

Abstract
Background:
Social communication interventions benefit children with ASD in early childhood. However, the mechanisms behind such interventions have not been rigorously explored. This study examines the mechanism underlying a naturalistic developmental behavioral intervention, JASPER (Joint Attention, Symbolic Play, Engagement, and Regulation), delivered by educators in the community. Specifically, the analyses focus on the mediating effect of joint engagement on children’s initiations of joint attention (IJA) skills and whether IJA postintervention are associated with later gains in children’s receptive and expressive language.
Methods:
One hundred seventy-nine children, age 2–5 years, were randomized to immediate JASPER treatment or waitlist (treatment as usual) control. Independent assessors blinded to time and treatment coded children’s time jointly engaged and IJA during a 10-min teacher–child interaction at baseline, exit, and follow-up. Age-equivalent receptive and expressive language scores from the Mullen Scales of Early Learning were collected at baseline and follow-up. Mediation analyses with linear mixed models were used to explore the potential mediating effect of joint engagement on IJA.
Results:
Joint engagement significantly mediated 69% of the intervention effect on young children’s IJA and IJA predicted improvements in standardized language scores.
Conclusions:
Small but sustained changes in child-initiated joint engagement improved IJA, a core challenge in children with ASD, which in turn led to improvements in language.
Keywords: Autism, early intervention, mediation, social communication, JASPER
Introduction
Notable gains have been made in effective early interventions for children with ASD, whether implemented by therapists, teachers, or parents (Smith & Iadarola, 2015). The increasing number of randomized controlled trials (RCTs) has yielded important information on the efficacy of different early intervention models (whether they lead to gains for children) as well as for whom the intervention works (moderators of treatment outcome) (Smith & Iadarola, 2015). Some data also suggest there are important predictors of early intervention outcome (Bottema-Beutel, Kim, Crowley, & Yoder, 2020). However, we have less information on the mechanism(s) or why the intervention works.
One important outcome of early intervention is improvement in social communication skills, a core challenge for young children, and a defining characteristic necessary for a diagnosis of autism. Social communication skills are defined especially by delayed or absent joint attention skills (Mundy, Sigman, Ungerer, & Sherman, 1986). Children’s ability to initiate joint attention (using gestures of point, show, and give to share; IJA) has been shown to improve downstream language abilities in children with autism (e.g., Mundy, Sigman, & Kasari, 1990) and predicts greater gains in language when improved in intervention (Kasari, Paparella, Freeman, & Jahromi, 2008). While these studies demonstrate the importance of IJA to later language development, we do not clearly understand why.
We have some evidence from studies of typically developing children that increasing joint engagement between parent and child facilitates children’s gesture and language learning (Tomasello & Farrar, 1986). Presumably when parent and child are jointly engaged around a topic (such as playing with toys), they have opportunities to communicate both verbally and nonverbally. Joint engagement is different from joint attention. Joint attention refers to the prelinguistic gestures children use to communicate before they learn to speak, such as pointing to something of interest. Joint engagement, on the other hand, refers to periods when adults and children actively focus on shared objects/events (JE; Adamson, Bakeman, & Deckner, 2004). Typically developing children spend more time in supported JE with their parents between the ages of 18 and 36 months, a time of increasing language learning (Adamson, Bakeman, Deckner, & Nelson, 2012). Supported JE refers to when children focus on shared objects and events with their parent but do not overtly direct the parent. They may provide only subtle signs of communication such as imitating a word or following actions of the other (Adamson et al., 2012; Adamson, Bakeman, Deckner, & Romski, 2009), but nevertheless are jointly engaged with the parent through signs of turn-taking, playing together in an activity and awareness of the social partner (Kasari, Freeman, & Paparella, 2006).
Periods of supported JE are distinguished from object engagement, where the child is focused on objects to the exclusion of the social partner. Object engagement is common among children with autism (Adamson et al., 2009). Here the child may be engaged with a toy, actively excluding the social partner to have total focus on the toy alone. Or the parent may follow in to focus on the same activity as the child, but the child is unaware of the parent. A goal of early intervention is to help the child become more aware of the social partner and to enter into states of joint engagement (supported and coordinated).
One recent study confirmed that IJA skills, JE during parent–toddler interaction, and expressive language skills were more impaired in toddlers with ASD than toddlers with developmental delays or typical development at the same chronological age (Adamson, Bakeman, Suma, & Robins, 2019). While IJA and language skills have long been noted to be more impaired in children with autism than children with developmental delays matched on age and developmental abilities (Mundy et al., 1986), these findings highlight the additional impairment in JE and the importance of JE to later expressive language (Adamson et al., 2019).
