

Abstract
Aim
To describe the surgical technique for gradual lengthening of the metatarsal using the Orthofix MiniRail System (Orthofix Medical Inc., Lewisville, TX, USA).
Background
Brachymetatarsia refers to the shortening of the metatarsal bone. When indicated, metatarsal lengthening is performed to treat this deformity.
Technique
A dorsal approach to the short metatarsal is performed, protecting the neurovascular structures and the extensor tendons. The most proximal wire or screw is inserted first, followed by the most distal wire or screw. The distal wire or screw should not be inserted in the metatarsal head. The middle wires or screws are inserted thereafter. All wires or screws should be placed perpendicular to the anatomic axis of the bone. Once the MiniRail lengthener is assembled, a 1.6 mm K-wire is inserted from the tip of the toe into the metatarsal head, blocking the motion of the metatarsophalangeal joint and avoiding joint subluxation during lengthening. The osteotomy is then performed perpendicular to the metatarsal shaft, in between the middle two wires and screws.
Conclusion
The surgical technique for gradual lengthening of the metatarsal using the Orthofix MiniRail System was described in detail with accompanying step-by-step intraoperative clinical and fluoroscopic images.
Clinical significance
This surgical technique of metatarsal lengthening is simple and effective. An understanding of the surgical technique of gradual lengthening of the metatarsal bone is important when treating shorting deformities of more than 1 cm.
How to cite this article
Marwan Y, Abu Dalu K, Bernstein M, et al. Metatarsal Gradual Lengthening for Brachymetatarsia Using a Mini-rail External Fixator System. Strategies Trauma Limb Reconstr 2022;17(3):184–188.
Keywords: Brachymetatarsia, Brachymetapody, Deformity, External fixator, Foot, Lengthening, Metatarsal
Background
Brachymetatarsia refers to the shortening of the metatarsal bone.1,2 When the condition involves more than one metatarsal bone, it is referred to as brachymetapody.2 The fourth and first metatarsals are the most involved.1–3 Females are more commonly affected by this condition.1–3
Brachymetatarsia can be congenital or acquired.2,4,5 This deformity is associated with multiple conditions and syndromes, including trisomy 21, Apert syndrome, sickle cell anaemia, Albright's osteodystrophy and dystrophic dwarfism.2,4,5
Surgical treatment for brachymetatarsia is indicated for various reasons.2,3 In most patients, the deformity is painless, and metatarsal lengthening is done for aesthetic reasons.2,3 In addition, restoring the metatarsal–phalangeal cascade improves the biomechanics of the foot by preventing abnormal loading on the metatarsal heads with stance and gait, preventing metatarsalgia.2–6
We describe the surgical technique for gradual lengthening of the metatarsal using the Orthofix MiniRail System (Orthofix Medical Inc, Lewisville, TX, USA). We provide a step-by-step description of the technique using clinical and radiographic images and include the perioperative assessment and care of patients undergoing this procedure.
Technique
Preoperative Evaluation
Preoperative weight-bearing X-rays of the foot should be obtained for surgical planning. The anteroposterior view is used to measure the metatarsal parabola to determine the desired lengthening distance (Fig. 1). The normal parabola angle between the metatarsal heads is 142.5°. The desired lengthening distance is measured from the current location of the metatarsal head to the line forming the normal parabola angle as demonstrated in Figure 1. For lengthening of more than 1–1.5 cm, it is advised to avoid acute lengthening to avert neurovascular and bone non-union complications.3,7,8
Fig. 1.

