

Abstract
Objectives:
Examine growth and maturation trends in dynamic balance using the anterior reach Y-Balance test, and its utility as an injury risk screening tool.
Design:
Cross sectional and prospective cohort.
Setting:
Elite male youth soccer players.
Participants:
346 players grouped as pre, circa or post peak height velocity (PHV).
Main outcome measures:
Pre-season anterior reach absolute and relative Y-Balance test scores and seasonal prospective lower extremity injury monitoring.
Results:
Absolute reach distances were greatest post-PHV (p < 0.05). Relative to leg length, pre-PHV achieved the highest scores and increased between-limb differences. Significant associations between injury and anterior reach scores were present in pre (OR: 0.94, CI: 0.91–0.98, p < 0.05) and circa-PHV (OR: 1.05, 95% CI: 1.05–1.10, p < 0.05). Increased age (OR: 1.49, 95% CI: 1.04–2.13, p < 0.05) and height (OR: 1.06, 95% CI: 0.99–1.13, p = 0.82) were risk factors post-PHV. No differences in injury occurrence were shown between players with absolute reach difference >4 cm in any group.
Conclusions:
Anterior reach scores increased injury risk, but associations were small and inconsistent. The Y-Balance should be used with caution as a screening tool in this cohort.
Keywords: Balance, Asymmetry, Maturation, Injury
1. Introduction
Injury rates increase linearly with age in male youth soccer players (Price et al., 2004), while heightened risk may also be present during periods associated with accelerated growth (Read, Oliver, De Ste Croix, Myer, & Lloyd, 2017a, 2017b; van der Sluis et al., 2014). Research has shown an increase in overall season incidence (1.56 vs. 1.32 injuries per player) and severe injury (0.42) rate for players during developmental stages corresponding to peak height velocity (PHV) (Read et al., 2017a, 2017b), defined as the period in which a child experiences their fastest upward growth in stature (Mirwald et al., 2002). In addition, these athletes experienced the longest time-loss per injury (~26 days) (Read et al., 2017a, 2017b). Rapid changes in stature and mass can result in aberrant movement patterns and momentary disruptions in motor control (Atkins et al., 2016; Philippaerts et al., 2006). However, analysis of injury risk factors in elite male youth soccer players is sparse (Read et al., 2016, 2018c), despite the frequency of injuries (Le Gall et al., 2006; Price et al., 2004).
Non-contact injuries occur most frequently in male youth soccer players, with the knee and ankle most susceptible (Read et al., 2017a, 2017b). A range of assessments are available to examine lower-limb performance and movement control in male youth soccer players (Read et al., 2019); however, these tests often demonstrate poor sensitivity for the identification of individuals at elevated risk of injury (Hegedus, McDonough, Bleakley, Cook, & Baxter, 1136; Hegedus et al., 2015). Reduced dynamic balance scores have been associated with lower extremity injuries, most frequently occurring at the knee and ankle (Plisky et al., 2006). Specifically, the sum of three out of eight reach directions in the star excursion balance test (anterior, posteromedial, and posterolateral) and asymmetrical anterior reach distances have shown associations with injury in male youth athletes (Hegedus et al., 2015; Plisky et al., 2006). Thus, a modified version of the original star excursion balance test comprising only these three reach directions has been developed, the Y-Balance test (Faigenbaum et al., 2014; Plisky et al., 2009). One available study in recreational school children reported the reliability of this method showing moderate to strong test re-test correlations (ICC range = 0.71–0.88) (Faigenbaum et al., 2014); however, these were not elite youth athletes who participate regularly in sport-specific training and competition.
The Y-Balance test has been suggested to measure dynamic balance due to the need to maintain the position of the body’s centre of mass during dynamic actions (Plisky et al., 2009). Improving dynamic balance through training has reduced the risk of knee and ankle sprains in youth soccer (Malliou et al., 2004; McGuineTAKeene, 2006) and ankle injuries in basketball players (McGuineTAKeene, 2006). When assessing and characterising balance abilities of non-injured soccer players, youth display greater postural sway than adults (Pau et al., 2014, 2015); however, only adolescents were included in the youth sample which does not account for changes seen due to growth and maturation. Variation in performance tests such as jumping and hopping are evident across different chronological age groups (Lloyd et al., 2012; Philippaerts et al., 2006; Read et al., 2017b, 2018a, 2018b, 2018d), indicating performance may be affected by the stage of maturation. There is a paucity of research to examine dynamic balance in male youth soccer players at different stages of their growth and development.
When a large number of players must be screened and there are obvious time constraints, the inclusion of multiple movement screens may not be possible. Of those available, the Y-Balance test, and in particular the anterior reach direction may, be considered important given its association with injury risk (Plisky et al., 2006; Smith et al., 2015). In male youth basketball players, an anterior right-left reach difference >4 cm displayed a 2.5 times greater risk of lower extremity injury (Plisky et al., 2006). Currently there is a lack of research to examine dynamic balance and y-balance anterior reach right-left differences in elite male youth soccer players at different maturity stages. These data are required to identify sensitive periods during a player’s development and can assist in the design of targeted interventions for injury risk reduction. Prospective cohort studies are also warranted to examine the clinical utility of the Y-Balance anterior reach test in this cohort to establish if similar between-limb differences are associated with heightened risk of injury.
This study was separated into two experiments and had two aims: 1) to screen elite male youth soccer players from a range of maturity groups and identify cross-sectional trends in dynamic balance using the Y-Balance test; and 2) to investigate the clinical utility of the Y-Balance test to identify associations with future injury.
