

Abstract
Introduction:
We examined whether factors identified as associated with cannabis use at age 14 to 16 years are also associated with ever use at age 12.
Methods:
Participants in the AdoQuest study (n=1852) were recruited in 2005 from among Grade 5 students in 29 French-language elementary schools in Montral, Canada. Self-report data were collected from participants in Grade 5 (spring 2005) and 6 (fall 2005 and spring 2006) and from parents/guardians in 2006/07. Inclusion in the analytic sample (n=1076; mean age [SD]=10.7[0.5]) required data from participant and parental questionnaires and data on cannabis use in Grade 6 (mean age [SD]=11.7 [0.4]). We estimated associations between ever use at age 12 with 33 potential correlates, separately in unadjusted and adjusted logistic regression models.
Results:
Fifty-three participants (4.9%) reported ever use at age 12. Factors associated with higher odds of ever use included older age, identifying as male, lower household income, more weekly spending money, ever tried cigarettes or other tobacco products, ever drank alcohol or binge drank, ever gambled, friends or siblings smoke cigarettes, greater nicotine dependence, higher depressive symptoms and greater impulsivity. Protective factors included higher levels of parental/guardian monitoring and greater self-esteem and school connectedness.
Conclusion:
Factors associated with cannabis use at later ages are also associated with ever use at age 12. Our findings suggest that surveillance for and interventions to prevent cannabis use are warranted before age 12.
Keywords: cannabis use, adolescents, early use, risk/protective factors
Highlights
We investigated if well-established risk factors for cannabis, alcohol and/or tobacco use during adolescence are associated with ever use of cannabis in youth aged 12 years.
Among 14- to 18-year-olds, higher odds of cannabis use are associated with the use of other substances, peers or siblings who smoke cigarettes, depressive symptoms and impulsivity.
Higher levels of parental/guardian monitoring and greater self-esteem and school connectedness are associated with lower odds of cannabis use among 14- to 18-year-olds.
We found similar associations with ever use of cannabis at age 12 years.
Our findings suggest that surveillance for and interventions to prevent cannabis use are warranted for youth younger than 12 years.
Introduction
Cannabis use typically begins during adolescence. In Canada, 18% of students in Grades 7 to 12 (12–18 years old) reported past-year cannabis use in 2018/19, including 2% of students in Grade 7 (aged 12–13years) and 4% of those in Grade 8 (aged 13–14 years).1 In the US in 2019, 15% of Grade 8 students (aged 13–14years) reported lifetime cannabis use and 12% reported past-year use.2 The mean (95% confidence interval [CI]) age of cannabis use initiation among secondary school students (aged 12–18 years) in Canada in 2018/19 was 14.3 (14.1–14.4) years.1
Data from the Canadian Youth Smoking Survey (YSS; 2002–2013) show that the mean age [SD] of initiation among younger adolescents in Grades 7–9 (aged 12–15 years) was 12.6 [1.3] years in 2002/03 and 12.7 [1.5] years in 2004/05.3 The mean age (95% CI) of initiation was 12.8 (12.7–12.9) in 2006/07, when AdoQuest data were collected (unpublished data, personal communication from Health Canada, 8 June 2022). This mean age remained steady until 2012/13, then fluctuated over the next 6 years, reaching 13.1 (12.9–13.2) in 2018/19 (unpublished data from the Canadian Student Alcohol and Drug Survey 2014–2019, personal communication from Health Canada, 8 June 2022). The net increase in age at initiation of 12- to 15-year-olds between 2002/03 and 2018/19 was 6 months.
Compared with later use, early substance use carries greater risk of eventual abuse and dependence as well as higher risks for poor outcomes in adulthood (e.g. lower educational attainment, substance dependence, crime, early pregnancy).4 Yet little is known about factors associated with early cannabis use. Using data from the annual, cross-sectional National Survey on Drug Use and Health, Forman-Hoffman et al.5 found that 5.5% of participating 12- to 14-year-olds (n ≈ 85000) in the US reported ever having used cannabis. The researchers also found a greater likelihood of early cannabis use associated with older age, male sex, White non-Hispanic ethnicity, household income below the federal poverty level (as defined by the US government), living in a large urban area, having ever used alcohol or tobacco, lifetime history of major depressive episodes and having been involved in serious physical fights at school.5
We reviewed 19 longitudinal studies in which cannabis use onset in adolescence or young adulthood was the outcome.6-24 Only 2 of the 19 studies examined onset of cannabis use prior to age 14 years. In the first, Baily and Hubbard6 recruited Grades 6 through 8 students (n=3454) at baseline and assessed cannabis use a year later. Of 1091 Grade 6 students, 9.7% had initiated cannabis use by Grade 7. “Importance of communication within the family” was protective and “ability to communicate within the family” was a risk factor. Bailey and Hubbard remarked that this finding was contrary to their expectations and speculated that the “‘ability to communicate within the family’ represents a dimension of liberal acceptance on the part of parents or a dimension of precociousness on the part of the young adolescents.”6,p. 65 They found no relationship between onset of cannabis use and peer attachment, school attachment, adults’ and friends’ attitudes towards alcohol use or cannabis use, or peer use of alcohol or cannabis.
In the second study, Tang and Orwin7 used data from the US National Survey of Parents and Youth (1998–2004) in which seven nationally representative age cohorts (i.e. 9–15-year-olds at baseline, with each age treated as a separate cohort) of never cannabis users were each followed for 2 years. Risk factors for initiation by age 13 years included parental drug use (not defined by a specific drug), friends’ cannabis use, participants’ own smoking and drinking, and having been offered cannabis.7 Parental monitoring was protective.7
Onset of smoking and drinking tends to occur earlier than onset of cannabis use,1 and risk and protective factors for tobacco and alcohol use in young adolescents might also be related to early cannabis use. Therefore, we consulted systematic reviews of risk and protective factors for adolescent onset of cigarette smoking25 and drinking,26 in addition to the 19 studies on cannabis use onset,6-24 to identify factors consistently associated with use of these substances.
Because early cannabis use has particularly harmful long-term effects on physical and mental health,27-32 and given the dearth of studies addressing use before age 14 years, we sought to determine whether factors associated with adolescent cannabis, tobacco and alcohol use are also associated with ever use of cannabis at age 12 years.
This study adds to the two extant longitudinal studies6,7 examining early initiation of cannabis use by examining a much broader range of potential risk and protective factors (i.e. sociodemographic characteristics, lifestyle factors, characteristics of the social environment, psychological characteristics and pubertal status) in a large population-based sample of Grade 5 and Grade 6 Canadian youth (10–12 years old).
