

Abstract
Introduction:
The Alaska Education and Research Towards Health (EARTH) Study assessed cancer risk among 3,821 Alaska Native people (AN). We present the prevalence of selected cancer risk factors and comparison with Healthy People 2010 goals.
Methods:
Participants completed extensive computer-assisted self-administered questionnaires on diet, physical activity, tobacco and alcohol use, cancer screening, family history of cancer, and environmental exposures. Measurement data were collected on blood pressure, height, weight, waist/hip circumference, fasting serum lipids and glucose.
Results:
Cancer risk factors are high for the Alaska EARTH study population. For all risk factors studied except for vegetable consumption, Alaska EARTH Study participants did not meet Healthy People 2010 goals.
Discussion:
This study is unique in providing questionnaire and measurement data of cancer risk factors on a larger study sample than any previous study among AN living in Alaska. Data show that the prevalence of most cancer risk factors exceeded national recommendations. Given the disease disparities that exist for the AN population, these data provide important baseline data that can be used to target health interventions and reduce health disparities.
INTRODUCTION
The profile of diseases contributing most heavily to morbidity and mortality in the United States has changed dramatically during the last century. Today, chronic diseases including cancer are among the leading causes of death and disability. They account for 75% of direct health care expenditures in the United States [1]. Many cancers are preventable or can be detected early and cured. Some common modifiable risk factors for cancer include: tobacco use and exposure to secondhand smoke; unhealthy diet, physical inactivity, obesity, and failure to undergo recommended cancer screening tests [2].
Alaska Native (AN) people are defined as indigenous persons whose ancestors, prior to European contact, occupied land that is now the state of Alaska. They are a heterogeneous population with over 200 federally recognized tribes reside widely dispersed across the state in numerous small, rural isolated communities. There is one large urban community in Anchorage and a few smaller cities. Similar to American Indian (AI) people in the contiguous United States, AN people are eligible for health care benefits provided by tribal organizations under compact with the Indian Health Service.
Compared to the US White population, AN people experience substantial disparities in morbidity and mortality. The overall mortality rate for 2004–2007 was 1.4 times that of US Whites and 1.5 times that of Alaska Whites [3, 4]. Mortality rates for cancer, cerebrovascular disease, chronic obstructive pulmonary diseases, and chronic liver disease exceed those of US Whites [3]. In contrast to the US White population, cancer rather than heart disease is the leading cause of AN death. For many diseases, and specifically cancer, AN mortality rates are higher than in other racial/ethnic minority populations in the US except African Americans [5].
In the 1950s cancer ranked low among causes of death among AN people. Cancer mortality has increased in the last fifty years and is now the leading cause of death among AN people. Incidence data from the Surveillance Epidemiology and End Results (SEER) Alaska Native Tumor Registry show that overall cancer incidence is now as high as US Whites, although the patterns of cancer differ. AN site-specific cancer incidence rates differ from those of other populations and rank among the highest especially for lung, colorectal, stomach, and gallbladder. Compared to AI people in the contiguous US, AN cancer incidence rates are higher than all but AI in the Northern Plains [6–8].
Data for AI, and AN people in particular, are scarce. If included at all in national health surveys, the numbers are usually too small to draw meaningful conclusions about health status. Aggregated data for all American Indian and Alaska Native people (AI/AN) are not representative of differences between specific geographic or ethnic populations.
The Alaska Education and Research Towards Health (EARTH) study targeted multiple chronic diseases among AN and collected baseline data on nearly 4000 AN residents of Alaska to evaluate the impact of lifestyle and clinical risk factors on the development of chronic diseases. This is the largest study of risk factors for chronic disease among this population undertaken to date. The focus for this report is on risk factors for cancer. To quantify disparities, findings from Alaska EARTH study participants are compared to both Healthy People 2010 goals and data from the Alaska Behavioral Risk Factor Surveillance System (BRFSS) [9, 10].
METHODS
Study population
The methods of the EARTH study have been described in detail elsewhere [11–13]. Only data from the Alaska component of the EARTH study are included in this analysis. Alaska Native participants came from multiple ethnic groups residing in three regions of the state: the southwest (Yukon-Kuskokwim Delta), southeast (Panhandle) and south central (Anchorage area). Eligibility criteria included the following: age ≥18 years; AI/AN eligible for health care through the Indian Health Service; and able to read, understand and sign written consent with the ability to complete study questionnaires and clinical measurements. The study was approved by the Alaska Area and the Indian Health Service IRBs, research and ethics review committees and Boards of Directors of each participating tribal health organizations, and Tribal Councils of each participating community.
