

Abstract
Aims: We assessed 27-year trends in obesity and blood lipid levels of 10-year-old children to estimate the risk of metabolic syndrome in adulthood.
Methods: Based on a screening program for lifestyle-related diseases in school children in Oita City, Japan, we evaluated secular trends in height, weight, percentage of overweight (POW), total cholesterol (TC), triglyceride (TG), HDL cholesterol (HDL-C), and non-HDL cholesterol (non-HDL-C) of fifth graders (median age: 10.8 years) in Oita City from 1991 to 2017. We focused on the secular trend in the percentage of children with inappropriate serum levels of each lipid. We also evaluated the long-term trends in the 95th, 50th, and 5th percentiles for each parameter, as dependent variables, with the calendar year as an independent variable. Percentages of children with mild obesity (POW-20), moderate obesity (POW-30), and severe obesity (POW-50) were set as dependent variables.
Results: A total of 58,699 boys and 56,864 girls were evaluated during the study period. The percentage of children with severe obesity (POW-50) consistently increased during these years, and the 95th percentile of degree of obesity significantly increased in both boys and girls. The plot of percentages of children with inappropriate levels of TC, TG, and non-HDL-C showed a mild inverted U shape during the study period. The HDL-C level typically decreased in the study period, and the TC, TG, and non-HDL-C levels were markedly higher while the HDL level was lower in obese children than in non-obese children.
Conclusion: The number of children with severe obesity increased, and obese children had higher percentages of inappropriate lipid levels than non-obese children. The rate of dyslipidemia with low HDL levels gradually increased in all children in Oita City, Japan, over the past 27 years.
Keywords: HDL cholesterol, Non-HDL cholesterol, Children, Percentage of overweight
See editorial vol. 29: 1693-1695
Introduction
In developed countries, the prevalence of childhood obesity has substantially increased among all age groups since 1988 1) . Recent studies from the United States demonstrated that obesity in children and adolescents was almost stable or decreased in the early 2000s with social or medical intervention 2 , 3) ; however, a marked increase in the prevalence of severe obesity was reported, particularly among adolescents and non-Hispanic African American children 4 , 5) . A report based on an analysis of 2012–2013 in England also demonstrated a significant increase in severe obesity among children of 2 to 5 years of age 6) , and an upward trend continued with a substantial excess of overweight-obesity among South Asian children and Black girls, even with implications for overweight prevention 7) .
In Japan, lifestyle-related diseases in adulthood were recognized in the early 1990s to be deeply involved in daily eating and exercise habits 8) . Approximately 8% of Japanese are diagnosed with lifestyle-related diseases or metabolic syndrome in adulthood 9) . Obesity in childhood was also recognized in the late 1990s to be associated with susceptibility to metabolic syndrome in adulthood 10) . A longitudinal study based on the data from cross-sectional annual nationwide surveys demonstrated that from 1975 to 2000, the mean (age-adjusted) body mass index (BMI) significantly increased in boys and girls of 6–14 years of age and that the increase in small towns was greater than that in medium-size cities or metropolitan areas (National Nutrition Survey, Japan) 11) . Early prevention of childhood obesity was advocated in 2001, and the diagnostic criteria for pediatric metabolic syndrome were clarified in 2007 by a Ministry of Health, Labor and Welfare research group 12) .
Preventive programs for lifestyle-related diseases have been carried out across many municipalities in Japan. Children at school age who are at risk of future lifestyle-related diseases have been screened and medical intervention has been provided. However, the screening strategy, the criteria for determining children who should receive intervention and intervention methods vary greatly among municipalities in Japan. Oita City, the capital of Oita Prefecture in Kyushu Island, Japan, is a mid-sized city in Japan with a population of >470,000 in 2015. The healthy check-up program for fifth graders (10-year-old children) called “screening for lifestyle-related diseases in elementary school children” has been carried out in Oita City since 1991.
We herein report the long-term trends in the 27-year anthropometric indices and serum lipid data of fifth-grade school children from the Oita City program.
Methods and Population
Participants
The municipal government of Oita City in Oita Prefecture started a screening program for the prediction of lifestyle-related diseases in 1979. Blood biochemistry tests were included in the program from 1991. As of 2020, Oita City administers 60 public elementary schools, which have had relatively stable student numbers over the last decade. The screening program was offered to all fifth graders in public elementary schools in the municipality; approximately 85%–95% were enrolled and gave their informed consent. The mean number of fifth graders each year was 2,174 for boys and 2,106 for girls. The anthropometric and blood data were reviewed each year by a committee of pediatric endocrine/metabolic disease experts, personal counseling was provided for participants as needed, and medical information on lifestyle-related diseases was provided to all citizens of Oita. The cumulative data of the medical examinations of 58,699 boys and 56,864 girls were analyzed.
Method of Examination
The screening program was conducted every year from August to December and anthropometric measurements and blood collection were performed at each school by the assigned pediatricians and nurses. The screening parameters included anthropometric measurements (height, weight, percentage of overweight [POW]) and a blood test. The degree of obesity was calculated from the measured height and weight. In Japan, POW is used in children more commonly than the BMI-for-age percentile and is calculated based on the measured weight and standard weight for height as follows: POW (%)=100×(measured weight - standard weight for height)/standard weight for height. The standard weight is the age- and sex-specific weight for height; the coefficients and formula have been described in detail previously. Children with a POW ≥ 20% and <30% (POW-20) are defined as mildly obese, those with POW ≥ 30% and <50% (POW-30) are defined as moderately obese, and those with POW ≥ 50% (POW-50) are defined as severely obese 13) . Blood collection was performed after at least two hours after breakfast but not in a fasting state in the strict sense. The test parameters included total cholesterol (TC), triglyceride (TG), HDL cholesterol (HDL-C), ALT, a complete blood count of the red blood cells, white blood cells, and platelets with the concentration of hemoglobin, and the hematocrit. Non-HDL cholesterol (non-HDL-C) was calculated as TC minus HDL-C. All blood samples were measured in the laboratory at the Oita Prefectural Adult Disease Screening Center. The anthropometric measurements of height, weight, and POW and blood data of TC, TG, HDL-C, and non-HDL-C from 1991 to 2017 were used in the present study and applied in the statistical analysis.
Trends in the Prevalence of Inappropriate Lipid Levels
Based on the cut-off levels for an elevated TC (≥ 220 mg/dl), TG (≥ 140 mg/dl), and non-HDL-C (≥ 150 mg/dl) and reduced HDL-C (<40 mg/dl), defined according to the Japan Atherosclerosis Society Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017 14) and the 2011 Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents 15) , the secular trends in the prevalence of children with inappropriate lipid levels are summarized as plots every three years. These data were also separately evaluated and shown in obese and non-obese children.
Geographic features of Oita City
The Oita Prefecture is located on the northeast side of the coastal area of Kyushu Island. Oita City is the capital city of Oita Prefecture, which is located in the center, on the coastal side of the prefecture. The population of Oita City was approximately 470,000 in 2015 and accounted for 40% of the prefecture’s population. The population of suburban areas of Oita City has been growing in recent years, accompanied by the development of new towns and shopping centers. Children <15 years of age and elderly individuals >65 years of age account for 13.7% and 27.1% of the population, respectively. The corresponding numbers of the national average in Japan are 12.1% and 27.6%, respectively. Primary, secondary, and tertiary accounted for 1.9%, 22.4%, and 70.5% of industries, respectively. In Japan, the corresponding percentages were 4.0%, 25.0%, and 71.0%, respectively.