Methods
The AdoQuest study
We drew data from the first three waves of the six-wave AdoQuest study. In spring 2005, we randomly sampled 40 French-language schools in Greater Montral (Quebec, Canada) with more than 90 students in Grade 5. We invited equal numbers of schools according to tertile groupings of a school socioeconomic status (SES) indicator.33 Of the invited schools, 29 (72.5%) agreed to participate, including 10 in the high, 10 in the moderate and 9 in the low SES grouping. Students were recruited from all Grade 5 classes in participating schools.
We collected data in classroom-administered questionnaires once in Grade 5 (spring 2005) and twice in Grade 6 (fall 2005 and spring 2006). Parents/guardians* completed mailed self-report questionnaires in 2006/07. Participants provided assent and parents/guardians provided informed consent.
Baseline characteristics of AdoQuest study participants aligned with those of two provincially representative samples of Quebec youth34,35 (data available on request from the authors).
Ethics approval
The study received approval from the institutional review boards of Concordia University (Concordia Ethics form 2006 number: UH2006-063) and the Centre de recherche du Centre Hospitalier de l’Universit de Montral (ADOQUEST F9-60229).
Study design
Data for ever use of cannabis were drawn from participant questionnaires completed in Grade 6 (i.e. fall 2005 and/or spring 2006). The value retained for analysis indicated whether the participant had ever reported cannabis use at either of these two time points. Data for 22 factors investigated as potentially associated with ever use were collected in Grade 5 or 6 (i.e. spring 2005, fall 2005 and/or spring 2006); for analysis, we retained the Grade 6 value of the factor unless the Grade 5 value was the only one available.
Data on nine variables (i.e. older sibling(s), lone parent family, parental education, household income, parental cannabis use, parental alcohol use and binge drinking, parental monitoring, parental attachment) were drawn from the parent questionnaire completed in 2006/07 (i.e. after participant data were collected), and data on two variables (i.e. parental smoking, home smoking ban) were collected in both participant and parent questionnaires. Because we could not ascertain the temporal ordering of the retained value of the potential correlate and the report of ever use, we consider the study design to be cross-sectional.
Study variables
Cannabis use was measured in the fall of Grade 6 with two questions: (1) “In your whole life, have you ever consumed cannabis (marijuana, pot, hashish)?” (Possible answers were “No,” “Yes,” or “I don’t know what cannabis is”); and (2)“In the past year, how many times did you consume cannabis?” We asked both questions again in the spring of Grade 6, but this time the second question referred to a 6-month time frame. Response options at both time points were “I don’t know what cannabis is,” “I have never consumed cannabis in my entire life” and “from 1–2 to 40+ times.” Participants who answered “No, I have never...” or “I don’t know...” at both assessments were classified as not having used cannabis; those who answered “Yes” or endorsed using cannabis any number of times at either assessment were classified as having used cannabis.
We selected the 33 potential correlates of cannabis use based on the literature as well as on their availability in the AdoQuest study (see Table 1). These included 8 sociodemographic characteristics (i.e. age, sex, older siblings, two-parent family, parents education, household income, neighbourhood deprivation index, participant’s weekly spending money); 10lifestyle factors (i.e. ever tried cigarettes, ever tried other tobacco products, ever drank alcohol, ever binge drank, ever gambled, perceived academic performance, hours/day of TV, hours/day of computer games, frequency of reading not assigned for school, weekly physical activity); 9 characteristics of the social environment (i.e. parents use cannabis, parents smoke cigarettes, parents drink alcohol, parents binge drink, smoking banned at home, siblings smoke cigarettes, friends smoke cigarettes, parental monitoring, quality of caregiver–child relationship); 5 psychological characteristics (i.e. feel mentally or physically dependent on nicotine, self-esteem, depressive symptoms, impulsivity, school connectedness); and pubertal status.36 Details on these variables, including questionnaire items, response choices, their coding for analyses and their psychometric properties (for derived scales), are available from the authors on request.
Table 1. Potential correlates of ever use of cannabis associated with adolescent onset of cannabis, alcohol or tobacco use in extant longitudinal studies.


|
Data analysis
Data analyses were conducted with Stata version 14.2 (Stat Corp LLC, College Station, TX, US).
Analytic sample
In Grade 5, 1801 students (mean age [SD]= 10.7 [0.6] years) provided data. By Grade 6, an additional 51 students joined the study (mean age [SD] of all Grade 6 participants = 11.7 [0.4] years), yielding a total 1852 participants. To develop the analytic sample, we first retained participants whose parents had completed the parental questionnaire in 2006/07 (n = 1127; 61% of 1852). Then we retained those participants who had provided data on cannabis use (n = 1076; 95% of 1127). Of the 1076 participants retained, 975 (90.6%) completed all three waves; 100 (9.3%) completed two waves and only 1 (0.1%) completed one wave.
Missing values
We used multiple imputation to account for missing values, with predictive mean matching with 10 nearest neighbour comparators for continuous and ordinal variables37 and logistic regression for binary variables. We employed von Hippel’s38 two-step calculation to determine the number of imputation sets needed to produce replicable estimates of standard errors. All variables to be examined in the analyses, including ever use, were entered into the imputation models.