An open recruitment method was used. Study staff gave presentations at formal and informal community gatherings, distributed posters and brochures at local health clinics, and posted advertisements/announcements in local newspapers, radio and television. In smaller communities, the study office was set up in available locations within each community, (e.g. tribal health clinics, community centers, and tribal council offices). EARTH research teams resided in the community for up to two months. In two larger communities, permanent offices were established for the duration of the enrollment period.
The baseline study visit consisted of the following: A written informed consent; intake questionnaire for demographic information; medical measurement; diet history and health, lifestyle and physical activity questionnaires; and an exit interview. Each participant received their own report (health risk appraisal) at the conclusion of the study visit. Medical measurements included seated blood pressure, height, weight, waist and hip circumference, and fasting blood glucose and lipid panel [14]. Blood was obtained by finger stick and tested using the Cholestech LDX (Cholestech, Hayward, California). Participants completed self-administered questionnaires after receiving instructions in the use of touch screen panels and head phones. Questions were presented in writing on the screens accompanied by an audio version of the questionnaire, in English or Yupik language.
RESULTS
This report summarizes data collected from 3,821 AN participants enrolled from March 2004 through August 2006 in 26 communities in Alaska. Table 1 describes selected sociodemographic characteristics of the Alaska EARTH study participants. There were more female than male participants (61% vs. 39%). A large proportion of participants had a high school education or higher (77%), were not currently married (57%) and were not employed (55%). Sixty–seven percent of participants reported speaking only English in their home while 8% spoke their Native language only. Participants were 62% Eskimo (Yupik, Siberian Yupik, Cupik or Inupiaq), 29% Southeast Alaska Indian (Tlingit, Haida, Tsimshian), and 10% Athabascan. Only 5% reported that they were descendants of an AI tribe in the contiguous United States.
Table 1.
Characteristics of Alaska Native participants in the EARTH Study, 2004–2006, compared to US Census, 2000
| Characteristic | EARTH Study N (%) |
Censusa N (%) |
|---|---|---|
| Total | 3,822 (100) | 119,331 (100) |
| Region b | ||
| Southcentral | 1,394 (36.5) | 36,428 (30.5) |
| Southeast | 887 (23.2) | 15,079 (12.6) |
| Southwest | 1,541 (40.3) | 20,226 (16.9) |
| Age, y c | ||
| 18–39 | 1,874 (49.0) | 37,235 (52.4) |
| 40–59 | 1,517 (39.7) | 24,816 (35.0) |
| ≥60 | 431 (11.3) | 8,913 (12.6) |
| Sex c | ||
| Men | 1,502 (39.3) | 60,212 (50.5) |
| Women | 2,320 (60.7) | 59,119 (49.5) |
| Marital status d | ||
| Married/living as married | 1,630 (42.8) | 30,705 (39.0) |
| Separated/divorced/never married | 2,177 (57.2) | 48,118 (61.0) |
| Education c | ||
| High school diploma or more | 2,933 (76.7) | 43,469 (74.0) |
| Employment status e | ||
| Employed or self-employed | 1,717 (44.9) | 45,734 (60.0) |
| Annual household income, $ f | ||
| ≤15,000 | 1,343 (41.2) | 6,536 (20.4) |
| 15,001–25,000 | 526 (16.1) | 5,178 (16.1) |
| 25,001–35,000 | 446 (13.7) | 4,403 (13.7) |
| 35,001–50,000 | 444 (13.6) | 5,074 (15.8) |
| ≥50,001 | 505 (15.4) | 10,904 (34.0) |
| Language spoken at home g | ||
| Non-English or both | 1,262 (33.2) | 31,130 (28.9) |
| English only | 2,542 (66.8) | 76,435 (71.1) |
| Ethnicity h | ||
| Eskimo | 2357 (61.8) | NA |
| Southeast Alaska Indian | 1089 (28.6) | NA |
| Athabaskan | 390 (10.2) | NA |
| Aleut | 323 (8.5) | NA |
| American Indian | 205 (5.4) | NA |
| Other Native (tribe unknown) | 285 (7.5) | NA |
Abbreviations: AI/AN, American Indian/Alaska Native; EARTH, Education and Research Towards Health; NA, not assessed.
