

Abstract
We report the technique of two handed transcanal endoscopic ossiculoplasty using tragal cartilage in the form of boomerang as an option for total ossicular replacement in absence of stapes superstructure. In this technique, the vertical strut is fashioned as a boomerang and measures 10 mm in length and 2 mm in breadth. A partial thickness cut is made on the vertical strut at 4–4.5 mm along the length so that it can be bent into boomerang, one end of which is placed on the stapes footplate and the other part rests in the hypotympanum. This stable assembly is placed on the footplate of the stapes (when all ossicles are absent). Tympanic membrane reconstruction is performed with or without attic reconstruction, using sliced tragal cartilage of 0.5 mm thickness. Boomerang ossiculoplasty is good option in cases of absent stapes providing a stable assembly. The use of endoscope holder during ear surgery gives additional advantages of panoramic view of middle ear spaces due to use of endoscope along with benefits of two handed technique (similar to microscopic ear surgery).
Supplementary Information
The online version contains supplementary material available at 10.1007/s12070-021-02854-9.
Keywords: Endoscope holder, Two handed technique, Minimal invasive transcanal approach, Cartilage boomerang Ossiculoplasty, Stapes superstructure absent, TORP
Introduction
In middle ear diseases involving ossicular chain like resorptive osteitis and cholesteatoma, ossicular reconstruction becomes mandatory for a favourable hearing outcome. Among the various options available for ossicular reconstruction including prosthesis like TORP, PORP, we prefer the use of tragal cartilage fashioned as boomerang for ossicular reconstruction as an option for total ossicular replacement when all ossicles are absent. We have been using the tragal cartilage since 2003 as the graft of choice for reconstructing of the tympanic membrane, attic and for the ossicular reconstruction. Till 2013, we performed all techniques of tympanoplasty and ossiculoplasty using microscope. In 2013, after development of endoscope holders, we have been performing these techniques of cartilage tympanoplasty with the additional advantages of endoscope and endoscope holders [1–13]. We report the use of tragal cartilage graft fashioned as a boomerang to be placed over the stapes footplate in the absence of stapes superstructure. We have been using this technique of cartilage ossiculoplasty since 2018. We report the use of the table model of endoscope holder having gas spring action and rack and pinion mechanism [14, 15].
Methods
Operating Theatre Requirements
Zero degree 3 mm Karl Storz endoscope, triple charge coupled device Camera (Karl Storz, Germany), and table model of endoscope holder, Endohold GS 201 B (Dr. Khan’s Creations, India).
The table model of the Endoscope holder (Fig. 1) is based on the concept of gas spring action with rack and pinion mechanism [16, 17]. A gas spring is a type of spring that, unlike a typical mechanical spring that uses compressed gas contained within an enclosed cylinder sealed by a sliding piston to pneumatically store potential energy and withstand external force applied parallel to the direction of the piston shaft [16]. A rack and pinion is a type of linear actuator that comprises a circular gear (the pinion) engaging a linear gear (the rack), which operate to translate rotational motion into linear motion [17]. The endoscope holder is dynamic, allowing the endoscope to be tilted in any direction (rotated forwards, rotated backwards, upwards, downwards and sidewise angular rotation). The peculiarity of the endoscope holder is that it is provided with rack and pinion mechanism which allows the additional few centimetres closer motion of the endoscope into the ear canal and middle ear cavity [2, 3, 14, 15] (Fig. 2).
Fig. 1.

Gas spring action of endoscope holder, endohold GS 201 B in endoscopic ear surgery
Fig. 2.
