

Abstract
Colonic lipomas, even though rare, are the most common intramural tumor and the second-most common benign tumor of the colon after adenomatous polyps. We present the case of a 4-year-old boy with a large rectal lipoma causing anal prolapse, bleeding, and constipation, to discuss differential diagnostic problems and the proper management. A 4-year-old boy presented with symptoms of anal prolapse and constipation. Anal prolapse was accompanied by a tumor that occasionally was bleeding. Computed tomography was performed to determine the origin of the tumor and its relations with the surrounding tissues. Excision of the mass was performed through retraction through the anus and the anal wall was closed with sutures. Histopathological findings revealed a submucosal lipoma of a 5 cm diameter, with the erosions of the overlying mucosa. The patient was discharged after 3 days with no postoperative complications. Colonic lipomas, even though rare, are the second-most common benign tumor of the colon. Essential reasons for the resection are the potential complications, such as abdominal pain, change in bowel pattern, bleeding, obstruction, intussusception, perforation, and rarely transformation into a liposarcoma. Resection is performed endoscopically if the tumor is <2 cm in diameter and has a narrow base that allows safe ligation. Otherwise, the open procedure should be considered. In our case, prolapse of the mass through the anal canal allowed the transanal resection.
KEYWORDS: Lipoma, prolapse, rectal, transanal
INTRODUCTION
Lipomas of the gastrointestinal tract are a rare condition that can be found all along the tract. Colonic lipomas are in the second position of frequency after adenomatous polyps.[1,2] Their incidence in literature is reported between 0.2% and 4.4%.[1,3] They are most common in adults between 50 and 69 years of age and they have a female predominance.[1,2,3,4] Their origin is, in the majority of the cases, from the submucosal layer and less frequently from the subserosal or the intermucosal layer.[1,2,4,5] Their allocation is greater from the rectum to the right colon.[1,3,4,5] Rectal lipomas account for approximately 3.4% of all colonic lipomas.[1,7,10] Only four cases in children have been described in the literature. Their structure is usually a soft polypoid mass with an overlying mucosa, either normal or with signs of inflammation, ulceration, or erosion.[1,3,4,5] These masses are mostly asymptomatic, but if they grow bigger than 2 cm in diameter symptoms may occur, such as rectal bleeding, intussusception, obstruction, or anal prolapse.[5,6,9]
CASE REPORT
A 4-year-old boy presented due to anal prolapse after bowel emptying. During prolapse, a round-shaped mass was also observed, about 4 cm in diameter. The mass was automatically retracted back to the rectum when lying down. During the last months, the patient had bowel disorders and skin lesions around the anus such as dermatitis. Magnetic resonance imaging was performed that revealed a mass in the pelvis, originating from the wall of the rectum, which shortened the anal canal. The imaging characteristics were not specific and the differential diagnosis included polyps, lymphoma, and mesenchymal tumors. Features of malignancy were not recognized.
When diagnostic tests were completed, the patient was transferred to the operating theater. The approach of external local excision was decided preoperatively since the location of the mass permitted easy manipulation through the anus. After the induction of anesthesia, a catheter was inserted into the rectum for administrating enemas to push the mass outside the anal canal. With the assistance of rectal examination, the mass was successfully extracted and grabbed with gauze. Macroscopically, the tumor was round with a smooth surface that had scattered erosions. The base of the tumor was dissected using an ultrasound scissor and after ligating the blood supplying vessels, it was excised in normal borders. The mucosa and submucosa were closed with interrupted absorbable sutures and a catheter dressed with Vaseline gauze was inserted as a splint. The patient started oral nutrition on the 3rd postoperative day and the catheter was removed. Rectal examination revealed a normal intestinal lumen without bleeding or remaining mass. He was discharged on the 5th postoperative day, after having normal stools and adequate oral nutrition, with instructions for reexamination after 1 month. Pathology examination revealed a rectal lipoma excised in normal borders [Figures 1-4].
Figure 1.

Rectal tumor in MRI (coronary). MRI: Magnetic resonance imaging
Figure 4.

Excision using an ultrasound scissor
Figure 2.
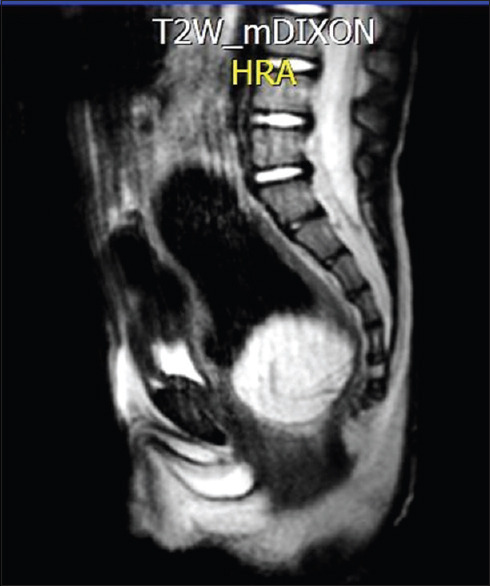
Rectal tumor in MRI (sagittal). MRI: Magnetic resonance imaging
Figure 3.

