

Abstract
In this study we aimed to compare external lateral osteotomy technique vs. internal one in the rhinoplasty. In this before-after clinical trial study 30 patients who were candidates for rhinoplasty involved. In each patient, external lateral osteotomy was performed on one side and internal lateral osteotomy was performed on the other side randomly. Information, including patients’ age, sex, grade of edema and ecchymosis 1, 3, and 7 days after the surgery, and the type of lateral osteotomy, the amount of step deformity, the need for the specialist intervention, nasal bone mobility, and flail nasal bone was recorded and analyzed. The incidence of edema and ecchymosis on the first and the third day was statistically lower in the external method (P value < 0.001). Although the incidence of edema and ecchymosis on the seventh day was lower in the external method, it was not statistically significant (P value > 0.05). Forty seven percent of patients in the internal method and 36% of patients in the external method had step deformity (p value < 0.001). Fifty percent of patients in the internal method and 41% of patients in the external method needed the specialist intervention (p value > 0.05). Seventy four of patients in the internal method and 83% of patients in the external method had nasal bone mobility (p value > 0.05). Out of 30 patients, only one had flail nasal bone. Based on our findings, the external technique is suggested as a more effective and convenient method with less complications for inexperienced surgeons.
Keywords: External lateral osteotomy, Internal lateral osteotomy, Rhinoplasty
Introduction
Today, rhinoplasty is the most common cosmetic surgery worldwide. Though various techniques are used to do this procedure, the process is similar. One of the major parts of rhinoplasty is lateral osteotomy, which is usually performed at the end of rhinoplasty and after modification of nasal hump and tip [1]. The purpose of lateral osteotomy is to narrow the dorsum after removing the hump, reduce the width of the dorsum, and straighten the nasal bones. Therefore, osteotomy technique should be accurate, performable and safe, so that it can be effective in reducing postoperative complications, such as ecchymosis and edema [2]. Lateral osteotomy, no matter which technique is used, forces a lot of energy and trauma on the bone and soft tissues of the nose, so it should be done in a way that does not cause instability of the nasal bone and descent of the bones into the nasal cavity [3]. Lateral osteotomy is performed by various techniques, the most important of which are external osteotomy or external percutaneous perforating osteotomy and internal continuous osteotomy [4]. There is no consensus on the superior technique and surgeons have different opinions in this regard. Some researchers, such as Rees and Ford, advocate the external osteotomy, arguing that it reduces trauma to soft tissues, mucosa, and periosteum [5]. Tardey, on the other hand, is a proponent of the internal osteotomy and believes that this technique reduces edema, ecchymosis, and mucosal damage [6]. Complications of rhinoplasty can disturb patients' social and occupational functioning [7]. In addition to complications, such as blurred vision and nasal stuffiness, that may result from excessive edema. periorbital edema and ecchymosis can slow the healing of other tissues and lead to permanent pigmentation [8]. The presence of edema and ecchymosis in the nasal area, although not permanent, can affect the early aesthetic outcome. In addition, edema post-rhinoplasty may even last longer than usual, leading to patient and surgeon dissatisfaction [9]. Nasal osteotomy is the most important cause of periorbital edema and ecchymosis because damage to the angular arteries that pass through the osteotomy area performed in standard rhinoplasty [10]. Therefore, it is better to perform osteotomy using a technique with least complications. Considering the disagreement about the incidence of edema and ecchymosis and the efficacy of external lateral osteotomy versus internal lateral osteotomy in rhinoplasty, we aimed to compare these two techniques which were done by inexperienced surgeons.
