

Abstract
Aim
To explore the effects of COVID‐19 pandemic restrictions varying in severity and duration on health‐related behaviours in children aged 5–17 years.
Methods
We used data from the Royal Children's Hospital National Child Health Poll, an online cross‐sectional survey of Australian caregivers. The survey assessed 1222 caregivers' perceived changes in health‐related behaviours (physical activity, sleep, screen‐time, diet, outdoor activity, family and peer connectedness) of 2011 children aged 5–17 years in a typical week from June to September 2020 (when jurisdictions experienced varying restriction severity and duration) compared to retrospective reports of behaviour before March 2020 (pre‐pandemic). To compare the effects of varying restriction severity in Victoria, New South Wales (NSW) and other states and territories on health‐related behaviours binary logistic regression was used, adjusting for caregiver demographics and weighted to reflect Australia's parent population.
Results
Compared to pre‐pandemic, Victoria's restrictions had a greater impact on child health‐related behaviours compared to NSW restrictions and an even stronger impact compared to other states and territories which experienced few or no restrictions. A greater proportion of Victorian children reported more recreational screen time (71.3%) than NSW (53.9%) and other states and territories (34.5%) and less physical activity (57.2%) than NSW (30.3%) and other states and territories (26.5%). Victorian children reported less outdoor activity (62.6%) than NSW (32.0%) and other states and territories (25.2%), and less social connectedness (68.0%) than NSW (35.4%) and other states and territories (27.3%).
Conclusions
More severe and longer COVID‐19 pandemic restrictions are associated with greater impacts and predominantly more negative impacts to children's health‐related behaviours. These should be mitigated through policies and programs to encourage healthier life‐styles.
Keywords: caregivers, children, health‐related behaviours, lockdown, parents, SARS COVID‐19 pandemic
What is already known on this topic
Previous studies have established lockdowns have had an impact on children worldwide in regards to sleep, physical activity, diet, screen time and social connection.
This has concerning implications for the long‐term effects of COVID‐19 pandemic restrictions.
What this paper adds
This is the first study to investigate the differing effects of restrictions varying in severity and duration on a broad range of children's health‐related behaviours.
Our study provides clarity on the impacts of COVID‐19 pandemic restrictions on diet and physical activity to redress discord in the literature.
Lockdowns were implemented world‐wide as a public health measure to reduce transmission of the SARS‐Corononavirus‐2 (henceforth COVID‐19) and have resulted in unprecedented impacts on the life‐style of families. 1 , 2 , 3 , 4 , 5 , 6 , 7 Following Australia's national lockdown (March to May 2020), restrictions differed across Australia due to varying transmission rates and state government responses. Victoria's lockdown from 8 July to 23 November 2020, featured measures including ‘four reasons to leave home’, exercise limits (1 h) and night‐time curfews. 8 Comparatively, New South Wales (NSW) had minimal community transmission in July 2020 and employed less severe restrictions; with capacity limits on gatherings in the hospitality sector, events and inside homes. 9 Contrastingly, the remaining states and territories had no community transmission and only minor or no restrictions in place during this period.
Studies on the acute effects of lockdown on children's life‐styles have predominantly focused on specific behaviours, such as physical activity, screen time and sleep in adolescents and some discrepancy pervades the literature. 1 , 2 , 3 , 4 , 5 For instance, while Greek and Australian studies showed lockdowns decreased adolescents' physical activity, 1 , 3 a German study reported physical activity increased, despite the same loss of organised sporting activities. 4 The implications of decreased physical activity and increased recreational screen usage caused by lockdowns may be associated with poorer long‐term health outcomes. 2 , 3 , 10 Investigating if increased sedentary behaviours, including screen use, are a direct impact of pandemic restrictions will help inform the public health intervention strategies.
Existing studies on children's behaviour changes due to restrictions compared before and after lockdown exposure without adequate control groups; therefore, possible confounding variables, including high‐community infection rates, were not considered. 1 , 2 , 4 , 6 By investigating Australian parents' perceptions of their children's life‐styles before COVID‐19 and during Victoria's lockdown, we aimed to explore the effects of restrictions differing in severity and duration on children's health‐related behaviours aged 5–17 years. It was hypothesised that Victorian children would experience greater impacts to health‐related behaviours (physical activity, sleep, screen time, diet, outdoor activity, family connectedness and social connection) compared to children in NSW and other states and territories, who experienced less severe restrictions.
Methods
Study design
A national‐level cross‐sectional survey was conducted online from 15th to 29th September 2020 by the Royal Children's Hospital (RCH) National Child Health Poll. The RCH Human Research Ethics Committee approved the study protocol (RCH HREC 35254).
Study sample
Participants were selected in two stages. First, a panel of over 100 000 caregivers were recruited by a private online survey vendor, the Online Research Unit, through online and offline measures creating a panel of Australian caregivers with demographic characteristics representative of the national distribution based on state and territory residency, gender and age. Caregivers were defined as primary carers for at least 1 day per week of a child aged less than 18 years and were required to be 18 years or older, current Australian residents and have internet access. Secondly, a sample of these caregivers (2.5 times the expected sample size of 2000) was randomly selected using age, sex and state stratified random sampling and invited to participate. Caregivers were assumed to provide consent if they voluntarily participated in the survey with a response rate of 81%. One respondent was permitted per household and allocated a unique numerical identifier to ensure anonymity and one‐time poll access. For this study, we have included caregivers of children aged 5–17 years.
Measures
The survey questionnaire was developed after extensive review of the scientific and grey literature in liaison with experts on the emerging impacts of the COVID‐19 pandemic on families and children.
The survey collected caregivers' gender, age, number of children, family structure, education status, country of birth, state/territory residency, region of residency based on Australian Bureau of Statistics (ABS) Accessibility and Remoteness Index of Australia, 11 Aboriginal and Torres Strait Islander (ATSI) status, and children's age, gender and level of schooling.
