

Abstract
Foreign bodies (FB) in the external auditory canal are relative medical emergency. The objective of this study was to describe the types of FB and their complications. Hospital-based descriptive study. This study is done at sub-district hospital Nasirabad (district Ajmer) from period 1 January2016 to 31 May 2020 for period of 3 years 5 months included all patients with foreign body ear. A total of 126 patients were included. All cases were attended by ENT specialist. In our study we concluded that most common incidence is children less than 5 years (63.49%), male:female ratio of 1.33:1, most of the patients present within 24 h of presentation, in maximum cases there is no complications, maximum the foreign body is present in right ear. All cases were attended by ENT specialist. Maximum cases are done in local anaesthesia or no anaesthesia at all, 4 case in light anesthesia and 3 cases referred to nearby higher centre. In this we concluded that foreign body is usually present in less than 5 years of age group. Proper instrumentation and proper skill is required to remove foreign body without any complications.
Keywords: Foreign body, External auditory canal, ENT specialist, Children
Introduction
Foreign body in the ear is relatively common in emergency medicine. Foreign bodies (FB) in the external auditory meatus are most commonly seen in children who have inserted them into their own ears. Adults are often seen with cotton wool or broken matchsticks which have been used to clean or scratch the ear canal [1]. Live insects in the ear [2], are annoying due to discomfort created by loud noise and movement. Accidental entry of foreign body, preexisting disease in ear causing irritation, and habitual cleaning of ear and nose with objects like ear buds [3, 4]. The earliest presentation of an aural foreign body generally occurs around the age of 9 months, when children develop a pincer grip and become able to manipulate small objects [5]. Foreign bodies in ear can be classified in many ways like organic–inorganic, animate-inanimate, metallic-nonmetallic, hygroscopic-nonhygroscopic, regular or irregular, soft or hard, and so forth, according to their nature [6]. The method of removal usually depends on the type of foreign body, its position, and cooperation of the patient [7, 8]. Most cases of a foreign body in the ear are not serious. The keys to successful removal are adequate vision, appropriate equipment, a cooperative patient, and a skilled ENT specialist [9]. The objective of this study was to describe the types of foreign bodies and their complications.
Material and Method
Hospital-based descriptive study done at sub-district hospital Nasirabad (District- Ajmer) from period 1 January 2016 to 31 May 2020 for a period of 3 years 5 months done by ENT specialist. All cases who present with foreign body ear are included in this study either by themselves or referred from nearby centers to our hospitals. Endoscopic view of foreign body headphone earbuds(Fig. 1) and insect(Fig. 2) has been given. All cases were attended by ENT specialist in either OPD or in operation theatre depending on need.
Fig. 1.
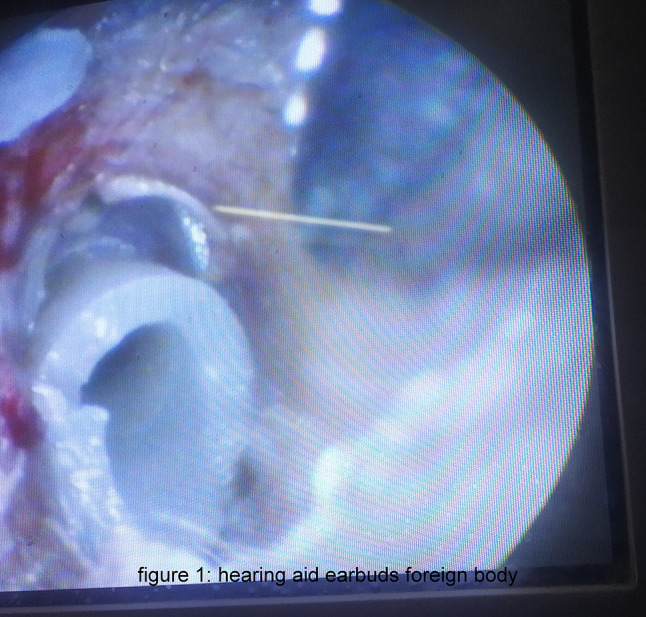
Hearing aid earbuds foreign body
Fig. 2.