Materials and Methods
After approval by the local ethics committee and obtaining written informed consent, in this before-after clinical trial study 30 patients who were candidates for rhinoplasty involved. Patients with a history of nasal surgery (rhinoplasty, nose reconstruction, etc.), nasal trauma, coagulation disorders, and HTN or DM and those consuming medications such as OCP and ASA were excluded. In each patient, external lateral osteotomy was performed on one side and internal lateral osteotomy was performed on the other side randomly. An open surgical procedure was performed for all the patients, and all the surgeries were controlled by the same surgeon (first author). All surgeries were performed under general anesthesia. At the beginning of the operation and 10 min before performing lateral osteotomy, adrenaline 1.100000 and 1% lidocaine were infiltrated in lateral osteotomy site. Periosteal elevation was not done in either technique patients. Before lateral osteotomy, the osteotomes were completely sharpened and cleaned. In all cases, after removal of the hump and performing tip plasty, median osteotomy was done by internal osteotomy technique. External lateral osteotomy was conducted with 2 mm osteotome on one side and doing interrupted osteotomy from pyriform aperture to intercanthal line. Green stick facture was done by finger push. Internal osteotomy was performed on the other side of nose with a 3 mm straight sharp unprotected osteotome from the pyriform aperture to intercanthal line. In all patients, immediately after osteotomy, nasal pack was applied into both sides of the nose to reduce ecchymosis. After doing lateral osteotomy by internal and external osteotomy techniques by a fourth-year resident of ENT, both osteotomy techniques were evaluated in terms of mobility of nasal bone, step deformity, flail nasal bone, and the need for intervention by the surgeon (first author). The patients received cephalexin capsule (500 mg) every 6 h for 7 days and acetaminophen for 2 days. All patients had nasal splint for seven days. Edema and ecchymosis were evaluated by a surgeon who was blinded to the study 1, 3, and 7 days after the surgery. Edema grading was performed using SPREE questionnaire.
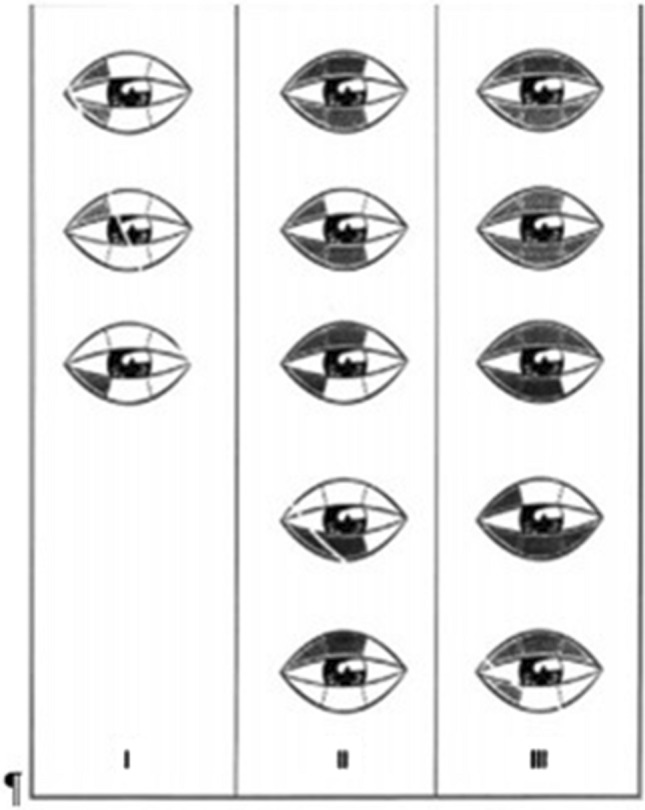
Based on degree of coverage of iris and pupil by upper and lower eyelids, edema grading was defined as follows:
No coverage of iris
Little overage of iris with eyelids
Complete coverage of iris with eyelids
Complete eye closure (Fig. 1)
Fig. 1.

Edema grading based on SPREE questionnaire
Ecchymosis grading was done based on a questionnaire developed by Kara and amount of discoloration in eyelids as follows:
Limited to 1/3 medial upper or lower eyelid
Limited to 1/3 middle upper or lower eyelid
Limited to 1/3 lateral upper or lower eyelid (Fig. 2)
Fig. 2.
Ecchymosis grading
In all cases, the highest grade was recorded without considering right or left side. Information, including patients’ age, sex, grade of edema and ecchymosis 1, 3, and 7 days after the surgery, and the type of lateral osteotomy (internal or external), and the amount of step deformity, the need for the specialist intervention in performing osteotomy, nasal bone mobility, and flail nasal bone, was recorded in a pre-prepared checklist. All data were analyzed by SPSS (version 22) and t-test and paired t-test were applied. P value < 0.05 was considered as a significant level.