For children with ASD, one early intervention model has consistently reported data on IJA, JE, and language skills in children with ASD as the result of the intervention. Across multiple randomized trials of the Joint Attention, Symbolic Play, Engagement, and Regulation (JASPER) intervention, JE has improved as a result of the intervention (Kaale, Smith, & Sponheim, 2012; Kasari et al., 2006, 2014; Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015). In JASPER, adults employ strategies to support children’s ability to initiate and maintain a joint engaged state. On average, children with autism enter intervention able to maintain JE for about 20% of an interaction with an adult (Chang, Shih, & Kasari, 2016a; Chang, Shire, Shih, Gelfand, & Kasari, 2016b; Kasari et al., 2006, 2014, 2015; Kasari, Gulsrud, Wong, Kwon, & Locke, 2010; Shire et al., 2016). Over the course of intervention, this can, on average double, with some children able to engage for most of an interaction (Kasari et al., 2015). Theoretically, IJA skills increase in the context of JE since longer periods of interaction allow the child to learn and demonstrate more communication skills. We have hypothesized that JE is a mechanism for the increase in IJA skills in previous randomized trials of JASPER, but this hypothesized mediational model has not been tested.
Similar to other areas of psychosocial interventions, studies of mediation are rare in ASD intervention science. As noted in one review of youth psychotherapy interventions, only 6% of the 67 included studies included formal mediation analyses (Weersing & Weisz, 2002). In ASD, treatment mechanism has been suggested in the literature (Maric, Prins, & Ollendick, 2015; Nelson, McDonnell, Johnston, Crompton, & Nelson, 2007), yet only two studies to date have rigorously tested the mechanisms underlying behavioral treatment outcomes in ASD (Gulsrud, Hellemann, Shire, & Kasari, 2016; Pickles et al., 2015). Both of these studies focused on caregiver-mediated, clinic-based intervention models. Gulsrud et al. (2016) tested the active ingredients (i.e., mirror pacing) of the parent-mediated JASPER intervention specifically for changes in joint engagement for toddlers with ASD. In another caregiver-mediated model (Pickles et al., 2015), parent synchronization, a major teaching element of the PACT trial, mediated core ASD symptom improvements as measured by the severity score from the Autism Diagnostic Observation Schedule (ADOS)-Generic in preschool children. Green and Garg (2018) noted that there are likely similarities between the caregiver strategies of synchronization and mirrored pacing. This suggests that there is some common mechanism for improving parent–child interaction outcomes that lead to gains in children’s social communication skills. However, educators have additional considerations when applying JASPER in their classroom environment filled with children with diverse strengths and needs. Further, educators are trained in basic interaction principles (DEC Recommended Practices Commission, 2014) and are expected to establish JASPER intervention fidelity as measured with the same standard applied to university clinicians. There has yet to be examination of treatment mechanism in educator-mediated JASPER.
The current study
Consistent with developmental theory, we hypothesized that increasing time jointly engaged is a potential underlying mechanism to improve children’s social communication skills (i.e., IJA skills). If JE does mediate the effect of treatment, then subsequently, we seek to investigate whether the smallest amount of change in JE found in prior JASPER RCTs (20% change) will lead to gains in children’s IJA skills among those who receive intervention.
This study combines data from two published independent RCTs of approximately 11-week educator-mediated JASPER intervention compared to community treatment as usual-TAU (Study 1: Chang, Shih, et al., 2016; Chang, Shire, et al., 2016 and Study 2: Shire et al., 2016). TAU consisted of regular classroom programming based on the Verbal Behavior model (Sundberg, 2008). The decision to combine the data from these studies was made due to their structural similarities (e.g., intervention type, dose, design, context, delivered by educators). This allows for examination of the mechanism of JASPER intervention delivered to young children with ASD by publicly funded educators in preschools (Study 1) and center-based early intervention classrooms (Study 2). Using the combined data of 179 children with ASD, the analyses first examine whether JE mediates the effect of community educator-mediated JASPER intervention on children’s IJA and second, whether IJA at intervention exit is associated with gains in children’s standardized receptive and expressive language scores at follow-up.
Methods
Participants: Children
Across the two studies, children were included if they had a school eligibility of autism or outside independent ASD diagnosis. In Study 1, diagnosis was confirmed by the research team using the ADOS-2 (Lord et al., 2012). In Study 2, state EI assessors provided the diagnosis. Five children entered the study with diagnoses other than autism, including cerebral atrophy, language delays, and global developmental delays. These five children qualified for the same state funded service offered by the community site. Their data were included in the original study analyses; therefore, they were included in the current study.