Preoperative clinical and weight-bearing X-ray images of a case of left third brachymetatarsia. The X-ray showing the metatarsal heads parabola angle (green) and the length of shortening of the third metatarsal (16 mm)
The surgeon should have a prior understanding of the fixator for this procedure to ensure its suitability for use. The distance between the most proximal and the most distal pins or wires in the fixator should be known. The metatarsal length should be measured to make sure it can accommodate the fixator pins without having pins in the metatarsal head.
Surgical Technique
The patient is positioned supine on a radiolucent table and the C-shaped arm is placed on the contralateral side of the limb that is operated on. Tourniquet use is optional. Before incising the skin, the short metatarsal is located under fluoroscopic guidance (Fig. 2). The skin incision is made dorsally over the short metatarsal and this is followed by soft tissue dissection to identify the toe extensor tendons and protect the digital neurovascular bundle (Fig. 3). Once the bone is exposed, a haemostat is used to hold it and fluoroscopy used to confirm that the exposed bone is the abnormal one (Fig. 4). The surgery can also be performed using a percutaneous technique; however, the open technique is preferred by the senior author (RCH) to avoid complications when inserting the wires or screws and when performing the osteotomy since the metatarsal is very small in addition to being short. The diameter and length of the wires or screws depend on the size of the bone; this should be assessed intraoperatively. The diameter of the implant used should not exceed 30–40% of the bone diameter at the site of insertion to ensure stability and avoid fractures during lengthening. The most proximal wire or screw is inserted first (Fig. 5). Before inserting the first wire or screw, it is critical to reconfirm, based on the location of the most proximal wire or screw, that the most distal wire or screw will be proximal to the metatarsal head (wire or screw in the metatarsal head is usually painful and intra-articular). This can be done by fluoroscopic imaging with the fixator overlying the bone before inserting any wire or screw (Fig. 6). In severe cases with a very short metatarsal, the most proximal wire or screw can be placed in the tarsal bone to allow proper application of the fixator and give room for a metaphyseal location of the osteotomy. The most distal wire or screw should be inserted next, followed by the middle wires or screws (Fig. 7). All wires or screws should be placed perpendicular to the anatomic axis of the bone to enable distraction in the correct direction and avoid translation or angulation; placing the wires or screws parallel to the floor should be considered in longer lengthening to avoid plantar flexion deformity (especially in the first metatarsal). Once the MiniRail lengthener is assembled, a 1.6-mm K-wire is inserted from the tip of the toe to the metatarsal head, blocking the motion of the metatarsophalangeal joint to avoid joint subluxation during lengthening (Fig. 8). The osteotomy is then performed perpendicular to the metatarsal shaft, between the second and third wires or screws, using a small diameter oscillating saw based on the size of the bone (Fig. 9). The osteotomy can also be performed using multiple drill holes and osteotome. Distraction should be confirmed; however, compression of the segments should be done before closure (Fig. 10). The incision is then irrigated thoroughly, and the wound is closed.
Fig. 2.

Planning the surgical incision using fluoroscopy
Figs 3A and B.

Exposure of the third metatarsal bone while protecting the extensor tendons and the digital neurovascular bundle
Fig. 4.

Confirming that the exposed metatarsal is the correct one
Figs 5A and B.

Inserting the most proximal pin
Fig. 6.

Confirming that all the pins will be in a proper location in the metatarsal bone, specially that the most distal pin is proximal to the metatarsal head
Fig. 7.

Inserting all pins and attaching the fixator lengthening rail
Fig. 8.

The K-wire placed to stabilise the metatarsophalangeal joint
Fig. 9.

