperative 3 months | 316.7 ± 224.9 | 307.9 ± 174.9 | 0.503 |
| Postoperative 6 months | 291.3 ± 151.4 | 309.9 ± 173.4 | 0.783 |
TMH, tear meniscus height.
Acknowledgments
The authors wish to thank Dr. Shunsuke Nakakura at the Department of Ophthalmology, Saneikai Tsukazaki Hospital, for his advice on statistical methods.
Data Availability
The data supporting the results of this study are available from the corresponding author upon request.
Disclosure
A part of this study will be presented at the 127th Annual Meeting of the Japanese Ophthalmological Society, which will be held during April 6–9, 2023..
Conflicts of Interest
The authors declare that they have no conflicts interest.
Authors' Contributions
Tatusro Yokoyama wrote the original draft. Aric Vaidya reviewed and edited the manuscript. Shinjiro Kono performed data curation and reviewed and edited the manuscript. Hirohiko Kakizaki reviewed and edited the manuscript. Yasuhiro Takahashi conceptualized the study, investigated the study, performed data curation and formal analysis, proposed the methodology, was responsible for project administration, and wrote the original draft.
References
- 1.Lin P., Kitaguchi Y., Mupas-Uy J., Sabundayo M. S., Takahashi Y., Kakizaki H. Involutional lower eyelid entropion: causative factors and therapeutic management. International Ophthalmology . 2019;39(8):1895–1907. doi: 10.1007/s10792-018-1004-1. [DOI] [PubMed] [Google Scholar]
- 2.Parsons S. R., O’Rourke M. A., Satchi K., McNab A. A. Corneal complications secondary to involutional entropion at presentation. Ophthalmic Plastic and Reconstructive Surgery . 2022;38(6):593–595. doi: 10.1097/iop.0000000000002219. [DOI] [PubMed] [Google Scholar]
- 3.Han J., Lee S. H., Shin H. J. Mini-incisional entropion repair for correcting involutional entropion: full description and surgical outcome. Medicine (Baltimore) . 2019;98(33) doi: 10.1097/md.0000000000016731.e16731 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ishikawa E., Takahashi Y., Kakizaki H. Modification of the Lazy-T procedure for correction of punctal ectropion. Journal of Craniofacial Surgery . 2019;30(1):226–227. doi: 10.1097/scs.0000000000004722. [DOI] [PubMed] [Google Scholar]
- 5.Narayanan K., Barnes E. A. Epiphora with eyelid laxity. Orbit . 2005;24(3):201–203. doi: 10.1080/01676830500192126. [DOI] [PubMed] [Google Scholar]
- 6.Guercio B., Keyhani K., Weinberg D. A. Snip punctoplasty offers little additive benefit to lower eyelid tightening in the treatment of pure lacrimal pump failure. Orbit . 2007;26(1):15–18. doi: 10.1080/01676830600975164. [DOI] [PubMed] [Google Scholar]
- 7.Vick V. L., Holds J. B., Hartstein M. E., Massry G. G. Tarsal strip procedure for the correction of tearing. Ophthalmic Plastic and Reconstructive Surgery . 2004;20(1):37–39. doi: 10.1097/01.iop.0000103005.81708.fd. [DOI] [PubMed] [Google Scholar]
- 8.Bothra N., Saini P., Ali M. J. Age-related changes in the lacrimal punctum morphology in a normal population: punctum update (PUP) study-paper 1. Ophthalmic Plastic and Reconstructive Surgery . 2022;39 doi: 10.1097/IOP.0000000000002225. (Online ahead of print) [DOI] [PubMed] [Google Scholar]
- 9.Iuchi T., Takahashi Y., Kang H., Asamura S., Isogai N., Kakizaki H. Involvement of inward upper eyelid push on the lower eyelid during eyelid closure in development of involutional lower eyelid entropion. European Journal of Ophthalmology . 2016;26(6):520–522. doi: 10.5301/ejo.5000770. [DOI] [PubMed] [Google Scholar]
- 10.Ishida Y., Takahashi Y., Kakizaki H. Posterior layer advancement of lower eyelid retractors with transcanthal canthopexy for involutional lower eyelid entropion. Eye . 2016;30(11):1469–1474. doi: 10.1038/eye.2016.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee H., Takahashi Y., Ichinose A., Kakizaki H. Comparison of surgical outcomes between simple posterior layer advancement of lower eyelid retractors and combination with a lateral tarsal strip procedure for involutional entropion in a Japanese population. British Journal of Ophthalmology . 2014;98(11):1579–1582. doi: 10.1136/bjophthalmol-2013-304830. [DOI] [PubMed] [Google Scholar]
- 12.Valencia M. R. P., Takahashi Y., Naito M., Nakano T., Ikeda H., Kakizaki H. Lacrimal drainage anatomy in the Japanese population. Annals of Anatomy - Anatomischer Anzeiger . 2019;223:90–99. doi: 10.1016/j.aanat.2019.01.013. [DOI] [PubMed] [Google Scholar]
- 13.Roszkowska A. M., Colosi P., Ferreri F. M. B., Galasso S. Age-related modifications of corneal sensitivity. Ophthalmologica . 2004;218(5):350–355. doi: 10.1159/000079478. [DOI] [PubMed] [Google Scholar]
- 14.Son D., Harijan A. Overview of surgical scar prevention and management. Journal of Korean Medical Science . 2014;29(6):751–757. doi: 10.3346/jkms.2014.29.6.751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Moffitt Cancer Center. Managing your scar. 2022. https://moffitt.org/media/1086/managing_your_scar.pdf .
- 16.Van Slyke A. C., Carr L. A., Carr N. J. The KS-pexy: a novel method to manage horizontal lower eyelid laxity. Plastic and Reconstructive Surgery . 2020;145(2):p. 306e. doi: 10.1097/PRS.0000000000006484. [DOI] [PubMed] [Google Scholar]
- 17.Kono S., Vaidya A., Naito M., et al. Positional relationship between lacrimal sac and skull base: implication of risk of cerebrospinal fluid leakage during dacryocystorhinostomy. Scientific Reports . 2022;12(1) doi: 10.1038/s41598-022-18859-5.14459 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data supporting the results of this study are available from the corresponding author upon request.