

Abstract
There has been always a need of new methods to control post operative complications in OMFS. A randomized prospective study was done to assess the effect of K tape on postoperative swelling, pain, trismus in Zygomatico-maxillary Complex (ZMC) fracture after open reduction with internal fixation using two point fixation. 30 patients of either gender undergoing ORIF for ZMC fracture using two point fixation of age group between 18 and 50 years were included in the study. Patients were divided into treatment either with or without Kinesiologic tape. Tape was applied directly after surgery and maintained for at least 5 days postoperatively. Facial swelling was quantified using a five-line measurement at six specific points of time. Pain and degree of mouth opening was measured. Patient’s subjective feeling was asked. The values were subjected to Fischer’s exact test, Independent sample test, Mann whitney U test, Wilocoxon sign rank test. The results of this study show that application of Kinesiologic tape after zygomatico maxillary complex fracture surgery significantly reduced the incidence of swelling with an earlier resolution of swelling, and decreased the maximum turgidity for more than 60% during the first 2 days after surgery. Although, Kinesiologic tape has no significant influence on pain control but reduction in trismus in the Kinesiologic tape group compared to the non-Kinesiologic tape group. Furthermore, patients with Kinesiologic tape felt significantly lower morbidity than those without Kinesiologic tape. This study suggests that Kinesiologic tape is a promising, simple, less traumatic, economical approach, which is free from adverse reaction and improves patients quality of life.
Keywords: Zygomaticomaxillary complex fracture, Kinesiologic tape (KT), Pain, Trismus, Swelling
Introduction
The zygomaticomaxillary complex plays a key role in the function and appearance of facial skeleton. The prominent convex shape of zygoma gives the contour of the cheek and makes it vulnerable to traumatic injury [1]. The frequency of zygomaticomaxillary complex fracture is common and about 45% [2]. The current method of treatment in maxillofacial fractures is open reduction with internal fixation (ORIF) with miniplates and screws which offers stable reduction of the fracture fragments. This would consequently allow for early mobilization of the jaw, early and optimal recovery of function and aesthetic [3, 4]. ORIF has revolutionised the treatment of ZMC fracture but it is often accompanied by pain, trismus and swelling. These postoperative morbidities are disadvantages that affect the quality of life of patients. These complications were managed by using various drugs like corticosteroids, NSAIDs, and opioids [5]. Opioids are effective analgesics, but they have a sedative effect too Corticosteroids are potent anti-inflammatory drugs but have a disadvantage of adrenal suppression and delayed wound healing [6]. NSAIDs can manage post-operative pain and inflammation, but long term use of them may have an adverse effect on the gastric mucosa. Post-operative application of lasers, cryotherapy to modulate the inflammatory response on injured tissues, use of surgical drains to remove excess inflammatory fluids and physical therapies to improve lymph flow and bring microcirculation and oxygenation to the tissues, thereby decreasing oedema and pain [7, 8]. Most of the treatment modalities have some disadvantages, associated with potential side effects and need specialised equipment. This study chooses the use of a non- invasive, elastic KT for the effective management of post-operative complications in ZMC fracture after ORIF with two point fixation.
Kinesio Taping is a technique developed by Dr. Kenzo Kase in the 70s. The adhesive pliable material, directly applied to the skin, differs from classical tape in its physical characteristics. Kinesio Taping technique claims four effects: to normalize muscular function, to increase lymphatic and vascular flow, to diminish pain and aid in the correction of possible articular malalignments [9]. There are limited studies done regarding the use of Kinesiologic (K) tape in oral and maxillofacial surgery. Hence a study was done to assess the effect of Kinesiologic tape (KT) on post operative swelling, pain, trismus in ZMC fracture after open reduction with internal fixation using two point fixation.
Aim and Objective
To evaluate the effect of Kinesiologic tape (K tape) on post operative swelling, pain, trismus in zygomaticomaxillary complex fracture after open reduction with internal fixation. To record and compare the swelling, pain, trismus and satisfaction in patients with K tape and patients without K tape after open reduction with internal fixation for ZMCfracture.