Osteotomy between the second and third pin
Fig. 10.
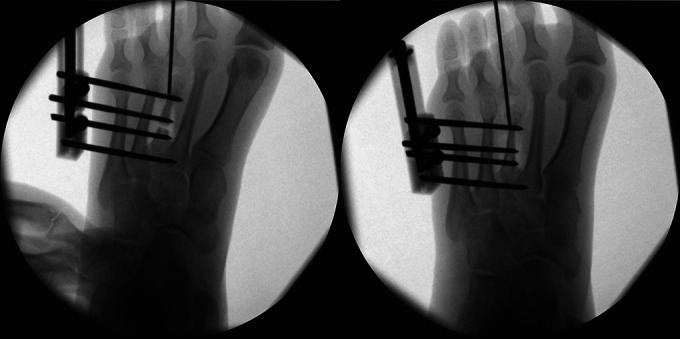
Distraction (left) and compression (right) to confirm the osteotomy is complete and the fixator is functioning well before closing the incision
Postoperative Protocol
Postoperatively, the foot is placed in a surgical shoe and weight bearing is not allowed. Distraction should start 7–10 days after the surgery. Distraction should be slow at a rate of 0.5–1 mm per day (i.e., one-quarter turn clockwise two to 4 times per day). The distraction of no more than 40% of the bone length is recommended to avoid complications.6–8 During the distraction phase (approximately the first 3–4 weeks postoperatively), the patient requires close monitoring on a weekly basis with X-rays to monitor the regenerate formation and the metatarsophalangeal joint alignment. Once the desired length is achieved, the K-wire should be removed and passive and active motion of the metatarsophalangeal joint should be done regularly. Moreover, X-rays should be obtained monthly until full consolidation of the regenerate is reached. The fixator is then removed and a gradual return to full weight bearing should start.
Discussion
Several surgical options are available to treat brachymetatarsia. The gradual lengthening of the metatarsal using an external fixation system was described in this article. This technique is simple and safe but an understanding of the principles of distraction osteogenesis is necessary before attempting to use this technique of metatarsal lengthening.
Metatarsal lengthening can be done acutely or gradually.3,7,8 Acute correction can be either through a lengthening-type osteotomy or lengthening with interposition of the bone graft.3,7–11 Such techniques are, however, limited to lengthening of 1.5 cm due to the risk of neurovascular compromise which could affect the viability of the toe.3,7–10 In addition, soft tissue tension and metatarsophalangeal joint dislocation are concerns with acute lengthening.3,7,8 In order to avoid such complications with acute lengthening, some surgeons have advocated performing shortening of the adjacent bones to minimise the lengthening distance needed to achieve the targeted parabola.7,8 The gradual lengthening of the metatarsal bone can also be done to avoid such complications.3,6–8 Nevertheless, rigidity, joint subluxation, pin site infection, poor bone formation and malalignment are possible complications with this technique.3,6–8 The rate of such complications can be minimised by lengthening no more than 40% of the metatarsal length.6,8,12,13
Osteotomy for metatarsal lengthening can be performed percutaneously or open and with high-energy (oscillating saw) or low-energy (multiple drills or wire holes and with an osteotome) techniques.2,3,13–16 While the open technique helps in performing a safe osteotomy by providing excellent exposure to the deformed and small bone, the percutaneous approach preserves the soft tissue envelope around the bone leading to a better biologic environment for the regenerate formation and consolidation.13–16 Moreover, the low-energy osteotomy provides a biological advantage by producing less heat at the osteotomy site; however, the use of an osteotome in such a small bone may lead to an extension of the osteotomy into the wire or screw site causing instability of the construct and hardware failure. Currently, the literature lacks high-level studies comparing different surgical approaches and osteotomy techniques for metatarsal lengthening.
Clinical Significance