Data set: Census 2000 American Indian and Alaska Native Summary File – Sample Data; Geographic Area: Alaska; Tribes alone or in any combination: American Indian and Alaska Native alone or in any combination. http://factfinder.census.gov/home/aian/index.html.
Census 2000 data for the corresponding Alaska Native Regional Corporations [ANRC]) Southcentral: Cook Inlet ANRC; Southeast: Sealaska ANRC; Southwest: Calista ANRC.
Census 2000 data for population aged 18 years or older.
Census 2000 data for population aged 15 years or older.
Census 2000 data for population aged 16 years or older.
Census 2000 data for households. EARTH data were missing 555 values for this variable.
Census 2000 data for population aged 5 years or older.
Percentages do not total 100 because participants could choose more than 1 ethnicity.
Figure 1 shows the prevalence of four major cancer risk factors among Alaska EARTH study participants compared with Healthy People 2010 (HP2010) goals. Current cigarette use among Alaska EARTH study participants was more than twice the prevalence of the HP2010 goal (32% vs. 12%) and current smokeless tobacco (ST) (both commercial and homemade) use was markedly higher: 18% vs. 0.4%. About a quarter (24%) of study respondents were former smokers or former ST users (18%) and likely to still be at risk for specific tobacco- related cancers.
Figure 1.
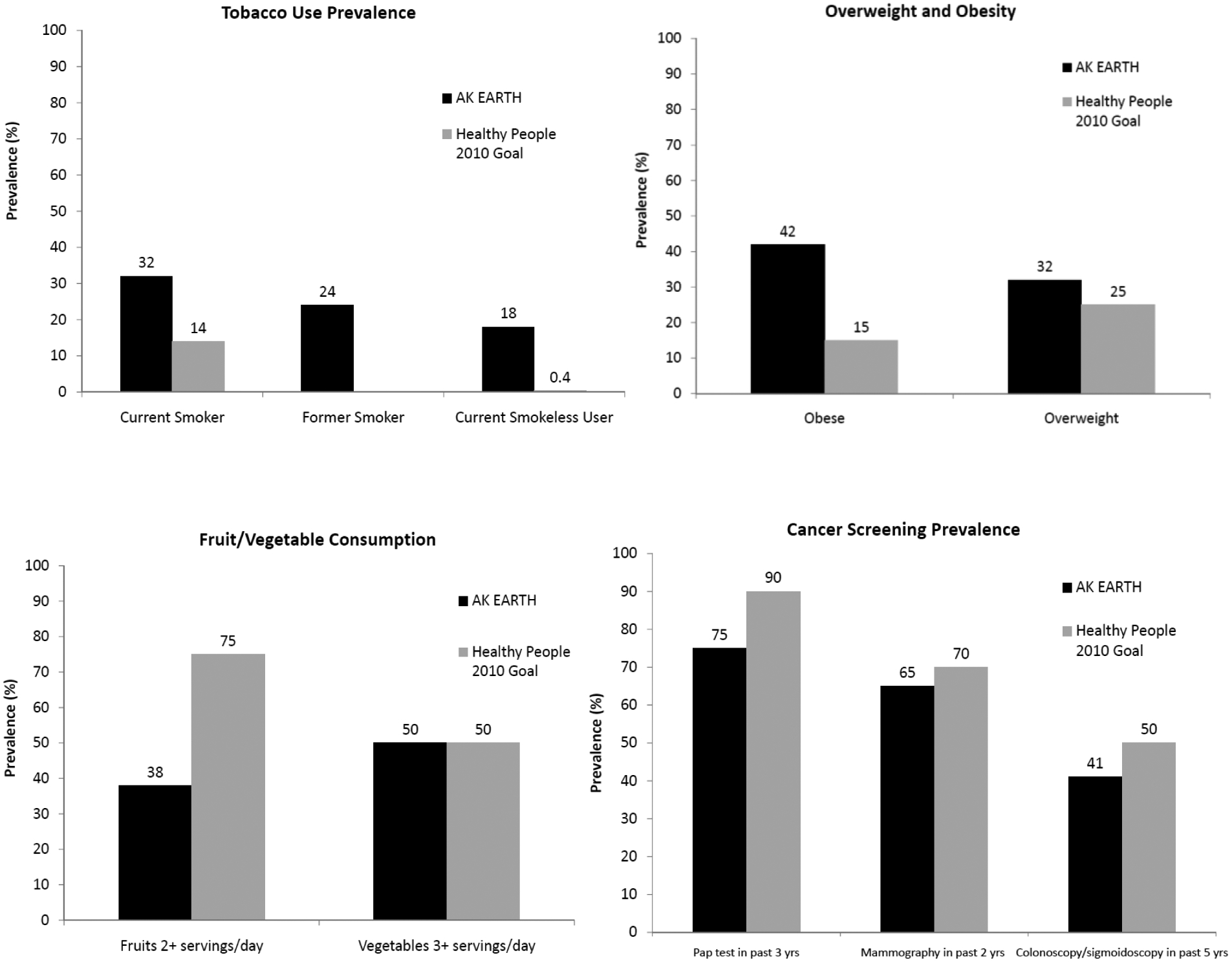
Selected cancer risk factors among Alaska Native participants in the EARTH Study, 2004–2006, compared to Healthy People 2010 Goals.
