

Abstract
Objective
This cross-sequential study examines whether the coronavirus disease 2019 pandemic affected the mental health of staff working at an Australian air medical service, the Royal Flying Doctors Service South Eastern (RFDSSE) Section.
Methods
The risk of anxiety and depression was measured using a prospective anonymized online survey using the Hospital Anxiety and Depression Scale, which was answered by 119 employees. This cross-sequential study was completed in December 2021 with reference to 2 time points: now and the beginning of the pandemic. A high risk of anxiety was defined using a Hospital Anxiety and Depression Scale score of 11 to 21 (low risk: 0-10). Chi-square testing was used to compare subgroups at single time points. McNemar testing was used to compare the risk of anxiety and depression between the beginning of the pandemic and December 2021.
Results
Employees recalled a higher risk of anxiety at the beginning of the pandemic (29%) compared with December 2021 (16%) (P = .012). At the beginning of the pandemic, nonoperational staff members were more anxious than operational staff (P = .019). One third (31%) of operational staff members were concerned about dying at the beginning of the pandemic.
Conclusion
Our findings demonstrate that RFDSSE employees recalled higher levels of anxiety at the beginning of the pandemic compared with their risk in December 2021. Operational and nonoperational staff have different mental health needs; anxiety experienced by nonoperational staff during a pandemic should not be underestimated. The overall prevalence of anxiety and depression is high, suggesting health care staff in an air medical service may require extra psychological support. Other air medical organizations may reflect on our study findings and plan how to better support their own staff as a result.
Health care workers around the world have been put under a huge strain during the coronavirus disease 2019 (COVID-19) pandemic in the challenge to control and treat the virus. At the time of writing in June 2022, the World Health Organization reported over 542 million infections and over 6.3 million deaths since the beginning of the pandemic.1 Numerous studies conducted globally during the COVID-19 pandemic2, 3, 4 and previous pandemics5 suggested health care workers are at risk of experiencing poorer mental health during an outbreak. A recent rapid review found multiple studies estimating the prevalence of mental health problems in health care workers during the coronavirus outbreak. Estimates varied from 12% to 45% for anxiety in 1 study and from 28% to 51% for depression. Between 11% and 73% of health care workers reported posttraumatic stress disorder.6 A recent meta-analysis reported an overall prevalence of anxiety of 43% and depression of 45% among frontline health care workers during the COVID-19 pandemic.7 Another study suggested that 33% of health care workers exposed to COVID-19 reported depressive symptoms and 42% anxiety features, with 32% displaying posttraumatic symptoms.8
Prepandemic, the Australian Bureau of Statistics9 reported the prevalence of anxiety as 14.4% and depression as 6.2% in Australia. Comparatively, the most recent National Study of Mental Health and Wellbeing from the Australian Bureau of Statistics was conducted between December 2020 and July 2021 during the COVID-19 pandemic, and initiatives were in place during this time to reduce the spread of COVID-19, including border control for some states and territories, stay-at-home orders, and social distancing; 16.8% of the general population had an anxiety disorder in the 12 months before this survey, and 7.5% had an affective (mood) disorder in the preceding 12 months.10 The prevalence of anxiety and depression among health care workers tends to be higher than the general population. Consequences of psychological distress or burnout include low commitment to organization and increased turnover of skilled staff11 and can be financially costly for an organization.12 Crucially, poor staff mental health can negatively impact patient satisfaction13 and the quality of patient care.14
However, risk factors for mental distress have been conflicting.15, 16, 17, 18 A 2021 Belgian study19 demonstrated a high prevalence of anxiety and depression among health care workers but found no differences between those working with COVID-19 patients and those who did not. Conversely, a different rapid review suggested that COVID-19 had a considerable impact on the psychological well-being of frontline hospital staff.20 Previous literature focused on the psychological impact on frontline hospital staff in the context of the pandemic2, 3, 4, 5, 6 , 20; there is minimal literature addressing the effect of COVID-19 on those working in air medical or retrieval services or in remote and rural locations. In addition, many studies are from Europe, North America, or China,2 , 3 , 5 , 6 , 9 , 13 , 19 , 20 which have had an entirely different experience of the pandemic compared with Australia.21 In February, March, and April 2020, there were rapidly rising COVID-19 case numbers worldwide22 and news of health care staff dying as a result,23 but there were very few case numbers in Australia24 and very limited knowledge about the disease.25 By December 2021, a prolonged lockdown was finally being lifted in New South Wales (NSW), case numbers were dropping, and vaccination was more widespread.26
The Royal Flying Doctors Service South Eastern (RFDSSE) Section is a not-for-profit charitable medical service. The RFDSSE provides clinical services to a geographic area of nearly 700,000 km2 including west and far west NSW, northern South Australia, and southwestern Queensland. The area is considered remote or rural, with a Modified Monash Model classification ranging from 3 to 7.27 Clinical services include retrieval and emergency services, primary health services including general practitioners and nursing, mental health services, alcohol and drug services, and dental services. The RFDSSE has also contributed greatly to the public health response to the COVID-19 pandemic by conducting vaccination clinics and transferring critically unwell patients, including ventilated patients with COVID-19. The RFDSSE has 2 main bases in Dubbo and Broken Hill but also has staff working around NSW (including Sydney) and in Launceston. The RFDSSE has a confidential employer-funded support service available to staff and volunteers experiencing personal or work-related concerns known as the Employee Assistance Program (EAP).