Materials and Methods
Thirty patients (belonging to experimental as well as control group) between the age group 18–50 years who reported to the Hospital in India diagnosed with conditions requiring open reduction with internal fixation of ZMC fracture from Mar 2016 to Dec 2018. Written informed consent was taken from the subjects prior to treatment.
II Study design: The patients with unilateral ZMC fracture requiring open reduction with internal fixation chosen as per the inclusion and exclusion criteria were the study subjects.
Inclusion Criteria
Patients with isolated unilateral ZMC fracture requiring open reduction with internal fixation using two point fixation.
Age group 18–50 years.
Exclusion Criteria
Patients with sensitivity to tape, Patient with extensive extraoral laceration and abrasion, Patient showing unwillingness to shave facial hair, Patients younger than 18 years, Patients with infected fractures, Patients with other maxillofacial fractures of same side, Patient with ZMC fracture which require treatment other than two point fixation.
The subjects were divided into two groups—Group A and Group B.
| A | With K tape | Experimental group | N = 15 |
| B | Without K tape | Control group | N = 15 |
Procedure
Preoperatively patients were checked for the sensitivity for the K tape. All surgical procedures were performed by single operator (Oral and Maxillofacial surgeon) under GA using nasal intubation. Surgery was performed under sterile conditions according to a standardized surgical protocol. All the ZMC fractures were treated by ORIF using two point fixation. Intraoral approach was used for plate fixation in zygomatico maxillary buttress region. Lateral eyebrow incision was used for plate fixation at frontozygomatic suture area. Closure was done in single layer by 3–0 vicryl intraorally and using 3–0 vicryl and 5–0 ethylon in layers extraorally. Postoperatively antibiotic and analgesic course was given to every patient. Patients were divided into Group A and Group B according to inclusion and exclusion criteria:
Group A (Experimental/ K Tape group) TAPING- All taping procedure were performed by the same investigator. The skin was cleaned, shaved if necessary and freed of moisture and oil before application. All taping applications were performed using skin coloured K Active tape. Tape length was measured for each patient starting at the clavicle to the point of greatest swelling. Measurement were carried out in a stretched position. The base was placed slightly above the lymph node area to which drainage was directed(supra clavicular nodes). Tails will be placed on the skin with slight tension (20%) [9]. Placement of the K tape was directed at the appropriate lymphatic duct crossing the cervical, submental, mandibular, submandibular, preauricular, and parotid nodes to area of maximum swelling [9] (Fig. 1). Tape was removed after 5 days post operatively.
Fig. 1.

Kinesiologic tape application
Group B (Control/Without K Tape): All the procedures were performed in the same manner as group A but without K tape application, postoperatively.
Clinical Parameters
Various parameters were used to evaluate the study subjects (Attachment 2). These patients were evaluated at 6 specific time intervals: Preoperatively (T-1), Baseline (T0), 1st Post-operative day (T1), 2nd Post-operative (T2), 3rd Post-operative day (T3), 7th Post-operative day (T4) for various parameters; swelling, pain, trismus, patient satisfaction.
Swelling Measurement
Swelling was assessed by a 5 line measurement given by Oliver Ristow using a standard plastic tape measure placed in contact to the skin [9] (Fig. 2).
Fig. 2.

Five-line measurement of swelling
Line A most posterior point of the tragus to the most lateral point of the lip commissure.
Line B most posterior point of tragus to the pogonion.
Line C most posterior point of the tragus to the lateral canthus of eye.
Line D lateral canthus of eye to the most inferior point of angle of the mandible.
Line E most inferior point of the angle of the mandible to the middle of the nasal bone.
Trismus Measurement
Maximum mouth opening was recorded after measuring the maximum interincisal distance using calipers (Fig. 3).
Fig. 3.