Analyses
We estimated the association for each potential correlate in two models only, an unadjusted model and then an adjusted model that included sociodemographic characteristics that were correlated with cannabis use (i.e. age, sex, household income and participants’ weekly spending money). Because the unadjusted and adjusted models for each potential correlate constitute a single hypothesis test, we did not correct for multiple comparisons.39 We did not estimate associations for potential correlates in an omnibus model (i.e. one that included all potential correlates) because omnibus models may include variables on the causal pathway for other covariates,40 which could lead to attenuated estimates.41 We conducted logistic regression analyses with cluster robust standard errors to minimize bias in variance estimates related to clustering by school.42
Results
Participants
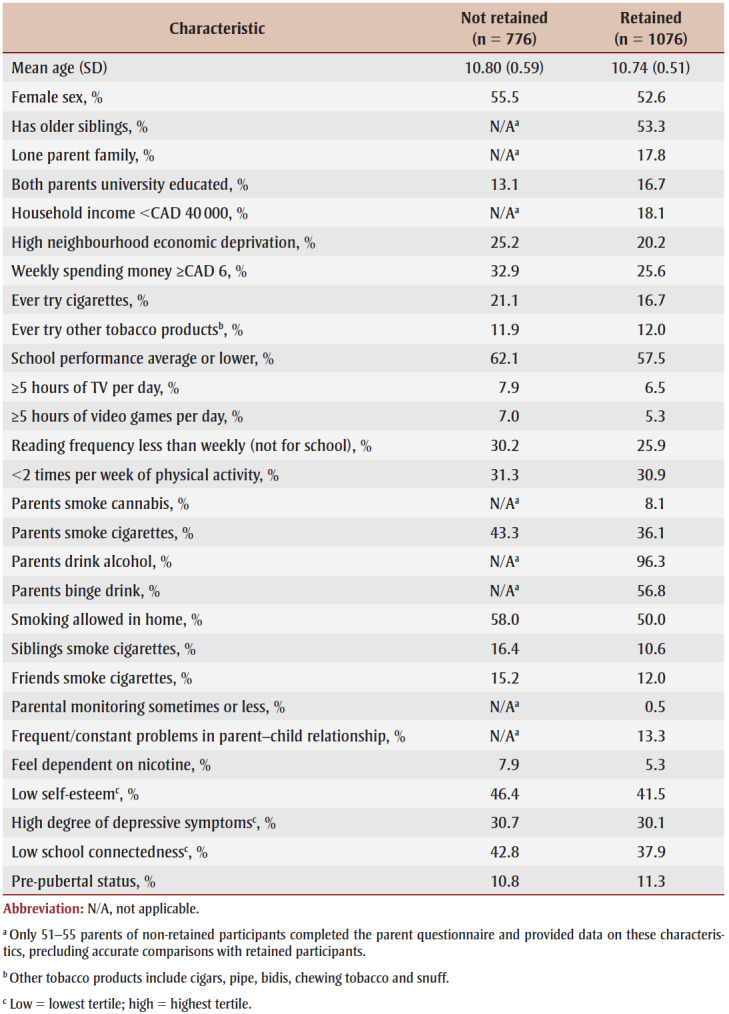
Based on recommendations on how to report descriptive data from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines,43 we compared characteristics of AdoQuest study participants retained for analysis (n= 1076) with those of participants who were lost to follow-up since inception or missing data on the variables of interest (n = 776) (see Table 2). Large differences between groups could indicate possible selection bias.
Table 2. Baseline characteristics of AdoQuest study participants not retained and retained for analyses.
|