Air medical retrieval organizations are unique working environments that continue to provide essential health care to rural and remote communities throughout the COVID-19 pandemic. Little is understood about working in this type of environment and the effect on the mental health of this critical workforce. Providing appropriate mental health support for workers has benefits that also extend to patients. This study examines 2 specific RDFSSE staff groups: operational and nonoperational. The operational staff group is composed of patient-facing staff, which includes clinical staff (eg, retrieval physicians, general practitioners, and nurses) and pilots. Pilots have the potential to be exposed to COVID-19 as a result of their work because they are in the confined space of the airplane with patients like clinical staff. Nonoperational staff are nonclinical staff (ie, those working in communications, human resources, airplane engineers, management, and charity fundraising staff) who are not exposed to patients with COVID-19 as part of their role.
The aim of this study was to identify whether different time points in the pandemic affected the risk of anxiety or depression in staff working for an air medical organization as assessed by the Hospital Anxiety and Depression Scale (HADS). This study also questioned whether the risk of anxiety or depression depends on whether staff are operational or nonoperational. We wished to elucidate whether any other demographics (eg, age, sex, or work location) led to an increased or reduced risk of anxiety or depression. Finally, we wished to identify key concerns for RDFSSE staff members and whether the aircraft is perceived as a high-risk workplace.
Methods
Ethics
This study was approved by the Human Research Ethics Committee of The University of Sydney (approval no. 2021/895) according to the National Statement on Ethical Conduct in Human Research (2007).
Study Design
We conducted a prospective cross-sequential survey of all staff members at RFDSSE. This study design was chosen to give rapid information about the impact of the pandemic and included both cross-sectional and longitudinal elements. The survey was distributed to all RFDSSE staff via e-mail on December 7, 2021. It contained a link to the questionnaire and a participant information sheet. Informed consent was gained by asking participants to verify that they had read the participant information sheet and then consent by clicking “Yes–I have read the participant information sheet and consent to participating in this study” or refuse by clicking “No–I do not consent to participating in this study.” The time frame for data collection was 3 weeks. Two reminder e-mails were sent over this period. Data were anonymized at the time of collection. All current RFDSSE employees were eligible and invited to participate.
Participants
All current employees of RFDSSE (at this time 488 employees in total) were eligible for the study and were invited to participate.
Variables
The primary outcome was whether different time points in the pandemic affected the risk of anxiety or depression as assessed by the HADS questionnaire. RFDSSE staff completed the HADS questionnaire with respect to the time of survey completion (December 2021) and recalling how they felt at the beginning of the pandemic (around March 2020).
The secondary outcome was subgroup analysis of the following questions:
-
1.
Is the risk of anxiety or depression higher in particular demographics? We specifically reviewed operational compared with nonoperational staff, age (over 40 years vs. under 40 years), location, and sex.
-
2.
Is working in an aircraft perceived as higher risk for contracting COVID-19?
-
3.
What main worries do RFDSSE staff members have? These were 4 specific questions to try to identify participants’ main pandemic-related concerns that may affect them via exposure through work. These included “I am worried about contracting COVID-19 through work and becoming unwell,” “I am worried about contracting COVID-19 through work and dying,” “I am worried about passing COVID-19 to friends and family through work, and that they might become unwell or die as a result,” and “I am worried about COVID-19 affecting my lifestyle.”
Data Measurement
The risk of anxiety and depression was assessed using HADS, a reliable self-report questionnaire that has been validated in many languages, countries, and settings.28, 29, 30 The HADS questionnaire is useful for an initial diagnosis and to track progression (or resolution) of psychological symptoms. It consists of 2 independent subscales: anxiety (HADS-A; sample item: “Worrying thoughts go through my mind”) and depression (HADS-D; sample item: “I have lost interest in my appearance”). In a review of 747 studies using the HADS questionnaire, reliability using the Cronbach alpha for HADS-A was between .68 and .93 (mean = .83), and for HADS-D it ranged from .67 to .90 (mean = .82). The sensitivity and specificity for both HADS-A and HADS-D were found to be approximately 0.80.31 Each subscale contains 7 items scored on a 4-point Likert scale with a total score between 0 and 21 for either anxiety or depression. In the original HADS, a score of 0 to 7 is considered low risk, 8 to 10 borderline, and 11 to 21 high risk. We chose to compare scores 0 to 10 with scores 11 to 21 in order to minimize false-positive identification of anxiety or depression by accepting a borderline score as high risk. Of note, a cross-sectional survey was performed in December 2021, and participants were also asked to recall how they felt at the beginning of the pandemic (March 2020). The latter measured the participants’ memory of how anxious or depressed they were at this time.
Statistical Methods
Data were analyzed using descriptive statistics with Excel (Microsoft, Redmond, WA) and GraphPad Prism (GraphPad Software, San Diego, CA). Chi-square testing was used to compare subgroups at single time points, including the comparison of operational and nonoperational staff, age, location, and sex. McNemar testing was used to compare the risk of anxiety and depression between the beginning of the pandemic and December 2021. The significance level was P < .05. For chi-square testing comparing 3 categories (ie, locations Dubbo, Broken Hill, and other), the significance level was P < .017 using the Bonferroni correction.
Results
The survey invitation e-mail was sent to 488 people. Survey responses were analyzed, with 119 completing HADS in full. Of the 119 participants, 114 participants completed the HADS questionnaire and all the required demographic data (Fig. 1 ).
Figure 1.