Statistical Analyses
The following two methods were used to analyze the secular trends for each parameter: the weighted least-squares method and the quadratic linear weighted least-squares (quadratic) method. The values of Akaike’s information criterion (AIC), R-Squared method (R-Squared), mean absolute error (MAE), and likelihood ratio test were referenced to select the most appropriate method; a smaller AIC value, larger R-Squared value, smaller MAE value, and larger likelihood ratio test value were considered to indicate a more appropriate method. The sample size was also included as an independent variable in each analysis model, and the fluctuation of the sample size was taken into consideration each year.
A regression analysis was performed to evaluate the annual trends in height, weight, POW, TC, TG, HDL-C, and non-HDL-C from 1991 to 2017. In all regression models, the calendar year was the independent variable, and the 95th, 50th, and 5th percentiles of the achievement rate were the dependent variables. For a further analysis of obesity, the percentages of children with mild obesity (POW-20), moderate obesity (POW-30), and severe obesity (POW-50) in each year were set as dependent variables. A generalized linear model was created that also included the sample size as an independent variable to account for the varying sample sizes each year. In the weighted non-linear least-squares model, weights were created by regressing the residuals with the fitted values of the un-weighted non-linear regression. Different sets of weights were calculated for each percentile group.
This study was approved by the Ethics Committee of Oita University School of Medicine (Approval number: 1525).
Results
Population Statistics
Table 1 shows the summary of the anthropometric and biochemical data from 1991 to 2017. The plot of the number of fifth-grade students in Oita City followed a U-shape pattern from 1991 to 2017; the number of students were 6235 in 1991, which declined to approximately 4000 and remained stable from 2001 to 2010 and gradually recovered from 2011 to 2017, reaching 4453 in 2017. The percentage of participants among all fifth graders (estimated median age of 10.8 years old) gradually decreased from >98% to approximately 83%, and the rate of participation among boys and girls was almost the same (94.7% vs. 94.9%). The sex distribution remained almost constant over time, with boys accounting for an average of 50.8% of the study population.
Table 1A. Secular trend in the percentile values of anthropometric measurements and serum lipid data. (Boys: n = 58699).
| Year | Number | Consultation rate (%) | Height (cm) | Weight (kg) | Percentage of overweight (%) | Total Cholesterol (mg/dL) Percentiles | Triglyceride (mg/dL) |
HDL Cholesterol (mg/dL) |
Non-HDL Cholesterol (mg/dL) |
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | |||
| 1991 | 3048 | 97.9 | 131 | 140 | 151 | 27 | 34 | 51 | -19 | -3 | 28 | 133 | 170 | 218 | 32 | 58 | 128 | 47 | 65 | 89 | 69 | 104 | 150 |
| 1992 | 2843 | 98.5 | 131 | 140 | 150 | 26 | 33 | 49 | -18 | -2 | 32 | 135 | 172 | 219 | 32 | 60 | 133 | 46 | 65 | 91 | 73 | 105 | 150 |
| 1993 | 2875 | 91.0 | 130 | 140 | 150 | 26 | 34 | 50 | -16 | -2 | 32 | 136 | 173 | 224 | 30 | 58 | 130 | 47 | 65 | 90 | 74 | 107 | 155 |
| 1994 | 2764 | 90.2 | 131 | 140 | 151 | 26 | 34 | 51 | -18 | -2 | 34 | 135 | 173 | 220 | 33 | 61 | 139 | 46 | 66 | 90 | 73 | 105 | 151 |
| 1995 | 2437 | 88.4 | 131 | 140 | 151 | 27 | 34 | 51 | -17 | -1 | 34 | 136 | 174 | 221 | 32 | 60 | 136 | 47 | 69 | 98 | 70 | 103 | 150 |
| 1996 | 2412 | 98.4 | 130 | 140 | 152 | 26 | 34 | 52 | -19 | -2 | 31 | 140 | 177 | 224 | 32 | 64 | 154 | 46 | 65 | 89 | 78 | 110 | 157 |
| 1997 | 2185 | 97.9 | 130 | 140 | 151 | 26 | 34 | 52 | -19 | -4 | 33 | 137 | 175 | 223 | 32 | 63 | 155 | 47 | 69 | 96 | 71 | 105 | 154 |
| 1998 | 2223 | 98.1 | 131 | 140 | 152 | 27 | 34 | 53 | -20 | -4 | 32 | 138 | 176 | 223 | 33 | 66 | 159 | 45 | 67 | 93 | 74 | 107 | 157 |
| 1999 | 2120 | 97.7 | 131 | 140 | 152 | 26 | 34 | 52 | -20 | -5 | 29 | 138 | 175 | 222 | 32 | 64 | 150 | 47 | 67 | 91 | 74 | 106 | 153 |
| 2000 | 2053 | 98.7 | 131 | 141 | 152 | 26 | 35 | 54 | -20 | -3 | 35 | 140 | 178 | 227 | 34 | 66 | 158 | 46 | 68 | 94 | 76 | 108 | 158 |
| 2001 | 2024 | 96.6 | 130 | 141 | 152 | 26 | 35 | 53 | -18 | -3 | 34 | 138 | 176 | 224 | 33 | 66 | 160 | 45 | 66 | 92 | 76 | 108 | 155 |
| 2002 | 2021 | 98.4 | 130 | 141 | 152 | 26 | 34 | 53 | -21 | -5 | 32 | 138 | 177 | 225 | 31 | 62 | 147 | 46 | 66 | 91 | 76 | 109 | 157 |
| 2003 | 2004 | 98.8 | 130 | 140 | 151 | 26 | 34 | 52 | -20 | -4 | 33 | 140 | 176 | 224 | 33 | 67 | 162 | 45 | 65 | 90 | 77 | 110 | 157 |