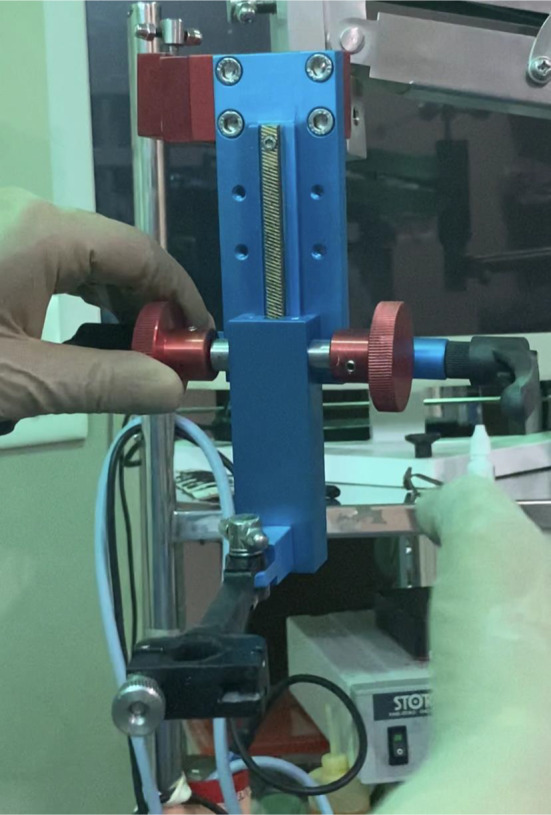
Rack and pinion action of endoscope holder, endohold GS 201 B in endoscopic ear surgery
The parts of the endoscope holder, Endohold GS 201B [14]:
O.T. table gripping attachment
Horizontal metallic rod
Gas Spring arm
Metallic connecting rod
Rack and pinion system attached
Attachment with slot for holding the endoscope
Position of Endoscope Holder
The endoscope holder is fixed to the operation table on the opposite side of the ear to be operated. The endoscope is mounted onto the endoscope holder with the camera. The endoscope is directed into the ear canal. The operating surgeon sits on the same side as the ear with the monitor facing the surgeon. The surgeon operates by seeing onto the monitor thus requiring hand-eye-monitor coordination.
Preparation of the Patient
The patient is prepared and draped in the usual fashion with the ipsilateral shoulder pulled down. The ear canal is infiltrated with 2 percent lidocaine with 1 in 2, 00,000 adrenaline.
Harvest of the Tragal Cartilage
Tragal cartilage is harvested via the horizontal incision on the tragus. Approximately 15 × 15 mm cartilage along with perichondrium is harvested. The incision is sutured.
Preparation of the Boomerang graft
The full thickness of tragal cartilage measuring 10 mm in length and 2 mm in breadth is cut from the full size harvested tragal graft. A partial thickness cut is made at 4–4.5 mm (Fig. 3) so as to bend the graft at the partial cut in the form of L shaped boomerang graft (Fig. 4). This part of the vertical graft measuring 4–4.5 mm is placed on the stapes footplate and the other limb of the boomerang measuring 5.5–6 mm rests into the hypotympanum. The advantage being the vertical length of 4–4.5 mm helps to increase the middle ear space by 4 to 4.5 mm. The breadth of 2 mm fits adequately well in relation to the dimensions of the footplate of stapes (2 × 3 mm). In paediatric population instead of 10 mm length, 7–8 mm vertical strut of cartilage (with intact perichondrium on both sides) is taken and the partial thickness cut is made at 4 mm. The remaining tragal cartilage graft is sliced [6–13] with metallic thickness plate of 0.3 mm with cartilage splitter to obtain 2 sliced tragal grafts (approximately 0.3 mm and 0.5 mm thickness (assuming the tragal cartilage is 1 mm in thickness, each perichondrium 0.1 mm and after slicing with 0.3 mm we get 0.3 mm and 0.5 mm). All the measurements are done with the ASM grid [18].
Approach: Minimal invasive Transcanal endoscopic approach.
Procedure of endoscopic cartilage boomerang ossiculoplasty (Figs. 5, 6, 7 and 8, video 1,):
Fig. 3.

Partial cut on the vertical tragal cartilage graft
Fig. 4.

Creation of boomerang
Fig. 5.

Cartilage boomerang while placement
Fig. 6.

Placement of cartilage boomerang
Fig. 7.

After placement of cartilage boomerang
Fig. 8.