The surgical technique for gradual lengthening of brachymetatarsia using the Orthofix MiniRail System (Orthofix Medical Inc, Lewisville, TX, USA) has been described in detail. This technique is relatively simple to perform using the external fixator system. Understanding the preoperative evaluation and postoperative management is critical in addition to knowing the surgical technique.
Orcid
Yousef Marwan https://orcid.org/0000-0001-5450-523X
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Urano Y, Kobayashi A. Bone lengthening for shortness of the fourth toe. J Bone Joint Surg Am. 1978;60(1):91–93. 624764 [PubMed] [Google Scholar]
- 2.Fusini F, Alessandro M, Rava A, et al. Aetiology, diagnosis, and treatment of brachymetatarsia: A narrative review. Musculoskelet Surg. 2022;106(2):99–109. doi: 10.1007/s12306-021-00720-z. [DOI] [PubMed] [Google Scholar]
- 3.Klauser HO. The surgical treatment of brachymetatarsia. Foot Ankle Clin. 2021;26(4):685–704. doi: 10.1016/j.fcl.2021.07.003. [DOI] [PubMed] [Google Scholar]
- 4.Robinson JF, Ouzounian TJ. Brachymetatarsia: Congenitally short third and fourth metatarsals treated by distraction lengthening. A case report and literature summary. Foot Ankle Int. 1998;19:713–718. doi: 10.1177/107110079801901012. [DOI] [PubMed] [Google Scholar]
- 5.Davidson RS. Metatarsal lengthening. Foot Ankle Clin. 2001;6(3):499–518. doi: 10.1016/s1083-7515(03)00110-4. [DOI] [PubMed] [Google Scholar]
- 6.Barbier D, Neretin A, Journeau P, et al. Gradual metatarsal lengthening by external fixation: A new classification of complications and a stable technique to minimize severe complications. Foot Ankle Int. 2015;36(11):1369–1377. doi: 10.1177/1071100715593373. [DOI] [PubMed] [Google Scholar]
- 7.Kim HT, Lee SH, Yoo CI, et al. The management of brachymetatarsia. J Bone Joint Surg Br. 2003;85(5):683–690. 12892191 [PubMed] [Google Scholar]
- 8.Shecaira AP, Fernandes RMP. Brachymetatarsia: One-stage versus two-stage procedures. Foot Ankle Clin. 2019;24(4):677–687. doi: 10.1016/j.fcl.2019.08.010. [DOI] [PubMed] [Google Scholar]
- 9.Giannini S, Faldini C, Pagkrati S, et al. One-stage metatarsal lengthening by allograft interposition: A novel approach for congenital brachymetatarsia. Clin Orthop Relat Res. 2010;468(7):1933–1942. doi: 10.1007/s11999-009-1212-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Desai A, Lidder S, Armitage AR, et al. Brachymetatarsia of the fourth metatarsal, lengthening scarf osteotomy with bone graft. Orthop Rev (Pavia) 2013;5(3):e21. doi: 10.4081/or.2013.e21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tabak B, Lefkowitz H, Steiner I. Metatarsal-slide lengthening without bone grafting. J Foot Surg. 1986;25(1):50–53. 3950333 [PubMed] [Google Scholar]
- 12.Shim JS, Park SJ. Treatment of brachymetatarsia by distraction osteogenesis. J Pediatr Orthop. 2006;26(2):250–254. doi: 10.1097/01.bpo.0000214922.18186.06. [DOI] [PubMed] [Google Scholar]
- 13.Fuiano M, Mosca M, Caravelli S, et al. Callus distraction with external fixator for the treatment of congenital brachymetatarsia of the fourth ray. Foot Ankle Surg. 2020;26(6):693–698. doi: 10.1016/j.fas.2019.08.018. [DOI] [PubMed] [Google Scholar]
- 14.Peña–Martínez VM, Palacios–Barajas D, Blanco–Rivera JC, et al. Results of external fixation and metatarsophalangeal joint fixation with K-wire in brachymetatarsia. Foot Ankle Int. 2018;39(8):942–948. doi: 10.1177/1071100718770388. [DOI] [PubMed] [Google Scholar]
- 15.Lamm BM. Percutaneous distraction osteogenesis for treatment of brachymetatarsia. J Foot Ankle Surg. 2010;49(2):197–204. doi: 10.1053/j.jfas.2009.09.005. [DOI] [PubMed] [Google Scholar]
- 16.Arata J, Kumakiri M, Yamashita T, et al. Nonincisional osteotomy for gradual lengthening by callus distraction for congenital brachymetatarsia. J Foot Ankle Surg. 2021;60(6):1293–1296. doi: 10.1053/j.jfas.2021.03.018. [DOI] [PubMed] [Google Scholar]