A total of 179 (Study 1: n = 66, Study 2: n = 113) children age two to five years (M = 38 months; SD = 9.35) were included in this study. Children were approximately 80% male and from diverse ethnic backgrounds: 49% Hispanic, 19% African American, 15% White, 10% Mixed race, and 7% Asian. Children’s age-equivalent receptive language (M = 21.79 months, SD = 13.70) and expressive language (M = 22.33 months, SD = 12.39) skills at baseline were measured using the Mullen Scales of Early Learning (Mullen, 1995). Ninety-eight children were considered preverbal, demonstrating ≤ 5 spontaneous requests or comments during a baseline 10-min teacher–child interaction. At baseline, children spent minimal time in child-initiated JE (average 10%) and displayed an average of 6.68 IJA skills. See Table 1.
Table 1.
Child characteristics at baseline–mean (SD)
| Child characteristics: mean (SD) | TAU (n = 85) | JASPER (n = 94) | p-Value |
|---|---|---|---|
|
| |||
| Age in months (range: 26–62) | 37.69 (9.77) | 38.16 (9.01) | 0.59 |
| Male: n (%) | 69 (81%) | 74 (79%) | 0.82 |
| Race/Ethnicity: n (%) | 0.03 | ||
| African American | 22 (26%) | 12 (12%) | |
| Asian | 3 (4%) | 10 (11%) | |
| White | 8 (10%) | 18 (19%) | |
| Hispanic | 44 (52%) | 43 (46%) | |
| Other/Mixed | 7 (8%) | 11 (12%) | |
| Language at baseline (Age equivalency: months) | |||
| Receptive (range: 1–62) | 21.24 (14.16) | 22.3 (13.32) | 0.49 |
| Expressive (range: 2–60) | 21.32 (12.42) | 23.26 (12.36) | 0.29 |
| Language Mental Age (range: 1.5–57.5) | 21.28 (12.91) | 22.78 (12.42) | 0.35 |
| Proportion of time in joint engagement (range: 0–1) | 0.08 (0.17) | 0.12 (0.2) | 0.05 |
| Initiating joint attention (range: 0–49) | 5.03 (8.52) | 8.32 (10.37) | 0.05 |
| Frequency of social communication ≤ 5: n (%) | 52 (76%) | 46 (68%) | 0.34 |
Participants: Educators
There were 72 educators, including teachers (n = 6) and teaching assistants (n = 66) across the two studies and treatment groups (JASPER: n = 41 and TAU: n = 31). Study 1 included six classrooms (three JASPER and three TAU) with educators from diverse ethnic backgrounds (38% Hispanic, 23% African American, 23% White, 8% Asian, and 8% Other). All educators had at least some college, with 67% reporting graduate degrees. Educators had been in their current positions for 4.09 years on average (SD = 3.3 years). Study 2 included four classrooms (2 JASPER and 2 TAU) across two sites. Within each classroom, four sequential two-hour long sessions were conducted each day where a total of 45 educators (69% Hispanic, 27% African American, 2% Asian, and 2% White; 91% females) were trained in JASPER. Educators held their current positions for an average of 2.56 years (SD = 2.28 years).
Ethical considerations
Informed consent was given by all participants (children and educators), and no serious adverse events were reported.
Intervention and training supports.
In Study 1, the educators in the JASPER classrooms received 60, 15-min in-person coaching sessions throughout the 11 weeks of intervention. In Study 2, remote support (weekly phone calls and written feedback) and two weeks of in-person training were provided by the research team, as well as on-site supervision from a staff member trained in JASPER. Educators in both studies delivered JASPER with high fidelity by exit (Study 1: 75%; Study 2: 80.9%). In both studies, educators in the TAU classrooms continued to implement their regular curriculum until the experimental classrooms completed the follow-up period. The TAU classrooms then received training and started JASPER. For all TAU classrooms, the regular classroom programming was based on the Verbal Behavior model (Sundberg, 2008). Study 1 TAU classrooms engaged in free play during the daily JASPER rotations. In Study 2, TAU classrooms engaged in music and movement. Full details of the intervention (i.e., JASPER protocol, study design, coding, and measures) have been published (Chang, Shih, et al., 2016; Chang, Shire, et al., 2016; Shire et al., 2016).
Child measures
All measurements were collected by assessors who were blinded to the children’s treatment assignment.
Language – Mullen Scales of Early Learning (MSEL; Mullen, 1995).
The MSEL was used to measure children’s expressive and receptive language abilities (age equivalency) at baseline and follow-up for Study 1 and baseline only for Study 2. Assessors in Study 1 included research assistants and graduate students, while assessors in Study 2 included graduated students in psychology under the supervision of the site school psychologist.
Teacher–Child Interactions (TCX: Chang, Shih, et al., 2016; Chang, Shire, et al., 2016).