2. Methods
2.1. Experimental design
2.1.1. Experiment 1: Reliability and cross-sectional analysis of anterior reach Y-Balance test by maturity status
Initially the test-retest reliability of the anterior reach Y-Balance test was examined using a repeated measures design in a subsample of 50 participants, including 25 pre-peak height velocity (PHV) (age 11.9 ± 0.4 years; height 151.4 ± 4.8 cm; body mass 41.1 ± 5.6 kg; maturity offset −2.3 ± 0.4 years) and 25 post-PHV players (age 17.3 ± 0.7 years; height 178.2 ± 5.5 cm; body mass 72.3 ± 6.9 kg; maturity offset 2.9 ± 0.8 years). Participants were required to attend their respective club’s training ground at the same time (pm) on three occasions separated by a period of seven days. The first occasion was used for familiarization prior to data collection in the second and third sessions. All procedures were replicated at each test session and the data were collected by the same individual.
A cross-sectional design was used to examine the effects of stage of maturation on anterior reach Y-Balance performance. 346 players from six clubs attended their respective club training grounds on two occasions, familiarization and testing, separated by a period of seven days. All testing occurred in pre-season (July) spread across a two-week period to ensure all players from the different clubs could be tested. Descriptive statistics are provided for each group in Table 1. All tests were conducted by the same researcher and a 10-min standardized warm up was completed prior to each session. Participants were asked to refrain from strenuous exercise at least 48 h prior to testing and avoid eating and drinking substances other than water 1 h prior to each test session.
Table 1.
Mean ± SD values for participant characteristics for each maturation group.
| Maturation group | N | Age (years) | Body mass (kg) | BMI | Stature (cm) | Leg length (cm) | Maturity offset |
|---|---|---|---|---|---|---|---|
| Pre PHV | 134 | 11.9 ± 1.1 | 39.7 ± 6.4 | 18.1 ± 2.1 | 148.2 ± 7.5 | 74.6 ± 3.5 | −2.2 ± 0.6 |
| Circa PHV | 83 | 14.4 ± 0.9 | 51.8 ± 6.7 | 19.2 ± 1.6 | 164.8 ± 7.6 | 82.3 ± 3.6 | 0.0 ± 0.3 |
| Post PHV | 129 | 16.1 ± 1.1 | 66.8 ± 8.0 | 21.5 ± 1.7 | 176.6 ± 6.7 | 88.6 ± 4.7 | 2.0 ± 0.8 |
PHV = peak height velocity; BMI = Body mass index.
2.1.2. Experiment 2: Prospective study examining associations between anterior reach Y-Balance test with future injury occurrence
Following baseline Y-Balance anterior reach injury risk screening occurring during pre-season (July), these players were then tracked for the remainder of the season to prospectively record all injuries sustained in soccer training and competitions at their respective clubs.
2.2. Participants
Elite male youth soccer players from the academies of professional soccer clubs volunteered to take part. None of the players reported injuries at the time of baseline screening and all were participating regularly in soccer training and competitions. The included sample were most frequently (78%) right limb dominant as defined by their preferred kicking limb. Parental consent and participant assent were collected prior to the commencement of testing. Ethical approval was granted by the institutional ethics committee in accordance with the declaration of Helsinki.
2.3. Procedures
2.3.1. Anthropometry
Body mass (kg) was measured on a calibrated physician scale (Seca 786 Culta, Milan, Italy). Standing and sitting height (cm) were recorded on a measurement platform (Seca 274, Milan, Italy). Leg length was also measured to the nearest 0.1 cm as the distance between the anterior superior iliac spine and the medial malleolus using a standard tape measure. Stage of biological maturation was assessed using a previously validated regression equation comprising measures of age, body mass, standing height and sitting height (Mirwald et al., 2002). Using this method, maturity offset (calculation of years from PHV) was completed using the following equation:
2.3.2. Anterior reach Y-Balance test
Participants placed their hands on their hips and began in a unilateral stance with the most distal aspect of their great toe behind the line on the centre of the Y-Balance test kit™ (Move2-Perform, Evansville, IN). The commercially available device is comprised of a central stance platform with three pieces of polyvinylchloride piping attached displaying incremental measurements of 0.5 cm complete with a reach indicator for each pipe. Distances were recorded by pushing the target reach indicator in the anterior direction only due to the heightened associations with injury of this specified direction for youth athletes (Plisky et al., 2006; Smith et al., 2015).
Four practice trials were provided to reduce learning effects as previously stated (Munro & Herrington, 2010), with technical competency observed by the principle investigator defined as meeting all the previously stated test requirements (Plisky et al., 2009). Due to the large subject numbers and to ensure time-efficiency in an elite sports setting, three of the specified practice trials were performed in a group setting away from the instrumented device in accordance with previous research (Faigenbaum et al., 2014), with an additional practice trial conducted on the Y-Balance kit. Tests were performed on both legs with the order randomized to eliminate an order effect. Throughout, no visible kicking of the target reach indicator was permitted, the heel of the non-reach leg was required to remain on the testing platform with the toe behind the start line, balance was to be maintained in a single leg stance, and the reach foot was required to return back to the platform (Riach & Stark, 1994). Maximal reach distances were recorded and normalized to leg length. Absolute anterior reach difference scores between limbs were also recorded (right minus left). Three trials were performed on each leg with the mean score reported.
2.3.3. Injury reporting
Non-contact, lower extremity injuries were diagnosed, classified and prospectively recorded by respective medical personnel at each club for the duration of an entire soccer season (July–May inclusive) in accordance with methods outlined previously and the regulations set out by the competitive league organizers (Read et al., 2017a, 2017b). Injuries were documented if they occurred during soccer-related activities and if the player was subsequently unable to participate in training or competition for a minimum of 48 h following the incident, not including the day of injury. Players were classified as injured until the medical staff (chartered physiotherapists) of their respective clubs deemed they were fit to resume full training. Due to the confounding effects of previous injuries, only the first incident experienced by each player during the season was used in the subsequent analysis.
2.4. Statistical analysis
Within-subject variation was determined using typical error of estimates, 95% confidence intervals (95% CI) and mean coefficients of variation (CV %). All data were computed through Microsoft Excel® 2010 using a freely-available spread sheet to compute all reliability statistics (Hopkins, 2000). Players were grouped by their stage of maturation (pre-, circa- or post-PHV). To account for the reported error (approx. 6 months) in the regression equation used (Mirwald et al., 2002), players were grouped into discrete bands based on their maturational offset (pre -PHV = < −1, circa-PHV = −0.5 to 0.5, post-PHV = >1) in accordance with previous research (Read et al., 2017b, 2018a, 2018b). Players tested who recorded a maturational offset between −1 and −0.5 and 0.5 to 1 were subsequently removed from the data set.