Overweight and obesity were likewise higher among Alaska EARTH study participants than HP2010 goals and national recommendations. Based on standard categorization of Body Mass Index (weight in kilograms divided by height in meters squared), 42% of participants met the definition of obesity (BMI 30.0 or greater), and 32% were overweight (BMI 25.0 to 29.9). The HP2010 goals for these measurements are 15% and 25% respectively. Only one quarter of the study population fell in the recommended range for healthy weight. Self-reported fruit consumption (2+ servings per day) was about half of HP2010 recommendations (38% vs. 75%). A larger percent of EARTH participants (50%) met the goal for vegetable consumption (3+ servings per day).
We queried participants regarding three evidence-based cancer screening tests: Pap test in the past 3 years and mammography in the past two years for women participants age 40 and older; and sigmoidoscopy/colonoscopy in last 5 years for both genders over age 50. Cancer screening rates among AN were lower than national HP2010 goals, specifically Pap test (75% vs. 90%), mammography (65% vs. 70%), and sigmoidoscopy/colonoscopy (41% vs. 50%).
AN people are concerned that increasing rates of cancer may be due to contaminants in their environment. At the request of the Alaska EARTH Study Tribal Advisory Board, exposure to nine specific environmental and occupational hazards were included in the EARTH study questionnaire. The hazards queried were asbestos, heavy metals, mineral or mining dust, pesticides, gasoline or other petroleum products (not including pumping own gas), radioactive materials including x-ray radiation, and silversmithing or welding. Many of these exposures have known carcinogenic effects [15]. Participants were to report exposures at work or their spare time as well as in or around their house or yard that occurred at least once a month for six months or more. Responses by gender are shown in Figure 2. Up to 20% of participants responded “don’t know” to various exposures. Among those who responded, more men than women reported exposure; the difference often being multifold. The highest exposure reported was for petroleum products (18%), for which 37% of men and 6% of women reported exposure. More than 5% of men reported exposure to all items queried, while the only item reported by more than 5% of women was petroleum products.
Figure 2.