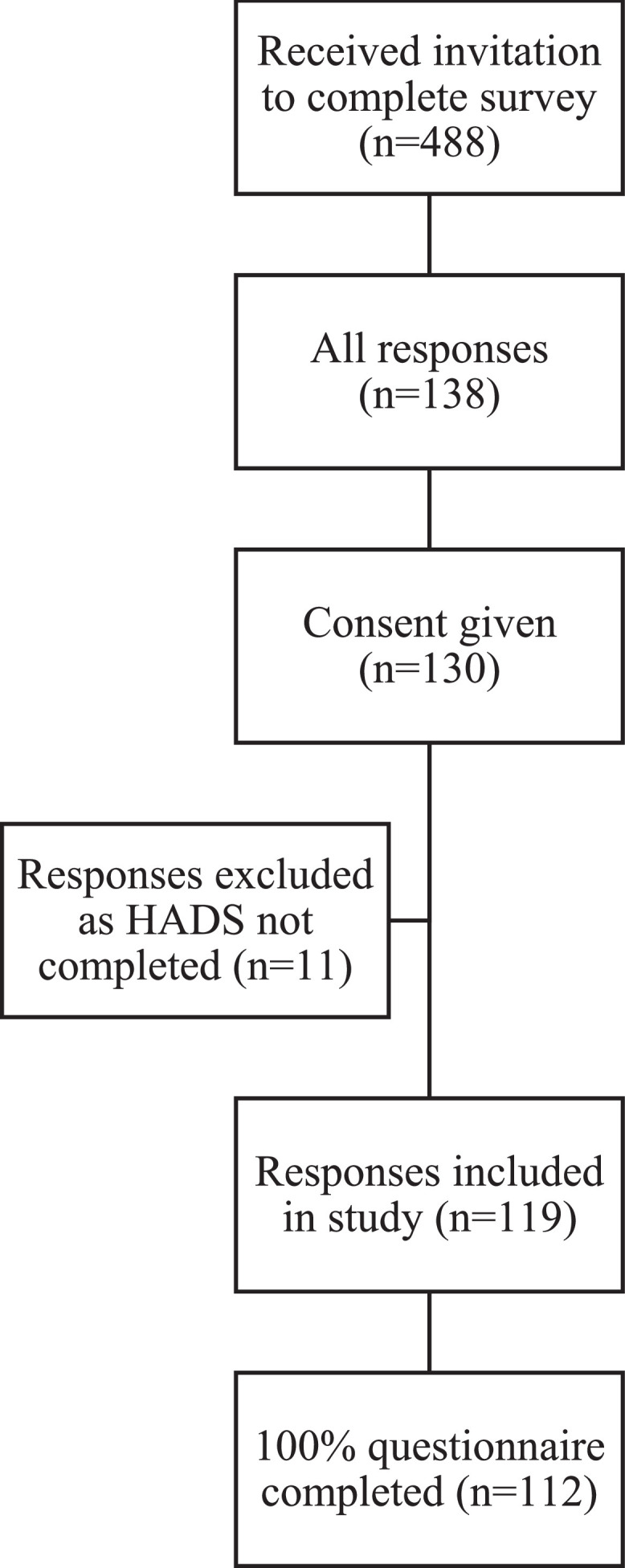
A flowchart illustrating the proportion of RFDSSE staff who consented to participate in the study and the proportion of responses included and analyzed.
Of the 119 responding participants, 61 (51.3%) were operational, and 53 (44.5%) were nonoperational. The mean age of respondents was 44.3 years. Men represented 42% of the respondents, and women represented 52.9% (Table 1 ).
Table 1.
Demographic Characteristics of the Royal Flying Doctors Service South Eastern Staff Members Who Completed the Hospital Anxiety and Depression Scale (N = 119)
| Demographic Category | Operational Staff, N (% of All Respondents) | Nonoperational Staff, N (% of all respondents) | Job Role Not Declared, N (% of All Respondents) | Total |
|---|---|---|---|---|
| Total | 61 (51.3) | 53 (44.5) | 5 (4.2) | 119 (100) |
| Age, y | ||||
| < 40 | 28 (23.5) | 21 (17.6) | 0 (0) | 49 (41.2) |
| ≥ 40 | 32 (26.9) | 31 (26.1) | 0 (0) | 63 (52.9) |
| Age not declared | 1 (0.8) | 1 (0.8) | 5 (4.2) | 7 (5.8) |
| Work location | ||||
| Dubbo | 29 (24.4) | 19 (16.0) | 0 (0) | 48 (40.3) |
| Broken Hill | 20 (16.8) | 13 (10.9) | 0 (0) | 33 (27.7) |
| Other location | 11 (9.2) | 20 (16.8) | 0 (0) | 31 (26.1) |
| Location not declared | 1 (0.8) | 1 (0.8) | 5 (4.2) | 7 (5.8) |
| Sex | ||||
| Female | 30 (25.2) | 33 (27.7) | 0 (0) | 63 (52.9) |
| Male | 30 (25.2) | 20 (16.8) | 0 (0) | 50 (42.0) |
| Sex not declared | 1 (0.8) | 0 (0) | 5 (4.2) | 6 (5.0) |
Almost one third (29.4%) of all RFDSSE staff members recalled a high risk of anxiety at the beginning of the pandemic compared with 16% in December 2021 (χ2 1 = 6.25, P = .012). This was true for the nonoperational subgroup in which 39.6% reported high levels of anxiety at the beginning compared with 17.0% in December 2021 (χ2 1 = 9.38, P = .002) but not for the operational subgroup in which 19.7% reported high scores at the beginning and 16.4% in December 2021 (χ2 1 = 0.00, P = 1.00). The risk of anxiety was higher in nonoperational staff (21%) compared with operational staff (12%) (χ2 1 = 5.49, P = 0.019) at the beginning of the pandemic. In December 2021, there was no difference (χ2 1 = 0.01, P = .933) between the 2 groups (Table 2 ).