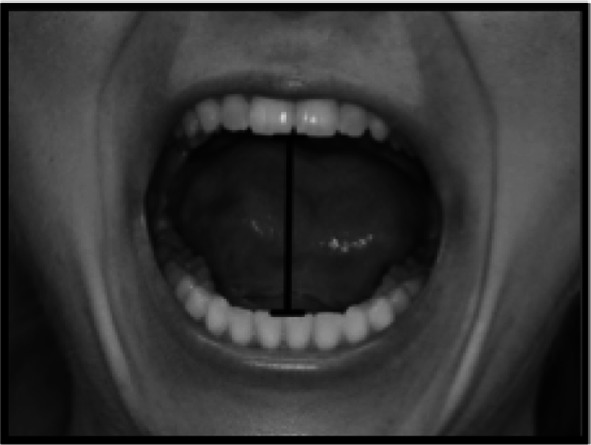
Measuring the inter incisal distance
Pain Measurement
Pain score was assessed using a 10-level VAS of 100 mm given by Oliver Ristow, which represented all pain sensations from none to maximum (0, no pain; 5, moderate pain; 10, worst possible pain) [9]. Patient were asked to place a mark along the line corresponding to the amount of pain they were experiencing (Fig. 4).
Fig. 4.
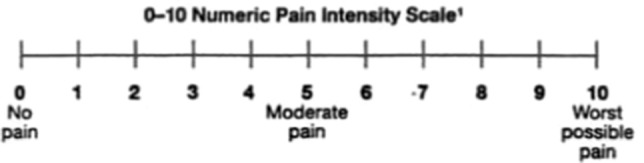
Pain score was assessed using a 10-level VAS
Patient Satisfaction
Patients were asked to note the satisfaction (0, not satisfied: 1, satisfied; 2, very satisfied).
Statistical Analysis
The data were collected on sheets and entered in MS-Excel and analysed in SPSS (version 22). Descriptive statistics were represented with percentages and Mean ± standard deviation. Independent t-test was applied to find the statistical significance by comparing measurements of pain, trismus, swelling, and patient satisfaction between the two groups for different observations during the various follow-up days. During the course of treatment starting preoperatively, these patients were evaluated at 6 specific time intervals. The values were subjected to Fischer’s exact test, Independent sample test, Mann whitney U test, Wilocoxon sign rank test. In all the tests p-value less than 0.05 was accepted as statistically significant.
Results
Thirty patients of ZMC fractures were divided into two groups namely Group A and Group B where Group A is the study group while Group B is the control group. Group A patients were applied K tape postoperatively.
Table 1 shows the gender distribution between Group A and Group B. Groups were compared using Fischer’s exact test and were statistically insignificant. There was no significant difference in gender distribution between the groups.
Table 1.
Gender distribution
| Gender | Group | Total | Fisher’s exact test | |
|---|---|---|---|---|
| With K tape | Without K tape | p-value | ||
| Male | 13(86.7%) | 14(93.3%) | 27(90.0%) | 1.00(NS) |
| Female | 2(13.3%) | 1(6.7%) | 3(10.0%) | |
| Total | 15(50.0%) | 15(50.0%) | 30(100.0%) | |
*P < 0.05 Statistically significant P > 0.05 Non significant, NS
Inference: There was no significant difference in gender distribution between the groups
Table 2 shows the age distribution among Group A and Group B. The mean age of the Group A patients was 30.2 and Group B was 31.8 which is statistically insignificant. There was no significant difference in age distribution between the groups.
Table 3.
Inter group comparison of patient satisfaction
| Groups | Fisher’s exact test | |||
|---|---|---|---|---|
| A | B | p-value | p-value | |
| T0 | ||||
| 0 | 1(6.7%) | 1(6.7%) | 2(6.7%) | |
| 1 | 8(53.3%) | 6(40.0%) | 14(46.7%) | |
| 2 | 6(40.0%) | 8(53.3%) | 14(46.7%) | 0.85(NS) |
| T1 | ||||
| 0 | 2(13.3%) | 3(20.0%) | 5(16.7%) | |
| 1 | 9(60.0%) | 9(60.0%) | 18(60.0%) | 1.00(NS) |
| 2 | 4(26.7%) | 3(20.0%) | 7(23.3%) | |
| T2 | ||||
| 0 | 1(6.7%) | 7(46.7%) | 8(26.7%) | |
| 1 | 5(33.3%) | 6(40.0%) | 11(36.7%) | |
| 2 | 9(60.0%) | 2(13.3%) | 11(36.7%) | 0.01* |
| T3 | ||||
| 0 | 1(6.7%) | 6(40.0%) | 7(23.3%) | |
| 1 | 6(40.0%) | 9(60.0%) | 15(50.0%) | |
| 2 | 8(53.3%) | 0 | 8(26.7%) | 0.001* |
| T4 | ||||
| 0 | 1(6.7%) | 2(13.3%) | 3(10.0%) | 0.18(NS) |
| 1 | 3(20.0%) | 7(46.7%) | 10(33.3%) | |
| 2 | 11(73.3%) | 6(40.0%) | 17(56.7%) | |
Inference: Patients were more very satisfied in Group A interval than Group B at T2 and T3 time
*P < 0.05 Statistically significant
Table 2.