| 2004 | 2015 | 98.3 | 130 | 140 | 151 | 26 | 34 | 53 | -19 | -4 | 34 | 137 | 174 | 222 | 33 | 64 | 156 | 44 | 61 | 83 | 80 | 111 | 158 |
| 2005 | 2099 | 99.0 | 130 | 140 | 151 | 26 | 34 | 52 | -20 | -4 | 35 | 137 | 175 | 221 | 31 | 63 | 152 | 45 | 65 | 89 | 76 | 109 | 156 |
| 2006 | 1984 | 98.6 | 130 | 140 | 151 | 26 | 34 | 53 | -20 | -4 | 34 | 138 | 178 | 227 | 33 | 64 | 157 | 46 | 65 | 90 | 78 | 111 | 158 |
| 2007 | 2018 | 98.3 | 130 | 140 | 152 | 26 | 34 | 53 | -19 | -3 | 34 | 140 | 178 | 225 | 31 | 64 | 151 | 48 | 67 | 93 | 77 | 108 | 156 |
| 2008 | 2009 | 98.6 | 131 | 141 | 152 | 26 | 34 | 52 | -18 | -3 | 33 | 138 | 178 | 228 | 30 | 61 | 147 | 46 | 66 | 90 | 78 | 110 | 160 |
| 2009 | 1948 | 97.7 | 131 | 140 | 152 | 26 | 34 | 51 | -18 | -3 | 34 | 139 | 176 | 226 | 32 | 60 | 139 | 47 | 66 | 90 | 75 | 108 | 158 |
| 2010 | 1959 | 97.5 | 131 | 140 | 151 | 26 | 34 | 52 | -19 | -3 | 33 | 136 | 176 | 224 | 33 | 63 | 155 | 47 | 67 | 90 | 74 | 108 | 156 |
| 2011 | 2025 | 98.6 | 130 | 140 | 151 | 26 | 34 | 51 | -18 | -2 | 34 | 137 | 174 | 221 | 32 | 65 | 141 | 46 | 66 | 90 | 75 | 107 | 153 |
| 2012 | 2085 | 98.5 | 131 | 141 | 152 | 26 | 34 | 51 | -17 | -1 | 34 | 133 | 170 | 217 | 30 | 61 | 151 | 44 | 61 | 86 | 76 | 107 | 151 |
| 2013 | 2006 | 88.1 | 131 | 140 | 152 | 26 | 34 | 51 | -17 | -1 | 34 | 133 | 170 | 218 | 30 | 59 | 143 | 45 | 63 | 87 | 75 | 105 | 149 |
| 2014 | 1966 | 84.6 | 130 | 141 | 152 | 26 | 34 | 52 | -19 | -3 | 31 | 133 | 170 | 218 | 31 | 58 | 135 | 45 | 64 | 87 | 75 | 106 | 153 |
| 2015 | 1926 | 85.9 | 130 | 140 | 151 | 26 | 34 | 52 | -19 | -3 | 35 | 134 | 172 | 218 | 29 | 60 | 143 | 44 | 63 | 86 | 75 | 107 | 152 |
| 2016 | 1789 | 84.5 | 130 | 140 | 152 | 26 | 33 | 52 | -19 | -3 | 35 | 134 | 172 | 218 | 30 | 58 | 146 | 44 | 63 | 85 | 76 | 107 | 152 |
| 2017 | 1861 | 83.0 | 131 | 140 | 152 | 26 | 34 | 52 | -19 | -2 | 33 | 135 | 172 | 218 | 30 | 61 | 143 | 44 | 63 | 85 | 77 | 106 | 150 |
Table 1B. Secular trend in the percentile values of anthropometric measurements and serum lipid data. (Girls: n = 56864).
| Year | Number | Consultation rate (%) | Height (cm) | Weight (kg) | Percentage of overweight (%) | Total Cholesterol (mg/dL) Percentiles | Triglyceride (mg/dL) |
HDL Cholesterol (mg/dL) |
Non-HDL Cholesterol (mg/dL) |
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | |||
| 1991 | 2867 | 91.9 | 131 | 142 | 153 | 26 | 35 | 49 | -18 | -3 | 26 | 130 | 169 | 216 | 37 | 65 | 132 | 46 | 62 | 86 | 72 | 106 | 150 |
| 1992 | 2741 | 96.3 | 131 | 142 | 154 | 26 | 35 | 50 | -17 | -2 | 27 | 133 | 170 | 218 | 36 | 66 | 132 | 46 | 62 | 84 | 74 | 107 | 152 |
| 1993 | 2778 | 91.1 | 131 | 142 | 153 | 26 | 34 | 49 | -17 | -3 | 27 | 135 | 171 | 221 | 35 | 62 | 124 | 45 | 62 | 85 | 76 | 109 | 154 |
| 1994 | 2706 | 91.4 | 131 | 142 | 153 | 26 | 34 | 49 | -19 | -3 | 26 | 134 | 170 | 214 | 38 | 67 | 133 | 45 | 62 | 84 | 75 | 107 | 150 |
| 1995 | 2450 | 91.1 | 131 | 142 | 153 | 26 | 34 | 49 | -18 | -2 | 28 | 137 | 173 | 219 | 37 | 66 | 139 | 45 | 65 | 91 | 74 | 106 | 152 |
| 1996 | 2363 | 98.7 | 131 | 142 | 153 | 26 | 35 | 52 | -18 | -2 | 29 | 138 | 176 | 221 | 37 | 67 | 149 | 45 | 62 | 84 | 79 | 112 | 157 |
| 1997 | 2280 | 98.3 | 131 | 142 | 154 | 26 | 35 | 51 | -19 | -4 | 28 | 137 | 174 | 222 | 38 | 69 | 148 | 46 | 66 | 91 | 73 | 105 | 152 |
| 1998 | 2068 | 98.8 | 132 | 142 | 154 | 26 | 35 | 51 | -19 | -3 | 28 | 138 | 175 | 220 | 37 | 69 | 152 | 47 | 65 | 90 | 76 | 109 | 152 |
| 1999 | 2078 | 98.9 | 131 | 142 | 154 | 26 | 35 | 50 | -19 | -3 | 27 | 136 | 174 | 219 | 37 | 68 | 149 | 46 | 64 | 87 | 76 | 108 | 152 |
| 2000 | 2012 | 98.7 | 131 | 143 | 153 | 26 | 35 | 50 | -19 | -4 | 28 | 137 | 174 | 224 | 37 | 69 | 142 | 47 | 65 | 89 | 75 | 109 | 154 |
| 2001 | 1826 | 95.8 | 131 | 143 | 154 | 26 | 35 | 50 | -19 | -3 | 28 | 139 | 173 | 218 | 38 | 69 | 146 | 45 | 63 | 87 | 78 | 109 | 154 |
| 2002 | 1986 | 99.0 | 131 | 142 | 154 | 26 | 35 | 51 | -19 | -3 | 28 | 135.4 | 174 | 221 | 37 | 66 | 144 | 46 | 63 | 85 | 77 | 109 | 154 |
| 2003 | 1953 | 99.4 | 131 | 142 | 153 | 26 | 34 | 50 | -20 | -4 | 30 | 136 | 175 | 220 | 37 | 68 | 154 | 44 | 62 | 83 | 77 | 111 | 156 |
| 2004 | 1842 | 99.2 | 131 | 142 | 154 | 26 | 35 | 52 | -19 | -5 | 27 | 135 | 173 | 220 | 36 | 66 | 149 | 43 | 59 | 79 | 79 | 112 | 158 |
| 2005 | 1997 | 99.0 | 131 | 143 | 154 | 26 | 35 | 51 | -19 | -5 | 27 | 137 | 173 | 222 | 35 | 66 | 140 | 45 | 62 | 84 | 78 | 110 | 155 |
| 2006 | 1909 | 98.7 | 131 | 143 | 154 | 26 | 35 | 51 | -20 | -4 | 30 | 137 | 175 | 225 | 38 | 69 | 149 | 45 | 62 | 84 | 77 | 112 | 157 |
| 2007 | 1927 | 99.3 | 131 | 143 | 154 | 26 | 35 | 50 | -19 | -3 | 28 | 138 | 176 | 226 | 37 | 69 | 147 | 46 | 65 | 88 | 77 | 110 | 157 |