Table 2.
Risk of Anxiety in Royal Flying Doctors Service South Eastern Staff Members at the Beginning of the Coronavirus Disease 2019 Pandemic and in December 2021 Assessed Using the Hospital Anxiety and Depression Scale (HADS)
| Staff Member Role | Risk of Anxiety at Beginning of Pandemic | Risk of Anxiety In December 2021 | Change in Risk of Anxiety, McNemar Test |
|---|---|---|---|
| Total | N (% of total) | N (% of total) | N = 119, P = .012 |
| All staff low score (HADS 0-10) | 84 (70.6) | 100 (84.0) | |
| All staff high score (HADS 11-21) | 35 (29.4) | 19 (16.0) | |
| Job role not declared | n (% of staff member role type) | n (% of staff member role type) | Insufficient numbers to test |
| Low score (HADS 0-10) | 3 (60.0) | 5 (100.0) | |
| High score (HADS 11-21) | 2 (40.0) | 0 (0.0) | |
| Nonoperational staff | n (% of staff member role type) | n (% of staff member role type) | n = 53, P = .002 |
| Low score (HADS 0-10) | 32 (60.4) | 44 (83.0) | |
| High score (HADS 11-21) | 21 (39.6) | 9 (17.0) | |
| Operational staff | n (% of staff member role type) | n (% of staff member role type) | n = 61, P = 1.00 |
| Low score (HADS 0-10) | 49 (80.3) | 51 (83.6) | |
| High score (HADS 11-21) | 12 (19.7) | 10 (16.4) | |
| Comparison of operational and nonoperational staff, chi-square test | n = 114, P = .019 | n = 114, P = .933 |
Comparison of time points (beginning of pandemic and December 2021) using the McNemar test, N =119 (all respondents who completed the HADS in full). Comparison of operational and nonoperational staff using the chi-square test, n = 114 (respondents who completed HADS in full and declared their job role).
There was no evidence of differences in recalled depression risk at the beginning of the pandemic (23.2%) compared with December 2021 (20.2%) for all staff (χ2 1 = 0.25, P = .617), the operational subgroup (χ2 1 = 0.41, P = .522), or the nonoperational subgroup (χ2 1 = 2.08, P = .149). There was no difference in depression risk between operational and nonoperational staff members at the beginning of the pandemic (χ2 1 = 0.03, P = 0.864) or in December 2021 (χ2 1 = 0.02, P = .886) (Table 3 ). Age, work location, and sex did not affect the risk of anxiety or depression in this study (Table 4 ).
Table 3.
Risk of Depression in Royal Flying Doctors Service South Eastern Staff Members at the Beginning of the Coronavirus Disease 2019 Pandemic and in December 2021 Assessed Using the Hospital Anxiety and Depression Scale (HADS)
| Staff Member Role | Risk of Depression at Beginning of Pandemic | Risk of Depression in December 2021 | Change in Risk of Depression, McNemar Test |
|---|---|---|---|
| Total | n (% of total) | n (% of total) | N = 119, P = .617 |
| Total staff low score (HADS 0-10) | 91 (76.5) | 95 (79.8) | |
| Total staff high score (HADS 11-21) | 28 (23.5) | 24 (20.2) | |
| Job role not declared | n (% of staff member role type) | n (% of staff member role type) | Insufficient numbers to test |
| Low score (HADS 0-10) | 2 (40.0) | 4 (80.0) | |
| High score (HADS 11-21) | 3 (60.0) | 1 (20.0) | |
| Operational staff | n (% of staff member role type) | n (% of staff member role type) | n = 61, P = .522 |
| Low score (HADS 0-10) | 48 (78.7) | 49 (80.3) | |
| High score (HADS 11-21) | 13 (21.3) | 12 (19.7) | |
| Nonoperational staff | n (% of staff member role type) | n (% of staff member role type) | n = 53, P = .149 |
| Low score (HADS 0-10) | 41 (77.4) | 42 (79.2) | |
| High score (HADS 11-21) | 12 (22.6) | 11 (20.8) | |
| Comparison of operational and nonoperational staff, chi-square test | n = 114, P = .864 | n = 114, P = .886 |
Comparison of time points (beginning of pandemic and December 2021) using the McNemar test, N = 119 (all respondents who completed the HADS in full). Comparison of operational and nonoperational staff using the chi-square test, n = 114 (respondents who completed HADS in full and declared their job role).
Table 4.