Although data for most variables were drawn from the baseline participant questionnaire, data for eight variables (i.e. older siblings, lone parent family, household income, parental cannabis use, parental drinking, parental binge drinking, parental monitoring, parent–child relationship) were collected in parental questionnaires only. Because only 51 to 55parents of the 773 AdoQuest study participants not retained for analysis completed the parent questionnaire, we did not report estimates for these variables in this group as they would likely be imprecise and biased.
Overall, there were few notable differences in the estimates for the 21 variables that we compared across groups, with two possible exceptions. Of participants not retained, 32.9% reported that they had weekly spending money of CAD 6 or more compared to 25.6% of participants retained for analysis; and of parents in the not retained group, 43.3% smoked cigarettes compared to 36.1% of parents in the retained group.
Missing data
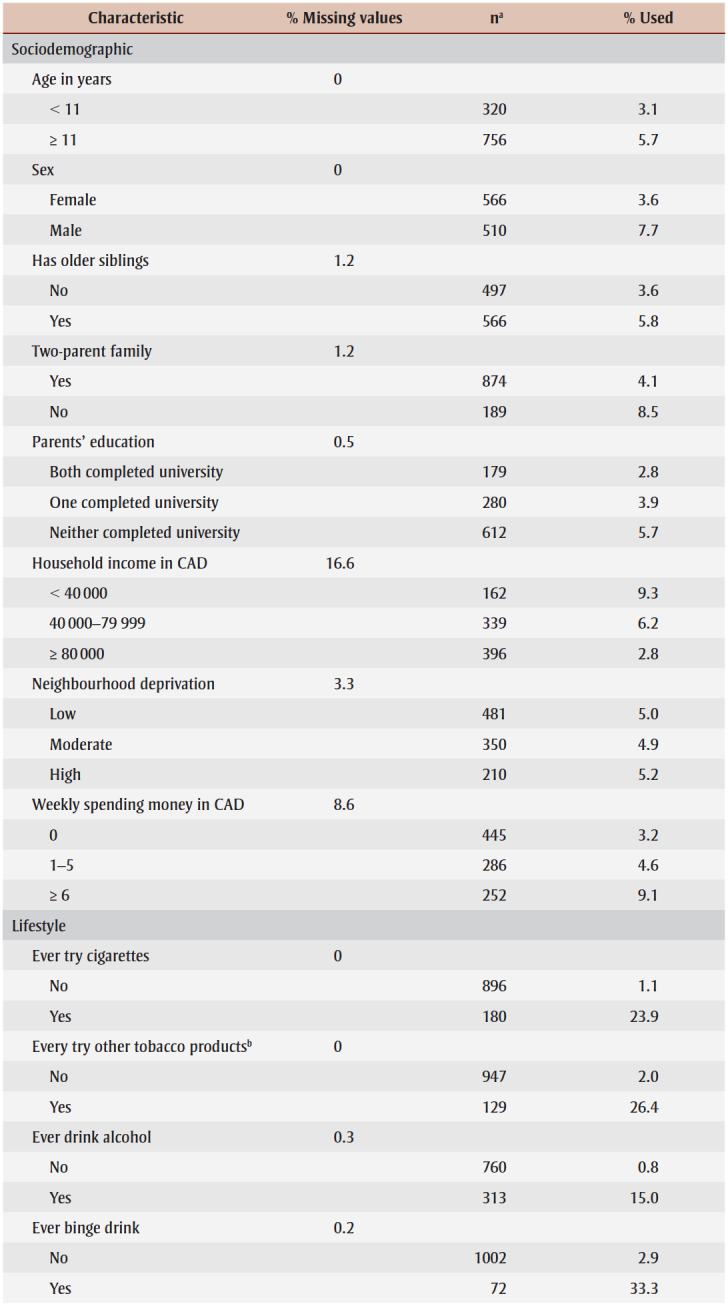
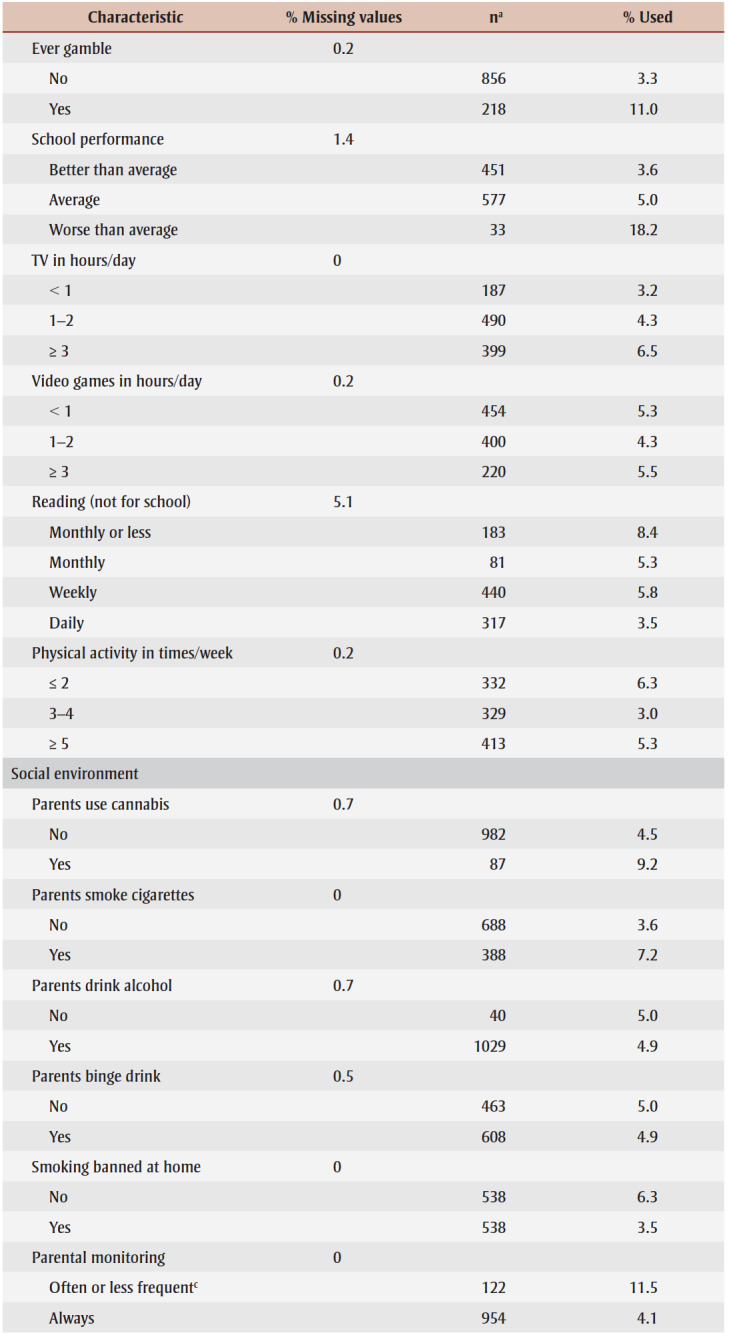
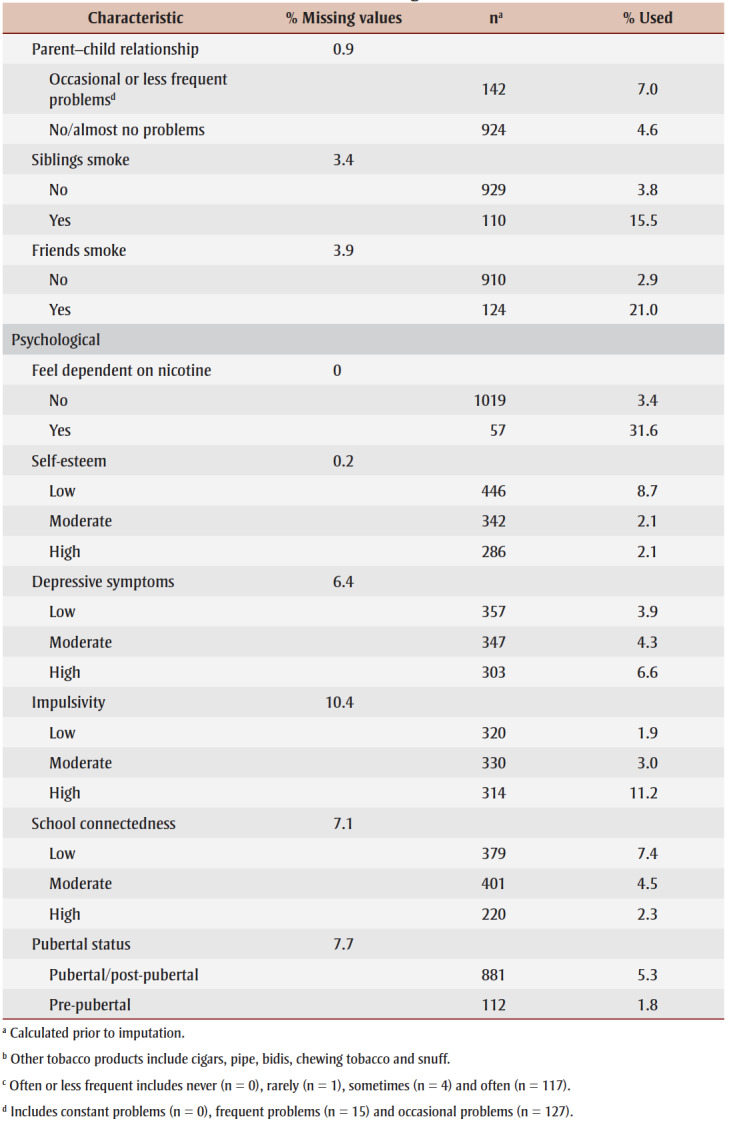
The proportion of missing values ranged from 0 (9 variables) to 16.6% (household income; see Table 3). The median (interquartile range) proportion of missing values was 0.5% (0–3.4). We therefore created 20 imputed datasets. Comparisons of imputed and raw data show that the imputations produce similar distributions. Further, sensitivity analyses with complete cases only yield similar estimates to those using imputed datasets (data available on request from the authors).
Table 3. Bivariate associations between participant characteristics and ever use of cannabis at age 12 (n = 1076).