| 2008 | 1926 | 98.2 | 132 | 143 | 154 | 27 | 35 | 50 | -18 | -3 | 28 | 137 | 175 | 225 | 37 | 66 | 145 | 45 | 63 | 85 | 80 | 111 | 158 |
| 2009 | 1937 | 97.8 | 131 | 143 | 153 | 26 | 34 | 50 | -19 | -4 | 27 | 136 | 175 | 227.1 | 36 | 66 | 138 | 45 | 63 | 85 | 77 | 111 | 159 |
| 2010 | 1958 | 98.7 | 132 | 142 | 153 | 26 | 34 | 49 | -18 | -3 | 27 | 136 | 174 | 222 | 37 | 68 | 145 | 46 | 64 | 85 | 77 | 109 | 154 |
| 2011 | 1961 | 99.3 | 132 | 142 | 154 | 26 | 34 | 50 | -17 | -2 | 27 | 136 | 173 | 224 | 39 | 70 | 147 | 45 | 63 | 85 | 77 | 109 | 159 |
| 2012 | 2072 | 98.9 | 131 | 143 | 154 | 26 | 35 | 50 | -18 | -2 | 27 | 133 | 169 | 219 | 35 | 64 | 133 | 43 | 60 | 80 | 78 | 109 | 154 |
| 2013 | 1924 | 90.6 | 131 | 143 | 154 | 26 | 35 | 50 | -17 | -2 | 30 | 134 | 171 | 220 | 35 | 65 | 139 | 44 | 61 | 81 | 78 | 108 | 154 |
| 2014 | 1869 | 87.2 | 131 | 143 | 153 | 26 | 35 | 50 | -19 | -3 | 27 | 133 | 170 | 218 | 34 | 64 | 135 | 44 | 61 | 81 | 78 | 108 | 152 |
| 2015 | 1775 | 86.3 | 132 | 142 | 154 | 26 | 35 | 50 | -17 | -2 | 29 | 133 | 171 | 219 | 35 | 64 | 132 | 44 | 61 | 82 | 77 | 109 | 155 |
| 2016 | 1774 | 83.4 | 132 | 143 | 154 | 26 | 35 | 50 | -17 | -2 | 29 | 133 | 171 | 215 | 34 | 63 | 135 | 45 | 60 | 80 | 76 | 109 | 151 |
| 2017 | 1885 | 85.3 | 131 | 142 | 154 | 26 | 34 | 50 | -18 | -3 | 31 | 135 | 171 | 216 | 34 | 64 | 140 | 45 | 61 | 82 | 76 | 108 | 152 |
Secular Trends in Obesity
The secular trends of the percentages of children with obesity (i.e., mild obesity (POW-20), moderate obesity (POW-30), and severe obesity (POW-50)) are shown in Fig.1 . The numbers of children with mild and moderate obesity seemed to slightly fluctuate, whereas those of severe obesity gradually increased during the observed years among both boys and girls.
Fig.1. Secular trends in the percentages of children with obesity.
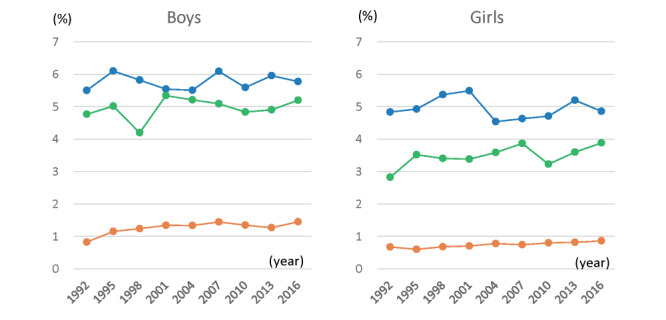
Left side, boys; right side, girls. Data obtained every three years are serially shown. Blue circles, mild obesity (POW-20); green circles, moderate obesity (POW-30); and orange cycles, severe obesity (POW-50).
The annual trend in obesity was statistically evaluated and matched to the quadratic method ( Suppl. Table 1 ) . The percentage of children with mild obesity (POW-20) showed weak peaks early in the observation period (in 1994 for boys and 2001 for girls, respectively). The percentages of moderate and severe obesity (POW-30 and POW-50) generally increased, with peaks observed later in the observation period (in 2014 and 2009 for boys, and 2017 and 2016 for girls) ( Suppl. Table 2 ) .
Supplementary Table 1. Validation of the regression models by four estimation methods.
| Percentage of overweight (%) | Regression models | Degree of suitability | Decision | |||||
|---|---|---|---|---|---|---|---|---|
| AIC | R-Squared | MAE | Likelihood Ratio Test | |||||
| boys | Prevalence of obesity (%) | 20 to <30 | WLS | 263.9979 | 0.0848 | 20.8958 | -128.9990 | Quadratic |
| Quadratic | 201.2367 | 0.8913 | 6.0901 | -95.6180 | ||||
| 30 to <50 | WLS | 243.5526 | 0.0147 | 13.6816 | -118.7760 | Quadratic | ||
| Quadratic | 207.4312 | 0.7599 | 7.4561 | -98.7160 | ||||
| ≥ 50 | WLS | 192.2043 | 0.3230 | 5.6575 | -93.1020 | Quadratic | ||
| Quadratic | 150.4751 | 0.7482 | 2.6621 | -70.2380 | ||||
| girls | Prevalence of obesity (%) | 20 to <30 | WLS | 252.7594 | 0.0914 | 18.9586 | -123.3800 | Quadratic |
| Quadratic | 212.8955 | 0.7325 | 8.3577 | -101.4500 | ||||
| 30 to <50 | WLS | 245.1583 | 0.0548 | 18.9712 | -119.5790 | Quadratic | ||
| Quadratic | 194.2519 | 0.4301 | 5.9545 | -92.1260 | ||||
| ≥ 50 | WLS | 138.5724 | 0.0548 | 2.2998 | -66.2860 | Quadratic | ||
| Quadratic | 135.7715 | 0.4301 | 1.9718 | -62.8860 | ||||
Supplementary Table 2. The estimated peak years of obesity.
| Sex | Boys | Girls | ||||
|---|---|---|---|---|---|---|
| Percentage of overweight(%) | 20 to <30 | 30 to <50 | ≥ 50 | 20 to <30 | 30 to <50 | ≥ 50 |
| Year | 1994 | 2014 | 2009 | 2001 | 2017 | 2016 |
| Peak value | 6.32 | 5.03 | 1.41 | 5.04 | 3.74 | 0.87 |
| P for trend | 3.10E-11* | 2.61E-07* | 4.48E-07* | 8.91E-07* | 3.71E-07* | 4.23E-03* |
Secular Trends in Anthropometric Data
A regression analysis was performed to evaluate the annual trends in height, weight, and POW, with only height ultimately being matched to the quadratic method ( Suppl. Table 3 ) ; however, the quadratic curves of height seemed very gentle ( Suppl. Fig.1 A ) . The 95th percentile of height for boys and the 5th, 50th, and 95th percentile of height for girls significantly increased. The body weight was almost consistent, except for a decrease in the 5th percentile of weight for boys ( Suppl. Fig.1B ) . The 95th percentile of POW significantly increased for both boys and girls ( Suppl. Fig.1C , Suppl. Table 4 ) .