Risk of Anxiety and Depression Using the Hospital Anxiety and Depression Scale (HADS) for Royal Flying Doctors Service Staff Comparing Age Groups, Locations, and Sex
| Demographic Category | Risk of Anxiety at Beginning of Pandemic | Risk of Anxiety in December 2021 | Risk of Depression at Beginning of Pandemic | Risk of Depression in December 2021 |
|---|---|---|---|---|
| Age < 40 y | n (% of age category) | n (% of age category) | n (% of age category) | n (% of age category) |
| Low score (HADS 0-10) | 34 (69.4) | 41 (83.7) | 39 (79.6) | 42 (85.7) |
| High score (HADS 11-21) | 15 (30.6) | 8 (16.3) | 10 (20.4) | 7 (14.3) |
| Age ≥ 40 y | ||||
| Low score (HADS 0-10) | 46 (73.0) | 53 (84.1) | 49 (77.8) | 48 (76.2) |
| High score (HADS 11-21) | 17 (27.0) | 10 (15.9) | 14 (22.2) | 15 (23.8) |
| Comparison of age < 40 y and age ≥ 40 y, chi-square test | n = 112, P = .673 | n = 112, P = .948 | n = 112, P = .816 | n = 112, P = .208 |
| Location Dubbo | n (% of location category) | n (% of location category) | n (% of location category) | n (% of location category) |
| Low score (HADS 0-10) | 33 (68.8) | 42 (87.5) | 37 (77.1) | 41 (85.4) |
| High score (HADS 11-21) | 15 (31.3) | 6 (12.5) | 11 (22.9) | 7 (14.6) |
| Location Broken Hill | ||||
| Low score (HADS 0-10) | 24 (72.7) | 26 (78.8) | 26 (78.7) | 24 (72.7) |
| High score (HADS 11-21) | 9 (27.3) | 7 (21.2) | 7 (21.2) | 9 (27.3) |
| Location other | ||||
| Low score (HADS 0-10) | 22 (71.0) | 26 (83.9) | 24 (77.4) | 25 (80.6) |
| High score (HADS 11-21) | 9 (29.0) | 5 (16.1) | 7 (22.6) | 6 (19.4) |
| Comparison of location, chi-square test | n = 112, P = .926 | n = 112, P = .577 | n = 112, P = .983 | n = 112, P = .368 |
| Sex: female | n (% of sex category) | n (% of sex category) | n (% of sex category) | n (% of sex category) |
| Low score (HADS 0-10) | 42 (66.7) | 55 (87.3) | 50 (79.4) | 54 (85.7) |
| High score (HADS 11-21) | 21 (33.3) | 8 (12.7) | 13 (20.6) | 9 (14.3) |
| Sex: male | ||||
| Low score (HADS 0-10) | 38 (76.0) | 40 (80.0) | 38 (76.0) | 37 (74.0) |
| High score (HADS 11-21) | 12 (24.0) | 10 (20.0) | 12 (24.0) | 13 (26.0) |
| Comparison of male and female, chi-square test | n = 113, P = .278 | n = 113, P = .292 | n = 113, P = .669 | n = 113, P = .118 |
Comparison of age, work location, and sex using the chi-square test.
Almost half (47.9%) of the RFDSSE staff overall felt that the confined space of the plane put them at higher risk of contracting COVID-19. This increased to 73.8% in the operational staff subgroup. Comparatively, 41.9% felt that the confined space of the office put them at higher risk of contracting COVID-19. At the beginning of the pandemic, 31% of operational staff agreed with the following statement: “I am worried about contracting COVID-19 through work and dying.” RFDSSE staff members were generally more worried at the beginning of the pandemic about becoming unwell (χ2 1 = 8.50, P = .004), dying (χ2 1 = 12.19, P = .001), and passing COVID-19 to friends or family (χ2 1 = 10.23, P = .001) compared with in December 2021. Operational staff members were more concerned than nonoperational staff about passing COVID-19 to friends and family (χ2 1 = 6.36, P = .012). “I am worried about COVID-19 affecting my lifestyle” was a major concern for both operational and nonoperational staff at both time points; 77.2% agreed with this statement at the beginning of the pandemic, and 72.8% still agreed with it in December 2021 (Table 5 ).
Table 5.
Royal Flying Doctors Service South Eastern Staff Members’ Worries and Concerns During the Coronavirus Disease 2019 (COVID-19) Pandemic
| Statements About Worries | Beginning of Pandemic |
December 2021 |
Comparison of Beginning Versus December 2021, McNemar Test | ||
|---|---|---|---|---|---|
| Agree, n (% of Row Total) | Total, N | Agree, n (% of Row Total) | Total, N | ||
| “I am worried about contracting COVID-19 through work and becoming unwell.” | P = .004 | ||||
| Operational staff | 40 (65.6) | 61 | 25 (41.0) | 61 | |
| Nonoperational staff | 28 (52.8) | 53 | 25 (47.2) | 53 | |
| Total | 68 (59.6) | 114 | 50 (43.9) | 114 | |
| Comparison between operational and nonoperational staff, chi-square test | P = .167 | P = .507 | |||
| “I am worried about contracting COVID-19 through work and dying.” | P = .001 | ||||
| Operational staff | 19 (31.1) | 61 | 5 (8.2) | 61 | |
| Nonoperational staff | 10 (18.9) | 53 | 7 (13.2) | 53 | |
| Total | 29 (25.4) | 114 | 12 (10.5) | 114 | |
| Comparison between operational and nonoperational staff, chi-square test | P = .133 | P = .385 | |||
| “I am worried about passing COVID-19 to friends and family through work, and that they might become unwell or die as a result.” | P = .001 | ||||
| Operational staff | 47 (77.0) | 61 | 37 (60.7) | 61 | |
| Nonoperational staff | 29 (54.7) | 53 | 23 (43.4) | 53 | |
| Total | 76 (66.7) | 114 | 60 (52.6) | 114 | |
| Comparison between operational and nonoperational staff, chi-square test | P = .012 | P = .066 | |||
| “I am worried about COVID-19 affecting my lifestyle.” | P = .383 | ||||
| Operational staff | 49 (80.3) | 61 | 45 (73.8) | 61 | |
| Non-operational staff | 39 (73.6) | 53 | 38 (71.7) | 53 | |
| Total | 88 (77.2) | 114 | 83 (72.8) | 114 | |
| Comparison between operational and nonoperational staff, chi-square test | P = .392 | P = .804 | |||
Comparison of time points (beginning of pandemic and December 2021) using the McNemar test and comparison of operational and nonoperational staff using the chi-square test. N = 114 for both the McNemar and chi-square tests (all respondents who completed questions about their worries).