|
Correlates of cannabis use
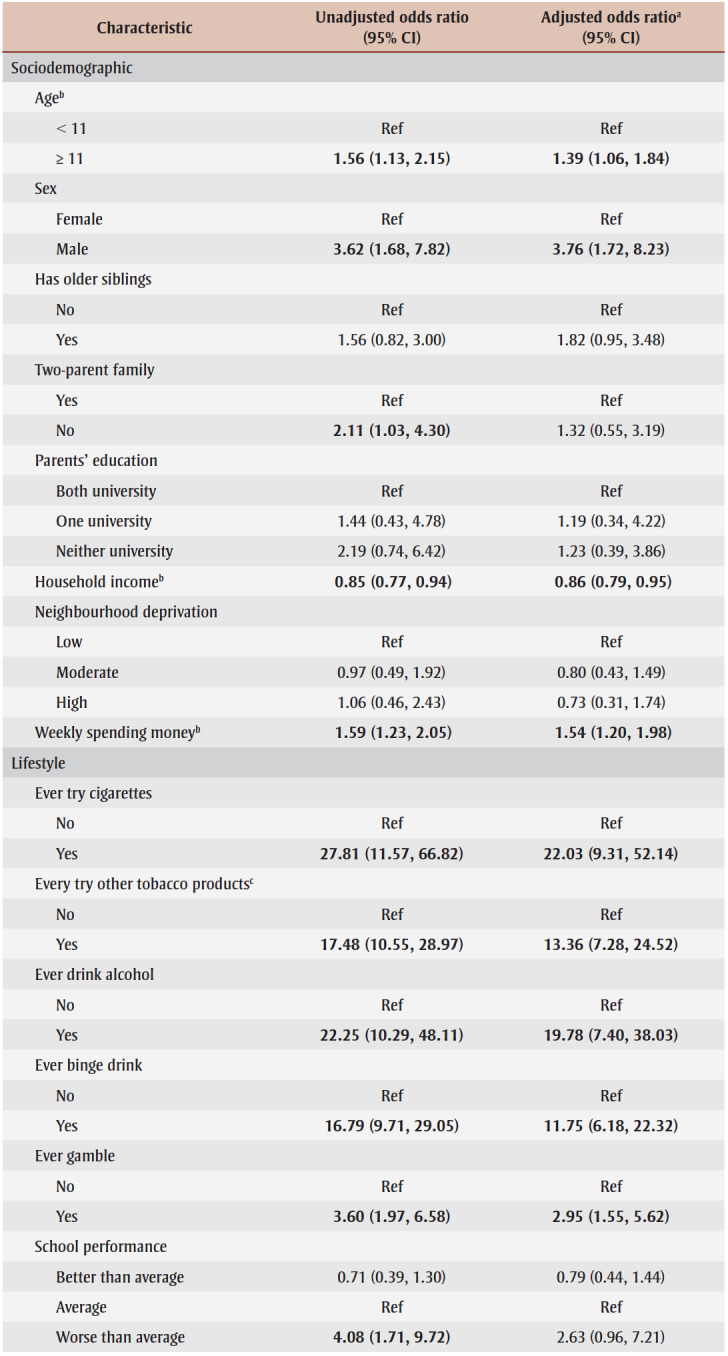
Fifty-three participants (4.9%) reported ever use of cannabis by the end of Grade 6 (mean age [SD] = 11.7 [0.4] years). Table3 presents bivariate relationships between participant characteristics and ever use of cannabis. Table 4 presents unadjusted and adjusted odds ratios (OR) and 95% CI from the logistic regression analyses.
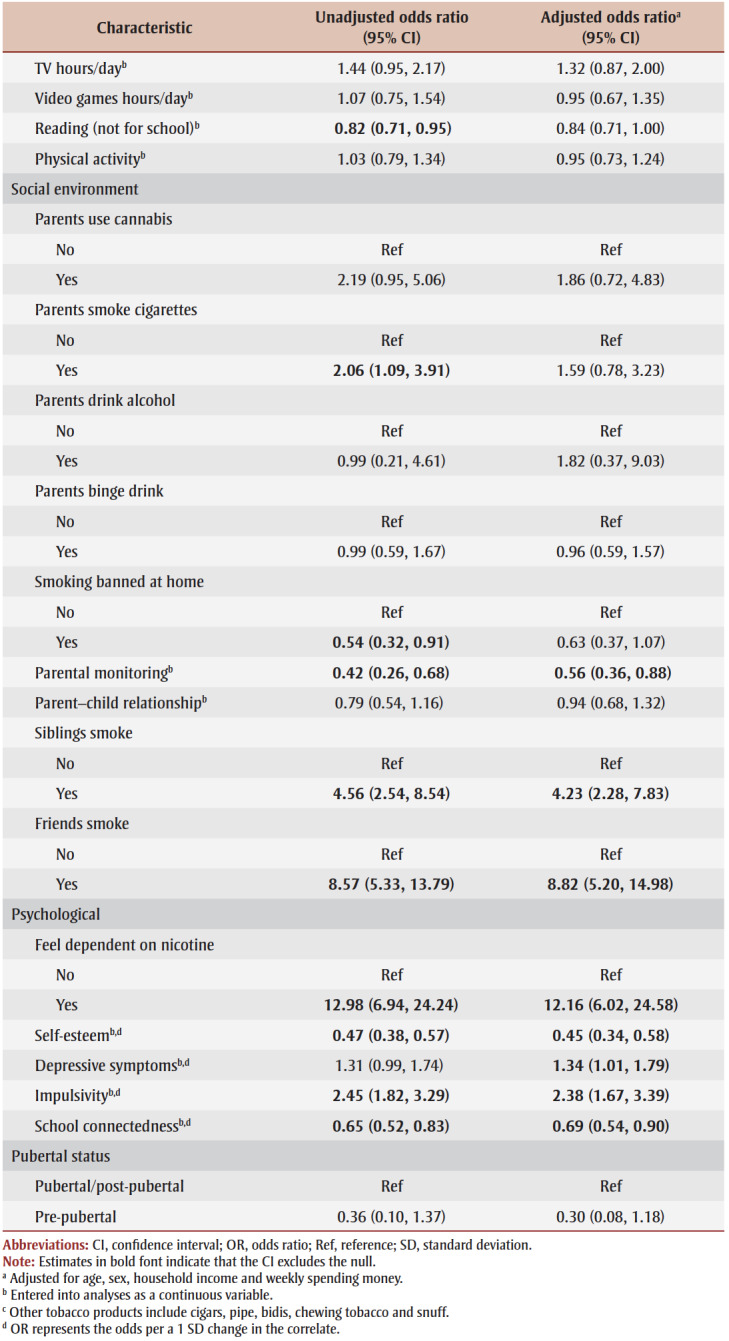
Table 4. Associations between participant characteristics and ever use of cannabis at age 12 (n = 1076).
|
We note one caveat in interpreting our findings. Categories for five variables (i.e. never tried cigarettes, never drank, parents used cannabis, parents did not drink, pre-pubertal status) had low frequencies and few participants in those categories initiated cannabis use. This affected our ability to report precise estimates, and the magnitude of the estimates for these variables should be interpreted with caution.
Of the 33 variables investigated as potential correlates, 17 were associated with ever use in adjusted models. Four of eight sociodemographic characteristics (i.e. older age, identifying as male, lower household income, having more spending money) were associated with higher odds of ever use, as were 5 of 10 lifestyle factors (i.e. ever tried cigarettes, ever tried other tobacco products, ever drank alcohol, ever binge drank and ever gambled).