Prolapse of the tumor with maneuvers
DISCUSSION
Lipomas of the colon are rare, asymptomatic submucosal lesions that vary in size,[1,3,4] most frequently located in the right colon[1,3,5] They are more common in adults and in women.[2,3,4] In children, they are the second-most common benign tumor of the colon after adenomatous polyps.[1,2] Malignant transformation to liposarcoma is rare but some cases have been reported.[8,11,12] Diagnosis is usually based on histopathology.[4] In most cases, indications for excision are symptoms such as abdominal pain, rectal bleeding, change in bowel pattern, intestinal obstruction, intussusception, and perforation.[1,4,5] Spontaneous prolapse of lipomas per rectum has been reported in a few cases.[3,4,5] In such cases, excision could be performed through transanal approach.[3,4] If this approach is not feasible, laparotomy or minimally invasive laparoscopic techniques can be considered, although with a controversial complication risk.[3,4,5] Endoscopic resection is considered a safe approach if the lipoma has a diameter <2 cm and the pedicle is narrow.[5,6] In bigger lipomas, the endoscopic approach is feasible, but the risk of bleeding and perforation is reported high in the literature.[1,3,4] Surgical repair, both open and laparoscopic, is suggested in the literature when: the lipoma is sessile or has a diameter of more than 4 cm, there is a risk of malignancy, symptoms occur, and muscular layer or serosal attachment is present.[3,4] In our case, the opportunity to eject the tumor with maneuvers allowed a minimally invasive transanal ablation, without leaving any residue and without any risk of rectal rupture. In cases where the tumor cannot easily be ejected through the anus and cannot be removed through endoscopic procedures, a laparotomy or a laparoscopy should be performed, keeping in mind all the possible postoperative complications.[4,5]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lapsia S, Khlevner J, Morganstern J, Chawla A. Rectal lipoma in a pediatric patient with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2013;56:e36–7. doi: 10.1097/MPG.0b013e318254c9fe. [DOI] [PubMed] [Google Scholar]
- 2.Zuber M, Harder F. Switzerland: Department of Surgery, University of Basel; 2001. Benign Tumors of the Colon and Rectum. [Google Scholar]
- 3.Tascilar O, Cakmak GK, Gün BD, Uçan BH, Balbaloglu H, Cesur A, et al. Clinical evaluation of submucosal colonic lipomas: Decision making. World J Gastroenterol. 2006;12:5075–7. doi: 10.3748/wjg.v12.i31.5075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kose E, Cipe G, Demirgan S, Oguz S. Giant colonic lipoma with prolapse through the rectum treated by external local excision: A case report. Oncol Lett. 2014;8:1377–9. doi: 10.3892/ol.2014.2317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kouritas VK, Baloyiannis I, Koukoulis G, Mamaloudis I, Zacharoulis D, Efthimiou M. Spontaneous expulsion from rectum: A rare presentation of intestinal lipomas. World J Emerg Surg. 2011;6:19. doi: 10.1186/1749-7922-6-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bentama K, Chourak M, Chemlal I, Benabbou M, Raiss M, Hrora A, et al. Intestinal subocclusion due to colonic lipoma: A case report. Pan Afr Med J. 2011;10:22. doi: 10.4314/pamj.v10i0.72232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shobeirian F, Mehrnahad M, Soleimantabar H. Rectal lipoma as a lead point for colo-colonic intussusception. Radiol Case Rep. 2018;13:431–3. doi: 10.1016/j.radcr.2018.01.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tiwari C, Zadpe A, Rathi P, Shah H. An unusual presentation of rectal carcinoma in a child. Pediatr Gastroenterol Hepatol Nutr. 2018;21:72–5. doi: 10.5223/pghn.2018.21.1.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Paškauskas S, Latkauskas T, Valeikaitė G, Paršeliūnas A, Svagždys S, Saladžinskas Z, et al. Colonic intussusception caused by colonic lipoma: A case report. Medicina (Kaunas) 2010;46:477–81. [PubMed] [Google Scholar]
- 10.Arora R, Kumar A, Bansal V. Giant rectal lipoma. Abdom Imaging. 2011;36:545–7. doi: 10.1007/s00261-010-9668-7. [DOI] [PubMed] [Google Scholar]
- 11.Chen CY, Wu CC, Hsiao CW, Chen CW, Jin JS, Jao SW. Primary non-Hodgkin's lymphoma of rectum presenting with rectal prolapse. J Pediatr Surg. 2009;44:e1–3. doi: 10.1016/j.jpedsurg.2009.01.014. [DOI] [PubMed] [Google Scholar]
- 12.Yang R, Cheung MC, Zhuge Y, Armstrong C, Koniaris LG, Sola JE. Primary solid tumors of the colon and rectum in the pediatric patient: A review of 270 cases. J Surg Res. 2010;161:209–16. doi: 10.1016/j.jss.2008.12.003. [DOI] [PubMed] [Google Scholar]