Caregivers were asked to report about a typical week from June to September 2020 compared to pre‐pandemic (defined as before March 2020). The impact of varying COVID‐19 pandemic restrictions, and specifically Victoria's lockdown, on children's life‐style was investigated using nine items assessing each child for: (i) time spent physically active, (ii) time spent outdoors, (iii) daily amount of sleep, (iv) difficulty falling/staying asleep, (v) connection to friends, (vi) connection to caregiver, (vii) unhealthy food consumption, (viii) fruit and vegetable consumption and (ix) amount of recreational screen time. Caregivers responded using a 5‐point Likert scale (options: a lot less, a little less, about the same, a little more and a lot more), which was converted into a 3‐point Likert scale, combining ‘a lot less’ and ‘a little less’ as ‘less’; ‘a lot more’ and ‘a little more’ as ‘more’ and retaining ‘about the same’.
Survey questions required a sixth‐grade level of literacy and were administered in English without provision of translators, meaning caregivers who did not speak English were unable to participate.
Data analysis
Demographic characteristics were reported as number (n) and percentage (%) separately for Victoria and NSW, while the remaining Australian states and territories were all combined (other states and territories). The impact on children's health‐related behaviours was reported as ‘more’, ‘about the same’ and ‘less’ using numbers and weighted proportions.
Changes in children's health‐related behaviours were assessed as either ‘more’ or ‘less’ compared to ‘about the same’ in both directions. To assess how the severity of lockdown impacted children's health‐related behaviours compared to pre‐pandemic, we analysed impacts as either ‘more’ or ‘less’ compared to ‘about the same’ to avoid missing significant changes in behaviour in either direction from children's' baselines. Hence, we compared ‘less’ against ‘about the same’ for each of the nine items excluding ‘more’. Subsequently, we compared ‘more’ against ‘about the same’ excluding ‘less’. We used logistic regression to assess changes in children's health‐related behaviours between Victoria, NSW and other states and territories during Victoria's lockdown both unadjusting and adjusting for the effect of caregiver demographics (age, gender, family structure, education, income, employment, remoteness and their corresponding child's education, age and gender). A generalised estimating equation was used to account for clustering of children within families. All estimates except for the demographic characteristics (Table 1) were weighted for caregiver's age, gender, number of children in family, state of residence, ATSI status and Socio‐Economic Indexes for Areas based on the Index of Relative Socio‐Economic Advantage and Disadvantage reflecting the distribution of Australian parent population using figures from the ABS. 12 Data were analysed using IBM SPSS Statistics version 27. 13
Table 1.
Demographic characteristics of the caregivers and children surveyed during September 2020 by Victorian, New South Wales, and other states and territories. Characteristics are reported as number (n) and proportions (%)
| Demographic information | VIC, n (%) | NSW, n (%) | Other states and territories, n (%) | Total, n (%) |
|---|---|---|---|---|
| Caregiver information | ||||
| Total | 386 | 387 | 449 | 1222 |
| Age group | ||||
| 18–29 years | 11 (2.2) | 11 (4.3) | 6 (1.4) | 28 (2.8) |
| 30–39 years | 95 (41.3) | 123 (41.5) | 126 (35.8) | 344 (39.8) |
| 40–49 years | 215 (47.2) | 207 (45.9) | 244 (55.5) | 666 (49.1) |
| >50 years | 65 (9.3) | 46 (8.2) | 73 (7.2) | 184 (8.3) |
| Gender | ||||
| Female | 200 (55.8) | 212 (61.5) | 226 (59.5) | 638 (59.1) |
| Family structure | ||||
| Single parent | 70 (15.1) | 77 (20.0) | 89 (15.1) | 236 (17.0) |
| Level of education completed | ||||
| Year 12 or less | 70 (15.9) | 62 (20.1) | 79 (18.0) | 211 (18.1) |
| Certificate/diploma or trade/apprenticeship | 84 (23.3) | 112 (30.4) | 143 (32.8) | 339 (28.8) |
| Undergraduate or post‐graduate | 232 (60.7) | 213 (49.5) | 227 (49.2) | 672 (53.1) |
| Country of birth | ||||
| Born in Australia | 296 (75.1) | 306 (80.6) | 329 (70.5) | 931 (75.8) |
| Speaks language other than English at home | ||||
| Yes | 88 (21.1) | 100 (28.0) | 72 (12.9) | 260 (21.3) |
| Aboriginal or Torres Strait Islander status | ||||
| Aboriginal or Torres Strait Islander | 15 (3.9) | 18 (4.7) | 14 (3.1) | 47 (3.9) |
| Region of caregiver's accommodation | ||||
| Metropolitan | 339 (83.3) | 339 (85.9) | 339 (6.0) | 1017 (82.2) |
| Regional | 47 (16.7) | 48 (14.1) | 110 (24.0) | 205 (17.8) |
| Employment status | ||||
| Full‐time | 215 (56.3) | 217 (50.0) | 240 (54.8) | 672 (53.5) |
| Part‐time or casual | 91 (19.2) | 91 (24.0) | 103 (22.7) | 285 (22.0) |
| Unemployed, retired and home duties | 80 (24.4) | 79 (26.1) | 106 (22.5) | 265 (24.5) |
| No. of children | ||||
| One child | 165 (29.9) | 127 (29.5) | 163 (26.4) | 455 (28.7) |
| Two or more children | 221 (70.1) | 260 (70.5) | 286 (73.6) | 767 (71.3) |
| Total | 617 | 636 | 758 | 2011 |
| Age group | ||||
| 5 to <13 years | 388 (68.7) | 437 (71.9) | 477 (67.7) | 1302 (69.6) |
| 13 to <18 years | 229 (31.3) | 199 (28.1) | 281 (32.3) | 709 (30.4) |
| Gender | ||||
| Female | 319 (51.3) | 316 (51.4) | 353 (43.4) | 988 (49.0) |
| Child's school, pre‐school or childcare status | ||||
| None | 12 (1.5) | 14 (2.4) | 20 (1.7) | 46 (1.9) |
| Childcare | 5 (0.6) | 18 (2.9) | 9 (0.8) | 32 (1.5) |
| Pre‐school (kindergarten) | 45 (8.2) | 72 (15.0) | 32 (4.5) | 149 (9.6) |
| School (including Prep, Foundation, Reception, Pre‐primary or home schooling) | 555 (89.7) | 532 (79.6) | 697 (93.1) | 1784 (87.0) |
Ethics
Participants were compensated with points to be exchanged for department store gift cards.