Of the nine social environmental influences investigated, two (i.e. sibling/s smoke cigarettes, friends smoke cigarettes) were positively associated with ever use and one (i.e. parental monitoring) was inversely associated with ever use.
All five psychological characteristics were associated with ever use. Three (i.e. feeling dependent on nicotine, higher depressive symptoms, greater impulsivity) were associated with higher odds, and two (i.e. greater self-esteem and higher school connectedness) were associated with lower odds. Pubertal status was unrelated to ever use of cannabis.
Discussion
This study is one of the few to identify factors associated with cannabis use among children younger than 14. We found that 5% of Grade 6 students in the AdoQuest study (who were on average 11.7 years old in the spring of Grade 6) reported that they had ever used cannabis. This is a full year before the mean age of onset reported among Canadian students in Grade 7 to 9, who were on average 12.8 years old when we conducted our study. It is not yet clear whether legalization has significantly affected age at onset or the prevalence of early cannabis use among youth in Canada, although 2% and 4% of students in Grade 7 and 8, respectively, reported past-year cannabis use in 2018/19.1
While the frequency of early cannabis use as well as the frequency of its risk factors can change over time in response to contextual changes such as legalization, the associations between these exposures and early onset are not likely to change substantially, especially over relatively short time spans such as a decade. As an analogy, despite decades of research and profound changes in the tobacco-related context, the main risk factors for the onset of cigarette smoking (i.e. parents’ smoking, friends’ smoking, psychosocial characteristics) have not changed significantly in decades. Thus, although more than a decade has passed since the AdoQuest study data were collected, the risk factors for early onset have likely also not changed notably and therefore the findings we report continue to be relevant today.
We found that a wide range of sociodemographic, lifestyle, social environmental and psychological factors known to be associated with cannabis use in middle to late adolescence6‑24,44 and with adolescent smoking25 and drinking26 have similar associations with cannabis use at an earlier age. A notable finding in the current study are the associations among Grade 6 children for numerous correlates including use of combustible cigarettes, other tobacco products and alcohol. Although causal inference is limited given the study design, it is possible that the social environmental and psychological risk factors we identified (e.g. friends and siblings smoking, lower parental monitoring, lower self-esteem, depressive symptoms, impulsivity and low school connectedness) signal vulnerabilities underpinning early use of multiple substances that are amenable to intervention. At a minimum, these data suggest that children who report early cannabis use are also at higher risk of early use of combustible cigarettes and alcohol, such that intervention to curb early onset of cannabis use should take polysubstance use into account.
In contrast to reports that parental lifetime and past-year cannabis use was associated with use by adolescents aged 12 to 17 years,44-46 we did not detect an association in the current study. We also found no association between parental smoking, drinking or binge drinking and early cannabis use. It is possible that young children are not yet cognizant of parental substance use so that role modelling of these behaviours is not yet an influence in terms of offspring substance use behaviours. Alternatively, our analyses were simply underpowered to detect these associations (i.e. only 87 parents reported cannabis use and only 40 did not drink alcohol). The relationship between parental substance use behaviours and early cannabis use warrants further study.
Early and frequent cannabis use has long-term implications for outcomes in young adulthood. Specifically, earlier cannabis use is linked to harmful effects on attention, memory and decision-making, and mental health.4,27-32 In addition, cannabis use before age 15 is associated with lower educational attainment; higher frequency of binge drinking, coupled with an increased risk of future alcohol abuse/dependence and greater alcohol-related harms; higher frequency and greater quantity of cannabis consumption and higher risk of cannabis use disorder symptoms; and more frequent use of other illicit drugs by age 30.44 Further, substance use trajectory studies indicate that risky behaviours, which can cluster in youth, are strongly related to substance use and abuse in early adulthood and beyond.47 Our data thus underscore that early cannabis use prevention interventions are critical for vulnerable children who already exhibit signs of engaging in other risky behaviours. Consequently, substance use interventions should be comprehensive, addressing numerous substances and risky behaviours concurrently.
Strengths and limitations
Study strengths include the large population-based sample and the investigation of a wide range of potential risk and protective factors. Limitations include its cross-sectional study design, which limits causal inference, and the use of self-report data, which may have contributed to recall error and/or misclassification bias. Loss to follow-up may have resulted in selection bias.
As the AdoQuest study was not designed as a cannabis use study, some potential correlates such as siblings’ or friends’ cannabis use were not measured. Given the 33 separate potential associations examined, some statistically significant findings may be attributable to chance. However, this seems unlikely as our findings align with those from numerous previous studies. In addition, the sample is 93% White, which may limit generalizability.
Finally, data collection predated legalization of non-medicinal cannabis use in Canada in 2018. However, legalization appears to have had little effect on ever or current (i.e. monthly or more frequently in the past year) cannabis use among Canadian high school students.48 Moreover, the effect of legalization on age at onset is as yet unknown, but it is not likely to have altered factors associated with early use.49
Conclusion
We found that many characteristics associated with cannabis use in mid to late adolescence are also associated with early use. Our findings suggest that surveillance for cannabis use and preventive intervention use are warranted even earlier than age 12. Interventions should incorporate consideration of impulsivity, other risky behaviours (e.g. tobacco use, drinking or gambling) and having friends who smoke as well as encouraging parents/guardians to monitor their children’s whereabouts. Surveillance to detect trends in risk factors is needed because these may differ across study populations or with time.
Future studies should assess early and later predictors of frequency and quantity of cannabis use. Moreover, studies should consider both individual and contextual level correlates or predictors, as illustrated by our finding that higher household income was inversely related to cannabis use after adjusting for weekly spending money, while having more spending money was directly related to cannabis use after adjusting for household income. Finally, replication is critical because different methods across studies can lead to different conclusions. In particular, replication studies using data collected post-legalization are needed to investigate whether risk factors for early cannabis use might have changed since 2018.
Acknowledgements
This project was funded by the Canadian Tobacco Control Research Initiative and the Institut national de sant publique du Qubec (INSPQ) through a financial contribution from the Ministre de la Sant et des Services sociaux to the INSPQ.
JO’L held a Canada Research Chair in the Early Determinants of Adult Chronic Disease 2006-21. M-PS holds a Fonds de Recherche-Sant salary award from the Fonds de Recherche du Qubec. The funders were not involved in the design or conduct of the study, data collection, management, analysis or interpretation or the preparation, review or approval of the manuscript.
We thank Anton Maslov, Senior Epidemiologist/Biostatistician in the Office of Drug Research and Surveillance, Controlled Substances and Cannabis Branch, Health Canada, for analyzing and providing data on age at initiation.