To perform the cross sectional analysis, descriptive statistics were calculated for each maturity group (mean ± SD). A one-way analysis of variance was performed to determine the existence of any between group differences. The level of significance was set at alpha level p ≤ 0.05. Homogeneity of variance was tested by Levene’s statistic, and where violated Welch’s adjustment was used to calculate the F-ratio. Post-hoc analysis was assessed using Gabriel’s test when equal variance was assumed, and Games-Howell tests when this assumption was violated. Cohen’s d effect sizes (ES) were calculated to interpret the magnitude of between group differences using the following classifications: standardized mean differences of 0.2, 0.5, and 0.8 for small, medium, and large effect sizes, respectively. Paired samples t-tests were also used to examine differences in performance between limbs. One-way analysis of variance and paired samples t-tests were processed using SPSS® (V.21. Chicago Illinois).
The first step of the injury risk analysis involved completion of an independent samples t-test to examine mean differences in age, anthropometry, and Y-Balance performance among players who sustained an injury and those who were not injured during the study period. This step was adopted to reduce the number of outcome variables and the error degree of freedom. Variables that displayed a p-value < 0.1 were considered for further regression analysis. Odds ratios (OR) were then calculated using stepwise backwards multivariate binary logistic regression with 95% confidence intervals (CI). An alpha value of p < 0.05 was indicative of a significant association. Chi-squared (χ2) was used to compare association of injury status with a previously suggested injury threshold (>4 cm between limb anterior reach difference) (Plisky et al., 2006; Smith et al., 2015), with statistical significance set at an alpha level of p < 0.05. Logistic regression and Chi-squared tests were processed using SPSS® (V.21. Chicago Illinois).
3. Results
3.1. Experiment 1: Cross-sectional analysis
Reliability statistics are displayed in Table 2. Typical error between test-sessions and the CV% were consistent with those of previous research and were deemed acceptable (<10%) (Faigenbaum et al., 2014) in both pre and post-PHV players. Mean (±standard deviation) Y-Balance absolute anterior reach distances and distances normalized to leg length for each limb and maturity group are displayed in Fig. 1a and b respectively. Absolute reach distances were greatest in post-PHV players (right = 64.3 ± 12.3 cm; left = 63.3 ± 11.5), although these differences were only significant when compared to the pre-PHV group with moderate effect sizes (right = 58.0 ± 9.5 cm; left = 57.2 ± 9.6 cm) (p < 0.001; d = 0.57–0.58). Pre-PHV players recorded the greatest reach differences relative to leg length (right = 74.2 ± 12.7 cm; left = 73.1 ± 12.6), although significant differences were present only when compared to post-PHV players, corresponding to a small effect size (right = 69.9 ± 13.8 cm; left = 68.8 ± 12.8), (p < 0.05; d = 0.32–0.34) (Fig. 1b). No significant inter-limb reach differences were observed between pre (3.6 ± 2.8 cm), circa (3.2 ± 3.1 cm) and post-PHV (3.4 ± 2.8 cm) players. Significantly greater reach distances were shown on the right leg (p < 0.001).
Table 2.
Reliability statistics.
| Test Variable | Typical Error | CV% (95% CI) |
|---|---|---|
| Pre-PHV | ||
| Y-Balance Anterior (cm) | 4.8 | 7.1 (6.1–8.6) |
| Post-PHV | ||
| Y-Balance Anterior (cm) | 6.3 | 8.2 (7.0–9.9) |
Fig. 1a.
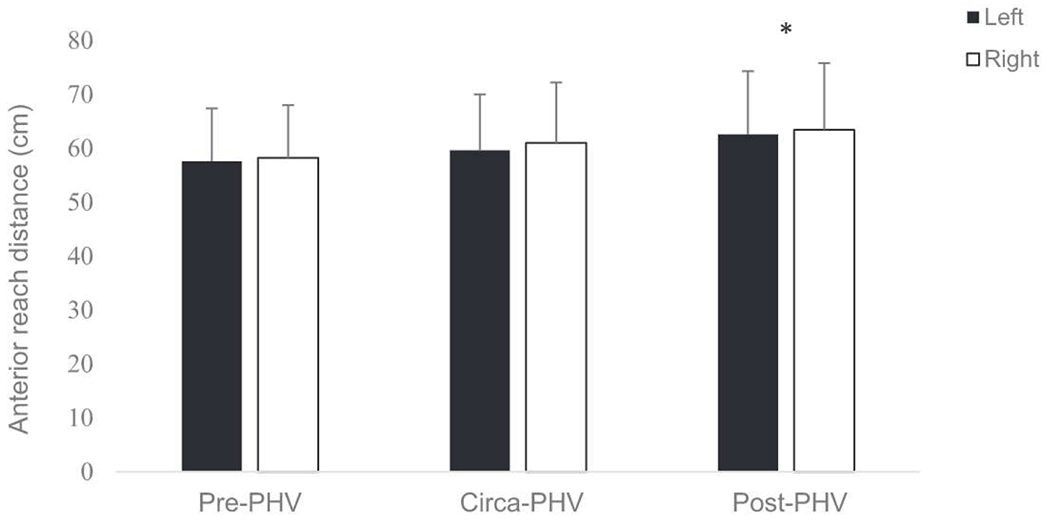
Absolute anterior reach scores for each maturity group. * significantly greater than pre-PHV p < 0.001.
Fig. 1b.