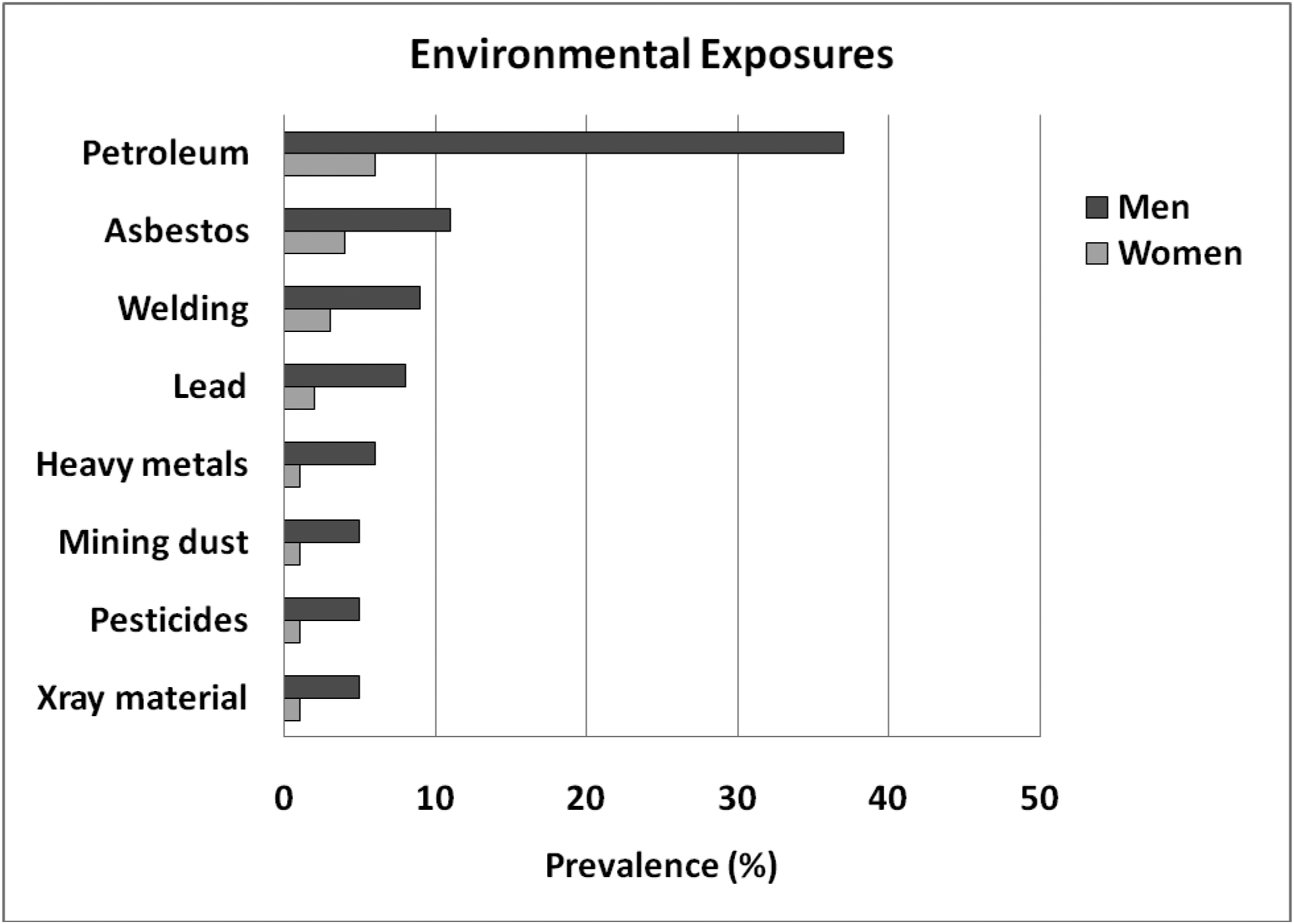
Environmental and occupational exposures among Alaska Native participants in the EARTH Study, 2004–2006.
Detailed findings for family history of multiple diseases and health-related conditions included in the EARTH study have been reported previously [16]. Here we review family history of cancers reported by Alaska EARTH study participants. Alaska EARTH study participants reported one or more first degree relative(s) diagnosed with the following cancers before age 50: colorectal (13%), breast (11%); prostate (6%), ovary (5%) and other cancers (24%).
DISCUSSION
This paper provides prevalence data on selected cancer risk factors from almost 4,000 AN people living in Alaska between 2004 and 2006. These findings document the large percentage of the population who do not meet HP2010 goals. Significant strengths of this study are the large numbers of AN participants; the collection of both clinical measurement and questionnaire data; and that the study targeted multiple chronic diseases and a wide range of risk factors - sociodemographic, lifestyle, and personal and family medical history.
This study has several limitations. First, analysis was a convenience sample based on self-selection in which more women agreed to participate than men. Because of this we report sex-specific data rather than both genders combined. Study participants appears to be representative of the AN population in each region. The sample proportions by age group, education levels, and marital status were similar to 2000 Census reports for AI/AN living in each region [17]. On the basis of the 2000 Census distribution, participation rates by community ranged from 2 to 49% of eligible adults; the median participation rate was 29%.