Age distribution
| Group | N | Mean | SD | Mean difference (95% CI) | T | df | p-value |
|---|---|---|---|---|---|---|---|
| 1 | 15 | 30.20 | 8.760 | − 1.66(− 8.90, 5.7) | − .47 | 28 | .64(NS) |
| 2 | 15 | 31.87 | 10.50 |
Independent sample t test
*P < 0.05 Statistically significant
P > 0.05 Non significant
NS Inference: There was no significant difference in age distribution between the groups
Table 3 shows Patient satisfaction at different time intervals between Group A and Group B. The groups were compared using Fischer’s exact test which shows at time interval T0, T1 and T4 difference in satisfaction was not significant while at time interval T2 and T3 it was statistically significant. The patients were more satisfied in Group A than Group B at T2andT3 time interval.
Figure 5 shows comparison of Swelling in Group A and Group B at different time intervals. Independent t test with 95% confidence interval taking T0 as the baseline for comparison shows the result as statistically significant reduction in swelling in Group A patients at T1, T2, T3 and T4 time interval when compared to the same in Group B patients. Also Intragroup comparison of swelling in Group A and Group B taking T-1 and T0 as baseline. Results are statistically significant which implies that swelling reduced in both the groups as time progressed.
Fig. 5.
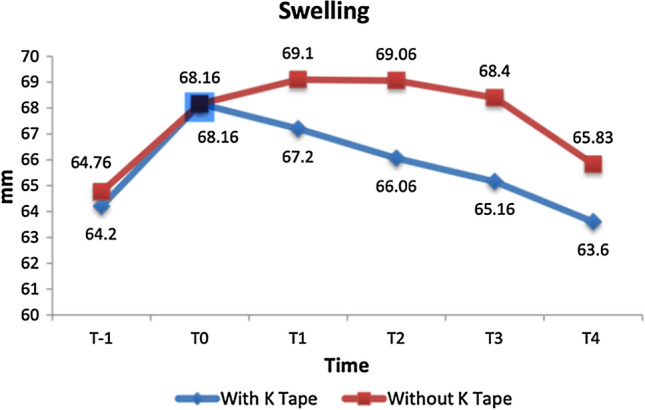
Comparison of Swelling
Figure 6 shows comparison of Pain in Group A and Group B at different time intervals using Mann whitney test. Pain difference between the groups is statistically insignificant at time interval T0, T1, T2 and T4 and significant at time T3. Friedman test was used to compare the mean of pain in Group A and Group B which shows less pain in Group A patients at T3 time interval. The intragroup comparison of pain taking T-1 as baseline. Group A patients results are significant at T1, T3 and T4 time interval which implies that pain reduced as time progressed. Group B patients results are significant at T1, T2 and T4 time interval which implies that pain reduced as time progressed.
Fig. 6.
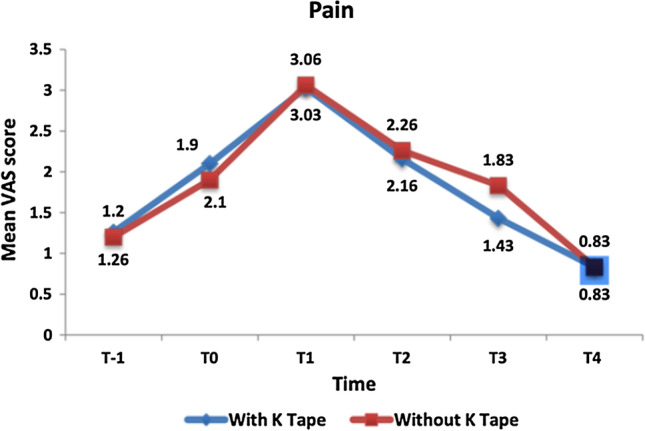
Comparison of Pain
Figure 7 shows the comparison of Trismus between Group A and Group B using independent t test which shows significant reduction in trismus in Group A at time intervals T1, T2, T3.