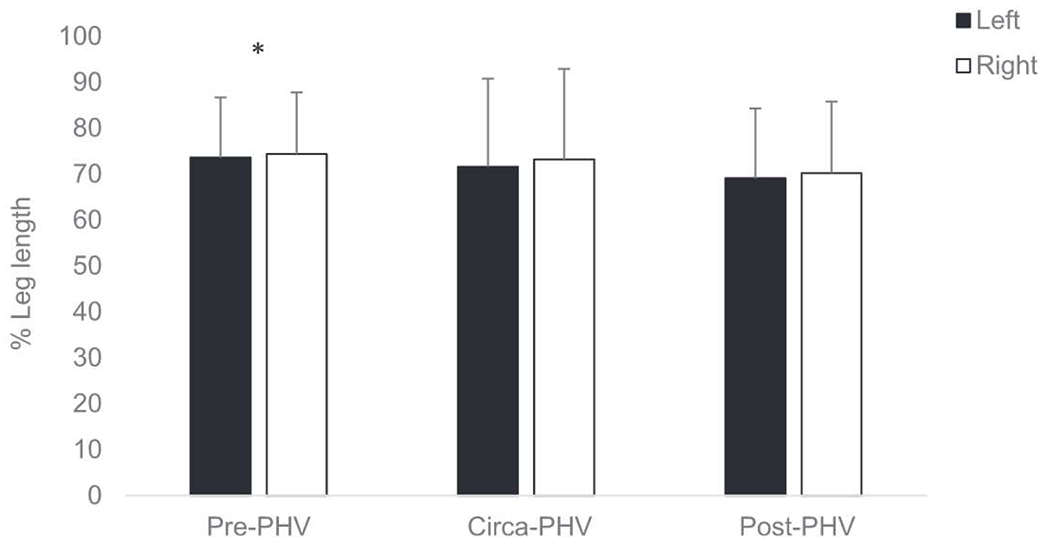
Anterior reach scores relative to leg length for each maturity group. * significantly greater than post-PHV p < 0.05.
3.2. Experiment 2: Injury analysis
Of the 346 players included, 99 sustained a non-contact lower extremity injury. The knee was the most frequently injured anatomical site (31%), followed by the ankle (19%). There were a high proportion of strain type injuries (32%), with ligament (19%) and growth/overuse (14%) the most prevalent diagnosis thereafter. Half of the injuries (50%) were moderate (1–4 weeks); however, severe injuries (>4 weeks absent) were also frequently reported (32%). Descriptive statistics for injured and non-injured players in each maturity group are displayed in Tables 3–5. The distribution of Y-Balance anterior reach absolute between-limb difference scores for injured and non-injured players in each maturity group is also shown in Fig. 2.
Table 3.
Descriptive characteristics of injured and non-injured pre-PHV players.
| Injured (n = 32) | Non-injured (n = 79) | p value | Cohens d | |
|---|---|---|---|---|
| Age (years) | 12.3 ± 0.9 | 11.9 ± 1.1 | .04* | 0.40 |
| Weight (kg) | 40.9 ± 6.9 | 39.7 ± 5.7 | .35 | 0.19 |
| Height (cm) | 149.8 ± 7.9 | 147.8 ± 7.3 | .19 | 0.26 |
| BMI | 18.1 ± 1.9 | 18.1 ± 2.3 | .91 | 0.01 |
| Maturational offset (years) | −2.01 ± 0.60 | −2.26 ± 0.67 | .07 | 0.39 |
| Leg length (cm) | 78.7 ± 5.2 | 78.5 ± 5.9 | .78 | 0.03 |
| y-balance Left (cm) | 53.0 ± 8.9 | 58.9 ± 9.4 | .003* | 0.64 |
| y-balance Right (cm) | 55.1 ± 9.1 | 59.3 ± 9.5 | .04* | 0.45 |
| y-balance (% of leg length) left | 67.3 ± 10.9 | 75.5 ± 12.6 | .002* | 0.69 |
| y-balance (% of leg length) right | 70.0 ± 11.6 | 75.9 ± 12.9 | .03* | 0.48 |
| Absolute reach difference (cm) | 3.8 ± 3.1 | 3.4 ± 2.8 | .54 | 0.13 |
indicates statistical significance.
Table 5.
Descriptive characteristics of injured and non-injured post-PHV players.
| Injured (n = 41) | Non-injured (n = 100) | p value | Cohens d | |
|---|---|---|---|---|
| Age (years) | 16.6 ± 1.1 | 16.0 ± 1.0 | .001* | 0.57 |
| Mass (kg) | 69.3 ± 7.2 | 66.1 ± 7.8 | .03* | 0.42 |
| Height (cm) | 178.1 ± 6.2 | 175.4 ± 6.2 | .02* | 0.44 |
| BMI | 21.8 ± 1.8 | 21.5 ± 1.7 | .28 | 0.17 |
| Maturational Offset (years) | 2.2 ± 0.8 | 1.9 ± 0.7 | .10 | 0.39 |
| Leg length | 92.8 ± 4.2 | 91.9 ± 4.9 | .28 | 0.19 |
| y-balance left | 65.8 ± 11.0 | 62.3 ± 11.7 | .09 | 0.31 |
| y-balance right | 67.0 ± 11.4 | 63.2 ± 12.5 | .08 | 0.32 |
| y-balance (% leg length) left | 70.6 ± 12.3 | 68.0 ± 13.1 | .25 | 0.20 |
| y-balance (% leg length) right | 72.2 ± 13.1 | 69.0 ± 14.1 | .21 | 0.24 |
| Absolute reach difference (cm) | 3.2 ± 2.7 | 3.4 ± 2.7 | .73 | 0.07 |
indicates statistical significance.
Fig. 2.
