

Abstract
Hamartoma presenting in the larynx is a rare entity. The common presentation of such a lesion may include stridor, hoarseness of voice, choking sensation, dyspnea and in children, failure to thrive. It is a benign lesion and can be confused with other benign lesions like lipoma, fibroma, chondromas etc. Pathologically it consists of a mesodermal compartment and a granular compartment. Hamartomas mainly occur in pediatric age group. When it occurs in adults, males are more commonly affected than females. With very few cases reported so far, we present a case of laryngeal hamartoma presenting in a lady with progressive hoarseness of voice as a presenting feature.
Keyword: Laryngeal hamratoma
Introduction
Laryngeal hamartoma is a very rare lesion. The term Hamartoma was derived from the greek word "hamartanein" which means to go wrong and introduced by Al brecht in 1904 [4]. The usual presenting features include change in voice, stridor and difficulty in breathing. The recurrence rate of Laryngeal Hamartoma is reported in 20% of cases. Only 35 cases of well documented Laryngeal Hamartoma cases are reported so far [2].
Case Report
A 50 year old lady presented with chief complaints of hoarseness of voice since 1 year which was gradually progressive in nature. There was no history of dysphagia or difficulty in breathing. On videolaryngoscopy (Fig. 1) a submucosal bulge involving the right false cord, ventricle and true cords was seen, with restricted Right vocal cord movement. The left vocal cord was normal. Phonatory gap was seen on phonation. Rest of larynx and hypopharynx was normal. No lymphadenopathy was seen. Rest of ENT and systemic examination was within normal limits.
Fig. 1.
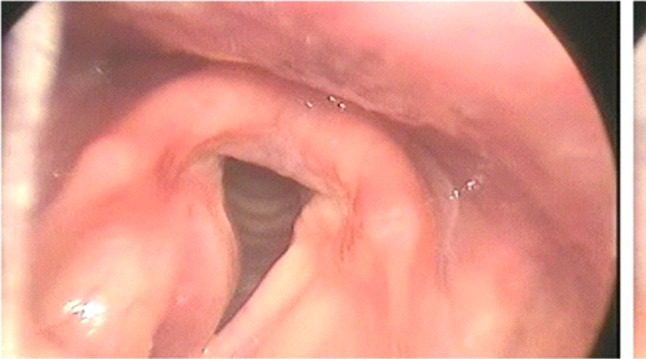
Videolaryngoscopy showing growth involving right true and false cords on ant 2/3rd
On MRI (Fig. 2) a focal lesion was noted involving right false and true cords showing fat signal intensities within central and posterolateral portion appearing hyper intense on T1W1 and hypointense on fat sat images and measured about 1.6 × 1.1 cm.
Fig. 2.

MRI showing posterior contrast T1 fat saturated image showing homogenous predominant peripheral contrast enhancement
The patient was posted for surgical excision under general anaesthesia. Direct laryngoscopy was performed and the lesion visualized. Using suspension microlaryngoscopy, Incision placed on the mucosa at the level of Right false cord. The lesion was exposed and partially dissected. However, because of the lateral extension and lack of visibility, the procedure was converted into midline thyrotomy approach. An incision was placed at the level of mid- thyroid cartilage (Fig. 3). Soft tissue and straps dissected, thyroid cartilage opened in midline lesion visualized extending from Right false cord to subglottis, excised and sent for HPE. Wound closure was done in layers and the patient was extubated on table. Post operative period was uneventful and patient discharged the next day in stable condition. She was kept nil per oral for 10 days and ryles tube was removed on the 10th post operative day.
Fig. 3.

Intra Operative picture of the Hamartoma specimen
The Histopathology report showed partly circumscribed lesion composed of nests of mature adipocytes in a fibrous connective tissue stroma.A few scattered thick walled blood vessels were seen with skeletal muscle fibres of varying diameter (Fig. 4). Focally in the periphery a moderately dense lymphocyte infiltrate was seen and was reported as Benign Hamartomatous lesion of larynx.
Fig. 4.