Results
Thirty patients were included in this clinical trial study with a mean age of (28.43 ± 6.49) years old. The oldest patient was 43 years old and the youngest one was 17 years old. Regarding gender, 15 patients were female and 15 were male. Internal lateral osteotomy was performed on the left in 18 patients (60%), and internal lateral osteotomy was performed on the right in 12 patients (40%). The incidence of edema on the first day was statistically lower in the external method (P value < 0.001). In addition, the incidence of edema on the third day was significantly lower in the external method (P value = 0.013). Although the incidence of edema on the seventh day was lower in the external method, it was not statistically significant (P value = 0.083). Similarly, the incidence of ecchymosis on the first day was significantly lower in the external method (P value < 0.001). The incidence of ecchymosis on the third day was also significantly lower in the external method (P value < 0.001). Although the incidence of ecchymosis on the seventh day was lower in the external method, it was not statistically significant (P value = 0.096). As shown in Fig. 3. 47% of patients in the internal method and 36% of patients in the external method had step deformity, leading to a significant difference between groups (p value < 0.001) and lower incidence in external method. Fifty percent of patients in the internal method and 41% of patients in the external method needed the specialist intervention. Although it was lower in the external method, it was not statistically significant (p value < 0.629). In terms of nasal bone mobility, 74% of patients in the internal method and 83% of patients in the external method had nasal bone mobility, but it did not lead to a statistically significant difference between two methods (p value < 0.453). Out of 30 patients, only one had flail nasal bone (Table 1).
Fig. 3.

Post operation periorbital edema and ecchymosis in patient under right side lateral osteotomy surgery via internal method
Table 1.
Percentages of under-study patients in the evaluated items
| Variables | Lateral osteotomy technique | |||
|---|---|---|---|---|
| Internal | External | |||
| Edema on first day | Grade | 0 | 3.3 | – |
| 1 | 10 | 40 | ||
| 2 | 50 | 56.7 | ||
| 3 | 33.3 | 3.3 | ||
| 4 | 3.3 | – | ||
| Edema on third day | Grade | 0 | 3.3 | 10 |
| 1 | 43.3 | 56.7 | ||
| 2 | 40 | 30 | ||
| 3 | 13.3 | 3.3 | ||
| 4 | – | – | ||
| Edema on seventh day | Grade | 0 | 73.3 | 83.3 |
| 1 | 26.7 | 16.7 | ||
| 2 | – | – | ||
| 3 | – | – | ||
| 4 | – | – | ||
| Ecchymosis on first day | Grade | 0 | – | 3.3 |
| 1 | 6.7 | 13.3 | ||
| 2 | 13.3 | 40 | ||
| 3 | 43.3 | 36.7 | ||
| 4 | 36.7 | 6.7 | ||
| Ecchymosis on third day | Grade | 0 | 3.3 | 3.3 |
| 1 | 13.3 | 30 | ||
| 2 | 10 | 50 | ||
| 3 | 63.3 | 10 | ||
| 4 | 10 | 6.7 | ||
| Ecchymosis on seventh day | Grade | 0 | 30 | 43.3 |
| 1 | 60 | 50 | ||
| 2 | 6.7 | 6.7 | ||
| 3 | 3.3 | – | ||
| 4 | – | – | ||
| Step deformity | 47 | 36 | ||
| Mobility of nasal bone | 74 | 83 | ||
| Specialist intervention | 50 | 41 | ||
Discussion
Modification and reshaping of the nasal bones is an important element in rhinoplasty surgery [3]. Therefore, choosing the best technique to perform osteotomy with least complications has always been attended by the surgeons. In addition, the selection of lateral osteotomy technique by different surgeons depends more on experience and comfortability of that technique than on articles’ findings [11]. The selected technique in any case should have accurate, ideal, and reliable results and minimize postoperative complaints. Postoperative edema and ecchymosis are the most common complaints of patients [12]. Although they are temporary and do not cause pain for the patients, patients may feel uncomfortable and anxious to appear in the society. Sometimes the surgeon's skill plays an important role in reducing these complications [13]. Several factors are involved in postoperative edema and ecchymosis, the most important of which is the type of osteotomy. Various types of osteotomy techniques and medical treatments are suggested to reduce these complications. Lateral osteotomy methods are of two main types, namely internal and external [14]. The external lateral osteotomy was first performed by Goria in 1955 and was welcomed by many surgeons [5] since this technique was precise and more controllable. It has been also shown that this technique causes less tissue and mucosal damage. In addition, due to periosteal preservation, it provides better control over fracture formation and maintains the stability of fractured parts due to periosteal connections. The internal technique using micro-osteotome has been used by some other researchers. Proponents of the internal technique believe that if this technique is performed with high accuracy, then it will be associated with less edema and ecchymosis [15]. Denneny and Tardy also used a 2–3 mm osteotome for internal osteotomy and stated that this technique was associated with less bleeding and edema [6]. As mentioned above, each osteotomy technique has its own advantages if performed precisely. Proponents of internal osteotomy technique, including Tardy and Denney and Yucel [8], have preferred internal osteotomy technique in lateral osteotomy since it is associated with less edema, ecchymosis, and soft tissue damage. However, advocates of external osteotomy preferred this technique since it results in less nasal mucosa damage. Similarly, in a study by Hashemi [16], the external technique was introduced as a better technique given that it was associated with less edema and ecchymosis, no asymmetry, and adequate bone medialization. Vikas Sinha also compared internal and external osteotomy techniques and described external osteotomy technique as a better technique because it was easy to carry out, caused less damage to the nasal mucosa, and was associated with less edema and ecchymosis [17]. Yazdani et al., studied the incidence of rupture in the nasal mucosa, edema, and ecchymosis in internal and external osteotomy techniques [18]. They yielded that the complications and severity of rupture in the nasal mucosa, edema, and ecchymosis reduced in the external group. However, this decrease was not statistically significant. Gholami et al., also examined step deformity in their study between the internal and external lateral osteotomy methods [19]. They did not observe a significant difference between the internal and external groups in this regard.