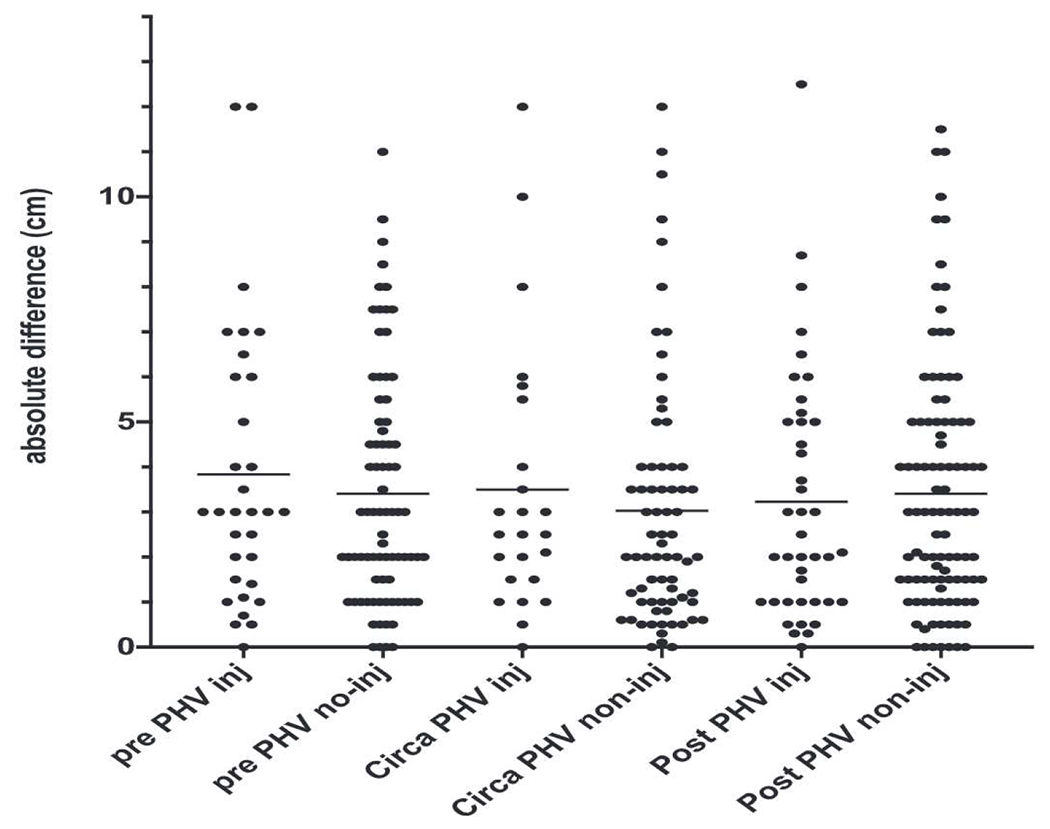
Distribution of inter-limb difference scores for prospectively injured and non-injured players in each maturity group. The mean scores is also displayed for each group by the marked line.
3.3. Pre-PHV injury risk factor associations
Injured players were significantly older, more physically mature, and had lower Y-Balance performance on both legs. The prevalence of injury in players with absolute reach difference >4 cm (27.8%) was not statistically different compared to players with absolute reach distance < 4 cm (29.3%) (p = 0.87). Multivariate analysis indicated lower relative scores on the left limb were the only variable associated with injury, such that for each unit reduction in relative left limb reach, the odds of experiencing an injury increased by 6% (OR: 0.94, CI: 0.91–0.98, p < 0.05) (Table 6). The model predicted 97.5% and 15.6% of non-injured and injured players respectively, with an overall prediction accuracy of 73.9% (R2 = 0.124).
Table 6.
Injury risk factors.
| Risk factors for injury | Beta (B) | Odds Ratio | 95% CI | P value |
|---|---|---|---|---|
| Pre-PHV group | ||||
| y-balance Left (% leg length) | −0.06 | 0.94 | 0.91–0.98 | <0.001* |
| Circa-PHV | ||||
| y-balance Right | 0.51 | 1.06 | 1.00–1.10 | <0.05* |
| Post-PHV | ||||
| Age | 0.4 | 1.49 | 1.04–2.13 | <0.05* |
| Height | 0.06 | 1.06 | 0.99–1.13 | 0.08 |
indicates statistical significance.
3.4. Circa-PHV injury risk factor associations
Injured players showed significantly greater Y-Balance scores than non-injured players on both legs. The prevalence of injury in players with absolute reach difference >4 cm (30%) was not statistically different compared to players with absolute reach distance < 4 cm (24.4%) (p = 0.61). Multivariate analysis indicated greater absolute scores on the right limb were the only variable significantly associated with injury (OR: 1.06, 95% CI: 1.05–1.10, p < 0.05), where a one-unit increase in y-balance scores on the right leg increased the odds of injury by 6% (Table 6). The model predicted 98.6% and 1% of non-injured and injured players respectively, with an overall prediction accuracy of 73.4% (R2 = 0.069).
3.5. Post-PHV injury risk factor associations
Injured players were older, taller, heavier and showed significantly greater Y-Balance scores than non-injured players on both legs. The prevalence of injury in players with absolute reach difference >4 cm (31.8%) was not statistically different compared to players with absolute reach distance < 4 cm (27.8%) (p = 0.63). The multivariate model consisted of age (OR: 1.49, 95% CI: 1.04–2.13, p < 0.05) and height (OR: 1.06, 95% CI: 0.99–1.13, p = 0.82) (Table 6); thus after adjusting for height, for each 1 year increase in age, there was a 1.5 times greater risk of injury. The model predicted 96% and 9.8% of non-injured and injured players respectively, with an overall prediction accuracy of 70.9% (R2 = 0.104).
4. Discussion
The aim of this study was to examine differences in the anterior reach Y-Balance test in elite male youth soccer players at different stages of maturity and its utility as an injury risk screening tool. Cross sectional data showed that absolute anterior reach distances were greatest in those who were post-PHV. Relative to leg length, pre-PHV players achieved the highest reach distances. Significant associations with future injury and y-balance anterior reach scores were present in pre and circa-PHV players; however, the strength of these relationships was low. Furthermore, no significant differences in the frequency of injury occurrence were shown between players breaching a pre-determined injury risk threshold (absolute reach difference > 4 cm) (Plisky et al., 2006; Smith et al., 2015), indicating that the Y-Balance anterior reach should be used with caution as an injury risk screening tool in elite male youth soccer players.