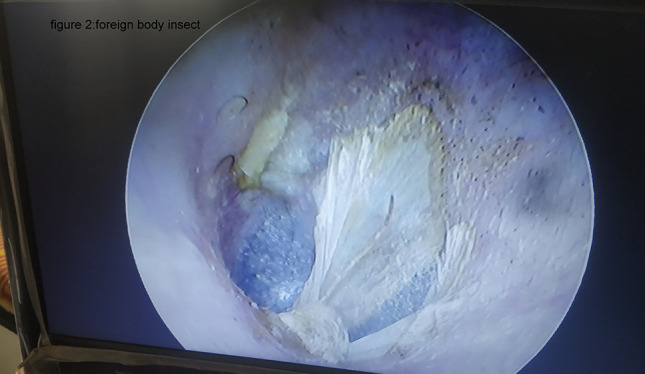
Foreign body insect
Technique
Method depends on position and nature of foreign body and patient and attendant corporation and previous attempt at removal of foreign body. Our technique mainly includes removal with Jobson –Horne probe, microforceps and syringing. If the foreign body is insect it is killed prior to its removal by instilling oil in external auditory canal.
Results
In our study we included 126 patients in total who present with foreign body ear and we concluded that most common incidence is children less than 5 years (63.49%) (Table 1), male: female ratio of 1.33:1(Table 1), most of the patients present within 24 h of presentation (Table 2), in maximum cases there is no complications (Table 3),type of foreign bodies we found in our study vary enormously(Table 4), maximum the foreign body is present in right ear (Table 5). Maximum cases are done in local anaesthesia or no anaesthesia at all, 4 case in light anesthesia and 3 cases referred to nearby higher centre due to non availability of our only anaesthetic in that time period.
Table 1.
Age and sex distribution
| Age (in years) | Males | Females | Total |
|---|---|---|---|
| < 5 | 46 | 34 | 80 |
| 5–15 | 4 | 3 | 7 |
| 15–30 | 2 | 1 | 3 |
| 30–45 | 10 | 7 | 17 |
| > 45 | 10 | 9 | 19 |
| Total | 72 | 54 | 126 |
Table 2.
Time of presentation
| Duration | Total |
|---|---|
| < 24 h | 116 |
| 1–3 day | 6 |
| > 3 days | 4 |
Table 3.
Complications
| Complications | Males | Females | Total |
|---|---|---|---|
| No | 68 | 50 | 118 |
| Tympanic membrane perforation | 1 | 0 | 1 |
| Bleeding | 3 | 3 | 6 |
| Secondary infection (pus discharge) | 1 | 1 | 2 |
| Otitis externa | 2 | 1 | 3 |
Table 4.
Types of foreign body
| Type of foreign body | Males | Females | Total |
|---|---|---|---|
| Stone | 8 | 6 | 14 |
| Paper | 10 | 4 | 14 |
| Beads | 14 | 10 | 24 |
| Eraser | 4 | 3 | 7 |
| Cotton buds | 6 | 8 | 14 |
| Matchstick | 2 | 4 | 6 |
| Battery | 0 | 1 | 1 |
| Insect | 15 | 8 | 23 |
| Seeds | 11 | 8 | 19 |
| Headphone earbuds | 0 | 1 | 1 |
| Thermacoal | 2 | 0 | 2 |
| Crayons | 0 | 1 | 1 |
| Total | 72 | 54 | 126 |
Table 5.
Side involved
| Right ear | Left ear | Bilateral | Total |
|---|---|---|---|
| 82 | 42 | 2 | 126 |
Discussion
The majority of foreign bodies that become impacted in the ear are placed there voluntarily, usually by children [10]. In our study we concluded that most common incidence is in children less than 5 years (63.49%) Other studies of aural foreign bodies have shown that 38.1 to 64.2% occurred in children aged 0 through 5 years [5, 11–14].
Male: female ratio of 1.33:1in our study.
Most of the patients present within 24 h of presentation this was also observed in other studies [15, 16].
In maximum cases foreign body was present in right ear.This is similar to those reported in other studies [5, 11, 12]. The higher proportion of foreign bodies in the right ear can be explained by the fact that most of the foreign bodies were inserted by patients themselves, and most of these patients were right-handed [11, 17].
Complications can happen either due to the foreign body itself or from the examination or from an attempt to remove the foreign body. The most common complications encountered are abrasions, bleeding due to injury, secondary infection and tympanic membrane perforation [18]. In our study we concluded that in majority of cases there is no complication at all, in rest bleeding is the most common complication noted.
Maximum cases are done in local anaesthesia or no anaesthesia at all, 4 case in light anesthesia and 3 cases referred to nearby higher centre due to non availability of our only anaesthetic in that time period. Type and nature of foreign bodies found varies enormously in our study.
Conclusion
In this we concluded that foreign body is usually present in children less than 5 years of age group. Proper instrumentation and proper skill and specialized doctor are required to remove foreign body without any complications. Every case should be individualized according to its need.
Funding
Nil.