Sliced tragal cartilage graft for TM reconstruction
Instruments are similar to those used in microscopic ear surgery. Pinna stay suture is taken to retract the ear canal and to provide additional few millimetres for instrumental manipulation [19]. Transcanal/ endaural incision is taken depending on the access required. Tragal cartilage graft is harvested. Tympanomeatal flap is elevated. Middle ear inspected for the evaluation of the pathology and for ossicular erosion. The disease (cholesteatoma/ granulations) is cleared depending on the type of pathology (squamosal or mucosal otitis media). Inside-out atticotomy and antrostomy is done to remove cholesteatoma. In the absence of all ossicles, the prepared cartilage boomerang graft placed onto the footplate of the stapes and the other end is placed into the hypotympanum (Figs. 5, 6, 7). This graft assembly is stable. Sliced cartilage of 0.5 mm thickness kept as underlay shield graft [9, 12] for tympanic membrane reconstruction (Fig. 8). Tympanomeatal flap reposed back. Throughout the procedure, the suction is held in left hand to avoid fogging and to achieve cooling of endoscope generated heat as reported in previous study [1, 20]. Intermittent irrigation is done for cooling of endoscope as well as to achieve cleaning of endoscope lens [1, 20]. The 3 mm 14 cm Karl Storz zero degree endoscope gives a panoramic view even in narrow canals, minimising the need for canalplasty. All procedures performed are recorded for documentation. The advantage of using an endoscope holder for boomerang ossiculoplasty is dual: to incorporate the advantages of endoscope and the allowing two handed technique similar to microscopic ear surgery. Use of endoscope allows the panoramic view of the nooks and corners of the middle ear spaces allowing the total disease clearance (cholesteatoma, granulations, glue) without much bone removal. As the endoscope is mounted on the endoscope holder, both the hands are free for surgical manipulation with the left hand holding the suction and right hand holding the microear instruments. This provides the stability as well as precision while placing the cartilage boomerang graft with its one end on the footplate and the other end of boomerang in the hypotympanum.
Discussion
Chronic suppurative otitis media -squamosal disease due to cholesteatoma formation causes ossicular erosion and various other complications. Ossiculoplasty is required in between 40 and 90% of all tympanoplasties. In cases of erosion of all ossicles, we perform ossiculoplasty with tragal cartilage graft fashioned as a boomerang.
What is Boomerang and why Boomerang Shape is Required? [21]
A boomerang is a tool that has two arms at an angle. When a boomerang shaped cartilage graft is used, it not only enables sound conduction by maintaining contact between the neo-tympanum and the stapes footplate, but the apex of the boomerang is believed to act as a fulcrum providing leverage which is then transmitted to the stapes footplate. Second advantage is the stability of the graft. The hitched arm of boomerang in the hypotympanum under the inferior bony annulus gives anchoring stability to the graft and prevents displacement of the graft. Thirdly, the loss of ossicles with the absence of a mobile stapes footplate often results in a conductive hearing loss of 60 dB. A boomerang shaped graft maintains the middle ear volume for aeration with a bowing architecture from the footplate to the hypotympanum, which is believed to better withstand the poor negative pressures in the middle ear as compared with synthetic materials or struts. It also prevents the formation of adhesions between the neotympanum graft and the promontory.
Advantages of two handed endoscopic cartilage boomerang ossiculoplasty
- Advantages of Endoscopes
- Minimally invasive technique with transcanal approach
- Panoramic view of the epitympanum, mesotympanum and hypotympanum allows better visualisation for ossicular defect and its correction.
- Precise visualisation and removal of pathology allowing complete disease clearance
- Better understanding of the mucosal folds and the ventilation pathways
- Complete view of tympanic membrane and the external canal wall
- Uses of endoscope holders
- As the endoscope is mounted on the endoscope holder, it allows simultaneous use of both hands (Two handed technique) similar to microscopic ear surgery
- There is ease and comfort during the two handed transcanal endoscopic ossiculoplasty as it allows total disease clearance with stable ossicular reconstruction in a minimal invasive approach. Whereas, this is not possible with the transcanal microscopic ossiculoplasty (due to limited exposure preventing complete disease clearance unless the bone is removed by postauricular approach)
- It thus offsets the disadvantage of single handed endoscopic ear surgery as well as transcanal microscopic ossiculoplasty due to the use of Endoscope holder.