Absolute Y-Balance reach distances were highest in post-PHV players and this can be attributed to greater standing height and leg length (see Table 1). This is expected as more mature (and subsequently taller) children have displayed better functional reach scores, and therefore, adjustments should be made for leg length (Habib & Westcott, 1998). Previous research has reported age-related improvements in balance and reduced postural sway in recreationally active youths (Cumberworth et al., 2007; Nolan et al., 2005), and elite soccer players (Pau et al., 2014, 2015). Also, as children mature, they display improvements in postural control and the magnitude of centre of pressure excursions reduces (Riach & Stark, 1994). With maturation, the ability to use visual, vestibular and somatosensory information improves, and they learn to adapt to changes in body configurations and proportions, resulting in more controlled and accurate movement strategies (Habib & Westcott, 1998; Riach & Stark, 1994).
Normalization of reach scores relative to leg length identified that the pre-PHV players displayed the greatest reach distances. This could be attributed to heightened ranges of motion occurring via reductions in passive stiffness associated with younger ages (Ochi et al., 2008). Thus, performance on this test may be determined more by mobility (predominantly at the ankle) as opposed to dynamic balance as shown previously in young adults (Overmoyer & Reiser, 2015). It is also plausible that to determine maturity-related changes in balance performance, alternative measures such as postural sway, or the dynamic postural stability index may be required (Wikstrom et al., 2006).
Reductions in normalized reach distances were evident between each consecutive maturity group; however, these differences were significant only when comparing pre to post-PHV players. A plateau or decline in flexibility has been associated with the onset of the adolescent growth spurt (Philippaerts et al., 2006). This may be related to heightened musculotendinous stiffness resulting from increased restriction of titin filaments (Ochi et al., 2008), collagen filaments, and cross linking (McCormack, 2003). Specifically, structural changes to the ligaments and tendons may be present elevating stiffness of the tissues with the onset of adolescence (McCormack, 2003). Bone growth occurring in the absence of muscle length changes may result in momentary decreases in flexibility. In addition, bony adaptations have been shown to develop from recurrent ball impact in soccer players (Tol et al., 2002) which could reduce ankle dorsiflexion range of motion. Cumulatively, these maturational and sport specific adaptations could provide a plausible explanation for the reductions seen in normalized reach distance. Thus, it would appear prudent to target flexibility and range of motion control to offset these growth-related reductions in mobility.
Previous research has indicated an anterior right-left reach difference >4 cm increases the risk of lower extremity injury (Plisky et al., 2006). This has been confirmed more recently where anterior reach asymmetry was the only Y-Balance variable significantly associated with non-contact injury in collegiate athletes (Smith et al., 2015). In the current study, cross sectional analysis showed no significant between group differences were present in absolute right/left reach differences and mean scores indicated that none of the maturity groups exceeded the 4 cm threshold. Furthermore, the injury analysis showed a wide distribution of scores (Fig. 2) and did not identify any significant differences between injured and non-injured players. There were also no differences in the frequency of injury occurrence between players breaching this threshold in any maturity group versus those who did not. The aforementioned research included a sample of youth basketball players (Plisky et al., 2006) and division I collegiate athletes from multiple sports (Smith et al., 2015) which in part may explain the disparate findings in the current study. Furthermore, large standard deviations were reported for most maturity groups indicating a wide dispersion of scores are likely in elite male youth soccer players. Our results suggest that absolute reach differences measured during the anterior reach of the Y-Balance test and specifically a threshold of >4 cm should be used with caution for the purposes of injury risk screening in elite male youth soccer players.
In this study, significant differences between injured and non-injured players were shown for combinations of anthropometric and Y-Balance anterior reach distances although variation was evident across the different maturity groups. Greater reach distances were observed on the right leg (when the stance leg was the left) in comparison to the left (when the stance leg was the right) in injured versus non-injured players regardless of maturity group (Tables 3–5). Furthermore, multivariate analysis indicated that significant associations with injury were present in pre and circa-PHV players. These data suggest that when the task is performed with the limb controlling the movement of what is typically their dominant kicking leg, reduced absolute reach scores are more important to monitor than absolute right-left differences. However, the odds ratio and thus, the strength of these associations could be considered low (Table 6), indicating that a large unit change in reach distances would be required to meaningfully increase injury risk. Furthermore, the prediction accuracy of each model was low and no associations between Y-Balance anterior reach distances and injury risk were identified in post-PHV players. Advanced chronological age was the only variable to remain significant in the multivariate model.
Previous research has shown no association between Y-Balance composite scores and injury risk in elite female youth soccer players (Nilstad et al., 2014). Effective performance during dynamic stability tasks requires the integration of visual, vestibular and proprioceptive inputs, which provide an efferent response to control the body’s centre of mass within its base of support (Guskiewicz et al., 1996). Thus, a weak association between y-balance anterior reach scores and injury risk in the current study could be explained in part by the multifactorial nature of injuries in soccer and the complex interaction of factors that comprise dynamic balance. Consequently, it may not be possible to accurately assess all of these constructs in a single field-based assessment (Nilstad et al., 2014).
When interpreting the data from the current study, practitioners should also be cognizant of some limitations. Firstly, previous injury, which has been reported as a risk factor for future injury occurrence (Hagguland et al., 2006), was not accounted for in this study. Due to the frequency with which players move between clubs in academy soccer, to record this information would have required the use of retrospective analysis which is subject to recall bias. Secondly, in the current study, all non-contact, lower extremity injuries were included. Future research should aim to investigate the clinical utility of this test in elite male youth soccer players with a focus on key anatomical locations and injury types such as knee and ankle ligament injuries.
5. Conclusions
The current study examined the utility of the anterior reach Y-Balance test in elite male youth soccer players. The key findings indicate the following: 1) the test displays acceptable typical error and can differentiate between maturity groups with a trend of reductions in relative reach scores as players mature and; 2) absolute reach scores on what is typically the dominant kicking leg display some small association with future injury. However, a large change in reach distances would be required to meaningfully increase injury risk and applying previously identified between-limb symmetry thresholds (>4 cm) could not differentiate between injured and non-injured players.
