

Short abstract
An electrocardiogram showing atrial flutter in which varying ratios of AV conduction and the cyclical recurrence of varying QRS morphologies are observed is presented.
Keywords: atrial flutter, fascicular blocks, multilevel AV block
Variable ratios of atrioventricular conduction observed during atrial flutter and other atrial tachyarrhythmias are widely considered to be caused by conduction delay or block at two or more levels of the conduction system. 1 In cases of atrial flutter, even ratios of conduction predominate. Multilevel block at the AV node, like concealed conduction, is inferred on the basis of the behavior of the distally recorded complexes. Proximal conduction through the His‐Purkinje system is not recorded on a surface electrocardiogram. Thus, AV node conduction comprises the upper AV node, lower AV node, and the His‐Purkinje system.
Here we present an electrocardiogram of a 42 year old obese, hypertensive gentlemen who had been binge drinking alcohol for 4 days prior to reporting to the emergency room with palpitations and shortness of breath. Initial electrocardiogram, recorded on arrival to the emergency room, showed atrial flutter with 2:1 conduction and heart rate of 160 bpm. The second electrocardiogram showing atrial flutter in which varying ratios of AV conduction and the cyclical recurrence of varying QRS morphologies was observed (Figure 1). It was recorded 2 h after the administration of IV diltiazem.
FIGURE 1.

Twelve lead ECG of atrial flutter with varying conduction.
The electrocardiogram shows atrial flutter with a cycle length of 200 ms and varying AV conduction. The flutter wave morphology in lead II is consistent with typical counterclockwise right atrial flutter. In each recurring cycle, there are 8 flutter waves and 3 QRS complexes, a narrow QRS complex with a duration of 80 ms is preceded by four flutter waves. A 2:1 conduction ratio at the upper level of the AV node and 2:1 conduction of flutter impulses at the second level of block result in net 4:1 conduction at the ventricular level (Figure 2). The 4:1 conduction ratio creates R‐R intervals of sufficient length to allow full recovery of the distal conduction system so that the first QRS complex in each cycle is narrow (Figure 3). These observations suggest multilevel block in the atrioventricular node and the His‐Purkinje system.
FIGURE 2.

Ladder diagram of rhythm strip, 3 different QRS morphologies. A, Atrium; AVN‐U, Atrioventricular node upper level; AVN‐L, Atrioventricular node lower level; F, Fascicular conduction system; V, Ventricle.  Right bundle branch block.
Right bundle branch block.  Left anterior fascicular block.
Left anterior fascicular block.  Incomplete right bundle branch block.
Incomplete right bundle branch block.
FIGURE 3.
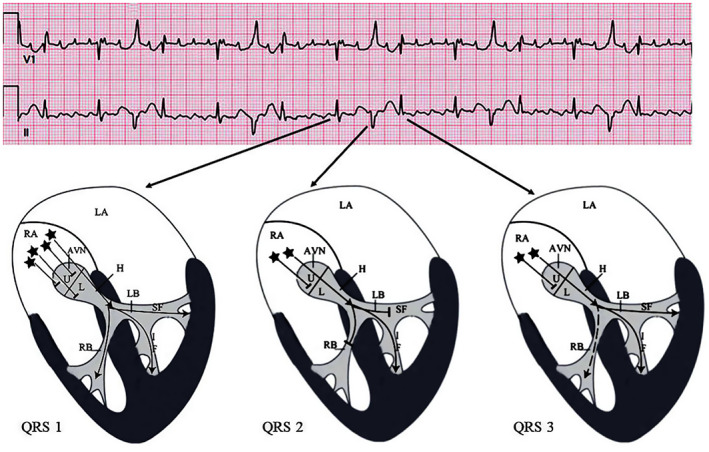
Cartoon illustration of multilevel AV block and 3 different QRS morphologies. AVN, Atrioventricular node; H, His bundle; IF, Inferior fascicle of the left bundle; L, AVN lower‐level; LA, Left atrium; LB, Left bundle branch; RA, Right atrium; RB, Right Bundle‐Branch; SF, Superior fascicle of the left bundle; U, AVN upper‐level.  Flutter waves.
Flutter waves.
The second QRS complex, with a duration of 120 ms, is preceded by two flutter waves, occurs 440 ms after the narrow QRS complex, and exhibits the morphology of right bundle branch block and left anterior fascicular block. Sudden shortening of the R‐R interval results in aberrant ventricular conduction, an example of the Ashman phenomenon 2 (Figures 2 and 3). The increase in f3‐QRS2 interval (160 ms.) as compared to f1‐QRS1 interval (120 ms) (Figure 4) is perhaps due to increased refractoriness at the AV node level as a result of preceding long cycle length followed by short cycle length. Other possibilities include concealed conduction, atypical Wenckebach periodicity, or antegrade conduction through slow pathway.
FIGURE 4.