Supplementary Table 3. Validation of regression models by four estimation methods.
| Regression models | Degree of suitability | Decision | ||||
|---|---|---|---|---|---|---|
| AIC | R-Squared | MAE | Likelihood Ratio Test | |||
| Height | WLS | 17.1555 | 0.9994 | 0.2537 | -5.5778 | Quadratic |
| Quadratic | 18.0632 | 0.9995 | 0.2217 | -4.0316 | ||
| Weight | WLS | 72.5468 | 0.9868 | 0.7178 | -33.2730 | WLS |
| Quadratic | 72.8696 | 0.9877 | 0.6807 | -32.4350 | ||
| Percentage of overweight | WLS | 84.4216 | 0.9607 | 0.8204 | -39.2110 | WLS |
| Quadratic | 86.7339 | 0.9659 | 0.8344 | -39.3670 | ||
| Total Cholesterol | WLS | 141.7150 | 0.9592 | 2.5360 | -67.8580 | Quadratic |
| Quadratic | 135.3710 | 0.9714 | 2.1415 | -63.6850 | ||
| Triglyceride | WLS | 195.2624 | 0.5710 | 7.1699 | 94.6310 | Quadratic |
| Quadratic | 161.4676 | 0.8845 | 3.5227 | 76.7340 | ||
| HDL cholesterol | WLS | 126.3208 | 0.9325 | 1.9583 | -60.1600 | Quadratic |
| Quadratic | 127.3320 | 0.9464 | 1.5778 | -59.6660 | ||
| Non-HDL cholesterol | WLS | 134.4495 | 0.9579 | 2.2635 | 64.2250 | Quadratic |
| Quadratic | 126.8145 | 0.9702 | 1.8225 | 59.4070 | ||
Supplementary Fig.1. Secular trends in the percentiles of anthropometric parameters.
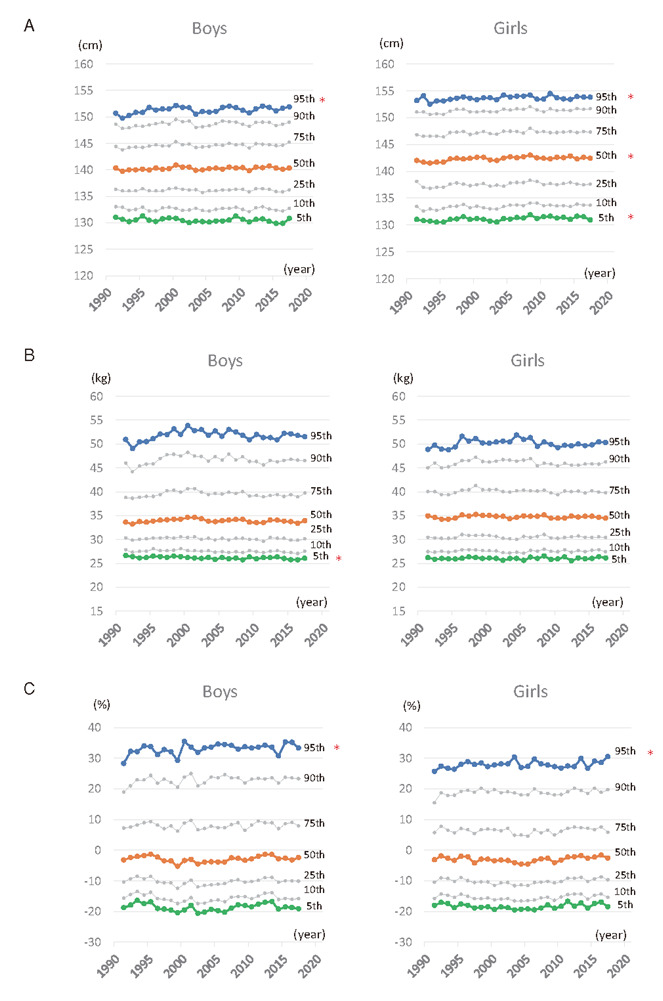
A, Height. B, Weight. C, Percentage of overweight (POW). Blue circles, 95th percentile; orange circles, 50th percentile; and green circles, 5th percentile. Gray circles, 10th, 25th, 75th, and 90th percentiles. Secular trends in the 5th, 50th, and 95th percentiles were statistically analyzed. *P<0.05.
Supplementary Table 4. Secular trends in body weight and the percentage of overweight children.
| Regression coefficient (95% CI) | ||
|---|---|---|
| boys (n = 58690) | girls (n = 56861) | |
| Body weight (kg) | ||
| 95th percentile | -0.005 (-0.049 to 0.039) | -0.006 (-0.042 to 0.031) |
| 50th percentile | -0.010 (-0.026 to 0.007) | -0.006 (-0.02 to 0.007) |
| 5th percentile | -0.021 (-0.031 to -0.011)a | 0.001 (-0.011 to 0.012) |
| Percentage of overweight (%) | ||
| 95th percentile | 0.081 (0.005 to 0.158)a | 0.066 (0.009 to 0.123)a |
| 50th percentile | 0.029 (-0.018 to 0.077) | 0.024 (-0.019 to 0.066) |
| 5th percentile | 0.012 (-0.046 to 0.070) | 0.004 (-0.039 to 0.047) |
Secular Trends in Serum Lipid Analytes
Table 1 also shows the long-term trends in serum lipids (TC, TG, HDL-C, and non-HDL-C). A regression analysis was performed to evaluate the annual trends in lipids, which mostly matched the quadratic method ( Suppl. Table 3 ) . The 5th, 50th, and 95th percentile values of TC, TG, and non-HDL-C values showed a mild inverted U shape with peaks during the later years of the observation period ( Suppl. Fig.2 A, B, and D ) . In contrast, the HDL-C level mostly decreased, with modest peaks during the earlier years of the observation period ( Suppl. Fig.2C and Suppl. Table 5 ) .
Supplementary Fig.2. Secular trends in the percentiles of serum lipid levels.
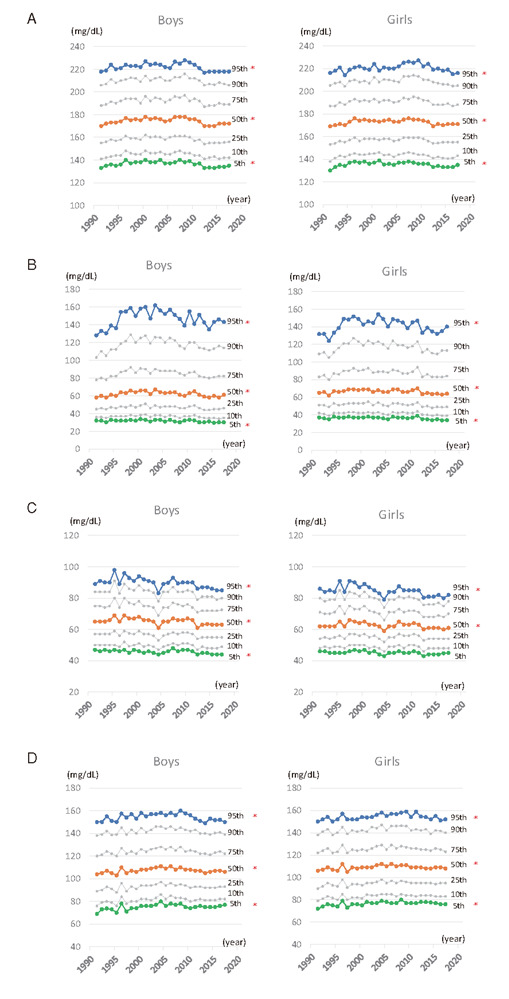
A, TC; B, TG; C, HDL-C; and D, non-HDL-C. Blue circles, 95th percentile; orange circles, 50th percentile; and green circles, 5th percentile. Gray circles, 10th, 25th, 75th, and 90th percentiles. The secular trends in the 5th, 50th, and 95th percentiles were statistically analyzed by the quadratic method. *P<0.05.