Cumulatively, these data provide evidence that the anterior reach of the Y-Balance test should be used with caution as an injury risk screening tool in elite male youth soccer players. In addition, the youngest and least mature players achieved the highest reach distances relative to leg length. This suggests that anterior reach scores are determined more by mobility, as opposed to dynamic balance. Given that the greatest reductions in reach distance/mobility were shown between pre and post-PHV players, it could be inferred that training programs should incorporate appropriate training to offset these likely growth-related reductions in mobility.
Table 4.
Descriptive characteristics of injured and non-injured circa-PHV players.
| Injured (n = 24) | Non-injured (n = 70) | p value | Cohens d | |
|---|---|---|---|---|
| Age (years) | 14.3 ± 1.0 | 14.1 ± 1.0 | .33 | 0.20 |
| Mass (kg) | 51.5 ± 7.0 | 51.8 ± 7.1 | .84 | 0.04 |
| Height (cm) | 164.1 ± 7.8 | 163.6 ± 7.6 | .78 | 0.06 |
| BMI | 19.1 ± 1.4 | 19.3 ± 1.6 | .50 | 0.12 |
| Maturational offset (years) | −0.16 ± 0.61 | −0.08 ± 0.62 | .59 | 0.13 |
| Leg length | 87.8 ± 4.6 | 86.1 ± 6.0 | .23 | 0.31 |
| y-balance left | 63.5 ± 8.4 | 58.5 ± 9.8 | .03* | 0.34 |
| y-balance right | 65.7 ± 7.7 | 59.8 ± 10.2 | .01* | 0.65 |
| y-balance (% leg length) left | 72.3 ± 9.7 | 68.2 ± 11.6 | .09 | 0.38 |
| y-balance (% leg length) right | 74.8 ± 8.6 | 69.6 ± 11.8 | .05* | 0.50 |
| Absolute reach difference (cm) | 3.7 ± 3.7 | 3.1 ± 2.9 | .41 | 0.18 |
indicates statistical significance.
Funding statement
The authors confirm that no sources of funding were obtained in connection with any aspect of this manuscript and the content represents the authors own work. Open access funding was provided by the Qatar National Library.
Footnotes
Ethical statement
Parental consent and participant assent were collected prior to the commencement of testing. Ethical approval was granted by the institutional ethics committee in accordance with the declaration of Helsinki.
Declaration of competing interest
Paul J. Read, Jon L. Oliver, Gregory D. Myer, PhD, Abdulaziz Farooq, Mark De Ste Croix, and Rhodri S. Lloyd confirm there are no conflicts of interest associated with any aspects or content of this manuscript.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ptsp.2020.06.002.
References
- Atkins SJ, Hesketh C, & Sinclair JK (2016). The presence of bilateral imbalance of the lower limbs in elite youth soccer players of different ages. The Journal of Strength & Conditioning Research, 4, 1007–113. [DOI] [PubMed] [Google Scholar]
- Cumberworth VL, Patel NN, Rogers W, & Kenyon GS (2007). The maturation of balance in children. Journal of Laryngology & otology, 121, 449–454. [DOI] [PubMed] [Google Scholar]
- Faigenbaum AD, Myer GD, Fernandez IP, Gomez Carrasco E, Bates N, Farrell A, Ratamess NA, & Kang. (2014). Feasibility and reliability of dynamic postural control measures in children in first through fifth grades. International Journal of Sports Physical Theraphy, 9, 140–148. [PMC free article] [PubMed] [Google Scholar]
- Guskiewicz KM, Perrin DH, & Gansneder B (1996). Effect of mild head injury on postural stability in athletes. Journal of Athletic Training, 31, 300–306. [PMC free article] [PubMed] [Google Scholar]
- Habib Z, & Westcott S (1998). Assessment of anthropometric factors on balance tests in children. Pediatric Physical Therapy, 10, 101–109. [Google Scholar]
- Hagguland M, Walden M, & Ekstrand J (2006). Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive seasons. British Journal of Sports Medicine, 40, 767–772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hegedus EJ, McDonough S, Bleakley C, Baxter DE, & Cook CE (2015). Clinician-friendly lower extremity physical performance tests in athletes: A systematic review of measurement properties and correlation with injury. Part 2 - the test for hip, thigh, foot and ankle including the star excursion balance test. British Journal of Sports Medicine, 49, 649–656. [DOI] [PubMed] [Google Scholar]
- Hegedus EJ, McDonough S, Bleakley C, Cook CE, Baxter DG. Clinician-friendly lower extremity physical performance measures in athletes: A systematic review of measurement properties and correlation with injury, part 1. The test for knee function including hop tests. British Journal of Sports Medicine doi: 10.1136/bjsports-2014-094094. [DOI] [PubMed] [Google Scholar]
- Hopkins WG (2000). Reliability from consecutive pairs of trials (Excel spreadsheet). In: A new view of statistics, sportsci.org: Internet Society for Sport Science. Available at: sportsci.org/resource/stats/xrely.xls. (Accessed 27 April 2016). [Google Scholar]
- Le Gall F, Carling C, Reilly T, Vandewalle H, Chruch J, & Rochcongar P (2006). Incidence of injuries in elite French youth soccer players; a 10-season study. The American Journal of Sports Medicine, 34, 928–938. [DOI] [PubMed] [Google Scholar]
- Lloyd RS, Oliver JL, Hughes MG, & Williams CA (2012). Age-related differences in the neural regulation of stretch–shortening cycle activities in male youths during maximal and sub-maximal hopping. Journal of Electromyography and Kinesiology, 22, 37–43. [DOI] [PubMed] [Google Scholar]
- Malliou P, Gioftsidou A, Pafis G, et al. (2004). Proprioceptive training (balance exercises) reduces lower extremity injuries in young soccer players. Journal of Back and Musculoskeletal Rehabilitation, 17, 101–104. [Google Scholar]
- McCormack RJ (2003). The flexibility of the collagen compartment of muscle. Meat Science, 36, 79–91. [DOI] [PubMed] [Google Scholar]
- McGuine TA, & Keene JS (2006). The effect of a balance training program on the risk of ankle sprains in high school athletes. The American Journal of Sports Medicine, 34, 1103–1111. [DOI] [PubMed] [Google Scholar]