Results
Demographics
A total of 1984 caregivers of children aged less than 18 years among 2445 invited caregivers participated in the survey. Among the total caregivers, 1222 caregivers of children aged 5–17; 386 (31.6%) from Victoria, 387 (31.7%) from NSW, and 449 (36.7%) from other states and territories, were included in this study. Caregivers reported for each of their children, totalling 2011: 617 (30.7%) from Victoria, 636 (31.6%) from NSW and 758 (37.7%) from other states and territories.
Close to half of caregivers were 40–49 years old (49.1%, n = 666), female (59.1%, n = 638) and 17.0% (n = 236) were single parents. Most respondents (81.9%, n = 1011) completed at least a high school level of education. Most respondents resided in cities (82.2%, n = 1017). Detailed sample demographics are provided in Table 1.
Impact of COVID‐19 pandemic restrictions on children's life‐styles
Impacts of pandemic restrictions on children's life‐style as reported by caregivers are presented in Figure 1.
Fig. 1.
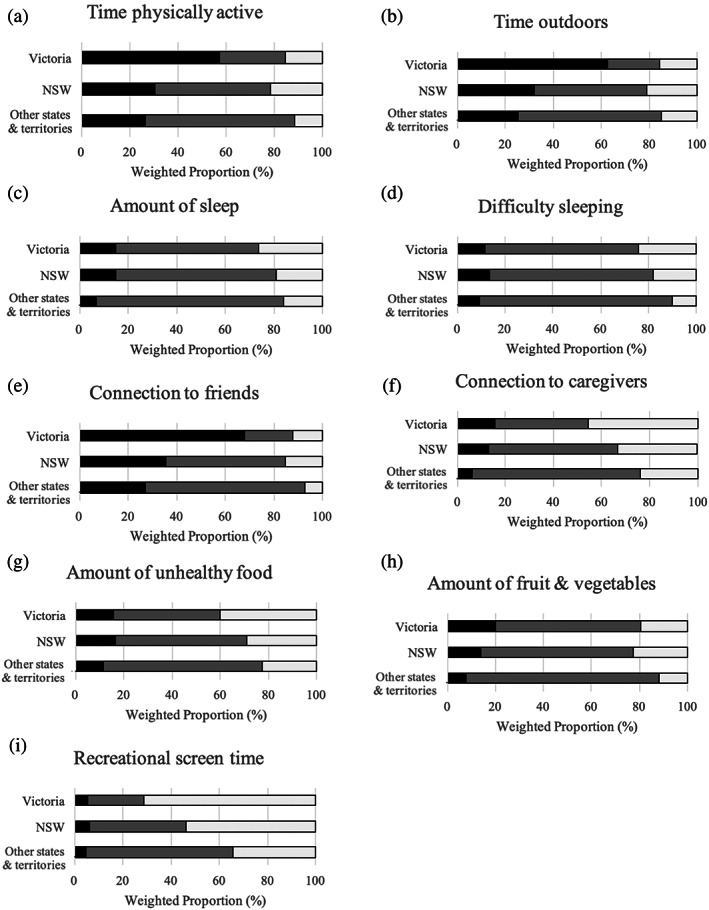
Impacts of COVID‐19 pandemic restrictions and lockdown on children's health‐related behaviours in Victoria (804), NSW (807) and other States and Territories (939) surveyed during September 2020. (a) Time spent outdoors, (b) Time physically active, (c) Amount of sleep, (d) Sleep difficulty, (e) Connection to friends, (f) Connection to caregivers, (g) Amount of unhealthy food, (h) Amount of fruit and vegetables, and (i) Recreational screen time. ( ) Less, (
) Less, ( ) About the same and (
) About the same and ( ) More.
) More.
Physical activity
Most (weighted 57.2%, n = 352) Victorian children were reported to be less physically active during the study period, compared to 30.3% (weighted, n = 183) of NSW children (adjusted odds ratio (AOR) = 3.7, 95% confidence interval (CI): 2.5–5.5, Table 2) and 26.5% (weighted, n = 182) of children from other states and territories (AOR: 5.6, 95% CI: 3.7–8.5). Similarly, most Victorian children were reported to spend less time outdoors during lockdown (weighted 62.6%, n = 383), compared to 32.0% (weighted, n = 198) NSW children (AOR = 4.5, 95% CI: 2.9–6.9) and 25.2% (weighted, n = 184) of children in other states and territories (AOR = 7.0, 95% CI: 4.4–11.1). Most Victorian children (weighted 71.3%, n = 440) were reported to experience increased recreational screen time during lockdown, compared to 53.9% (weighted, n = 333) (AOR = 2.4, 95% CI: 1.6–3.6) of NSW children, and 34.5% (weighted, 305) (AOR = 5.9, 95% CI: 3.9–8.9) of children in other states and territories (Table 3).
Table 2.