The 10-min TCX videos were recorded at major time points (baseline, exit, and follow-up) in study 1 by a research assistant and in study 2 by a school staff member. A random 10-min segment was recorded to capture the children in JASPER with the educators. Coders were trained using practice videos until reliability was established (i.e., at 80%). Three independent raters (graduate students and research assistants) blinded to treatment condition, site, and time scored engagement states and three additional raters independently scored IJA skills.
Joint engagement.
The TCX videos were coded in 10 one-minute intervals at major time points. Each interval was assigned one mutually exclusive engagement state that represented the child’s engagement for the majority of the interval (31 + seconds), including unengaged (e.g., wanders, looks around), person engaged (e.g., attends to a person only-song or social game with no object), object engaged (e.g., focuses exclusively on an object without noticing person), or jointly engaged (e.g., coordinates the person and the shared activity). The interval was also coded as either adult-directed (e.g., educator redirects the child’s attention to their choice of activity or verbally/physically prompts participation) or child-initiated (e.g., child selects toys, initiates an action/comment, and the educator follows). Total time in child-initiated JE was calculated by summing the intervals coded as both jointly engaged and child-initiated. Kappa scores for engagement states ranged from 0.76 to 1.0. Kappa scores for the child-initiated or adult-directed ranged from 0.84 to 0.88. The intraclass coefficient (ICC) for child-initiated JE was 0.95.
Social communication – initiations of joint attention (IJA).
Independent raters coded the TCX at major time points for the frequency of spontaneous IJA (verbal and nonverbal), including eye contact (coordinated joint looks-child looks to the toy, to the adult to share, and back to the toy), gestures (point, show, and give to share), and language (comments). Prompted or elicited behaviors (e.g., time delay, responses to a question) were not considered spontaneous initiations. Further, initiations to communicate for another function (e.g., to request) were not counted within IJA. The range of ICCs for IJA was 0.87–0.99 across the two studies.
Statistical analysis
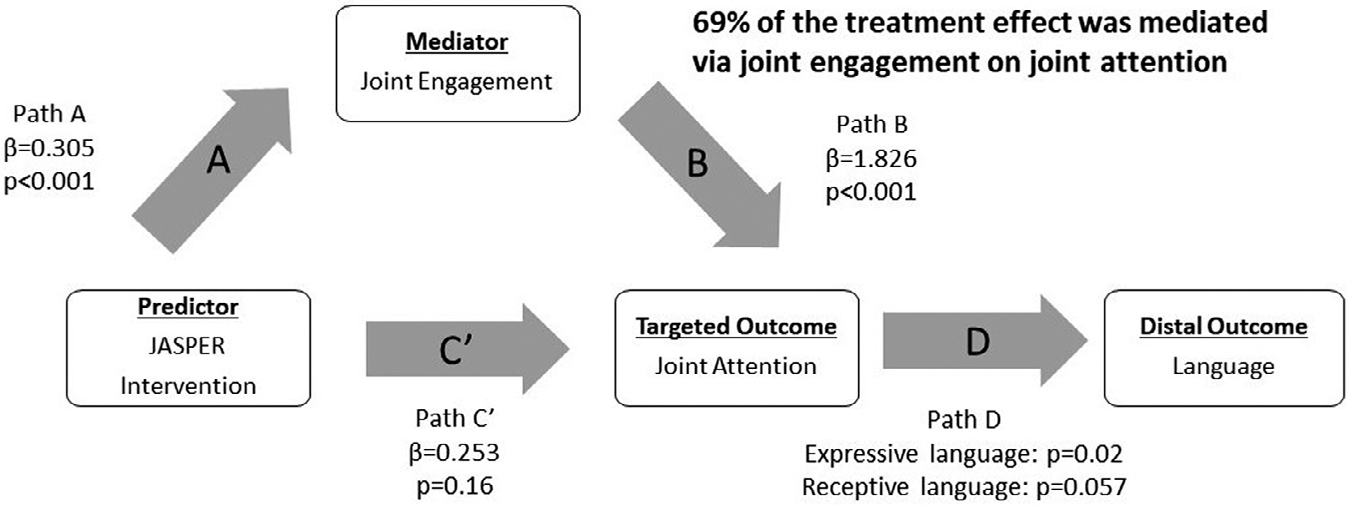
Mediation analyses with linear mixed models were used to explore the potential mediating effect of JE on IJA while controlling for study and child language age (average of MSEL receptive and expressive language age-equivalent scores). Linear mixed models were used to model the difference in treatment trajectories in JE and IJA from baseline to exit. The proposed mediation mechanism is depicted in Figure 1, where path A, B, and C’ are adapted from The Four Steps (Baron & Kenny, 1986). The predictor/causal factor is the JASPER intervention, the mediator is JE, and the target outcome is IJA. Path A denotes the association between the predictor/causal factor with the mediator (i.e., treatment difference in JE), path B denotes the association between the mediator and the target outcome (i.e., JE and IJA across time), and path C’ denotes the direct effect between the predictor/causal factor with the target outcome after adjusting for the mediator (i.e., effect of intervention on IJA after adjusting for JE). Path C (not shown) is the total effect of treatment on the target outcome, which is the sum of the direct effect (Path C’) and the indirect effect (Path A*Path B). Last, Path D is the relationship between IJA and language outcomes.