Fig. 7.
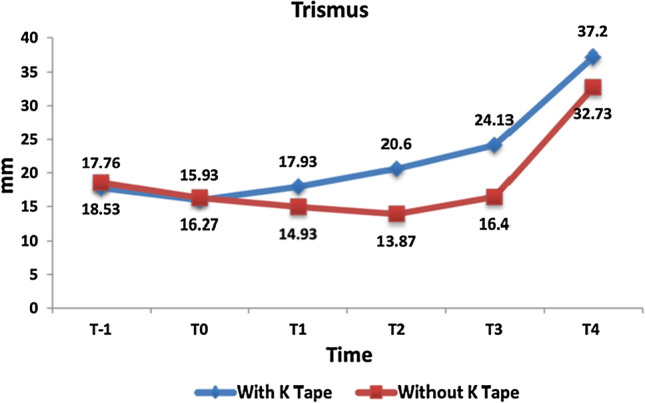
Comparison of Trismus
Discussion
K tape was developed in the 1970s in Japan by Dr. Kenzo Kase who was looking for a tape that would heal traumatized tissue. The popularity of Kinesio tape is due to its elastic and non restrictive nature [9]. There are specific techniques to apply the tape that allows the tape be used for multiple purposes. Its uses include: supporting weaker muscle, relax tight muscle, pain relief, correction of biomechanical problem, reduce swelling, provide sensory feedback for postural awareness and alignment [9–11]. The main objective of KT was to support injured muscles and joints and thus relieve pain and lymphoedema. The principle behind the KT is that it lifts the skin, thus improving blood and lymph flow beneath the skin. Inflammatory fluids in tissue spaces are directed to move from areas of higher pressure toward areas of lower pressure under influence of the tape to desired direction [12]. KT has been designed to allow 30 to 40% longitudinal stretch. By extending and rotating the muscles the skin of the area to be treated is stretched. KT is then applied to the skin with a slight stretch. When the body parts return to their starting points the tape subsequently recoils back to its original length following the application. This creates a pulling force to the skin forming convolutions below the taped area. It is believed that these convolutions increase the interstitial space between the skin and underlying connective tissue, thus promoting the flow of blood and lymphatic fluid [12–14].
In our study significant reduction in swelling is found in K tape group with maximum swelling on the 2nd and 3rd postoperative day which was same in both the groups. Furthermore reduction in swelling was faster in K tape group than without K tape group. The results of the study done by Oliver Ristow also showed that the application of KT after Zygomatico-orbital surgery has a significant influence on tissue reaction and swelling. The primary endpoint, increase of swelling was significantly lower for the KT group than the non-KT group [15–17].
According to the existing literature, the elastic nature of KT causes stretching and lifting of the skin during movement, which arouses low- threshold cutaneous mechanoreceptors and reduction in pain [17]. Kase et al., found out that KT decreases pain by alleviating pressure on nociceptors and thereby helps in pain reduction [18]. In our study no reduction of pain for the KT group compared to the no-KT group was demonstrated. Other studies performed by Gonzalez-Iglesias et al. and Thelen et al., are in agreement with these findings [18, 19]. The results of our study show patients scored moderate pain or less in both groups (VAS < 5) for all six specific measurement times.
In our study a significant increase in mouth opening (decreased trismus) was seen in K tape group as compared to non K tape group. Similar results were found by Oliver Ristow et al. in their studies on zygomatico orbital fracture. This might be because the swelling resolves faster, taking the tension from the skin [19].