Parent's perception of changes to health‐related behaviour due to COVID in Victoria, New South Wales and other states and territories surveyed during Victoria's lockdown in September 2020. Proportions were reported as ‘about the same’ against ‘less’ for each group. Values reported as number (n) with proportion (%, weighted†) or odds ratio (OR) with 95% confidence intervals (CIs) and P values (unadjusted and adjusted‡) unless otherwise specified
| VIC, n (%, weighted†) | Other states and territories, n (%, weighted†) | VIC compared to other states and territories | VIC compared to NSW | |||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR† (95% CI; P value) | Adjusted‡ OR† (95% CI; P value) | VIC, n (%, weighted†) | NSW, n (%, weighted†) | Unadjusted OR† (95% CI; P value) | Adjusted‡ OR† (95% CI; P value) | |||
| Time spent being physically active | ||||||||
| About the same | 168 (32.3) | 480 (70.1) | 1.0 | 1.0 | 168 (32.3) | 316 (61.5) | 1.0 | 1.0 |
| Less | 352 (67.7) | 182 (29.9) | 4.9 (3.2–7.5; P < 0.001) | 5.6 (3.7–8.5; P < 0.001) | 352 (67.7) | 183 (38.5) | 3.4 (2.2–5.0; P < 0.001) | 3.7 (2.5–5.5; P < 0.001) |
| Time spent outdoors | ||||||||
| About the same | 132 (25.8) | 461 (70.3) | 1.0 | 1.0 | 132 (25.8) | 299 (59.5) | 1.0 | 1.0 |
| Less | 383 (74.2) | 184 (29.7) | 6.8 (4.3–10.7; P < 0.001) | 7.0 (4.4–11.1; P < 0.001) | 383 (74.2) | 198 (40.5) | 4.2 (2.7–6.6; P < 0.001) | 4.5 (2.9–6.9; P < 0.001) |
| Amount of sleep per day | ||||||||
| About the same | 365 (79.3) | 614 (91.8) | 1.0 | 1.0 | 365 (79.3) | 445 (81.3) | 1.0 | 1.0 |
| Less | 96 (20.7) | 45 (8.2) | 2.9 (1.5–5.7; P = 0.001) | 3.4 (1.8–6.5; P < 0.001) | 96 (20.7) | 81 (18.7) | 1.1 (0.7–1.9; P = 0.64) | 1.4 (0.9–2.4; P = 0.14) |
| Difficulty falling or staying asleep | ||||||||
| About the same | 393 (84.6) | 629 (89.4) | 1.0 | 1.0 | 393 (83.3) | 446 (89.4) | 1.0 | 1.0 |
| Less | 84 (15.4) | 56 (10.6) | 1.5 (0.8–2.9; P = 0.118) | 1.5 (0.8–2.8; P = 0.23) | 84 (15.4) | 85 (16.7) | 0.9 (0.5–1.5; P = 0.71) | 1.0 (0.6–1.6; P = 0.90) |
| Being connected to friends | ||||||||
| About the same | 123 (22.5) | 480 (70.5) | 1.0 | 1.0 | 123 (22.5) | 323 (58.2) | 1.0 | 1.0 |
| Less | 415 (77.5) | 191 (29.5) | 8.2 (5.2–12.8; P < 0.001) | 9.6 (6.1–15.2; P < 0.001) | 415 (77.5) | 213 (41.8) | 4.8 (3.1–7.4; P < 0.001) | 4.9 (3.2–7.6; P < 0.001) |
| Being connected to caregivers | ||||||||
| About the same | 272 (71.5) | 536 (91.8) | 1.0 | 1.0 | 272 (71.5) | 356 (80.4) | 1.0 | 1.0 |
| Less | 88 (28.5) | 44 (8.2) | 4.5 (2.1–9.6; P < 0.001) | 4.5 (2.0–10.0; P < 0.001) | 88 (28.5) | 70 (19.6) | 1.6 (0.9–3.0; P = 0.11) | 1.7 (1.0–2.9; P = 0.075) |
| Amount of unhealthy food eaten | ||||||||
| About the same | 270 (73.5) | 502 (85.3) | 1.0 | 1.0 | 270 (73.5) | 352 (76.9) | 1.0 | 1.0 |
| Less | 104 (26.5) | 66 (14.7) | 2.1 (1.1–4.0; P = 0.022) | 1.8 (1.0–3.4; P = 0.066) | 104 (26.5) | 105 (23.1) | 1.3 (0.7–2.1; P = 0.52) | 1.1 (0.7–2.0; P = 0.64) |
| Amount of fruit and vegetables eaten | ||||||||
| About the same | 382 (75.7) | 599 (87.3) | 1.0 | 1.0 | 382 (75.7) | 401 (73.7) | 1.0 | 1.0 |
| Less | 133 (24.3) | 97 (12.7) | 2.2 (1.3–3.7; P = 0.004) | 2.1 (1.2–3.7; P = 0.007) | 133 (24.3) | 160 (26.3) | 0.9 (0.6–1.4; P = 0.90) | 0.9 (0.6–1.4; P = 0.57) |
| Amount of time using screens and digital media for entertainment (not school/education) | ||||||||
| About the same | 141 (80.4) | 427 (92.8) | 1.0 | 1.0 | 141 (80.4) | 260 (86.0) | 1.0 | 1.0 |
| Less | 36 (19.6) | 26 (7.2) | 3.1 (1.2–8.4; P = 0.023) | 3.2 (1.1–10.1; P = 0.040) | 36 (19.6) | 43 (14.0) | 1.5 (0.7–3.2; P = 0.29) | 1.3 (0.7–2.6; P = 0.45) |
All estimates except for the demographic characteristics were weighted for caregiver's age, gender, number of children, state of residence, ATSI status and Socio‐Economic Indexes for Areas based on the Index of Relative Socio‐Economic Advantage and Disadvantage reflecting the distribution of Australian parent population using figures from the ABS. 13
Adjusted for the effect of caregiver demographics (age, gender, family structure, education, income, employment, remoteness and their corresponding child's education, age and gender).
Table 3.