According to the mentioned studies, each surgeon, based on her/his skills and experience, selects one of the osteotomy techniques with least complications as a preferred one and uses it in rhinoplasty. In contrast with previous studies, the variable of experience and skill was omitted in our study since the surgeries were performed by a last year ENT resident. Therefore, we could suggest the most effective method inducing least complications for inexperienced surgeons. According to the results, the incidence of edema and ecchymosis was less one and three days after surgery in the external method. On the seventh day, there was no significant difference between two methods regarding the incidence of edema and ecchymosis. From the viewpoints of adequate bone mobility and the need for specialist intervention after osteotomy, comparing the findings yielded from employed internal and external methods revealed that there is no significant difference between those methods statistically; whereas, the bone mobility was better in the external technique than in the internal one and the need for specialist intervention was less in the external method step deformity rate in the external technique was significantly lower than the internal one and only one case of flail nasal bone was reported. According to the results of our study and previous studies revealing less damage to nasal mucosa tissue, periosteal preservation, and a more controlled fracture with fewer steps in the external technique, the external lateral osteotomy technique is suggested as a convenient and effective method with less complication for inexperienced surgeons.
Conclusion
The best technique in lateral osteotomy can vary depending on the surgeon’s experience and skill and the surgical instruments available. However, in the case of inexperienced surgeons, the results of this study showed that in general there was difference between internal and external techniques. In this study, on the first and third days, the incidence of edema and ecchymosis was significantly lower in the external group and the rate of step deformity in the external method was significantly less than the internal method. Based on our findings, the external technique is suggested as a more effective and convenient method with less complications for inexperienced surgeons.
Declarations
Conflict of interest
Authors have no conflicts of interest.
Ethical Approval
Study protocol was in accordance with the latest Declaration of Helsinki for medical research involving human subjects and was approved by the ethics committee of Shahid Sadoughi University of medical sciences. Ethical approval code: IR.SSU.REC.1399.310
Human or Animal Rights
This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all participants of the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Schlabe J, Echlin K, Atherton D. A comparison of piezo surgery osteotomies with conventional internal osteotomies as performed by trainee surgeons: a cadaveric study. Annals Royal Colleg Surg England. 2021;103(4):272–277. doi: 10.1308/rcsann.2020.7120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Meymaneh Jahromi A, Nour Elahian M, Seyedi M, Salehi M, Afzal Aghaei M. Comparison between external and internal lateral osteotomy regarding postoperative edema and ecchymosis in rhinoplasty. Iran J Otorhinolaryngol. 2006;18(2):44. [Google Scholar]
- 3.Erişir F, Tahamiler R. Lateral osteotomies in rhinoplasty: a safer and less traumatic method. Aesthetic Surg J. 2008;28(5):518–520. doi: 10.1016/j.asj.2008.07.007. [DOI] [PubMed] [Google Scholar]
- 4.Kiliç C, Tuncel Ü, Cömert E, Sencan Z. Effect of the rhinoplasty technique and lateral osteotomy on periorbital edema and ecchymosis. J Craniofacial Surg. 2015;26(5):e430–e433. doi: 10.1097/SCS.0000000000001885. [DOI] [PubMed] [Google Scholar]