Magnified section of the electrocardiogram. f, flutter wave; ML, Marker line showing the onset of the QRS complex.
Ashman's phenomenon refers to an aberrant conduction due to critical prematurity. A long R‐R interval is followed by a short R‐R interval that ends with a wide QRS complex, often with RBBB morphology. 3 Similar combinations of long and short cycle lengths results in aberrantly conducted second QRS complex in subsequent cycles.
Heart rate has a modulating effect on the refractory period of cardiac conduction system. As the heart rate slows, the refractory period of the conduction system lengthens and as heart rate speeds up, the refractory period shortens. Thus, the cycle length of the preceding R‐R interval determines the refractory period of the following beat.
The refractory periods of the right and left bundle are different. The longer refractory period of the right bundle branch predisposes it to conduction slowing or failure, particularly with sudden acceleration of the heart rate as seen in atrial flutter, premature atrial beats or atrial fibrillation. As a result aberrant conduction, a transient functional block, more often exhibits RBBB morphology in lead V1.
The third QRS complex in each cycle has a duration of 100 ms, occurs 400 ms after the second QRS complex, and exhibits the morphology of incomplete right bundle branch block without left anterior fascicular block. This QRS complex in each cycle is narrower perhaps as a result of supernormal conduction or peeling of refractory period.
During the recovery phase of AP supernormal conduction may exist when a subthreshold stimulus may produce a response. 4 Similar stimulus may fail to generate response before or after supernormal conduction period. The property of supernormal excitability and conduction exists only in Purkinje fibers. Arrival of an electrical impulse during supernormal excitability conducts when otherwise a slowing of conduction or block would have been expected. 5 During accelerated heart rate a widening of QRS complex may occur as a result of acceleration dependent aberrancy and occasional occurrence of atrial premature beats with narrow QRS complex may be a manifestation of supernormal conduction.
Cyclical allorhythmic repetitions is a result of multilevel block at the AV node and the His‐Purkinje system. Although conduction through the His‐Purkinje system is not recorded on the surface electrocardiogram, the lack of it can be stipulated from fascicular blocks. Following the third QRS complex in each cycle, the resumption of 4:1 AV conduction permits full recovery of the distal conduction pathway. The chain of events then repeats in cyclical fashion resulting in an allorhymia displaying three different QRS morphologies.
FUNDING INFORMATION
No funding was involved.
CONFLICT OF INTEREST
There was no conflict of interest.
ETHICS APPROVAL STATEMENT
Ethics guidelines were followed. IRB approval is not required.
PATIENT CONSENT STATEMENT
N/A.
CLINICAL TRIAL REGISTRATION
N/A.
Abedin Z, Conner RP, Ali S, Dahal R, Abedin M. Atrial flutter with multilevel atrioventricular block and cyclical occurrence of varying QRS morphologies. J Arrhythmia. 2023;39:78–81. 10.1002/joa3.12798
REFERENCES
- 1. Scholz EP, Kehrle F, Vossel S, Hess A, Zitron E, Katus HA, et al. Discriminating atrial flutter from atrial fibrillation using a multilevel model of atrioventricular conduction. Heart Rhythm. 2014;11(5):877–84. [DOI] [PubMed] [Google Scholar]
- 2. Luzza F, Calabrò MP, Carerj S, Oreto G. Bundle branch block in alternate beats during 2:1 atrial flutter. J Electrocardiol. 2006;39(1):38–41. [DOI] [PubMed] [Google Scholar]
- 3. Abedin Z. Differential diagnosis of wide QRS tachycardia: a review. J Arrhythm. 2021;37(5):1162–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Costantini M. Supernormal and alternating conduction in intermittent bundle branch block and intermittent or concealed ventricular preexcitation. Electrophysiological study, mechanisms and clinical considerations. G Ital Cardiol. 2016;17(5):370–6. [DOI] [PubMed] [Google Scholar]
- 5. Oreto G, Smeets JLRM, Rodriguez LM, Timmermans C, Wellens HJJ. Supernormal conduction in the left bundle branch. J Cardiovasc Electrophysiol. 1994;5(4):345–9. [DOI] [PubMed] [Google Scholar]