Parent's perception of changes to health‐related behaviour due to COVID in Victoria, New South Wales and other states and territories surveyed during Victoria's lockdown in September 2020. Proportions were reported as ‘about the same’ against ‘more’ for each group. Values reported as number (n) with proportion (%, weighted†) or odds ratio (OR) with 95% confidence intervals (CIs) and P values (unadjusted and adjusted‡) unless otherwise specified
| VIC, n (%, weighted†) | Other states and territories, n (%, weighted†) | VIC compared to other states and territories | VIC compared to NSW | |||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted OR† (95% CI; P value) | Adjusted‡ OR† (95% CI; P value) | VIC, n (%, weighted†) | NSW, n (%, weighted†) | Unadjusted OR† (95% CI; P value) | Adjusted‡ OR† (95% CI; P value) | |||
| Time spent being physically active | ||||||||
| About the same | 168 (63.6) | 480 (84.4) | 1.0 | 1.0 | 168 (63.6) | 316 (69.2) | 1.0 | 1.0 |
| More | 97 (36.4) | 96 (15.6) | 3.1 (1.7–5.5; P < 0.001) | 3.2 (1.8–5.6; P < 0.001) | 97 (36.4) | 137 (30.8) | 1.3 (0.8–2.2; P = 0.35) | 1.4 (0.8–2.3; P = 0.25) |
| Time spent outdoors | ||||||||
| About the same | 132 (58.2) | 461 (79.8) | 1.0 | 1.0 | 132 (58.2) | 299 (68.9) | 1.0 | 1.0 |
| More | 102 (41.8) | 113 (20.2) | 2.8 (1.6–5.0; P < 0.001) | 3.1 (1.7–5.5; P < 0.001) | 102 (41.8) | 139 (31.1) | 1.6 (0.9–2.7; P = 0.081) | 1.7 (1.0–2.8; P = 0.061) |
| Amount of sleep per day | ||||||||
| About the same | 365 (68.9) | 614 (82.9) | 1.0 | 1.0 | 365 (68.9) | 445 (77.5) | 1.0 | 1.0 |
| More | 156 (31.1) | 99 (17.1) | 2.2 (1.4–3.5; P = 0.001) | 2.0 (1.2–3.3; P = 0.009) | 156 (31.1) | 110 (22.5) | 1.6 (1.0–2.4; P = 0.056) | 1.6 (1.1–2.6; P = 0.029) |
| Difficulty falling or staying asleep | ||||||||
| About the same | 393 (72.7) | 629 (88.7) | 1.0 | 1.0 | 393 (72.7) | 446 (79.0) | 1.0 | 1.0 |
| More | 140 (27.3) | 73 (11.3) | 3.0 (1.8–4.9; P < 0.001) | 3.4 (2.0–5.9; P < 0.001) | 140 (27.3) | 105 (21.0) | 1.4 (0.9–2.2; P = 0.14) | 1.6 (1.0–2.5; P = .0035) |
| Being connected to friends | ||||||||
| About the same | 123 (61.9) | 480 (89.9) | 1.0 | 1.0 | 123 (61.9) | 323 (76.4) | 1.0 | 1.0 |
| More | 79 (38.1) | 87 (10.1) | 5.5 (2.9–10.2; P < 0.001) | 5.6 (2.8–11.3; P < 0.001) | 79 (38.1) | 100 (23.6) | 2.0 (1.1–3.7; P = 0.030) | 2.1 (1.1–3.9; P = 0.020) |
| Being connected to caregivers | ||||||||
| About the same | 272 (46.4) | 536 (74.7) | 1.0 | 1.0 | 272 (46.4) | 356 (61.6) | 1.0 | 1.0 |
| More | 257 (53.6) | 178 (25.3) | 3.4 (2.2–5.2; P < 0.001) | 3.5 (2.2–5.4; P < 0.001) | 257 (53.6) | 210 (38.4) | 1.9 (1.2–2.8; P = 0.002) | 1.9 (1.3–2.8; P = 0.002) |
| Amount of unhealthy food eaten | ||||||||
| About the same | 270 (52.5) | 502 (74.5) | 1.0 | 1.0 | 270 (52.5) | 352 (65.5) | 1.0 | 1.0 |
| More | 243 (47.5) | 190 (25.5) | 2.6 (1.7–3.1; P < 0.001) | 2.8 (1.8–4.3; P < 0.001) | 243 (47.5) | 179 (34.5) | 1.7 (1.1–2.6; P = 0.009) | 1.9 (1.3–2.8; P = 0.002) |
| Amount of fruit and vegetables eaten | ||||||||
| About the same | 382 (75.7) | 599 (87.3) | 1.0 | 1.0 | 382 (75.7) | 401 (73.7) | 1.0 | 1.0 |
| More | 133 (24.3) | 97 (12.7) | 2.2 (1.3–3.7; P = 0.004) | 2.1 (1.2–3.7; P = 0.007) | 133 (24.3) | 160 (26.3) | 0.9 (0.6–1.4; P = 0.62) | 0.9 (0.6–1.4; P = 0.57) |
| Amount of time using screens and digital media for entertainment (not school/education) | ||||||||
| About the same | 141 (24.5) | 427 (63.8) | 1.0 | 1.0 | 141 (24.5) | 260 (42.4) | 1.0 | 1.0 |
| More | 440 (75.5) | 305 (36.2) | 5.4 (3.6–8.3; P < 0.001) | 5.9 (3.9–8.9; P < 0.001) | 440 (75.5) | 333 (57.6) | 2.3 (1.5–3.5; P < 0.001) | 2.4 (1.6–3.6; P < 0.001) |
All estimates except for the demographic characteristics were weighted for caregiver's age, gender, number of children, state of residence, ATSI status and Socio‐Economic Indexes for Areas based on the Index of Relative Socio‐Economic Advantage and Disadvantage reflecting the distribution of Australian parent population using figures from the ABS. 13
Adjusted for the effect of caregiver demographics (age, gender, family structure, education, income, employment, remoteness and their corresponding child's education, age and gender).