We examined several major risk factors associated with increased risk for cancer. Tobacco use accounts for an estimated 32% of all cancers [18]. Alaska Native EARTH study participants reported a higher smoking prevalence than the HP 2010 goal. Alaska BRFSS surveys indicate more AN people are current smokers (32% vs. 20%), and are current smokeless tobacco users (18% vs. 4%) than Alaska non-Natives. In addition, BRFSS data available in Alaska since 1991 demonstrate that the percent of current smokers and ST users among AN adults has not declined since 1991 and remains two-fold or greater than among Alaska non-Native people [4].
Unhealthy diet and physical inactivity are estimated to account for a third of all cancers [19]. While obesity was virtually non-existent in Alaska before European explorations [20], several studies have documented an increase in the prevalence of obesity among Alaska Native people. Studies in the 1960s-1980s of residents of Alaskan villages documented a steady increase in the percentage of the population >40 years weighing 13.6 kg above the Caucasian average for the same age, height, and gender [21]. The HP2010 goal for obesity is to reduce the proportion of adults >20 years of age who are obese to 15%. The rate of obesity among EARTH study men was more than twice the HP2010 goal and for women more than three times this rate [14, 22]. The prevalence of obesity among Alaska EARTH study participants exceeded the rate among Alaska non-Native BRFSS respondents (42% vs. 25%) [4].
The EARTH Study measured the proportion of participants who reported five hours or more per week of moderate and vigorous physical activity. Fewer women (35%) than men (61%) reported this level of activity. Alaska BRFSS data showed that 17% of AN men and women combined met the goal of moderate and vigorous activity as defined as moderate activity on 30 or more minutes per day on five or more days per week or vigorous physical activity for 20 minutes or more per day, for three or more days per week. This is in comparison with 27% of non-Native Alaska residents who met the goal.
Dietary factors such as regular consumption of fruits and vegetables are associated with reduced cancer risk. Alaska Native EARTH study men (62%) and women (63%) reported less consumption of fruits than the HP2010 goal of at least 2 daily servings. The HP2010 goal for vegetable intake is for at least three daily servings and in the EARTH survey, 55% of AN men and 48% of women did not meet that goal.
Cancer screening rates are low but show less disparities from the goals than for other risk factors. This is a result of increased efforts of the Alaska Tribal Health System and the State of Alaska to improve cancer screening, coupled with increased resources from the Centers for Disease Control and Prevention Breast and Cervical Cancer Early Detection Programs and Colorectal Cancer Control Programs.
Among EARTH study participants, 11 to 13% reported occurrences of colorectal and breast cancer in their first degree relatives. Close relatives of cancer patients are known to be at higher risk for cancer, especially breast, colorectal, prostate and ovarian cancer. The American Cancer Society estimates that breast cancer and colorectal cancer risk due to heredity factors is 5–10%. Whereas AN breast cancer incidence is currently similar to US whites, colorectal cancer incidence and mortality rates have been twice the incidence of US whites for more than 20 years, and may account for higher rates of first degree relatives with cancer reported here. Among AN people, the collection of family history of cancer can be used to identify individuals at higher risk who could benefit from early screening, particularly when resources and access to care are limited [24, 25].
There are no national data available to compare to the environmental and occupational exposures reported by EARTH participants. However, because of the large number of persons reporting exposure to petroleum products, these and other environmental exposure factors deserve further consideration.
In conclusion, we have documented high rates of cancer risk factors among the AN population that may partially explain the known excess burden of cancer. Although tobacco rates are falling in most US populations, there is no evidence for decline among AN adults. Rates of obesity in AN are increasing rapidly as are those in US adults, however, AN rates have been higher at least since the 1990s, and the disparity persists in more recent data [22]. The EARTH study and others have previously reported on the shift in AN diet from wild to store bought foods, and decreases in physical activity with availability of motorized vehicles [26–29]. These trends, along with the cancer risk factors documented in this study and the aging of the population, will continue to contribute to increases in cancer incidence. The vision of the Alaska Native Tribal Health Consortium is “Alaska Natives are the healthiest people in the world.” Steps are being taken to reduce disparities, but continued effort and resources will be needed to make this vision a reality.