It is also observed in our study, patients were more satisfied in K tape group as compared to non K tape group. This might be possible because KT effect detracts from pain and perception. Movement stresses Kinesiologic Tape, it only partially adjusts its length to that of the skin, and thus deforms the skin. This constant stimulus stimulates the skin and diverts patients’ recognition, but our study was not designed to exclude possible placebo effects caused by the KT [19–21].
The present study was designed to use therapeutic KT to minimise the post-operative complications in patients undergoing ORIF for ZMC fractures. The advantages of KT are that it is easy to handle, non-invasive, less traumatic, cost-effective, light weight and has ventilation characters (free movement of air through the skin as KT is made of 100% cotton). The disadvantages of KT are that it causes friction due to elasticity of tape; can irritate the skin and sometimes adhesives may produce allergic reaction [21, 22]. Limitations of the study is limited sample size used to assess the efficiency of K tape.
Conclusion
The KT can be used as a potential adjunct to other treatment modalities in managing post-surgical complications such as pain, trismus and swelling The beneficial effect of tape is due to its elastic and non restrictive nature. This technique claims four effects: to normalize muscular function, to increase lymphatic and vascular flow, to diminish pain and aid in the correction of possible articular malalignments. In OMFS, literature regarding use of this technique is limited. Our study showed significant reduction in swelling and trismus postoperatively. The use of KT appears promising, because it is simple to carry out, less traumatic, economical, can be performed anywhere in the world and free from side effects on the body. Further studies in larger sample have to be performed to find out if KT can reduce or replace the need for additional medications such as the use of steroids in Oral and Maxillofacial surgery.
Funding
None.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, Govt hospital, India.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Kritant Bhushan, Email: Kritant83@gmail.com.
Mansi Luthra Sharma, Email: drmansi17@gmail.com.
References
- 1.Kamadjaja DB, Pramono DC (2008) Management of zygomatic-maxillary fracture (The principles of diagnosis and surgical treatment with a case illustration). Dent J (Maj Ked Gigi) 41(2):77–83
- 2.Marinho RTM, Maia BF. Management of fractures of the zygomaticomaxillary complex. Oral Maxillofacial Surg Clin N Am. 2013;25(4):617–636. doi: 10.1016/j.coms.2013.07.011. [DOI] [PubMed] [Google Scholar]
- 3.Kim JH, Lee JH, Hong SM. The effectiveness of 1-point fixation for zygomaticomaxillary complex fracture. Arch Otolaryngol Head Neck Surg. 2012;138(9):828–832. doi: 10.1001/archoto.2012.1815. [DOI] [PubMed] [Google Scholar]
- 4.Ungari C, Filiaci F, Riccardi E. Etiology and incidence of zygomatic fracture: a retrospective study related to a series of 642 patients. Eur Rev Med Pharmacol Sci. 2012;16:1559–1562. [PubMed] [Google Scholar]
- 5.Gandi LN, Kattimani VS, Gupta AV, Chakravarthi VS, Meka SS. Prospective blind comparative clinical study of two point fixation of zygomatic complex fracture using wire and mini plates. Head Face Med. 2012;6(8):7. doi: 10.1186/1746-160X-8-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aznar-Arasa L, Harutunian K, Figueiredo R, Valmaseda-Castellon E, GayEscoda C. Effect of preoperative ibuprofen on pain and swelling after lower third molar removal: a randomised controlled trial. Int J Oral Maxillofac Surg. 2012;41(8):1005–1009. doi: 10.1016/j.ijom.2011.12.028. [DOI] [PubMed] [Google Scholar]
- 7.Cebi AT, Kasapoglu MB, Eren S, Kasapoglu C. Comparison of the effects of diclofenac potassium and tenoxicam on postoperative pain, swelling, and trismus following third molar surgery. Turk J Med Sci. 2018;48(2):271–278. doi: 10.3906/sag-1702-100. [DOI] [PubMed] [Google Scholar]