Supplementary Table 5. The estimated peak years of serum lipid levels.
| Sex | Boys | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total cholesterol (mg/dL) | Triglyceride(mg/dL) | HDL cholesterol (mg/dL) | Non-HDL cholesterol (mg/dL) | |||||||||
| Percentiles | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th |
| Year | 2001 | 2001 | 2002 | 2000 | 2001 | 2001 | 1993 | 1997 | 1997 | 2008 | 2005 | 2003 |
| Peak value | 139 | 177 | 225 | 33 | 65 | 157 | 47 | 67 | 93 | 77 | 109 | 157 |
| P for trend | 9.20E-06* | 1.21E-05* | 0.0001* | 0.002* | 4.46E-05* | 5.91E-06* | 0.02* | 0.004* | 0.001* | 0.002* | 0.001* | 9.76E-05* |
| Sex | Girls | |||||||||||
| Total cholesterol (mg/dL) | Triglyceride(mg/dL) | HDL cholesterol (mg/dL) | Non-HDL cholesterol (mg/dL) | |||||||||
| Percentiles | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th | 5th | 50th | 95th |
| Year | 2005 | 2001 | 2001 | 2002 | 2001 | 2001 | 2001 | 1998 | 2008 | 2005 | 2005 | |
| Peak value | 138 | 175 | 224 | 37 | 69 | 152 | 64 | 87 | 78 | 110 | 156 | |
| P for trend | 0.0001* | 5.26E-05* | 0.0003* | 0.001* | 0.001* | 2.51E-05* | 0.07 | 0.04* | 0.005* | 0.0006* | 0.008* | 0.0009* |
Trends in Inappropriate Levels of Serum Lipid in Obese and Non-Obese Children
The secular trends in the percentage of children with TC, TG, and non-HDL-C above or HDL-C values below the cut-off levels are shown in Figure 2A-D . Inverse U shapes were observed in the percentages of increased TC, TG, and non-HDL-C levels, whereas a gradual increase in children with reduced HDL-C levels was shown. The inappropriate lipid levels in non-obese and obese children were separately evaluated, and the percentages of obese children with inappropriate levels of lipids were markedly higher than among non-obese children ( Fig.3A-D ) . In particular, the percentage of severely obese children with reduced HDL-C levels gradually increased during the 27-year period ( Fig.4 ) .
Fig.2. Secular trends in the percentage of children with inappropriate levels of lipids.
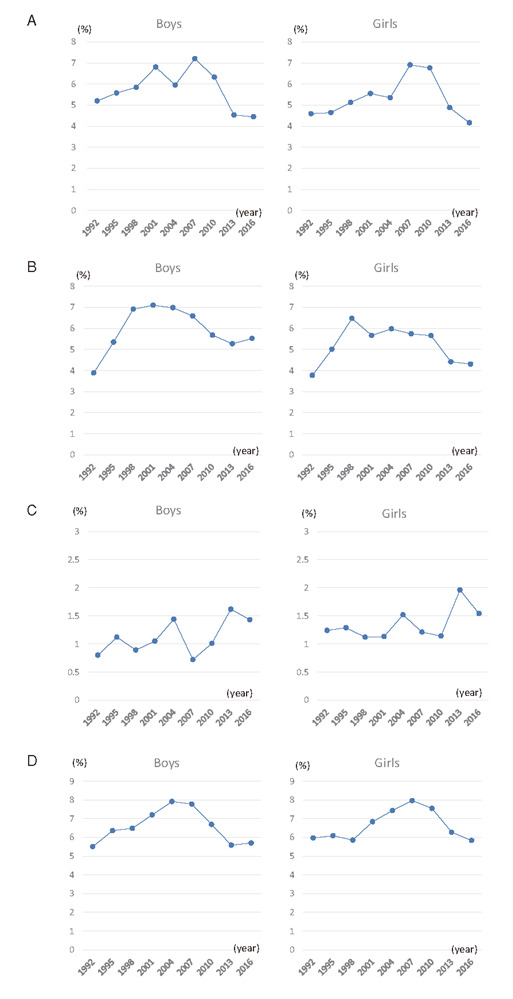
A, TC ≥ 220 mg/dl; B, TG ≥ 140 mg/dl; C, HDL-C <40 mg/dl; and D, non-HDL-C ≥ 150 mg/dl. Left side, boys; right side, girls. Data obtained every three years are serially shown.
Fig.3. Secular trends in the percentages of children with inappropriate levels of lipids in non-obese or obese.
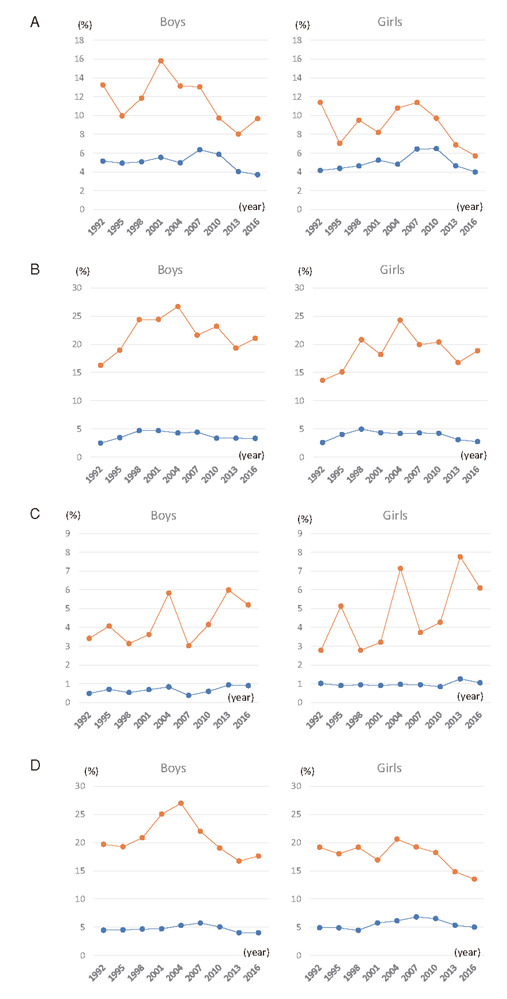
A, TC ≥ 220 mg/dl; B, TG ≥ 140 mg/dl; C, HDL-C <40 mg/dl; and D, non-HDL-C ≥ 150 mg/dl. Left side, boys; right side, girls. The dots of three-year data are serially shown. Blue circles, non-obese (POW <20) and orange circles, obese (POW ≥ 20).
Fig.4. Comparison of secular trends in the percentages of children with lower HDL-cholesterolemia divided by POWs.