Acknowledgements:
This study was funded by grants CA88958 and CA96095 from the National Cancer Institute and Y1PC403309 from the National Institute of Health, National Cancer Institute Surveillance Epidemiology and End Results (SEER) Program. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official view of the National Cancer Institute. We would like to acknowledge the contributions and support of the Indian Health Service, the Alaska Native Tribal Health Consortium Board of Directors, Southcentral Foundation, Southeast Alaska Regional Health Consortium, and the Yukon-Kuskokwim Health Corporation.
Footnotes
Conflict of Interest
The authors declare that they have no conflict of interest.
REFERENCES
- 1.National Center for Chronic Disease Prevention and Health Promotion. Chronic disease overview. www.cdc.gov/nccdphp/overview.htm. Accessed 10/4/2010.
- 2.Eyre H, Kahn R, Robertson RM, Clark NG, Doyle C, Hong Y, Gansler T et al. 2004. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Circulation 109 (25):3244–3255. doi: 10.1161/01.CIR.0000133321.00456.0001.CIR.0000133321.00456.00 [pii]. [DOI] [PubMed] [Google Scholar]
- 3.Day GE, Provost E, and Lanier AP. 2009. Alaska Native mortality rates and trends. Public Health Rep 124 (1):54–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Alaska Native Epidemiology Center. 2009. Alaska Native health status report. http://www.anthc.org/chs/epicenter/dd.cfm. Accessed October 7, 2010.
- 5.Health status of American Indians compared with other racial/ethnic minority populations--selected states, 2001–2002. 2003. MMWR Morb Mortal Wkly Rep 52 (47):1148–1152. doi:mm5247a3 [pii]. [PubMed] [Google Scholar]
- 6.Surveillance, Epidemiology, and End Results (SEER)*Stat Database: Mortality - All COD, Aggregated With State, Total U.S. (1990–2007) <Katrina/Rita Population Adjustment>. June 2010. National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch. www.seer.cancer.gov. [Google Scholar]
- 7.Perdue DG, Perkins C, Jackson-Thompson J, Coughlin SS, Ahmed F, Haverkamp DS, and Jim MA. 2008. Regional differences in colorectal cancer incidence, stage, and subsite among American Indians and Alaska Natives, 1999–2004. Cancer 113 (5 Suppl):1179–1190. doi: 10.1002/cncr.23726. [DOI] [PubMed] [Google Scholar]
- 8.Wiggins CL, Espey DK, Wingo PA, Kaur JS, Wilson RT, Swan J, Miller BA, Jim MA, Kelly JJ, and Lanier AP. 2008. Cancer among American Indians and Alaska Natives in the United States, 1999–2004. Cancer 113 (5 Suppl):1142–1152. doi: 10.1002/cncr.23734. [DOI] [PubMed] [Google Scholar]
- 9.U.S. Department of Health and Human Services. November 2000. Healthy People 2010, Chapter 3: Cancer. Washington, DC: U.S. Government Printing Office. [Google Scholar]
- 10.Alaska Department of Health and Social Services. 2005. Alaska Behavioral Risk Factor Surveillance System: Alaska Department of Health and Social Services.
- 11.Slattery ML, Schumacher MC, Lanier AP, Edwards S, Edwards R, Murtaugh MA, Sandidge J et al. 2007. A prospective cohort of American Indian and Alaska Native people: study design, methods, and implementation. American Journal of Epidemiology 166 (5):606–615. doi:kwm109 [pii] 10.1093/aje/kwm109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Slattery ML, Murtaugh MA, Schumacher MC, Johnson J, Edwards S, Edwards R, Benson J, Tom-Orme L, and Lanier AP. 2008. Development, implementation, and evaluation of a computerized self-administered diet history questionnaire for use in studies of American Indian and Alaskan native people. J Am Diet Assoc 108 (1):101–109. doi:S0002–8223(07)01929–3 [pii] 10.1016/j.jada.2007.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Edwards SL, Slattery ML, Murtaugh MA, Edwards RL, Bryner J, Pearson M, Rogers A, Edwards AM, and Tom-Orme L. 2007. Development and use of touch-screen audio computer-assisted self-interviewing in a study of American Indians. American Journal of Epidemiology 165 (11):1336–1342. doi:kwm019 [pii] 10.1093/aje/kwm019. [DOI] [PubMed] [Google Scholar]
- 14.Redwood DG, Lanier AP, Johnston JM, Asay ED, and Slattery ML. 2010. Chronic disease risk factors among Alaska Native and American Indian people, Alaska, 2004–2006. Prev Chronic Dis 7 (4):A85. doi:A85 [pii]. [PMC free article] [PubMed] [Google Scholar]
- 15.Rom WN, and Markowitz SB. 2006. Environmental and occupational medicine, 4th Edition. Lippincott Williams & Wilkins. [Google Scholar]
- 16.Slattery ML, Murtaugh MA, Lanier AP, Ma KN, Ferucci ED, Etzel RA, and Edwards S. 2009. Family health history and health behaviors in Alaska native and American Indian people. J Health Care Poor Underserved 20 (3):678–694. doi:S1548686909300078 [pii] 10.1353/hpu.0.0191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.US Census Bureau. 2000. Census 2000 American Indian Alaska Native Summary File. http://factfinder.census.gov. Accessed 4/28/06.