Declarations
Conflict of interest
Nil.
Footnotes
Rashmi Yadav and Dinesh Kumar Yadav Work done at Government General Hospital (sub-district hospital), Nasirabad, Ajmer.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Kroukamp GR, Loock JW, et al. Foreign bodies in the ear, 7th edn. In: Gleeson M, Browning GG, Burton MJ, et al., editors. Scott-Brown’s otorhinolaryngology, head and neck surgery. NY, USA: New York; 2008. pp. 3370–3372. [Google Scholar]
- 2.Kroukamp G, Londt JGH. Ear-invading arthropods: a South African survey. S Afr Med J. 2006;96(4):290–292. [PubMed] [Google Scholar]
- 3.Das SK. Aetiological evaluation of foreign bodies in the ear and nose (a clinical study) J Laryngol Otol. 1984;98(10):989–991. doi: 10.1017/S002221510014784X. [DOI] [PubMed] [Google Scholar]
- 4.Kalan A, Tariq M. Foreign bodies in the nasal cavities: a comprehensive review of the aetiology, diagnostic pointers, and therapeuticmeasures. Postgrad Med J. 2000;76(898):484–487. doi: 10.1136/pmj.76.898.484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fasunla J, Ibekwe T, Adeosun A. Preventable risks in the management of Aural foreign bodies in western Nigeria. Int J Otorhinolaryngol. 2007;7(1):3–5. [Google Scholar]
- 6.Schulze SL, Kerschner J, Beste D. Pediatric external auditory canal foreign bodies: a review of 698 cases. Otolaryngol Head and Neck Surg. 2002;127(1):73–78. doi: 10.1067/mhn.2002.126724. [DOI] [PubMed] [Google Scholar]
- 7.Balbani APS, Sanchez TG, Butugan O, et al. Ear and nose foreign body removal in children. Int J Pediatr Otorhinolaryngol. 1998;46(1–2):37–42. doi: 10.1016/S0165-5876(98)00118-9. [DOI] [PubMed] [Google Scholar]
- 8.Thompson SK, Wein RO, Dutcher PO. External auditory canal foreign body removal: management practices and outcomes. Laryngoscope. 2003;113(11):1912–1915. doi: 10.1097/00005537-200311000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Helm SW, Maughan KL. Foreign bodies in the ears nose, and throat. Am Fam Physician. 2007;76(8):1185–1189. [PubMed] [Google Scholar]
- 10.Rull G (2010) Foreign bodies in the ear. Patient.co.uk. http://www.patient.co.uk/doctor/Foreign-bodies-in-the-Ear.htm. Accessed 4 Oct 2011
- 11.Ijaduola GT, Okeowo PA. Foreign body in the ear and its importance: the Nigerian experience. J Trop Pediatr. 1986;32(1):46. doi: 10.1093/tropej/32.1.4. [DOI] [PubMed] [Google Scholar]
- 12.Bhatia PL. Aural and nasal foreign bodies. Niger Med Pract. 1987;14(1/2):17–20. [Google Scholar]
- 13.Iseh KR, Yahaya M. Ear foreign bodies: observations on the clinical profile in sokoto, Nigeria. Ann Afr Med. 2008;7(1):18–23. doi: 10.4103/1596-3519.55689. [DOI] [PubMed] [Google Scholar]
- 14.Ologe FE, Dunmade AD, Afolabi OA. Aural foreign bodies in children. Indian J Paediatr. 2007;74(8):755–758. doi: 10.1007/s12098-007-0133-8. [DOI] [PubMed] [Google Scholar]
- 15.Olajide TG, Ologe FE, Arigbede OO. Management of foreign bodies in the ear: a retrospective review of 123 cases in Nigeria. Ear, Nose Throat J. 2011;90(11):E16. [PubMed] [Google Scholar]
- 16.Hon SK, Izam TM, Koay CB, Razi A. A prospective evaluation of foreign bodies presenting to the Ear, Nose and Throat Clinic, Hospital Kuala Lumpur. Med J Malays. 2001;56(4):463–470. [PubMed] [Google Scholar]
- 17.Wada I, Kase Y, Iinuma T. Statistical study on the case of aural foreign bodies. J Otolaryngol Jpn. 2003;106(6):678–684. doi: 10.3950/jibiinkoka.106.678. [DOI] [PubMed] [Google Scholar]
- 18.Votey S, Dudley JP. Emergency ear, nose and throat procedures. Emerg Med Clin North Am. 1989;7(2):117–154. doi: 10.1016/S0733-8627(20)30509-5. [DOI] [PubMed] [Google Scholar]