Sleep
Victorian children were reported to have slightly increased difficulty sleeping (weighted 24.1%, n = 140) compared to NSW (weighted 18.1%, n = 105) (AOR = 1.6, 95% CI: 1.0–2.5) and other states and territories (weighted 10.2%, n = 73) (AOR = 3.4, 95% CI: 2.0–5.9). Similarly, Victorian children reported to have increased amount of sleep (weighted 26.3%, n = 156) was slightly higher than NSW children (weighted 19.1%, n = 110) (AOR = 1.6, 95% CI: 1.1–2.6) and other states and territories (weighted 15.9%, n = 99) (AOR = 2.0, 95% CI: 1.2–3.3).
Diet
Victorian children were reported to have similar increases in fruit and vegetable intake during lockdown (weighted 19.4%, n = 133) as NSW children (weighted 22.7%, n = 160) (AOR = 0.9, 95% CI: 0.6–1.4) but higher increase compared to other states and territories (weighted 11.7%, n = 97) (AOR = 2.1, 95% CI: 1.2–3.7). Victorian children were reported eating more unhealthy food (weighted 39.9%, n = 243) compared to children in both NSW (weighted 28.8%, n = 179) (AOR = 1.9, 95% CI: 1.3–2.8) and other states and territories (weighted 22.6%, n = 190) (AOR = 2.8, 95% CI: 1.8–4.3).
Connection to peers and caregivers
Most (68% weighted, n = 415) Victorian children were reported to feel less connected to their peers during lockdown, compared to 35.4% (weighted, n = 213) NSW children (AOR = 4.9, 95% CI: 3.2–7.6) and 27.3% (weighted, n = 191) of children from other states and territories (AOR = 9.6, 95% CI: 6.1–15.2). Contrastingly, 45.3% (weighted, n = 257) of Victorian children were reported to have increased connection to caregivers, compared to 33.4% (weighted, n = 210) of NSW children (AOR = 1.9, 95% CI: 1.3–2.8) and 23.7% (weighted, n = 178) of children in other states and territories (AOR = 3.5, 95% CI: 2.2–5.4).
Impact of COVID‐19 pandemic restrictions on children's life‐styles by age group
The effects of varying levels of pandemic restrictions on health‐related behaviours in children were reported to be similar between children aged 5–12 years and 13–17 years except for sleep duration in Victoria and recreational screen time in other states and territories (Fig. S1).
Discussion
This is the first study to investigate the effects of restrictions differing in severity and duration on a broad range of children's health‐related behaviours. In contrast to other studies, we compared differing restrictions in Victoria and NSW against other states and territories, which acted as a national control group due to the absence of strict regulations. Our results suggest a dose–response relationship between severity and duration of pandemic restrictions and impacts on children's life‐styles. As hypothesised, Victorian children, who experienced more severe restrictions, were more likely to experience greater impacts and predominantly more negative impacts to their health‐related behaviours than children in NSW and other states and territories. This is in the context of NSW children who experienced fewer restrictions for a shorter period, and other jurisdictions that did not impose restrictions during the study period.
Our results are consistent with previous studies demonstrating associations between lockdown and increased sedentary behaviours in children largely as a result of increased screen time, 2 decreased physical activity and the disruption to organised sport activities. 1 These findings have implications for the current and future health of affected children, as lockdown‐related sedentariness was positively correlated with negative moods 1 and sedentary habits created in childhood often persist into adulthood. 14 Contrasting with German reports of increased physical activity of adolescents' during the pandemic, our findings support Greek and Australian studies suggesting time‐based outdoor restrictions are detrimental to children's physical activity levels. 1 , 2 , 3 , 4 Pandemic restrictions increased sedentary activity, including screen‐based activity across Australia, with effects greatest in Victorian children. 15 Decreased physical activity in other states may be explained by a correlation between fears of catching COVID‐19 and behaviour changes. 4 In context, under 20% of Australian teenagers met physical activity or daily screen time guidelines in 2018. 16 Victorian children's further regression from a low pre‐COVID baseline is concerning for preventable long‐term health conditions. 3 , 17
Researchers have hypothesised that children slept longer but with greater disturbance due to changed schedules and increased sedentary activity during lockdowns. 18 While our results support a potential link between sleep duration and lockdown, we did not find a substantial increase in sleep difficulties despite Victorian children's increased sedentary activity. 1 , 18
The impact of lockdown on diet has seen polarising effects on children's nutrition world‐wide. 3 , 5 , 6 Remote learning in French children was linked to increased boredom and stress and greater accessibility to food during school hours, contributing to emotional overeating. 5 This is mirrored in our findings of more unhealthy food behaviours in Victorian children, possibly exacerbated by the established link between increased screen time and unhealthy snacking. 10 However, more flexibility for caregivers working from home may have allowed time for home‐cooked meals and increased children's fruit and vegetable intake. 3 , 9
Previous research found social isolation due to lockdown increased loneliness in youth. 2 , 3 , 7 Our finding of decreased peer connectivity among Victorian children is concerning given prolonged peer‐related loneliness predisposes children to depression in adolescence. 19 This may be mitigated through online social interaction to protect mental well‐being. 2 Our results support mixed findings on the impact of lockdown on children's relationships with caregivers. 3 , 7 Forced time together either raised conflicts 7 or created opportunities for positive habits and shared activities. 3
