

Abstract
Background
The study aimed to compare the dentoskeletal effects of Vanbeek Activator, Herbst, Twin-Block and Mandibular Advancement with clear aligners in children with skeletal Class II malocclusions.
Methods
A sample with sixty-three patients (37 males, 26 females) was included and divided into untreated control group (C, n = 12), Vanbeek Activator group (V, n = 14), Herbst group (H, n = 11), Twin-Block group (TB, n = 12) and MA group (MA, n = 14). Cephalometric analysis and Johnston Pitchfork analysis were performed to quantify the skeletal and dentoalveolar components in molar relationship and overjet correction. Compare the differences of cephalometric data and Johnston-analysis data.
Results
The treatment changes showed significant differences in SNB, FH-NP, NA-PA, Co-Go, Co-Pog, ANB, lower facial height ratio, U1-PP, U6-PP, L1-MP and U1-L1. All the appliances improved overjet relationships significantly (Vanbeek, Herbst, Twin-Block and MA were 2.77 mm, 5.53 mm, 4.73 mm and 3.66 mm respectively) with significant retraction of maxillary incisors. The lower incisor displacement of group V and MA was negative, while that of group H and TB was positive and there were significant differences. Molar relationships were also improved by 3.45 mm, 6.85 mm, 3.48 mm and 0.92 mm for Vanbeek, Herbst, Twin-Block and MA. Mandible displacement showed a trend of group H > TB > V > MA. The displacement of maxillary molars in group H was greater than that in group C, TB and MA, and that of mandibular ones was greater than that in group C, V and MA, significantly. Herbst, Twin-Block and MA have more significant dentoalveolar effect than Vanbeek, while Vanbeek has more skeletal effect than the others especially in restraining maxillary growth.
Conclusions
Four appliances are all effective in mandibular advancement, modification of class II molar relationship and deep overjet, with unavoidable increase in lower facial ratio. Vanbeek Activator has the most skeletal effects. Vanbeek and MA have a good control of mandibular incisors while more compensatory lower incisors proclination in Herbst and Twin-Block. Herbst has greater maxillary molar distalization. MA allows aligning and leveling meanwhile leading the mandible forward.
Keywords: Class II malocclusion, Clear aligners, Functional appliances, Cephalometric, Johnston’s Pitchfork Analysis
Introduction
Skeletal Class II malocclusion is a common orthodontic problem, mostly the mechanism of which is hypoplasia or retraction of the mandible. Differing from the epiphyseal plates of long bones, the condylar cartilage responds positively to mechanical stimulation [1]. Therefore, for such adolescent patients, the ideal treatment method is enhancing the growth and development potential of the condyle to correct the sagittal dysregulation of both jaws and reduce the possibility of orthognathic surgery in adulthood. Functional appliance has been used to correct skeletal class II malocclusion with a history over 100 years, since Robin and Andresen found it effective in stimulating mandibular growth [2].
Various appliances, such as Activator, Herbst and Twin-Block, would produce a combined effect of skeletal and dentoalveolar changes, because they are supported directly by teeth instead of bone. Dentoalveolar effects are ascribed to retrusion of upper anterior incisors and protrusion of lower incisors [3–5], while skeletal effects are well known as the expected correction, such as mandibular advancement and elongation. Mandible clockwise rotation and increase of lower facial height often occurred meanwhile, which is detrimental to long-face patients. Headgear is always believed as one of the most effective methods for maxilla growth inhibition and vertical control, Vanbeek Activator, as a modification of Headgear-Activator, placing the extraoral bow directly into the plastic base and moving it forward to canine and first premolar region from molar region grew out of that. Vanbeek Activator combined with high-pull headgear could actualize vertical dimension and occlusal plane control [6].
In recent years an invisible appliance called Invisalign Mandibular Advancement (MA) implemented by Align Technology™ has been gradually put into clinical use, which could align teeth while repositioning the lower jaw to the forward extension with a “precision wing brace”. Compared with traditional appliances, MA has good aesthetics, high wearing comfort, higher accuracy and can complete orthopedic and orthodontic treatment at the same time. MA appears to be effective in the treatment of class II malocclusions with mandibular retrusion [7–9]. Like functional appliances, the correction of occlusion relationships is combined skeletal and dental effects, and Sabouni et.al found that the skeletal changes may be minor [10].
The actual effect of functional appliances has always been a controversial topic. Some previous studies focused on common traditional functional appliances, but limited studies were based on MA. Therefore, this retrospective study aimed to deeply compare the skeletal and dentoalveolar effects of MA, Vanbeek Activator, Herbst and Twin-Block in children with Skeletal Class II Malocclusion.