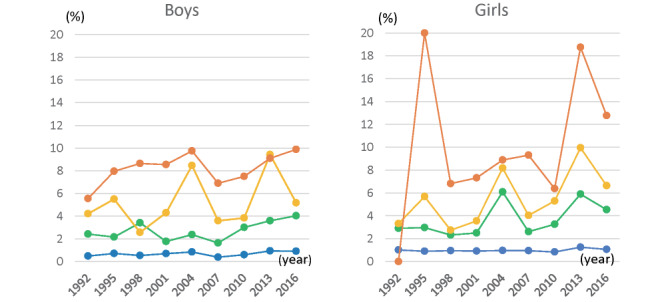
Left side, boys; right side, girls. The dots of three-year data are serially shown. Blue circles, non-obese; green cycles, mild obesity (POW-20); yellow cycles, moderate obesity (POW-30); and orange circles, severe obesity (POW-50).
Secular trends in lipid levels were separately evaluated and classified by the degree of obesity: mild obese (POW-20), moderate obese (POW-30), severe obese (POW-50), and non-obese ( Suppl. Fig.3A-D ) . TG and non-HDL-C levels were consistently higher in obese children than in non-obese ones, and HDL-C levels were lower in obese children than in non-obese ones.
Supplementary Fig.3. Comparison of a secular trend in lipid levels divided by POWs.
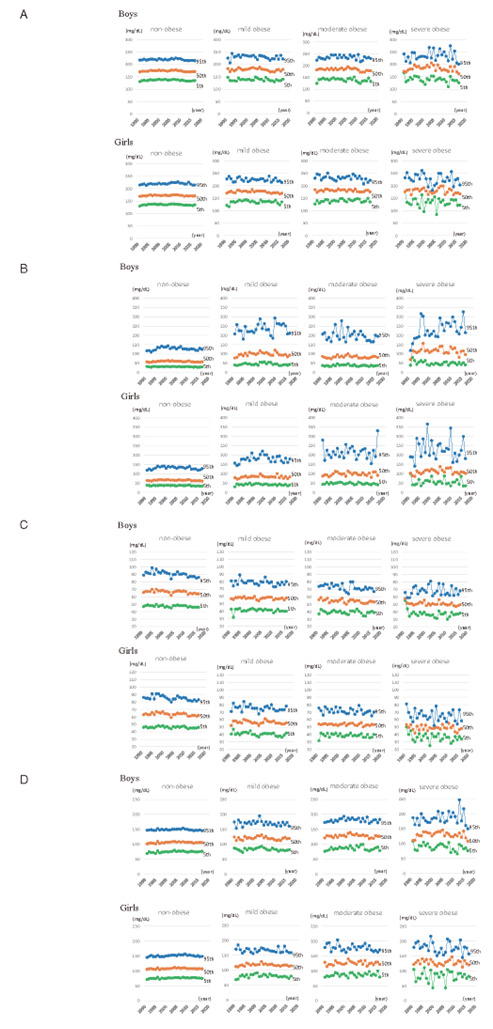
Upper panels for boys; lower ones for girls. A, TC; B, TG; C, HDL-C; and D, non-HDL-C. Blue circles, 95th percentile; orange circles, 50th percentile; and green circles, 5th percentile.
Discussion
This study reported the secular trends in overweight children and the blood lipid profiles of fifth-grade elementary school students. The trend in the rate of severe obesity in children in Oita City showed a gradual increase over the 27-year study period. The data seem consistent with the data of the school health statistics reported by the Ministry of Education, Culture, Sports, Science and Technology. The percentage of obese children of 11 years of age in Japan was increased from 6.72% for boys and 6.18% for girls in 1977 to 11.82% for boys and 9.65% for girls in 2006, then gradually decreased to 9.69% for boys and 8.72% for girls in 2017, and then re-increased to 11.11% for boys and 8.84% for girls in 2019 16) . Kouda et al. reported that the prevalence of obesity tended to increase in children in Iwata City from 1997 to 2001 17) , whereas they also reported that the 95th percentile of BMI increased, and that the 5th percentile decreased from 1993 to 2008 18) . Kouda et al. also reported that children in Fukuroi City, adjacent to Iwata City in Shizuoka Prefecture, were almost stable from 2007 to 2017 19) . In contrast, Shirakawa et al. reported that the prevalence of obesity of children in the small town of Ina in Saitama Prefecture, Japan, tended to decrease according to a survey conducted from 2003 to 2012 20) . Tanaka et al. also reported a decreasing trend from 2009 to 2011 and that the rates of moderate or severe obesity remained almost stable thereafter in the Setagaya area in Tokyo, a metropolitan area of Japan 21) . Overall, the obesity of Japanese children tended to increase from the 1980s to 2000, and the increasing trend peaked in the early 2000s and stabilized or generally decreased, especially in large cities or metropolitan areas in comparison to small towns. A further study, however, indicated that the rate of severe obesity in rural areas or small towns continued to increase, as shown in Iwata City by Kouda et al., and in Oita City in the present study. This probably depends on the environmental or cultural aspects of life in each city. In particular, in Oita City, the rates of childhood obesity have long been consistently higher than the national average (fifth graders: 10.3% in 1994, 11.2% in 2000, 10.1% in 2010, and 11.1% in 2018). These results suggest that it would be difficult to change the rate of childhood obesity in municipalities with a high rate of childhood obesity, especially small-size rural cities.
To our knowledge, there have been no reports on the long-term secular trend (>+25 years) of serum lipid values in Japanese children of around 10 years of age. According to reports on the secular trend in serum lipids, there were no significant changes in TC, non-HDL-C, and HDL-C in Iwata City from 1993 to 2008 18) , whereas HDL-C seemed to slightly increase in Fukuroi from 2007 to 2017 19) ; both were adjacent small cities in Shizuoka. In contrast, our longitudinal study of Oita City, a mid-size capital city of Oita Prefecture, from 1991 to 2017 demonstrated a downward trend in HDL-C after the late 1990s and a slight upward trend in TC, TG, and non-HDL-C after the early 2000s. Notably, these trends were remarkable in obese children. These data suggest that the risk of dyslipidemia or cardiovascular disease in adulthood seemed consistent in Oita City, but careful observations are needed, especially concerning the decreasing secular trend in HDL-C, particularly in obese children.
The present study was associated with some limitations. First, since the rate of registration was approximately 80%–90%, the remaining unenrolled children might have had different characteristics (i.e., an underlying selection bias might have affected the results). It has been reported that the rate of severely lean children with psychological disorders, such as anorexia nervosa, has been increasing in Japan; this trend was not observed in the present study. We hypothesize that severely lean children, especially girls, would have avoided enrolling in this health check-up program; this is suggested by the lower enrollment ratios in the later years. Second, the serum HDL-C and LDL-C levels are negatively associated with testosterone or estradiol in boys or girls during puberty; however, we could not evaluate the stage of puberty. Since the height, weight, and obesity index of the enrolled children gradually increased during the 27-year period, especially in girls, it might be associated with the trend in the rejuvenation of puberty. This might—at least in part—have influenced the secular trend in serum cholesterol values. Finally, affected individuals with familial hypercholesterolemia (FH) were included in this study although we did not evaluate this point. FH is an autosomal dominant disease caused by abnormalities in the genes that encode low-density lipoprotein (LDL) receptors or related molecules, characterized by hyper-LDL cholesterolemia with an estimated prevalence of approximately 1 in 200–500 in Japan 22) . It is estimated that about 10–20 children with FH were included per year, showing very high cholesterolemia without obesity. A further study considering the familial history of FH or medical information of the enrolled children will be important when re-evaluating the findings of the present study.