Figure 1.

Proposed mechanism in social communication interventions
The mediation model was adapted from Pickles et al.’s (2015) repeated measures mediation model while controlling for potential baseline confounding variables such as children’s baseline language age and study. Study differences were also included as a fixed effect when data were pooled from two studies as suggested by Curran and Hussong (2009) to control for differences by study. The measures collected in both studies were developmental measures and were anticipated to increase with age.
As noted in Pickles et al. (2015), a naïve mediation model typically assumes no unobserved confounds between the mediator and the outcome and no measurement error in the mediator. However, such assumptions can lead to biased estimates. Hence, the repeated measures of both the mediator and the target outcome were assessed at two points (a) before randomization and (b) treatment exit to take into account both measurement error and potential confounds via linear mixed models.
Within Study 2, there were five children with diagnoses other than ASD. A sensitivity analysis was performed to compare the mediation estimates with and without these five children. All final inferences were the same as the parameter estimates were extremely similar. Hence, the final results included all children.
In a secondary post hoc analysis, logistic regression was used to explore whether the children receiving JASPER who gained at least 20% time in JE from baseline to exit, made any significant gains in IJA (binary outcome: change in JA = 0 versus change in JA > 0). This value of 20% cutoff was a data-driven decision based on published JASPER studies (Kasari et al., 2006, 2010, 2014, 2015) where there were significant treatment effects for JE. Based on five JASPER studies, the average improvement in JE ranged from 20 to 40% (2–4 min) from baseline. Hence, the study sought to evaluate whether the smallest amount of gain in JE (20%) was associated with any gains in IJA. The association between IJA at treatment exit with receptive and expressive language at follow-up was examined using linear regression models in a subgroup analysis (Path D) while adjusting for treatment differences.
Unlike linear mixed models that automatically handle missing data by producing unbiased estimates as long as observations are missing at random, linear and logistic regression models perform case-wise deletion in the presence of missing values (max 27% missing data in current study). Multiple imputations (MI) were used to replace missing values (Little & Rubin, 1989; White, Royston, & Wood, 2011) in the secondary analyses. MI is a simulation-based method to handle missing data by estimating plausible values to replace the current missing data. The algorithm was implemented using the Multiple Imputation by Chain Equations package (Groothuis-Oudshoorn & van-Buuren, 2011) for R CRAN version 3.3.2 (R Core Team, 2016) to generate 30 imputed data sets with 100 iterations. Pooled estimated coefficients and standard errors did not differ much by number of imputations applied (20 or 100 imputations) indicating that the number of imputations performed was acceptable.
Results
Mediation: Time jointly engaged to IJA
There was a significant treatment difference from baseline to exit in both JE (Path A: β= .305, p < .001, Figure 2A) and IJA (β = .80, p < .001, Figure 2B) where children receiving JASPER made significantly more improvement than children in TAU. After adjusting for JE, the treatment effect diminished to nonsignificance (Path C’: β = .253, p = .16) while JE remained significantly associated with IJA (Path B: β = 1.826, p < .001). As suggested by Baron and Kenny (1986), the total path (Path C) should be inferred from the sum of the direct (Path C’, Figure 3) and the indirect path (Path A × Path B) when using mixed models to estimate the mediation effect. Consequently, the total effect indicated by Path C is equivalent to 0.81 (Path A × Path B + Path C’). This implies that approximately 69% [(Path A × Path B)/Path C] of the treatment effect on IJA was mediated by time in JE. The remaining 31% of the treatment effect remains identified as a direct effect of treatment on IJA.
Figure 2.

Children receiving JASPER intervention improved significantly more in (A) child-initiated JE and (B) IJA from baseline to exit compared to children in TAU waitlist
Figure 3.
Joint engagement as a mechanism in social communication intervention
We do not expect an exclusive focus on objects (i.e., object engagement) to increase in an intervention designed to increase social engagement. There was no intervention effect on object engagement (F (1,128) = 2.88, p = .09, Path A) and, consequently, did not support object engagement as a potential mediator.