Conflicts of interest
The authors have no financial relationships relevant to this article and no conflicts of interest to disclose.
Authors’ contributions and statement
RJW reviewed the literature, conducted analyses and wrote the first draft.
EKO’L coordinated data collection in the AdoQuest study and conducted analyses.
M-PS consulted on the analytic plan.
END reviewed the literature.
JO’L conceived, obtained funding for and oversaw all aspects of the AdoQuest study.
All authors contributed to conceptualization of the study, interpreted the results, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Views expressed in this document are those of the authors and do not necessarily reflect those of the Ministre de la Sant et des Services sociaux or of the Government of Canada.
References
- Summary of results for the Canadian Student Tobacco, Alcohol and Drugs Survey 2018-19 [Internet] Ottawa(ON): Ottawa (ON): Government of Canada; [modified 2019 Dec 23; cited 2020 Mar 7] Available from: https://www.canada.ca/en/health-canada/services/canadian-student-tobacco-alcohol-drugs-survey/2018-2019-summary.html. [Google Scholar]
- Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME, et al. Monitoring the Future national survey results on drug use, 1975-2019: Overview, key findings on adolescent drug use. Institute for Social Research, University of Michigan. 2020:Overview, key findings on adolescent drug use. [Google Scholar]
- Leatherdale ST, Hammond D, Ahmed R, et al. Alcohol, marijuana, and tobacco use patterns among youth in Canada. Cancer Causes Control. 2008;19((4)):361–9. doi: 10.1007/s10552-007-9095-4. [DOI] [PubMed] [Google Scholar]
- Odgers CL, Caspi A, Nagin DS, et al, et al. Is it important to prevent early exposure to drugs and alcohol among adolescents. Psychol Sci. 2008;19((10)):1037–44. doi: 10.1111/j.1467-9280.2008.02196.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forman-Hoffman VL, Glasheen C, Batts KR, et al. Marijuana use, recent marijuana initiation, and progression to marijuana use disorder among young male and female adolescents aged 12-14 living in US households. Subst Abuse. 2017:1178221817711159–44. doi: 10.1177/1178221817711159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey SL, Hubbard RL, et al. Developmental variation in the context of marijuana initiation among adoles-cents. J Health Soc Behav. 1990;31((1)):58–70. [PubMed] [Google Scholar]
- Tang Z, Orwin RG, et al. Marijuana initiation among American youth and its risks as dynamic processes: prospective findings from a national longitudinal study. Subst Use Misuse. 2009:195–211. doi: 10.1080/10826080802347636. [DOI] [PubMed] [Google Scholar]
- Andrews JA, Hops H, Ary D, Tildesley E, Harris J, et al. Parental influence on early adolescent substance use: specific and nonspecific effects. J Early Adolesc. 1993;13((3)):285–310. [Google Scholar]
- Atherton OE, Conger RD, Ferrer E, Robins RW, et al. Risk and protective factors for early substance use initiation: a longitudinal study of Mexican-origin youth. J Res Adolescence. 2016;26((4)):864–79. doi: 10.1111/jora.12235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brook JS, Kessler RC, Cohen P, et al. The onset of marijuana use from preadolescence and early adolescence to young adulthood. Dev Psychopathol. 1999;11((4)):901–14. doi: 10.1017/s0954579499002370. [DOI] [PubMed] [Google Scholar]
- Brook JS, Lukoff IF, Whiteman M, et al. Initiation into adolescent marijuana use. J Genet Psychol. 1980;137((1)):133–42. doi: 10.1080/00221325.1980.10532808. [DOI] [PubMed] [Google Scholar]
- Coffey C, Lynskey M, Wolfe R, Patton GC, et al. Initiation and progression of cannabis use in a population-based Australian adolescent longitudinal study. Addiction. 2000;95((11)):1679–90. doi: 10.1046/j.1360-0443.2000.951116798.x. [DOI] [PubMed] [Google Scholar]
- D’Amico EJ, McCarthy DM, et al. Escalation and initiation of younger adolescents’ substance use: the impact of perceived peer use. J Adolesc Health. 2006;39((4)):481–7. doi: 10.1016/j.jadohealth.2006.02.010. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Med J, et al. Cannabis use and dependence in a New Zealand birth cohort. N Z Med J. 2000;113((1109)):156–8. [PubMed] [Google Scholar]
- Fergusson DM, Lynskey MT, Horwood LJ, et al. Conduct problems and attention deficit behaviour in middle childhood and cannabis use by age 15. Conduct problems and attention deficit behaviour in middle childhood and cannabis use by age 15. Aust N Z J Psychiatry. 1993:673–82. doi: 10.3109/00048679309075830. [DOI] [PubMed] [Google Scholar]
- Guxens M, Nebot M, Ariza C, et al. Age and sex differences in factors associated with the onset of cannabis use: a cohort study. Drug Alcohol Depend. 2007;88((2-3)):234–43. doi: 10.1016/j.drugalcdep.2006.10.018. [DOI] [PubMed] [Google Scholar]
- Hammer T, Vaglum P, et al. Users and nonusers within a high-risk milieu of cannabis use. Int J Addict. 1991;26((5)):595–604. doi: 10.3109/10826089109058907. [DOI] [PubMed] [Google Scholar]
- Korhonen T, Huizink AC, Dick DM, Pulkkinen L, Rose RJ, Kaprio J, et al. Role of individual, peer and family factors in the use of cannabis and other illicit drugs: a longitudinal analysis among Finnish adolescent twins. Drug Alcohol Depend. 2008;97((1-2)):33–43. doi: 10.1016/j.drugalcdep.2008.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen W, Mastekaasa A, m L, et al. Conduct problems and early cannabis initiation: a longitudinal study of gender differences. Addiction. 2001:415–31. doi: 10.1046/j.1360-0443.2001.9634156.x. [DOI] [PubMed] [Google Scholar]
- Spechler PA, Allgaier N, Chaarani B, et al. The initiation of cannabis use in adolescence is predicted by sex-specific psychosocial and neurobiological features. Eur J Neurosci. 2019;50((3)):2346–56. doi: 10.1111/ejn.13989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bree MB, Pickworth WB, et al. Risk factors predicting changes in marijuana involvement in teenagers. Arch Gen Psychiatry. 2005;62((3)):311–9. doi: 10.1001/archpsyc.62.3.311. [DOI] [PubMed] [Google Scholar]
- Sydow K, Lieb R, Pfister H, fler M, Wittchen HU, et al. What predicts incident use of cannabis and progression to abuse and dependence. Drug Alcohol Depend. 2002:49–64. doi: 10.1016/s0376-8716(02)00102-3. [DOI] [PubMed] [Google Scholar]