- 8.Kim K, Brar P, Jakubowski J, Kaltman S, Lopez E. The use of corticosteroids and nonsteroidal antiinflammatory medication for the management of pain and inflammation after third molar surgery: a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:630–640. doi: 10.1016/j.tripleo.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 9.Ristow O, Majert BH, Kehl V, Koerdt S, Hahnefeld L, Pautke C. Does elastic therapeutic tape reduce post operative swelling, pain, and trismus after open reduction and internal fixation of mandibular fractures. J Oral Maxillofac Surg. 2013;71:1387–1396. doi: 10.1016/j.joms.2013.03.020. [DOI] [PubMed] [Google Scholar]
- 10.Zachariades N, Mezitis M (1998) Anagnostopoulos. Changing trends in the treatment of the zygomaticomaxillary complex fracture: a 12 year evaluation of methods used. J Oral Maxfac Surg 56:1152–1156 [DOI] [PubMed]
- 11.Montalvo AM, Buckley WE, Sebastianelli W, Vairo GL. An evidence- based practice approach to the efficacy of kinesio taping for improving pain and quadriceps performance in physically-active patellofemoral pain syndrome patients. J Nov Physiother. 2013;3:151. [Google Scholar]
- 12.Chang HY, Wang CH, Chou KY, Cheng SC. Could forearm Kinesio Taping improve strength, force sense and pain in baseball pitchers with medial epicondylitis? Clin J Sport Med. 2012;22(4):327–333. doi: 10.1097/JSM.0b013e318254d7cd. [DOI] [PubMed] [Google Scholar]
- 13.Lee YS, Bae SH, Hwang JA, Kim KY. The effects of kinesio taping on architecture, strength and pain of muscles in delayed onset muscle soreness of biceps brachii. J Phys Ther Sci. 2015;27(2):457–459. doi: 10.1589/jpts.27.457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shakeri H, Keshavarz R, Arab AM, Ebrahimi I. Clinical effectiveness of kinesiological taping on pain and pain-free shoulder range of motion in patients with shoulder impingement syndrome: a randomized, double blinded, placebo-controlled trial. Int J Sports Phys Ther. 2013;8(6):800–810. [PMC free article] [PubMed] [Google Scholar]
- 15.Genc A, Cakarer S, Yalcin BK, Kilic BB, Isler SC, Keskin C. A comparative study of surgical drain placement and the use of kinesiologic tape to reduce postoperative morbidity after third molar surgery. Clin Oral Investig. 2018;23(1):345–350. doi: 10.1007/s00784-018-2442-x. [DOI] [PubMed] [Google Scholar]
- 16.Szolnoky G, Szendi-Horvath K, Seres L, Boda K, Kemeny L. Manual lymph drainage efficiently reduces postoperative facial swelling and discomfort after removal of impacted third molars. Lymphology. 2007;40(3):138–142. [PubMed] [Google Scholar]
- 17.Ristow O, Hohlweg-Majert B, Kehl V, Koerdt S, Hahnefeld L, Pautke C. Does elastic therapeutic tape reduce postoperative swelling, pain, and trismus after open reduction and internal fixation of mandibular fractures? J Oral Maxillofac Surg. 2013;71(8):1387–1396. doi: 10.1016/j.joms.2013.03.020. [DOI] [PubMed] [Google Scholar]
- 18.Tozzi U, Santagata M, Sellitto A, Tartaro GP. Influence of kinesiologic tape on postoperative swelling after orthognathic surgery. J Maxillofac Oral Surg. 2016;15(1):52–58. doi: 10.1007/s12663-015-0787-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ristow O, Pautke C, Kehl V, Koerdt S, Schwarzler K, Hahnefeld L, et al. Influence of kinesiologic tape on postoperative swelling, pain and trismus after zygomatico- orbital fractures. J Craniomaxillofac Surg. 2014;42(5):469–476. doi: 10.1016/j.jcms.2013.05.043. [DOI] [PubMed] [Google Scholar]
- 20.Kase K, Wallis J, Kase T (2003) Clinical therapeutic applications of the kinesio taping method. 2nd ed. Kinesio Taping Association, Tokyo
- 21.Merino-Marban R, Mayorga-Vega D, Fernandez-Rodriguez E. Effect of kinesio tape application on calf pain and ankle range of motion in duathletes. J Hum Kinet. 2013;37:129–135. doi: 10.2478/hukin-2013-0033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kase K, Stockheimer KR (2006) Kinesio taping for lymphoedema and chronic swelling. Kinesio Taping Manual. 01–172