IJA as a predictor of language
Language at follow-up was collected in study 1. IJA at intervention exit was significantly and positively associated with expressive language (β = 0.175, t (47.23) = 2.44, 95% CI (0.03, 0.32), p = .02) and modestly associated with receptive language (β = .170, t(51.08) = 1.94, 95% CI (−0.006, 0.35), p = .057) at the one-month follow-up (Path D).
Minimum degree of improvement in joint engagement
Given that JE mediates the effect of JASPER on children’s IJA skills, we can anticipate that children will have more opportunities to learn discrete JA skills while socially connected. During JE, children are more likely to share with a partner or notice the adult’s JA models. Hence, we wished to explore the smallest amount of improvement in time in JE that children receiving JASPER needed to make to see growth in IJA. We made a data-driven decision to evaluate whether the smallest anticipated gain of 20% (or 2 min) in a 10-min observation will lead to any gains in IJA. Consistent with our hypothesis, we found that a gain of at least 20% out of 10 min was significantly associated with increased odds of having gains in IJA from baseline to exit (β= 1.45, t(50.82) = 2.44, 95% CI (0.26, 2.64), p = .017).
Discussion
Social engagement with an adult provides young children with a plethora of learning opportunities throughout their day. This natural path to development is also present for young children with ASD, albeit often significantly diminished by time exclusively focused on objects or unengaged where children accumulate missed learning opportunities. A primary goal of the JASPER intervention is to increase the amount of time children spend in JE with a social partner. Although time in JE is hypothesized to lay the groundwork for gains in IJA and language (Adamson et al., 2019), JE has not previously been examined as a mechanism of change in early intervention. Findings from the current study demonstrate that time in JE mediated 69% of the effect of JASPER treatment on children’s IJA, indicating that JASPER intervention is effective in improving IJA via the theoretically expected pathway of increasing children’s JE. This partial mediation (Kenny, Kashy, & Bolger, 1998) indicates that 31% of the treatment effect on IJA remains unexplained.
Other engagement states, such as exclusive attention to objects (object engagement), have been explored in the intervention literature (Mcduffie, Lieberman, & Yoder, 2012). In JASPER, our goal is to decrease time where children are solely object engaged and to increase the time the child coordinates social communication between objects and the social partner. While object engagement decreased in the intervention, there was no significant treatment difference and was, thus, not a potential mediator on social communication. Therefore, this study builds upon extant data demonstrating a unique link between JE and the development of language (e.g., Adamson et al., 2009) and extends the literature to highlight the mechanistic role of JE in social communication intervention.
The mediation model applied has several strengths. First, the model establishes a clear temporal sequence for the pathway to the target outcome. As Pickles et al. (2015) suggested, a critical concern is the potential for reverse causation when the mediator and outcomes are measured at the same time points. However, in this study, we have a strong base of developmental theory and prior experimental data to establish the upstream (i.e., mediator – JE) and downstream effect (i.e., social communication) where the context of JE between the child and the social partner creates social communication learning opportunities. A second strength of the current study is the use of randomization that allows for causal interpretation of Path A. Randomization ensures that the mediator (i.e., time in JE) is not correlated with potential confounders (e.g., children’s mental age as measured by Mullen).
Children with ASD, including those in this study, initiate JE at a fraction of the frequency and duration of their typically developing peers. At baseline, children spent less than a tenth of their interactions with educators jointly engaged. Thus, even small increases in JE could create meaningful learning opportunities to improve core social communication skills. The study findings demonstrate that a 20% gain in JE was associated with increased odds of gaining in IJA. We see a parallel impact of this amount of JE in the study of peer interactions for children with autism. For example, we have found that school-age children who demonstrated this same increase of 20% JE with peers on the playground (or 2 min within a 10-min interaction) by mid-treatment (one month), continued gaining in JE to treatment exit. In contrast, children who did not meet this midpoint benchmark remained primarily unengaged (Shih, Patterson, & Kasari, 2016). This same amount of change in JE has also been associated with having friends and developing more meaningful friendships for preschool children with ASD (Chang, Shih, et al., 2016; Chang, Shire, et al., 2016; Howes, 1983). Hence, this 20% (2-min) increase in JE over a 10-min interaction is not only statistically significant but clinically valuable. This preliminary exploration of a benchmark for change in JE, leading to gains in social communication may be further explored as a measure of response to intervention. Such data may have utility as a tailoring variable to indicate an adaptation or augmentation to a child’s intervention program.