- Simultaneous use of drill and the suction possible similar to microscopic surgery
- No repeated fogging due to the suction in the non-dominant hand unlike single handed endoscopic ear surgery
- Comfort during handling and manipulation of the boomerang graft due to the two handed technique.
- Precision during cartilage boomerang graft placement (on the footplate of stapes and in hypotympanum) due to the two handed technique
- Two handed technique allows control of bleeding through continuous suction held in the non-dominant hand
- Stability of the image on the monitor
- No fatigue of the surgeon to hold the endoscope in the non-dominant hand as the endoscope is mounted on endoscope holder
- Learning curve is faster as the technique is similar to that of microscopic ear surgery with the added advantages of the endoscope.
- Advantages of tragal Cartilage boomerang placed on stapes footplate
- Cartilage graft of 15 × 15 mm suffices both for ossiculoplasty as well as for TM reconstruction.
- Partial thickness cut on the vertical cartilage strut provides the adequate angulation for creating the two arms of the boomerang for ossiculoplasty
- Gives adequate graft stability
- No displacement or extrusion of the boomerang graft as it is hitched in the hypotympanum under the inferior bony annulus
- Good hearing with post-operative air bone gap closure up to 20 dB.
- It is reinforced by a sliced tragal cartilage for TM reconstruction.
Limitations.
No depth perception.
Conclusion
Tragal Cartilage Boomerang graft is a good option for ossiculoplasty in cases of absence of stapes superstructure. The use of endoscope holder during ear surgery gives additional advantages of panoramic view of middle ear spaces due to use of endoscope along with benefits of two handed technique (similar to microscopic ear surgery). There is ease and comfort during the two handed transcanal endoscopic ossiculoplasty as it allows total disease clearance with stable ossicular reconstruction in a minimal invasive approach. It thus offsets the disadvantage of both single handed endoscopic ear surgery as well as transcanal microscopic ossiculoplasty due to the use of Endoscope holder.
Supplementary Information
Below is the link to the electronic supplementary material.
VIDEO 1 : Preparation of the Cartilage boomerang
Supplementary file1 (MP4 12699 KB)
Acknowledgements
We wish to express our gratitude to Dr Mrs Shirin M. Khan for the technical support provided and to Asim Khan for the help during proof reading and editing of the manuscript.
Author contributions
Dr Mubarak M. Khan: conceptualisation, study design, manuscript drafting; Dr Sapna Ramkrishna Parab: conceptualisation, study design, manuscript drafting.
Funding
This study was not financially supported from external sources.
Declarations
Conflict of interest
The author(s) declare that they have no competing interests. Endohold GS 201 B is registered and trademarked under the name of Dr. Mubarak M. Khan and applied for patent under the name of Dr. Mubarak M. Khan under Patent Act, India.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional committee and with the 1964 helsinski declaration and its later amendments or comparable ethical standards, Institutional Ethics Committee has approved the study.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Khan MM, Parab SR. Endoscopic cartilage tympanoplasty: a two-handed technique using an endoscope holder. Laryngoscope. 2016;126:1893–1898. doi: 10.1002/lary.25760. [DOI] [PubMed] [Google Scholar]