Histopathology section showing adipocytes, scattered skeletal muscle fibres congested blood vessels
Discussion
Dysphonia, with the cardinal symptom of hoarseness, has a prevalence of around 1% among patients in general [1] and a lifetime prevalence of approximately 30%.
The causes of hoarseness are [3]:
Acute and chronic laryngitis (accounting for 42.1% and 9.7% of cases respectively).
Functional dysphonia (30%).
Benign and malignant tumors (10.7–31.0% and 2.2–3.0% respectively).
Neurogenic factors such as vocal cord paralysis (2.8–8%).
Physiological aging (2%).
Psychogenic factors (2.0–2.2%).
Hamartoma term was derived from greek word "hamartanein" means to go wrong and introduced by Al Brecht in 1904 [4]. Hamartomas have been described as occurring throughout the body, however they remain a rare finding in the head and neck region. The lesion usually presents as a Submucosal mass with ill-defined margins. The symptoms caused by such lesions are related to the affected site; they are not pathognomonic and when presenting in larynx may include stridor, hoarseness, choking, dyspnea and, in children, failure to thrive [5]. In our patient the presenting symptom was hoarseness of voice from 1 year which was progressive in nature. Males are more commonly affected than Females. It is seen mostly in early childhood and middle age (39–56 years) [6].
Pathologically hamartomas can be classified into most common Mesodermal component element and less common Granular or epithelial element. The present case showed more of Mesodermal component. The surgical approach planned was microlaryngeal excision. However due to lateral extension of the lesion, laryngofissure surgery or thyrotomy was performed. Depending upon the size of the tumor the management also differs from Conservative modes of treatment like Laser to Partial and Complete laryngectomies.
Although the recurrence of Laryngeal Hamartoma is rare but in a study conducted by Le Ber and Stouthave [7] reported about 20% recurrence rate in Pediatric age groups in different organs of the body like kidney, liver, upper and lower extremities, etc., and termed it as "Benign Mesenchymomas".
Conclusion
Laryngeal hamartoma are very rare benign lesions. They can be confused with other Benign lesions like fibroma, chondromas, schwanommas etc. Diagnosis can only be made on Histopathological examination. The treatment includes conservative approach to partial and complete laryngectomies depending upon size of tumor and involvement of neighbouring structures.
Funding
No funding was obtained from any source.
Declarations
Conflict of interest
There is no conflict of interest with anyone.
Ethical approval
This report has been prepared with ethical standards and with due consent of the patient.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Saud Ahmed, Email: drsaudent@gmail.com.
S. Sharfa Afreen, Email: shaiksharfaafreen@yahoo.com.
S. R. Raja Parthiban, Email: indianpathology@gmail.com.
H. K. Anand, Email: dranandhk@yahoo.com
Quddusia Fatima, Email: quddusia.bushra@gmail.com.
Purushottam Chavan, Email: drplchavan@gmail.com.
References
- 1.Cohen SM, Kim J, Roy N, Asche C, Courey M. Prevalence and causes of dysphonia in a large treatment—seeking population. Laryngoscope. 2012;122:343–348. doi: 10.1002/lary.22426. [DOI] [PubMed] [Google Scholar]
- 2.Amir JA, Sheikh SS. Mesenchymal hamartoma of the larynx: a rare case report and review of literature. Case Rep Clin Pathol. 2015 doi: 10.5430/crcp.v2n3p40. [DOI] [Google Scholar]
- 3.Reiter R, Hoffmann TK, Pickhard A, Brosch S. Hoarse ness—causes and treatments. Dtsch Arztebl Int. 2015;112:329–337. doi: 10.3238/arztebl.2015.03293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Albrecht E (1904) Uber hamartoma. Verh Dtsch Geo Pathol 7:153–157
- 5.Windfuhr JP. Laryngeal hamartoma. Acta Otolaryngol. 2004;124(3):301–308. doi: 10.1080/00016480310014831. [DOI] [PubMed] [Google Scholar]
- 6.Işık Gönül I, Asal K, Ceylan A, et al. Hamartoma of the larynx: an unusual cause of upper airway obstruction. Eur Arch Otorhinolaryngol. 2004;261:435–438. doi: 10.1007/s00405-003-0712-x. [DOI] [PubMed] [Google Scholar]
- 7.Le Ber MS, Stout AP. Benign mesenchymomas in children. Cancer. 1962;15:598–605. doi: 10.1002/1097-0142(196205/06)15:3<598::AID-CNCR2820150321>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]