While these data provide important information on the mechanism of an early intervention, there are also limitations. First, data on language at the follow-up were collected in only one of the studies due to staffing limitations in a real-world community setting. Second, the interval coding scheme adopted for the current study may be subjected to measurement error (i.e., misclassification of the engagement states). However, we tried to minimize measurement error by using known reliability indices such as ICC (child-initiated JE ICC = 0.95) and repeated measures over time in the current study. Third, different play assessments were conducted in each study; therefore, play data could not be collapsed to examine play as another potential mediator of treatment. Within JASPER, interventionists also focus on developing children’s play diversity, flexibility, and level (complexity). Over time, our goal is to increase children’s spontaneous initiations of new play acts and play acts at higher levels through the development of social play routines with an adult. Embedded within these routines are opportunities for children to initiate both nonverbal and spoken communication. By engaging children through play, the interaction helps children build skills such as turn-taking and conversation. Therefore, considering the central role of increasing diversity, flexibility, and complexity in the context of play, it is possible that play skills may serve as a mediator in this intervention and could be the focus of additional research.
Conclusion
Findings from this study demonstrate that increasing children’s ability to initiate periods of JE may be the underlying mechanism to improve IJA, a core developmental challenge for children with ASD. Even small but sustained changes in child-initiated JE can enhance core challenges in IJA. Improved IJA then, in turn, influence children’s language skills. Findings of meaningful treatment mediators could be used in turn to target more effective future interventions.
Key points.
Understanding the mechanism of the intervention can help researchers maximize programs that are critical for improving children’s communication.
There is a significant JASPER intervention effect on children’s initiated joint engagement and joint attention.
Joint engagement mediates 69% of the effect of JASPER intervention on children’s social communication skills and leads to gains in children’s spoken language.
Acknowledgements
This study was funded by Autism Speaks Grant #7495 (PI: Kasari) and FAR Fund (to NYCIT). The authors also acknowledge the support of NIH grant (R01 HD098248; PI, Kasari). They would like to thank the children and families who participated in the study, the educators, Los Angeles Unified School District, and New York Center for Infants and Toddlers. The authors have declared that they have no competing or potential conflicts of interest.
Footnotes
Conflict of interest statement: No conflicts declared.
References
- Adamson LB, Bakeman R, & Deckner DF (2004). The development of symbol-infused joint engagement. Child Development, 75, 1171–1187. [DOI] [PubMed] [Google Scholar]
- Adamson LB, Bakeman R, Deckner DF, & Nelson PB (2012). Rating parent–child interactions: Joint engagement, communication dynamics, and shared topics in autism, Down syndrome, and typical development. Journal of Autism and Developmental Disorders, 42, 2622–2635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adamson LB, Bakeman R, Deckner DF, & Romski M (2009). Joint engagement and the emergence of language in children with autism and Down syndrome. Journal of Autism and Developmental Disorders, 39, 84–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adamson LB, Bakeman R, Suma K, & Robins DL (2019). An expanded view of joint attention: Skill, engagement, and language in typical development and autism. Child Development, 90, e1–e18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron RM, & Kenny DA (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182. [DOI] [PubMed] [Google Scholar]
- Bottema-Beutel K, Kim SY, Crowley S, & Yoder PJ (2020). Developmental associations between joint engagement and autistic children’s vocabulary: A cross-lagged panel analysis. Autism, 25, 566–575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang YC, Shih W, & Kasari C (2016). Friendships in preschool children with autism spectrum disorder: What holds them back, child characteristics or teacher behavior? Autism, 20, 65–74. [DOI] [PubMed] [Google Scholar]
- Chang YC, Shire SY, Shih W, Gelfand C, & Kasari C (2016). Preschool deployment of evidence-based social communication intervention: JASPER in the classroom. Journal of Autism and Developmental Disorders, 46, 2211–2223. [DOI] [PubMed] [Google Scholar]
- Curran PJ, & Hussong AM (2009). Integrative data analysis: The simultaneous analysis of multiple data sets. Psychological Methods, 14, 81–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DEC Recommended Practices Commission. (2014). DEC recommended practices.