- Mirwald RL, Baxter-Jones ADG, Bailey DA, & Beunen GP (2002). An assessment of maturity from anthropometric measurements. Medicine & Science in Sports & Exercise, 34, 689–694. [DOI] [PubMed] [Google Scholar]
- Munro A, & Herrington L (2010). Between-session reliability of the star excursion balance test. Physical Therapy in Sport, 11, 128–132. [DOI] [PubMed] [Google Scholar]
- Nilstad A, Andersen TE, Bahr R, Holme I, & Steffen K (2014). Risk factors for lower extremity injuries in elite female soccer players. The American Journal of Sports Medicine, 42, 940–948. [DOI] [PubMed] [Google Scholar]
- Nolan L, Grigorenko A, & Thorstennson A (2005). Balance control: Sex and age differences in 9 to 16 year olds. Developmental Medicine and Child Neurology, 47, 449–454. [DOI] [PubMed] [Google Scholar]
- Ochi E, Nakazato K, Song H, & Nakajima H (2008). Aging effects of passive resistive torque in the rat ankle joint after lengthening contractions. Journal of Orthopaedic Science, 13, 218–224. [DOI] [PubMed] [Google Scholar]
- Overmoyer GV, & Reiser RF (2015). Relationships between lower –extremity flexibility, asymmetries and the y-balance test. The Journal of Strength & Conditioning Research, 29, 1240–1247. [DOI] [PubMed] [Google Scholar]
- Pau M, Arippa F, Leba B, Corona F, Ibba G, Todde F, & Scorcu M (2015). Relationship between static and dynamic balance abilities in Italian professional and youth league soccer players. Physical Therapy in Sport, 16, 236–241. [DOI] [PubMed] [Google Scholar]
- Pau M, Ibba G, & Leban Scorcu M (2014). Characterization of static balance abilities in elite soccer players by playing position and age. Research in Sports Medicine: International Journal, 22, 355–367. [DOI] [PubMed] [Google Scholar]
- Philippaerts RM, Vaeyens R, Janssens M, Van Renterghem B, Matthys D, Craen R, Bourgois J, Vrijens J, Beunen GP, & Malina RM (2006). The relationship between peak height velocity and physical performance in youth soccer players. Journal of Sports Sciences, 24, 221–230. [DOI] [PubMed] [Google Scholar]
- Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, & Elkins B (2009). The reliability of an instrumented device for measuring components of the star excursion balance test. North American Journal of Sports Physical Therapy : NAJSPT, 4(2), 92–99. [PMC free article] [PubMed] [Google Scholar]
- Plisky PJ, Rauh MJ, Kaminski TW & Underwood FB (2006). Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players .Journal of Orthopaedic & Sports Physical Therapy, 36, 911–919. [DOI] [PubMed] [Google Scholar]
- Price RJ, Hawkins RD, Hulse MA, & Hodson A (2004). The football association and medical research programme: An audit of injuries in academy youth football. British Journal of Sports Medicine, 38, 466–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, & Lloyd RS (2016). Neuromuscular risk factors for knee and ankle injuries in male youth soccer players. Sports Medicine, 46, 1059–1066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, & Lloyd RS (2017a). An audit of injuries in six professional soccer academies. Journal of Sports Science, 1–7. [DOI] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, & Lloyd RS (2017b). Hopping and landing performance in youth soccer players: Effects of age and maturation. Int J Sports Med, 38, 902–908. [DOI] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, & Lloyd RS (2018). The effects of maturation on measures of asymmetry during physical performance tests in elite male youth soccer players. Ped Ex Science, 30, 168–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, & Lloyd RS (2018). Landing kinematics in elite male youth soccer players of different chronologic age and stage of maturation. Journal of Athletic Training, 53, 372–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, & Lloyd RS (2018). Risk factors for lower extremity injury risk in male youth soccer players: A prospective cohort study. Scandinavian Journal of Medicine & Science in Sports, 28, 1244–1251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, Belshaw A, & Lloyd RS (2018). Altered landing mechanics are shown by male youth soccer players at different stages of maturation. Physical Therapy in Sport, 33, 48–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read PJ, Oliver JL, De Ste Croix M, Myer GD, & Lloyd RS (2019). A review of field-based assessments of neuromuscular control and their utility in male youth soccer players. The Journal of Strength & Conditioning Research, 33, 283–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riach CL, & Stark JL (1994). Velocity of centre of pressure excursions as an indicator of postural control systems in children. Gait & Posture, 2, 167–172. [Google Scholar]
- van der Sluis A, Elferink-Gemser MT, Coelho-e-Sliva MJ, Nijboer JA, Brink MS, & Visscher C (2014). Sports injuries aligned to peak height velocity in talented pubertal soccer players, Int J Sports Med, 35, 351–355. [DOI] [PubMed] [Google Scholar]
- Smith CA, Chimera NJ, & Warren M (2015). Association of y balance test reach asymmetry and injury in division I athletes. Medicine & Science in Sports & Exercise. 47(1), 136–141. [DOI] [PubMed] [Google Scholar]
- Tol JL, Slim E, van Soest AJ, & van Dijk CN (2002). The relationship of the kicking action in soccer and anterior ankle impingement syndrome. A biomechanical analysis. The American Journal of Sports Medicine, 30(1), 45–50. [DOI] [PubMed] [Google Scholar]
- Wikstrom EA, Tillman MD, Chmielewski TL, & Borsa PA (2006). Measurement and evaluation of dynamic joint stability of the knee and ankle after injury. Sports Medicine, 36, 393–410. [DOI] [PubMed] [Google Scholar]