Discussion
This study used a validated tool to assess the risk of anxiety and depression in an air medical retrieval workforce. Participants’ recalled responses suggested a higher risk of anxiety at the beginning of the pandemic compared with December 2021. This was true overall and also for the nonoperational subgroup. The risk of anxiety was higher in nonoperational staff compared with operational staff at the beginning of the pandemic, although by December 2021 this was no longer the case. The risk of depression did not change over the course of the pandemic and was not significantly different between operational and nonoperational staff. RFDSSE staff members were generally more worried at the beginning of the pandemic about becoming unwell, dying, and passing COVID-19 to friends or family compared with December 2021.
There were multiple pandemic, policy, and societal changes globally between the beginning of the pandemic and December 2021. In February, March, and April 2020 (the “beginning of the pandemic”), the pathogenesis and disease process of COVID-19 was largely unknown,25 and news coverage of the devastation in Europe and North America was widespread. There were health care staff members dying in China, Europe, and North America23 in the context of an unvaccinated population. However, there were very few case numbers in Australia at this time.22 , 24 By October 2021 (when this study underwent ethical review), knowledge about the disease had increased, there were more case numbers, and NSW had been in prolonged lockdown for months with international and state border closures.26 Finally, at the time of participant survey completion (December 2021), lockdown was in the process of being lifted, cases were on their way down, and a larger proportion of the community had been vaccinated. These factors taken together may explain why a larger proportion of RFDSSE staff recalled feeling more anxious at the beginning of the pandemic compared with December 2021. Because the particular time point within a pandemic may affect the risk of anxiety for staff members working in an air medical setting, similar services should reflect on how to provide extra psychological support to staff at these particular times of stress and increased workload.
The risk of anxiety may have been lower in operational staff at the beginning of the pandemic (12%) compared with nonoperational staff (21%) because they were more likely to have medical knowledge, which may have been a protective factor. Although both groups witnessed the widespread international devastation caused by the pandemic in the news, operational staff members are predominantly clinical and therefore had prior knowledge on how viruses are usually transmitted as well as the ability to interpret the (limited) primary data sources available. This suggests that operational and nonoperational staff may require differing, albeit complementary, levels of support during a pandemic. Anxiety experienced by nonoperational staff should not be underestimated by air medical services.
Although there were differences found between the subgroups, it is crucial to note that the overall risk of anxiety and depression in this study is higher than in the general population both prepandemic and during the pandemic.9 , 10 At the beginning of the pandemic, nearly 1 in 3 staff members were at high risk of anxiety, and approximately 1 in 5 staff members were at high risk of depression. This is comparable to that found in other studies of Australian (hospital) health care workers during the pandemic4 and is in fact lower than some global estimates of anxiety (43%7 and 42%8) and depression (45%7 and 33%8) among frontline health care workers during the pandemic from recent meta-analyses . However, it is still startlingly high compared with the general population, particularly with regard to affective disorders (the general population Australian peripandemic incidence of an affective disorder was 7.5%10 compared with the 20%-23% found in this study).
The RFDSSE currently funds a support service for staff members (EAP). They have a team of psychologists who provide a confidential support and counseling service for RFDSSE staff, immediate family, and volunteers experiencing personal or work-related concerns. We presented a summary of the results of this study and subsequent recommendations to the RFDSSE executive team to aid in improved support of employees during the pandemic. These recommendations were collated from participants’ free-text responses to the questionnaire and included an immediate review of the EAP to assess fitness for purpose, review of working from home and fatigue management policies, and review of shared housing. In addition, we suggested regular communication between the executive team and other staff members, including using internal expertise on health matters to improve health literacy on COVID-19 across the workforce as a method to improve anxiety related to the pandemic.
However, air medical organizations may consider additional options to support staff given the high burden of anxiety and depression evident in the workforce. This may include reasonable adjustments to meet individual workers’ needs and effective broader organizational strategies to create an inclusive and flexible workplace. Along with benefits to staff, there are a myriad of potential benefits to the service of improved staff mental health (eg, improved skilled staff retention).11 Furthermore, it is potentially cost-effective because of reduced sickness leave as a result of mental illness,12 although cost efficiency is controversial because initiatives themselves may be costly.32 This is an important consideration, particularly in air medical services that tend to have significantly fewer employees compared with larger organizations such as hospitals. Crucially, extrapolating from hospital-based research, poor staff mental health is likely to have a negative effect on patient outcomes.14 These data are useful to other air medical organizations worldwide in general and particularly when planning for future pandemic situations.
At the beginning of the pandemic, operational staff members were more worried than nonoperational staff about passing COVID-19 to friends and family and that loved ones might become unwell and die as a result (Table 5). Operational staff members are by definition exposed to patients with COVID-19 as part of their work and are potentially in close proximity. The majority of operational staff felt that the confined space of the plane placed them at higher risk of contracting COVID-19, and at the beginning of the pandemic, 31% of operational staff agreed with the following statement: “I am worried about contracting COVID-19 through work and dying.” The fact that almost one third of operational staff feared death as a consequence of their work is shocking and may reflect news reports of numerous health care staff dying worldwide23 at this time.