- Green J, & Garg S (2018). Annual Research Review: The state of autism intervention science: Progress, target psychological and biological mechanisms and future prospects. Journal of Child Psychology and Psychiatry, 59, 424–443. [DOI] [PubMed] [Google Scholar]
- Groothuis-Oudshoorn K, & Van Buuren S (2011). Mice: Multivariate imputation by chained equations in R. Journal of Statistical Software, 45, 1–67. [Google Scholar]
- Gulsrud AC, Hellemann G, Shire S, & Kasari C (2016). Isolating active ingredients in a parent-mediated social communication intervention for toddlers with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 57, 606–613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howes C. (1983). Patterns of friendship. Child Development, 54, 1041–1053. [Google Scholar]
- Kaale A, Smith L, & Sponheim E (2012). A randomized controlled trial of preschool-based joint attention intervention for children with autism. Journal of Child Psychology and Psychiatry, 53, 97–105. [DOI] [PubMed] [Google Scholar]
- Kasari C, Freeman S, & Paparella T (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47, 611–620. [DOI] [PubMed] [Google Scholar]
- Kasari C, Gulsrud A, Paparella T, Hellemann G, & Berry K (2015). Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. Journal of Consulting and Clinical Psychology, 83, 554–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Gulsrud AC, Wong C, Kwon S, & Locke J (2010). Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40, 1045–1056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Lawton K, Shih W, Barker TV, Landa R, Lord C, … & Senturk D (2014). Caregiver-mediated intervention for low-resourced preschoolers with autism: an RCT. Pediatrics, 134, e72–e79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Paparella T, Freeman S, & Jahromi LB (2008). Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76, 125–137. [DOI] [PubMed] [Google Scholar]
- Kenny DA, Kashy DA, & Bolger N (1998). Data analysis in social psychology (In Gilbert D, Fiske S, & Lindzey G (Eds.). The handbook of social psychology (Vol. 1, pp. 233–265). Boston, MA: McGraw-Hill. [Google Scholar]
- Little RJ, & Rubin DB (1989). The analysis of social science data with missing values. Sociological Methods & Research, 18, 292–326. [Google Scholar]
- Lord C, Rutter M, DiLavore P, Risi S, Gotham K, & Bishop S (2012). Autism Diagnostic Observation Schedule– 2nd edition (ADOS-2). Los Angeles, CA: Western Psychological Corporation. [Google Scholar]
- Maric M, Prins PJ, & Ollendick TH (Eds.) (2015). Moderators and mediators of youth treatment outcomes. New York, NY: Oxford University Press, USA. [Google Scholar]
- Mcduffie AS, Lieberman RG, & Yoder PJ (2012). Object interest in autism spectrum disorder: A treatment comparison. Autism, 16, 398–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mullen EM (1995). Mullen scales of early learning (pp. 58–64). Circle Pines, MN: AGS. [Google Scholar]
- Mundy P, Sigman M, & Kasari C (1990). A longitudinal study of joint attention and language development in autistic children. Journal of Autism and Developmental Disorders, 20, 115–128. [DOI] [PubMed] [Google Scholar]
- Mundy P, Sigman M, Ungerer J, & Sherman T (1986). Nonverbal communication and play correlates of language development in autistic children. Journal of Autism and Developmental Disorders, 17, 349–364. [DOI] [PubMed] [Google Scholar]
- Nelson C, McDonnell AP, Johnston SS, Crompton A, & Nelson AR (2007). Keys to play: A strategy to increase the social interactions of young children with autism and their typically developing peers. Education and Training in Developmental Disabilities, 42, 165–181. [Google Scholar]
- Pickles A, Harris V, Green J, Aldred C, McConachie H, Slonims V, … & Charman T (2015). Treatment mechanism in the MRC preschool autism communication trial: Implications for study design and parent-focussed therapy for children. Journal of Child Psychology and Psychiatry, 56, 162–170. [DOI] [PubMed] [Google Scholar]
- R Core Team (2016). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. Available at: https://www.R-project.org/. [Google Scholar]
- Shih W, Patterson SY, & Kasari C (2016). Developing an adaptive treatment strategy for peer-related social skills for children with autism spectrum disorders. Journal of Clinical Child & Adolescent Psychology, 45, 469–479. [DOI] [PubMed] [Google Scholar]
- Shire SY, Chang YC, Shih W, Bracaglia S, Kodjoe M, & Kasari C (2016). Hybrid implementation model of community-partnered early intervention for toddlers with autism: A randomized trial. Journal of Child Psychology and Psychiatry. 10.1111/jcpp.12672 [DOI] [PubMed] [Google Scholar]
- Smith T, & Iadarola S (2015). Evidence base update for autism spectrum disorder. Journal of Clinical Child & Adolescent Psychology, 44, 897–922. [DOI] [PubMed] [Google Scholar]
- Sundberg ML (2008). VB-MAPP Verbal Behavior Milestones Assessment and Placement Program: A language and social skills assessment program for children with autism or other developmental disabilities: Guide. Concord, CA: AVB Press. [Google Scholar]
- Tomasello M, & Farrar MJ (1986). Joint attention and early language. Child Development, 57, 1454–1463. [PubMed] [Google Scholar]
- Weersing VR, & Weisz JR (2002). Mechanisms of action in youth psychotherapy. Journal of Child Psychology and Psychiatry, 43, 3–29. [DOI] [PubMed] [Google Scholar]
- White IR, Royston P, & Wood AM (2011). Multiple imputation using chained equations: Issues and guidance for practice. Statistics in Medicine, 30, 377–399. [DOI] [PubMed] [Google Scholar]