- 5.Thomas JR, Griner NR, Remmler DJ. Steps for a safer method of osteotomies in rhinoplasty. Laryngoscope. 1987;97(6):746–747. doi: 10.1288/00005537-198706000-00021. [DOI] [PubMed] [Google Scholar]
- 6.Tardy ME, Denneny JC. Micro-osteotomies in rhinoplasty—a technical refinement. Facial Plast Surg. 1984;1(02):137–145. doi: 10.1055/s-0028-1085244. [DOI] [Google Scholar]
- 7.Dionyssiou D. A simple and effective combined method for the management of postrhinoplasty ecchymosis and edema. Plast Reconstr Surg. 2008;121(6):2176. doi: 10.1097/PRS.0b013e31817073a1. [DOI] [PubMed] [Google Scholar]
- 8.Yücel ÖT. Which type of osteotomy for edema and ecchymosis: external or internal? Ann Plast Surg. 2005;55(6):587–590. doi: 10.1097/01.sap.0000185396.94875.4a. [DOI] [PubMed] [Google Scholar]
- 9.van Loon B, van Heerbeek N, Maal TJ, Borstlap WA, Ingels K, Schols J, et al. Postoperative volume increase of facial soft tissue after percutaneous versus endonasal osteotomy technique in rhinoplasty using 3D stereophotogrammetry. Rhinology. 2011;49(1):121. doi: 10.4193/Rhino10.056. [DOI] [PubMed] [Google Scholar]
- 10.Gun R, Yorgancılar E, Yıldırım M, Bakır S, Topcu I, Akkus Z. Effects of lidocaine and adrenaline combination on postoperative edema and ecchymosis in rhinoplasty. Int J Oral Maxillofac Surg. 2011;40(7):722–729. doi: 10.1016/j.ijom.2011.02.022. [DOI] [PubMed] [Google Scholar]
- 11.Mehdizadeh M, Ghassemi A, Khakzad M, Mir M, Nekoohesh L, Moghadamnia A, et al. Comparison of the effect of dexamethasone and tranexamic acid, separately or in combination on post-rhinoplasty edema and ecchymosis. Aesthetic Plast Surg. 2018;42(1):246–252. doi: 10.1007/s00266-017-0969-x. [DOI] [PubMed] [Google Scholar]
- 12.Zojajy M, Alani N, Abdi-Soofi S, Akbari-Delmaghani N. Does injection of lidocaine with 1/100000 epinephrine immediately before lateral osteotomy reduce post-operative periorbital edema and ecchymosis in rhinoplasty. Novelty Biomed. 2014;2(2):59–63. [Google Scholar]
- 13.Gurlek A, Fariz A, Aydogan H, Ersoz-Ozturk A, Eren AT. Effects of different corticosteroids on edema and ecchymosis in open rhinoplasty. Aesthetic Plast Surg. 2006;30(2):150–154. doi: 10.1007/s00266-005-0158-1. [DOI] [PubMed] [Google Scholar]
- 14.Xu F, Zeng W, Mao X, Fan G-K. The efficacy of melilotus extract in the management of postoperative ecchymosis and edema after simultaneous rhinoplasty and blepharoplasty. Aesthetic Plast Surg. 2008;32(4):599–603. doi: 10.1007/s00266-008-9149-3. [DOI] [PubMed] [Google Scholar]
- 15.Saedi B, Sadeghi M, Fekri K. Comparison of the effect of corticosteroid therapy and decongestant on reducing rhinoplasty edema. Am J Rhinol Allergy. 2011;25(4):e141–e144. doi: 10.2500/ajra.2011.25.3601. [DOI] [PubMed] [Google Scholar]
- 16.Hashemi M, Mokhtarinezhad F, Omrani MA (2005) Comparison between external versus internal lateral osteotomy in rhinoplasty. J Res Med Sci (JRMS) 10(1)
- 17.Sinha V, Gupta D, More Y, Prajapati B, Kedia B, Singh SN. External vs. internal osteotomy in rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2007;59(1):9–12. doi: 10.1007/s12070-007-0002-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yazdani M, Bohluli B, Sarkarat F, Nowruzi A, Davoudmanesh Z (2017) Evaluation of the effect of internal and external osteotomy on the amount of mucosal rupture, edema, and ecchymosis in rhinoplasty. J Craniomaxillofac Res 4(1)
- 19.Gholami M, Vaezi A. Comparison of the effects of external and internal lateral nasal osteotomies on ecchymosis, periorbital edema, and step off deformity after rhinoplasty. World J Plastic Surg. 2019;8(3):345. doi: 10.29252/wjps.8.3.345. [DOI] [PMC free article] [PubMed] [Google Scholar]