RFDSSE staff recalled being significantly more worried at the beginning of the pandemic about becoming unwell, dying, and passing COVID-19 to friends or family compared with December 2021 (Table 5). “I am worried about COVID-19 affecting my lifestyle” was a major concern for both operational and nonoperational staff at both time points. This is unsurprising because border closures within Australia and internationally resulted in restricted travel, and even by December 2021, restrictions were still not fully eased.26 Furthermore, Australia generally and NSW specifically were still reeling from the memory of a harsh lockdown.
Two limitations of this study must be acknowledged. Although 130 staff members (27% of the workforce) consented to participate in the survey, 119 (24%) completed a sufficient proportion of the survey for their response to be eligible for analysis. A low response rate is a typical issue for online surveys targeting health care professionals.33 This may be because of survey fatigue or fear of identification within the workplace (despite immediate anonymization of data, secure storage, and assurance of anonymization to potential participants) because RFDSSE is a relatively small organization. Many people are wary of discussing their mental health, particularly in a context related to their work. However, the data remain relevant and important; this study is the first time that the psychological impact of the COVID-19 pandemic has been undertaken in the context of staff working in an air medical service, and it has implications for other retrieval services globally. Second, there was a potential for recall bias because we required participants to remember how they felt at the beginning of the pandemic when answering the HADS questionnaire; this measures the participants’ memory of how anxious they were at that time. This may have minimized or exaggerated the potential effects found. Mechanisms including adaptation, learning, and potential development of coping mechanisms may have affected the way that participants remember that time and may have contributed to the demonstrated reduction in anxiety over the course of the pandemic. However, the inclusion of the earlier time point was crucial to ascertain our primary outcome.
Conclusion
Our findings demonstrated that RFDSSE employees recalled higher levels of anxiety at the beginning of the pandemic compared with their risk in December 2021. This may be a response to the changes in COVID-19 prevalence and policy over this period. We demonstrated that operational and nonoperational staff have different mental health needs, and this should guide future RFDSSE executive policy. Other air medical organizations can use our study to reflect and plan how to support their own staff, particularly noting that anxiety experienced by nonoperational staff should not be underestimated. The overall risk of anxiety and depression in this study is similar to that found in other studies of Australian (hospital) health care workers during the pandemic and is much higher than in the general population prepandemic. This suggests health care staff in an air medical service may indeed require extra psychological support, and this is a vital consideration for other air medical organizations worldwide. Along with the obvious benefits to staff themselves, there are a myriad of potential benefits to the service. Improved staff mental health is likely to improve skilled staff retention. Furthermore, it is potentially cost-effective because of reduced sickness leave as a result of mental illness; this is an important consideration, particularly in air medical services that tend to have significantly fewer employees compared with larger organizations such as hospitals. Crucially, extrapolating from hospital-based research, improved staff mental health is likely to have a positive effect on patient outcomes. Future research should consider whether mental illness in staff working in air medical services has an independent effect on patient outcomes, which may already be negatively impacted by the increased case numbers of a pandemic.
Footnotes
We are grateful to Dr Randall Greenberg, chief medical officer at the Royal Flying Doctors Service South Eastern Section, for his help in circulating the survey to staff members and for his input in the planning of the project.
References
- 1.World Health Organization . World Health Organization; Geneva, Switzerland: 2020. WHO Coronavirus (COVID-19) dashboard.https://covid19.who.int/ Available at: Accessed June 29, 2022. [Google Scholar]
- 2.Trumello C, Bramanti SM, Ballarotto G, et al. Psychological adjustment of healthcare workers in Italy during the COVID-19 pandemic: differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-frontline professionals. Int J Environ Res Public Health. 2020;17:8358. doi: 10.3390/ijerph17228358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shechter A, Diaz F, Moise N, et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen Hosp Psychiatry. 2020;66:1–8. doi: 10.1016/j.genhosppsych.2020.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dobson H, Malpas CB, Burrell AJC, et al. Burnout and psychological distress amongst Australian healthcare workers during the COVID-19 pandemic. Australas Psychiatry. 2021;29:26–30. doi: 10.1177/1039856220965045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wong TW, Yau JKY, Chan CLW, et al. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur J Emerg Med. 2005;12:13–18. doi: 10.1097/00063110-200502000-00005. [DOI] [PubMed] [Google Scholar]
- 6.Uphoff EP, Lombardo C, Johnston G, et al. Mental health among healthcare workers and other vulnerable groups during the COVID-19 pandemic and other coronavirus outbreaks: a rapid systematic review. PLoS One. 2021;16 doi: 10.1371/journal.pone.0254821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen Y, Wang J, Geng Y, et al. Meta-analysis of the prevalence of anxiety and depression among frontline healthcare workers during the COVID-19 pandemic. Front Public Health. 2022;10 doi: 10.3389/fpubh.2022.984630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aymerich C, Pedruzo B, Pérez JL, et al. COVID-19 pandemic effects on health worker's mental health: systematic review and meta-analysis. Eur Psychiatry. 2022;65:310. doi: 10.1192/j.eurpsy.2022.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Australian Bureau of Statistics . October 23, 2008. National Survey of Mental Health and Wellbeing: summary of results.https://www.abs.gov.au/statistics/health/mental-health/national-survey-mental-health-and-wellbeing-summary-results/2007#data-download Accessed April 22, 2022. [Google Scholar]
- 10.Australian Bureau of Statistics. National Survey of Mental Health and Wellbeing: summary statistics on key mental health issues including the prevalence of mental disorders and the use of services. 2020-2021. Available at:https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release. Accessed September 8, 2022.