- 2.Khan MM, Parab SR. Concept, design and development of innovative endoscope holder system for endoscopic otolaryngological surgeries. Indian J Otolaryngol Head Neck Surg. 2015;67(2):113–119. doi: 10.1007/s12070-014-0738-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khan MM, Parab SR. Novel concept of attaching endoscope holder to microscope for two handed endoscopic tympanoplasty. Indian J Otolaryngol Head Neck Surg. 2016;68(2):230–240. doi: 10.1007/s12070-015-0916-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Khan MM, Parab SR. Primary cartilage tympanoplasty: our technique and results. Am J Otolaryngol. 2011;32(5):381–387. doi: 10.1016/j.amjoto.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 5.Khan MM, Parab SR. Reinforcement of sliced tragal cartilage perichondrium composite graft with temporalis fascia in type I tympanoplasty: our techniques and results. J Rhinolaryng-Otologies. 2013;1:57–62. [Google Scholar]
- 6.Khan MM, Parab SR. Day care ear surgery: our experience of 4 years. Indian J Otolaryngol Head Neck Surg. 2012;64(3):280–284. doi: 10.1007/s12070-011-0303-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khan MM, Parab SR. Sliced Island tragal cartilage perichondrial composite graft: early results and experience. J Rhinolaryng-Otologies. 2014;2:4–9. [Google Scholar]
- 8.Khan MM, Parab SR. Comparative study of sliced Tragal cartilage and temporalis fascia in type i tympanoplasty. J Laryngol Otol. 2015;129(1):16–22. doi: 10.1017/S0022215114003132. [DOI] [PubMed] [Google Scholar]
- 9.Khan MM, Parab SR. Average thickness of tragal cartilage for slicing techniques in tympanoplasty. J Laryngol Otol. 2015;129(05):435–439. doi: 10.1017/S0022215115000055. [DOI] [PubMed] [Google Scholar]
- 10.Parab SR, Khan MM. Endoscopic management of tympanic membrane retraction pockets: a two handed technique with endoscope holder. Indian J Otolaryngol Head Neck Surg. 2019;71(4):504–511. doi: 10.1007/s12070-019-01682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parab SR, Khan MM. Modified endoscope holder for two handed endoscopic ear surgery. Indian J Otolaryngol Head Neck Surg. 2020 doi: 10.1007/s12070-020-01841-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Parab SR, Khan MM. New cartilage slicer for slicing techniques in tympanoplasty: design and applications. Indian J Otolaryngol Head Neck Surg. 2018;70(4):515–520. doi: 10.1007/s12070-018-1467-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zaidi A, Khan MM, Parab SR. The goat model for exclusive two handed endoscopic middle ear surgery training: a novel technique. Indian J Otolaryngol Head Neck Surg. 2019;71(2):1478–1484. doi: 10.1007/s12070-018-1563-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Parab SR, Khan MM. Endoscope holder-assisted endoscopic coblation tonsillectomy. Eur Arch Otorhinolaryngol. 2020;277(11):3223–3226. doi: 10.1007/s00405-020-06249-4. [DOI] [PubMed] [Google Scholar]
- 15.Khan MM, Parab SR. Endoscopic septoplasty—two handed technique with endoscope holder: a novel approach. Indian J Otolaryngol Head Neck Surg. 2016;68(4):475–480. doi: 10.1007/s12070-016-0997-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.https://en.wikipedia.org/wiki/Gas_spring
- 17.https://en.wikipedia.org/wiki/Rack_and_pinion
- 18.Parab SR, Khan MM, Rana AK. Accurate and specific measuring grid for otorhinolaryngological surgeries. Indian J Otolaryngol Head Neck Surg. 2020 doi: 10.1007/s12070-020-01886-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Parab SR, Khan MM. Pinna stay suture in two handed endoscopic ear surgery: our experience. Am J Otolaryngol. 2020;41(5):102582. doi: 10.1016/j.amjoto.2020.102582. [DOI] [PubMed] [Google Scholar]
- 20.Kozin ED, Lehman A, Carter M, et al. Thermal effects of endoscopy in a human temporal bone model: implications for endoscopic ear surgery. Laryngoscope. 2014;124(8):E332–9. doi: 10.1002/lary.24666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Elaprolu S, Alexander A, Ganesan S, Manu CB. Effect of a boomerang-shaped conchal cartilage graft for type three tympanoplasty on hearing. Int Arch Otorhinolaryngol. 2020 doi: 10.1055/s-0040-1712934. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
VIDEO 1 : Preparation of the Cartilage boomerang
Supplementary file1 (MP4 12699 KB)