Little research exists on the longitudinal impacts of pandemic restrictions on health‐related behaviours. A study of English adults showed that 29% of participants had persistent reduced physical activity post‐lockdown. 20 Children's increase in sedentary behaviour may persist due to poor re‐engagement with extracurricular activities due to low motivation and fear, 21 while increased screen usage and less outdoor activity pose risks for early‐onset short‐sightedness 17 and poorer mental wellbeing. 22 As half of the adults with mental health disorders experience their onset by mid‐teens, policies should focus on ways to prevent deterioration of children's health‐related behaviours affected by pandemic restrictions in order to improve long‐term mental health outcomes. 23
Some limitations of our study include the possibility of social desirability bias due to underreporting of less desirable behaviours and overestimation of socially acceptable behaviours; however, respondent anonymity may have reduced the potential for this. The study design required parents to respond for their children, future research could address the potential for measurement bias through parent‐led behaviour diaries or children self‐reporting. In addition, as a retrospective study, there is potential for recall bias. In Victoria, the caregivers may have over reported behaviour changes due to frustrations with ongoing lockdowns. Age‐related changes in child behaviour may have occurred over the six‐month recall period, irrespective of pandemic restrictions. We have included the age of the child in the statistical model and explored comparison between states to control for the potential age effect. Metropolitan children were not separated from regional children in Victoria, where restrictions were less severe during the survey period. However, children in regional Victoria experienced harsher restrictions than in NSW, where restrictions were consistent state‐wide. Eligibility for the COVID vaccine commenced near the end of the survey period for 12–15 year olds, with 5–11 year olds remaining ineligible. Hence, uptake of vaccination in the 12–15 year old age group and subsequently caregivers' decision‐making for their children's activity may have a limited influence on the study findings. Furthermore, we did not identify the characteristics of children at risk of multiple adverse health‐related behaviours which could be redressed in future studies so that targeted interventional strategies are directed at children needing the most help. Transferability of our findings to the non‐English speaking Australian population may also be limited by English literacy requirements and future studies may want to address language inclusivity within survey delivery. Additionally, the effect of cultural backgrounds on parental response to pandemic restrictions is an important area of research for future studies to provide targeted interventional strategies and would be best explored using qualitative methodology.
Conclusions
Our findings show more severe and longer COVID‐19 pandemic restrictions, including lockdowns, are associated with greater impacts and predominantly more negative impacts on child health‐related behaviours with serious implications for children's current and future physical and mental wellbeing. Considering the ongoing risk of COVID‐19 and the emergence of new variants, our findings have significant relevance for the future use of lockdowns and pandemic restrictions in public health policies world‐wide. Immediate government action post‐pandemic restrictions are required to mitigate the long‐term health effects of lockdowns on children through policies and programs to encourage healthier life‐style behaviours. Future policies to control pandemics, should allow increased outdoor activity and ‘social bubbles’ for children to support their physical and mental health.
Supporting information
Figure S1 Impacts of COVID‐19 pandemic restrictions and lockdown on children's health‐related behaviours in Victoria (617), NSW (636) and other States and Territories (761) surveyed during September 2020 represented as children aged 5 to <13 and 13 to <18 years.
Acknowledgements
The Royal Children's Hospital Australian Child Health Poll is a research concept developed with the support of Professor Gary Freed of the CS Mott Children's Hospital in Ann Arbor, Michigan, who has been leading the US National Poll on Child Health since its inception and launch in 2007 (http://mottnpch.org/). The authors would like to thank all clinicians, experts and researchers who contributed to the development of Royal Children's Hospital National Child Health Poll. The Authors are also grateful to the Royal Children's Hospital Communication Team for developing communication materials based on the findings of poll. The authors are also thankful to the participants of the Royal Children's Hospital poll and the poll sponsor, the Royal Children's Hospital Foundation for funding this research (Grant number 2018‐1003). Lauren Robinson conducted the statistical analysis, analysed and interpreted all data and wrote the manuscript. Dr Mary‐Anne Measey provided epidemiological expertise in the design of the study and revised the manuscript. A.Prof Darryl Efron provided paediatric and child developmental expertise in the design of the study and revised the manuscript. Dr Lisa Mundy provided expertise in interpreting the results with respect to developmental psychology and reviewed the manuscript. Dr Monsurul Hoq provided advice and support on statistical analysis, contributed to the design of the study and was a major contributor in writing the manuscript. Dr Anthea Rhodes conceived the study, contributed to the design of the study and was a major contributor in writing the manuscript. All authors contributed to the interpretation of the data, read and approved the final manuscript as submitted and agree to be accountable for all aspects of the work. Open access publishing facilitated by The University of Melbourne, as part of the Wiley ‐ The University of Melbourne agreement via the Council of Australian University Librarians.
Conflict of interest: None declared.
Data Availability Statement
Individual participant data that underlie the results (text, tables, figures and appendix) reported in this article, after de‐identification, will be shared upon request between 9 months and ending 36 months following publication of the article. Requests will be honoured from researchers who provide a methodologically sound proposal and execute a Data Use Agreement with National Child Health Poll. Requests should be directed by email to the corresponding author.