- Wade TJ, Pevalin DJ, et al. Adolescent delinquency and health. Can J Criminol Crim Justice. 2005;47((4)):619–54. [Google Scholar]
- Washburn IJ, Capaldi DM, et al. Influences on boys’ marijuana use in high school: a two-part random intercept growth model. J Res Adolesc. 2014:117–30. doi: 10.1111/jora.12030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wellman RJ, Dugas EN, Dutczak H, et al, et al. Predictors of the onset of cigarette smoking: a systematic review of longitudinal population-based studies in youth. Am J Prev Med. 2016:767–78. doi: 10.1016/j.amepre.2016.04.003. [DOI] [PubMed] [Google Scholar]
- Donovan JE, et al. Adolescent alcohol initiation: a review of psychosocial risk factors. J Adolesc Health. 2004:529–78. doi: 10.1016/j.jadohealth.2004.02.003. [DOI] [PubMed] [Google Scholar]
- Levine A, Clemenza K, Rynn M, Lieberman J, et al. Evidence for the risks and consequences of adolescent cannabis exposure. J Am Acad Child Adolesc Psychiatry. 2017;56((3)):214–25. doi: 10.1016/j.jaac.2016.12.014. [DOI] [PubMed] [Google Scholar]
- Meier MH, Caspi A, Ambler A, et al, S A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012;109((40)):E2657–64. doi: 10.1073/pnas.1206820109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fischer B, Russell C, Sabioni P, et al, et al. Lower-risk cannabis use guidelines: a comprehensive update of evidence and recommendations. Am J Public Health. 2017;107((8)):e1–12. doi: 10.2105/AJPH.2017.303818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saxena S, Poznyak V, m M, Gehring E, Rekve D, et al. World Health Organization. Geneva(CH): The health and social effects of nonmedical cannabis use. Available from: https://apps.who.int/iris/bitstream/handle/10665/251056/9789241510240-eng.pdf?sequence=1&isAllowed;=y. [Google Scholar]
- Chadwick B, Miller ML, Hurd YL, et al. Cannabis use during adolescent development: susceptibility to psychiatric illness. Front Psychiatry. 2013 doi: 10.3389/fpsyt.2013.00129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynskey MT, Heath AC, Bucholz KK, et al, users vs, et al. Escalation of drug use in early-onset cannabis users vs. JAMA. 2003;289((4)):427–33. doi: 10.1001/jama.289.4.427. [DOI] [PubMed] [Google Scholar]
- La carte de la population scolaire et les indices de dfavorisation. Qubec Ministre de l’ducation. :1e9–33. Available from: http://www.education.gouv.qc.ca/fileadmin/site_web/documents/PSG/statistiques_info_decisionnelle/bulletin_26.pdf. [Google Scholar]
- Paradis G, Lambert M, O’Loughlin J, et al, et al. The Qubec Child and Adolescent Health and Social Survey: design and methods of a cardiovascular risk factor survey for youth. Can J Cardiol. 2003;19((5)):523–31. [PubMed] [Google Scholar]
- Elton-Marshall T, Leatherdale ST, Manske SR, Wong K, Ahmed R, Burkhalter R, et al. Research methods of the Youth Smoking Survey (YSS) Chronic Dis Inj Can. 2011;32((1)):47–54. [PubMed] [Google Scholar]
- Patton GC, McMorris BJ, Toumbourou JW, Hemphill SA, Donath S, Catalano RF, et al. Puberty and the onset of substance use and abuse. Pediatrics. 2004:e300–6. doi: 10.1542/peds.2003-0626-F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris TP, White IR, et al. Tuning multiple imputation by predictive mean matching and local residual draws. BMC Med Res Methodol. 2014;14((1)):75–6. doi: 10.1186/1471-2288-14-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hippel PT, et al. How many imputations do you need. Sociol Methods Res. 2020;49((3)):699–718. [Google Scholar]
- Bender R, Lange S, et al. Adjusting for multiple testing—when and how. J Clin Epidemiol. 2001;54((4)):343–9. doi: 10.1016/s0895-4356(00)00314-0. [DOI] [PubMed] [Google Scholar]
- Westreich D, Greenland S, et al. The Table 2 fallacy: presenting and interpreting confounder and modifier coefficients. Am J Epidemiol. 2013;177((4)):292–8. doi: 10.1093/aje/kws412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schisterman EF, Cole SR, Platt RW, et al. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. 2009;20((4)):488–95. doi: 10.1097/EDE.0b013e3181a819a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams RL, et al. A note on robust variance estimation for cluster-correlated data. Biometrics. 2000;56((2)):645–6. doi: 10.1111/j.0006-341x.2000.00645.x. [DOI] [PubMed] [Google Scholar]
- Vandenbrouke JP, Elm E, Altman DG, et al, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4((10)):e297–6. doi: 10.1371/journal.pmed.0040297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merrin GJ, Leadbeater BJ, Sturgess CM, Ames ME, Thompson K, et al. Predictors of early-onset cannabis use in adolescence and risks for substance use disorder symptoms in young adulthood. J Drug Issues. 2022;52((2)):182–206. [Google Scholar]
- Madras BK, Han B, Compton WM, Jones CM, Lopez EL, McCance-Katz EF, et al. Associations of parental marijuana use with offspring marijuana, tobacco, and alcohol use and opioid misuse. JAMA Netw Open. 2019:e1916015–206. doi: 10.1001/jamanetworkopen.2019.16015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Loughlin JL, Dugas EN, O’Loughlin EK, et al, et al. Parental cannabis use is associated with cannabis initiation and use in offspring. J Pediatr. 2019:142–7. doi: 10.1016/j.jpeds.2018.10.057. [DOI] [PubMed] [Google Scholar]
- Taylor M, Collin SM, MacLeod J, Hickman M, Heron J, et al. Patterns of cannabis use during adolescence and their association with harmful substance use behaviour: findings from a UK birth cohort. J Epidemiol Community Health. 2017:764–70. doi: 10.1136/jech-2016-208503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuckermann AM, Battista KV, langer RE, et al, et al. Trends in youth cannabis use across cannabis legalization: data from the COMPASS prospective cohort study. Prev Med Rep. 2021;22((4)):101351–70. doi: 10.1016/j.pmedr.2021.101351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melchior M, Nakamura A, Bolze C, et al, et al. Does liberalisation of cannabis policy influence levels of use in adolescents and young adults. BMJ Open. 2019;9((7)):e025880–70. doi: 10.1136/bmjopen-2018-025880. [DOI] [PMC free article] [PubMed] [Google Scholar]