- 11.Hou H, Pei Y, Yang H, et al. Factors associated with turnover intention among healthcare workers during the Coronavirus disease 2019 (COVID-19) pandemic in China. Risk Manag Healthc Policy. 2021;14:4953–4965. doi: 10.2147/RMHP.S318106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Johnston K, Westerfield W, Momin S, Phillippi R, Naidoo A. The direct and indirect costs of employee depression, anxiety, and emotional disorders–an employer case study. J Occup Environ Med. 2009;51:564–577. doi: 10.1097/JOM.0b013e3181a1f5c8. [DOI] [PubMed] [Google Scholar]
- 13.Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397–422. doi: 10.1146/annurev.psych.52.1.397. [DOI] [PubMed] [Google Scholar]
- 14.Hall LH, Johnson J, Watt I, Tsipa A, O'Connor DB. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11 doi: 10.1371/journal.pone.0159015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhang W-R, Wang K, Yin L, et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother Psychosom. 2020;89:242–250. doi: 10.1159/000507639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tan BYQ, Chew NWS, Lee GKH, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med. 2020;173:317–320. doi: 10.7326/M20-1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lai J, Ma Simeng, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3 doi: 10.1001/jamanetworkopen.2020.3976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lu W, Wang H, Lin Y, Li L. Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. 2020;288 doi: 10.1016/j.psychres.2020.112936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tiete J, Guatteri M, Lachaux A, et al. Mental health outcomes in healthcare workers in COVID-19 and non-COVID-19 care units: a cross-sectional survey in Belgium. Front Psychol. 2021;11 doi: 10.3389/fpsyg.2020.612241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.De Kock JH, Latham HA, Leslie SJ, et al. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: implications for supporting psychological well-being. BMC Public Health. 2021;21:104–118. doi: 10.1186/s12889-020-10070-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wahlquist C. Australia's coronavirus lockdown - the first 50 days. The Guardian. 2020 https://www.theguardian.com/world/2020/may/02/australias-coronavirus-lockdown-the-first-50-days Available at: Accessed December 31, 2022. [Google Scholar]
- 22.Ritchie H, Mathieu E, Rodés-Guirao L, et al. University of Oxford Global Change Data Lab; 2020. Our world in data: daily new confirmed COVID-19 cases per million people.https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01.latest&facet=none&pickerSort=asc&pickerMetric=location&Metric=Confirmed+cases&Interval=7-day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=AUS∼GBR∼CHN∼USA∼ITA Available at: Accessed June 29, 2022. [Google Scholar]
- 23.World Health Organization. The impact of COVID-19 on health and care workers: a closer look at deaths. September 13, 2021. Report #WHO-HWF-WorkingPaper-2021.1. Available at: https://www.who.int/publications/i/item/WHO-HWF-WorkingPaper-2021.1. Accesed June 29, 2022.
- 24.Australian Institute of Health Welfare . AIHW; Canberra: 2021. The first year of COVID-19 in Australia: direct and indirect health effects.https://www.aihw.gov.au/reports/burden-of-disease/the-first-year-of-covid-19-in-australia Report #PHE 287. Available at: Accessed June 29, 2022. [Google Scholar]
- 25.Mason RJ. Pathogenesis of COVID-19 from a cell biology perspective. Eur Respir J. 2020;55 doi: 10.1183/13993003.00607-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Edwards B, Barnes R, Rehill P, et al. University of Oxford, Australian National University; 2022. Variation in policy response to COVID-19 across Australian states and territories. Blavatnik School of Government. [Google Scholar]
- 27.Australian Goverment Department of Health. Modified Monash Model. Updated December 14, 2021. Available at: https://www.health.gov.au/health-topics/rural-health-workforce/classifications/mmm. Accessed June 29, 2022.
- 28.Hodgson CL, Udy AA, Bailey M, et al. The impact of disability in survivors of critical illness. Intensive Care Med. 2017;43:992–1001. doi: 10.1007/s00134-017-4830-0. [DOI] [PubMed] [Google Scholar]
- 29.Jutte JE, Needham DM, Pfoh ER, Bienvenu OJ. Psychometric evaluation of the Hospital Anxiety and Depression Scale 3 months after acute lung injury. J Crit Care. 2015;30:793–798. doi: 10.1016/j.jcrc.2015.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tan BYQ, Kanneganti A, Lim LJH, et al. Burnout and associated factors among health care workers in singapore during the COVID-19 pandemic. J Am Med Dir Assoc. 2020;21 doi: 10.1016/j.jamda.2020.09.035. 1751-1758.e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52:69–77. doi: 10.1016/s0022-3999(01)00296-3. [DOI] [PubMed] [Google Scholar]
- 32.Van De Poll MK, Bergström G, Jensen I, et al. Cost-effectiveness of a problem-solving intervention aimed to prevent sickness absence among employees with common mental disorders or occupational stress. Int J Environ Res Public Health. 2020;17:5234. doi: 10.3390/ijerph17145234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cunningham CT, Quan H, Hemmelgarn B, et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15:32. doi: 10.1186/s12874-015-0016-z. [DOI] [PMC free article] [PubMed] [Google Scholar]