- 18.Harvard Report on Cancer Prevention. Volume 1: Causes of human cancer. 1996. Cancer Causes Control 7 Suppl 1:S3–59. [DOI] [PubMed] [Google Scholar]
- 19.Byers T, Nestle M, McTiernan A, Doyle C, Currie-Williams A, Gansler T, and Thun M. 2002. American Cancer Society guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 52 (2):92–119. [DOI] [PubMed] [Google Scholar]
- 20.Michael H 1967. Lieutenant Zagoskin’s Travels in Russian America, 1842–1844. Translation from Russian sources, No. 7. Toronto: University of Toronto Press. [Google Scholar]
- 21.Murphy NJ, Schraer CD, Bulkow LR, Boyko EJ, and Lanier AP. 1992. Diabetes mellitus in Alaskan Yup’ik Eskimos and Athabascan Indians after 25 yr. Diabetes Care 15 (10):1390–1392. [DOI] [PubMed] [Google Scholar]
- 22.Slattery ML, Ferucci ED, Murtaugh MA, Edwards S, Ma KN, Etzel RA, Tom-Orme L, and Lanier AP. 2010. Associations among body mass index, waist circumference, and health indicators in American Indian and Alaska Native adults. Am J Health Promot 24 (4):246–254. doi: 10.4278/ajhp.080528-QUAN-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Physical Activity Guidelines Advisory Committee report, 2008. To the Secretary of Health and Human Services. Part A: executive summary. 2009. Nutr Rev 67 (2):114–120. doi:NURE136 [pii] 10.1111/j.1753-4887.2008.00136.x. [DOI] [PubMed] [Google Scholar]
- 24.National Institute of Health Consensus Development Program. 2010. NIH State-of-the-Science Conference. In Enhancing use and quality of colorectal cancer screening. Bethesda, Maryland. [Google Scholar]
- 25.U.S. Preventive Services Task Force, Agency for Healthcare Research and Quality. 2002. Screening for colorectal cancer: recommendations and rationale. Rockville, MD. [Google Scholar]
- 26.Redwood DG, Ferucci ED, Schumacher MC, Johnson JS, Lanier AP, Helzer LJ, Tom-Orme L, Murtough MA, and Slattery ML. 2008. Traditional foods and physical activity patterns and associations with cultural factors in a diverse Alaska Native population. Int J Circumpolar Health 67 (4):335–348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bersamin A, Zidenberg-Cherr S, Stern JS, and Luick BR. 2007. Nutrient intakes are associated with adherence to a traditional diet among Yup’ik Eskimos living in remote Alaska Native communities: the CANHR Study. Int J Circumpolar Health 66 (1):62–70. [DOI] [PubMed] [Google Scholar]
- 28.Murphy NJ, Schraer CD, Theile MC, Boyko EJ, Bulkow LR, Doty BJ, and Lanier AP. 1997. Hypertension in Alaska Natives: association with overweight, glucose intolerance, diet and mechanized activity. Ethnicity & Health 2 (4):267–275. [DOI] [PubMed] [Google Scholar]
- 29.Johnson JS, Nobmann ED, Asay E, and Lanier AP. 2009. Dietary intake of Alaska Native people in two regions and implications for health: the Alaska Native Dietary and Subsistence Food Assessment Project. Int J Circumpolar Health 68 (2):109–122. [DOI] [PubMed] [Google Scholar]