Conclusion
We reported the analysis of 27 years of anthropometric and blood chemistry data from a children’s lifestyle-related disease screening program in Oita City. The obese children had higher percentages of inappropriate lipid levels than non-obese ones. Primary intervention to prevent obesity at earlier school grades would be important for decreasing childhood obesity and for reducing lifestyle-related diseases when these children reach adulthood.
Acknowledgements
The authors wish to acknowledge Dr. Keishi Mori in the Shido Corp. for his help in interpreting the significance of the results of the statistical analysis in this study.
Notice of Grant Support
This study was supported by the Grants‐in‐Aid for Scientific Research (C) (20K11648) from JSPS; a Japanese Society for Pediatric Endocrinology Future Development Grant supported by Novo Nordisk Pharma Ltd; a grant from Oita City Pediatric Association. The funders had no role in the design of the study, in the collection, analysis, or interpretation of data, or in the writing the manuscript.
Conflict of Interest
The authors declare no conflicts of interest in association with the present study.
Ethics
This study was approved by the ethics committee of Oita University Hospital, Oita, Japan (No. 1525). All procedures followed were performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
References
- 1).Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, Flegal KM. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988-1994 Through 2013-2014. JAMA, 2016; 315: 2292-2299 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2).Pan L, Freedman DS, Sharma AJ, Castellanos-Brown K, Park S, Smith RB, Blanck HM. Trends in Obesity Among Participants Aged 2-4 Years in the Special Supplemental Nutrition Program for Women, Infants, and Children - United States, 2000-2014. MMWR Morb Mortal Wkly Rep, 2016; 65: 1256-1260 [DOI] [PubMed] [Google Scholar]
- 3).Pan L, Blanck HM, Park S, Galuska DA, Freedman DS, Potter A, Petersen R. State-Specific Prevalence of Obesity Among Children Aged 2-4 Years Enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children - United States, 2010-2016. MMWR Morb Mortal Wkly Rep, 2019; 68: 1057-1061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4).Skinner AC, Perrin EM, Skelton JA. Prevalence of obesity and severe obesity in US children, 1999-2014. Obesity (Silver Spring), 2016; 24: 1116-1123 [DOI] [PubMed] [Google Scholar]
- 5).Skinner AC, Ravanbakht SN, Skelton JA, Perrin EM, Armstrong SC. Prevalence of Obesity and Severe Obesity in US Children, 1999-2016. Pediatrics, 2018; 141: e20173459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6).Ells LJ, Hancock C, Copley VR, Mead E, Dinsdale H, Kinra S, Viner RM, Rutter H. Prevalence of severe childhood obesity in England: 2006-2013. Arch Dis Child, 2015; 100: 631-636 [DOI] [PubMed] [Google Scholar]
- 7).Hudda MT, Nightingale CM, Donin AS, Owen CG, Rudnicka AR, Wells JCK, Rutter H, Cook DG, Whincup PH. Patterns of childhood body mass index (BMI), overweight and obesity in South Asian and black participants in the English National child measurement programme: effect of applying BMI adjustments standardising for ethnic differences in BMI-body fatness associations. Int J Obes (Lond), 2018; 42: 662-670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8).Murata M. Secular trends in growth and changes in eating patterns of Japanese children. Am J Clin Nutr, 2000; 72: 1379s-1383s [DOI] [PubMed] [Google Scholar]
- 9).Urashima M, Wada T, Fukumoto T, Joki M, Maeda T, Hashimoto H, Oda S. Prevalence of metabolic syndrome in a 22,892 Japanese population and its associations with life style. Japan Medical Association Journal, 2005; 48: 441-450 [Google Scholar]
- 10).Kubo T. Common approach to childhood obesity in Japan. J Pediatr Endocrinol Metab, 2014; 27: 581-592 [DOI] [PubMed] [Google Scholar]
- 11).Matsushita Y, Yoshiike N, Kaneda F, Yoshita K, Takimoto H. Trends in childhood obesity in Japan over the last 25 years from the national nutrition survey. Obes Res, 2004; 12: 205-214 [DOI] [PubMed] [Google Scholar]
- 12).Ozeki T. The concept of metabolic syndrome in children, diagnostic criteria for Japanese children. “A cohort study on the concept, pathophysiology, diagnostic criteria and effective intervention of childhood metabolic syndrome”. Ministry of Health, Labor and Welfare Research Grant Subsidy Comprehensive Research Project for Measures against Lifestyle-related Diseases such as Cardiovascular Diseases; 2008 [Google Scholar]
- 13).Dobashi K. Evaluation of Obesity in School-Age Children. J Atheroscler Thromb, 2016; 23: 32-38 [DOI] [PubMed] [Google Scholar]
- 14).Kinoshita M, Yokote K, Arai H, Iida M, Ishigaki Y, Ishibashi S, Umemoto S, Egusa G, Ohmura H, Okamura T, Kihara S, Koba S, Saito I, Shoji T, Daida H, Tsukamoto K, Deguchi J, Dohi S, Dobashi K, Hamaguchi H, Hara M, Hiro T, Biro S, Fujioka Y, Maruyama C, Miyamoto Y, Murakami Y, Yokode M, Yoshida H, Rakugi H, Wakatsuki A, Yamashita S. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017. J Atheroscler Thromb, 2018; 25: 846-984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15).Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics, 2011; 128 Suppl 5: S213-256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16).Ministry of Education, Culture, Sports, Science and Technology. [Annual Report of School Health Statistics Survey in 2019.] [Available from: https://www.mext.go.jp/b_menu/toukei/chousa05/hoken/1268826.htm. [Google Scholar]
- 17).Kouda K, Nakamura H, Tokunaga R, Takeuchi H. Trends in levels of cholesterol in Japanese children from 1993 through 2001. J Epidemiol, 2004; 14: 78-82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18).Kouda K, Nakamura H, Nishio N, Fujita Y, Takeuchi H, Iki M. Trends in body mass index, blood pressure, and serum lipids in Japanese children: Iwata population-based annual screening (1993-2008). J Epidemiol, 2010; 20: 212-218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19).Kouda K, Iki M, Fujita Y, Nakamura H, Ohara K, Tachiki T, Nishiyama T. Trends in Serum Lipid Levels of a 10- and 13-Year-Old Population in Fukuroi City, Japan (2007-2017). J Epidemiol, 2020; 30: 24-29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20).Shirasawa T, Ochiai H, Nanri H, Nishimura R, Ohtsu T, Hoshino H, Tajima N, Kokaze A. Trends of Underweight and Overweight/Obesity Among Japanese Schoolchildren From 2003 to 2012, Defined by Body Mass Index and Percentage Overweight Cutoffs. J Epidemiol, 2015; 25: 482-488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21).Tanaka H, Morisaki N, Piedvache A, Harada S, Urayama KY. Trends in obesity and blood lipid abnormalities in school-age children in Japan. Pediatr Int, 2021; 63: 825-832 [DOI] [PubMed] [Google Scholar]
- 22).Harada-Shiba M, Arai H, Ishigaki Y, Ishibashi S, Okamura T, Ogura M, Dobashi K, Nohara A, Bujo H, Miyauchi K, Yamashita S, Yokote K. Guidelines for Diagnosis and Treatment of Familial Hypercholesterolemia 2017. J Atheroscler Thromb, 2018; 25: 751-770 [DOI] [PMC free article] [PubMed] [Google Scholar]