References
- 1. Morres ID, Galanis E, Hatzigeorgiadis A, Androutsos O, Theodorakis Y. Physical activity, sedentariness, eating behavior and well‐being during a COVID‐19 lockdown period in Greek adolescents. Nutrients 2021; 13: 1449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Li SH, Beames JR, Newby JM, Maston K, Christensen H, Werner‐Seidler A. The impact of COVID‐19 on the lives and mental health of Australian adolescents. Eur. Child Adolesc. Psychiatry 2021; 28: 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Rhodes A. COVID‐19 pandemic: Effects on the lives of Australian children and families. Parkville, Vic: Royal Children's Hospital National Child Health Poll; 2020 [updated 2020 Jul 18; cited 2021 Jul 17]. Available from: https://www.rchpoll.org.au/wp-content/uploads/2020/07/nchp-poll18-report-covid.pdf
- 4. Schmidt SCE, Anedda B, Burchartz A et al. Physical activity and screen time of children and adolescents before and during the COVID‐19 lockdown in Germany: A natural experiment. Sci. Rep. 2020; 10: 21780. https://www.nature.com/articles/s41598-020-78438-4#citeas. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Philippe K, Chabanet C, Issanchou S, Monnery‐Patris S. Child eating behaviors, parental feeding practices and food shopping motivations during the COVID‐19 lockdown in France: (how) did they change? Appetite 2021; 161: 105132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Ruiz‐Roso MB, de Carvalho PP, Mantilla‐Escalante DC et al. Covid‐19 confinement and changes of adolescent's dietary trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020; 12: 1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Evans S, Mikocka‐Walus A, Klas A et al. From "it has stopped our lives" to "spending more time together has strengthened bonds": The varied experiences of Australian families during COVID‐19. Front. Psychol. 2020; 11: 588667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Murray‐Atfield, Y , Dunstan, J . Melbourne placed under stage 4 coronavirus lockdown, stage 3 for rest of Victoria as state of disaster declared. ABC News; 2020 Aug 2 [cited 2021 Jul 15]. Available from: https://www.abc.net.au/news/2020‐08‐02/victoria‐coronavirus‐restrictions‐imposed‐death‐toll‐cases‐rise/12515914
- 9. NSW Premier Deputy Premier, Minister for Digital, Minister for Customer Service . COVID‐19 Restrictions to be Tightened. Sydney, NSW: NSW Government; 2020 [updated 2020 Jul 17; cited 2021 Jul 16]. Available from: https://www.nsw.gov.au/media‐releases/covid‐19‐restrictions‐to‐be‐tightened
- 10. Marsh S, Ni Mhurchu C, Maddison R. The non‐advertising effects of screen‐based sedentary activities on acute eating behaviors in children, adolescents, and young adults. A systematic review. Appetite 2013; 71: 259–73. [DOI] [PubMed] [Google Scholar]
- 11. Australian Bureau of Statistics . Australian Statistical Geography Standard (ASGS): Volume 5 – Remoteness Structure, July 2016. Belconnen, ACT: ABS; 2016 [updated 2018 Mar 16; cited 2021 Oct 13]. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.005
- 12. Australian Bureau of Statistics . Census of Population and Housing: Socio‐Economic Indexes for Areas (SEIFA), Australia, 2016. Belconnen, ACT: ABS; 2016 [updated 2018 Mar 27; cited 2021 Oct 13]. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSAD~20
- 13. International Business Machines Corportation . Chicago IL: IBM; 2021. Downloading IBM SPSS Statistics 27; 2021 May 21 [cited 2021 Sep 2]. Available from: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-27
- 14. van Ekris E, Wijndaele K, Altenburg TM et al. Tracking of total sedentary time and sedentary patterns in youth: A pooled analysis using the International Children's Accelerometry Database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2020; 17: 65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Australian Government Department of Health . Exercising and Staying Active During Coronavirus (COVID‐19) Restrictions. Canberra, ACT: Department of Health; 2021 [updated 2021 Jul 7; cited 2021 Sep 16]. Available from: https://www.health.gov.au/news/health‐alerts/novel‐coronavirus‐2019‐ncov‐health‐alert/ongoing‐support‐during‐coronavirus‐covid‐19/exercising‐and‐staying‐active‐during‐coronavirus‐covid‐19‐restrictions
- 16. Active Healthy Kids Australia . Muscular Fitness: It's Time for a Jump Start. The 2018 Active Healthy Kids Australia Report Card on Physical Activity for Children and Young People. Adelaide, South Australia: Active Healthy Kids Australia; 2018 [updated 2018 Nov 27; cited 2021 Sep 13]. Available from: 10.25954/5b862301479a1 [DOI]
- 17. Wong CW, Tsai A, Jonas JB et al. Digital screen time during the COVID‐19 pandemic: Risk for a further myopia boom? Am. J. Ophthalmol. 2020; 223: 333–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Altena E, Baglioni C, Espie CA et al. Dealing with sleep problems during home confinement due to the COVID‐19 outbreak: Practical recommendations from a task force of the European CBT‐I academy. J. Sleep Res. 2020; 29: e13052. [DOI] [PubMed] [Google Scholar]
- 19. Qualter P, Brown SL, Munn P, Rotenberg KJ. Childhood loneliness as a predictor of adolescent depressive symptoms: An 8‐year longitudinal study. Eur. Child Adolesc. Psychiatry 2009; 19: 493–501. [DOI] [PubMed] [Google Scholar]
- 20. Bu F, Bone JK, Mitchell JJ, Steptoe A, Fancourt D. Longitudinal changes in physical activity during and after the first national lockdown due to the COVID‐19 pandemic in England. Sci. Rep. 2021; 11: 17723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Elliott S, Drummond MJ, Prichard I, Eime R, Drummond C, Mason R. Understanding the impact of COVID‐19 on youth sport in Australia and consequences for future participation and retention. BMC Public Health 2020; 21: 448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Jackson SB, Stevenson KT, Larson LR, Peterson MN, Seekamp E. Outdoor activity participation improves adolescents' mental health and well‐being during the COVID‐19 pandemic. Int. J. Environ. Res. Public Health 2021; 18: 2506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kessler RC, Amminger GP, Aguilar‐Gaxiola S, Alonso J, Lee S, Ustün TB. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2008; 20: 359–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Impacts of COVID‐19 pandemic restrictions and lockdown on children's health‐related behaviours in Victoria (617), NSW (636) and other States and Territories (761) surveyed during September 2020 represented as children aged 5 to <13 and 13 to <18 years.
Data Availability Statement
Individual participant data that underlie the results (text, tables, figures and appendix) reported in this article, after de‐identification, will be shared upon request between 9 months and ending 36 months following publication of the article. Requests will be honoured from researchers who provide a methodologically sound proposal and execute a Data Use Agreement with National Child Health Poll. Requests should be directed by email to the corresponding author.