Materials and methods
Subjects
In this retrospective study, a sample of 63 patients (Table 1) was collected from the Class II patients who were treated by Dr. Min Zhu. The inclusion criteria included skeletal class II malocclusion with ANB greater than 4°; increased overjet greater than 5 mm; Angle class II molar and canine relationship; cervical vertebral maturation (CVM) CVM2 and no history of orthodontic treatment before. All the cases were divided into Vanbeek Activator group (V, n = 14), Herbst group (H, n = 11), Twin-Block group (TB, n = 12) and MA group (MA, n = 14) according to the therapeutic options. And 12 untreated subjects were selected as control group to assess the effect of growth.
Table 1.
Sample characteristics
| Group | Boys(n) | Girls(n) | Age at T1 (y) | Interval (T2 − T1) (m) |
|---|---|---|---|---|
| Vanbeek | 7 | 7 | 10.71 ± 1.44 | 7.28 ± 2.30 |
| Herbst | 4 | 7 | 11.55 ± 0.69 | 10.18 ± 3.06 |
| Twin-Block | 7 | 5 | 11.00 ± 1.04 | 10.16 ± 5.46 |
| MA | 12 | 2 | 12.11 ± 1.16 | 22.84 ± 8.98 |
| Control | 7 | 5 | 10.41 ± 0.90 | 10.25 ± 3.74 |
Cephalometric method
All the included subjects have taken lateral cephalograms before (T1) and immediately after treatment (T2). Every radiograph was traced 3 times on different times by the same examiner using Dolphin Imaging software. 20 dentoalveolar measurements were calculated, including SNA, SNB, ANB, mandibular plane angle (MP-FH), facial angle (FH-NP), angle of convexity (NA-PA), Co-Go, Go-Pog, Y-Axis angle, lower facial height ratio, vertical ratio (ALFH/PLFH), P-A face height (S-Go/N-Me), maxillary incisor angle (U1-SN), mandibular incisor angle (L1-MP), occlusal plane angle (OP-FH), inter incisal angle (U1-L1), maxillary incisor to palatal plane (U1-PP), maxillary molar to palatal plane (U6-PP). A simplified Johnston’s Pitchfork diagram was applied to analyze dental and skeletal movements (Fig. 1).
Fig. 1.
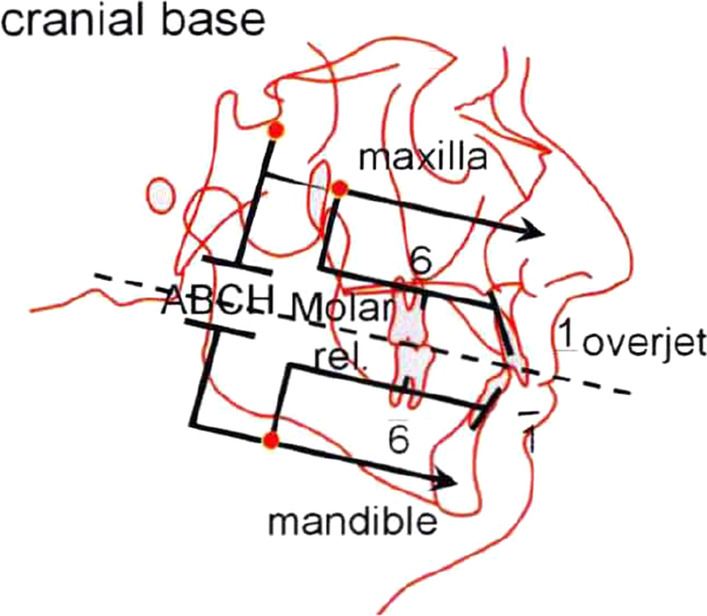
Johnston’s Pitchfork Analysis. Max: maxilla; ABCH: relative AP movement between mandible and maxilla; Mand: mandible; U1: upper incisors; L1: lower incisors; U6: upper molars; L6: lower molars. Max described the AP movement of cranial base landmark, which represented the change of maxilla. Apical base change (ABCH) described the relative AP movement between mandible and maxilla, and Mand described the AP movement of mandible which was the algebraic sum of Max and ABCH. Similarly, U1, L1, U6 and L6 described the AP movements of incisors and molars. All the changes in position benefit to correct class II malocclusion were counted as plus signs while those worsen the malocclusion were counted as minus signs(11)
Statistical analysis
All the measurements were transferred to SPSS Statistics 26.0 software for analysis. Group comparisons were made by analysis of variance (ANOVA) when the variables fitted the normal distribution, and Post Hoc test were conducted by Least Significant Difference (LSD) t-test for those meet homogeneity of variance and by analysis of Games-Howell for those of heterogeneity of variance. For some variables that were not normally distributed, Kruskal–Wallis test was used. A probability level of 0.05 was used to determine statistical significance.
Results
In comparison at T1, NA-PA (P = 0.004), Go-Pog (P = 0.000), Co-Pog (P = 0.003), ANB (P = 0.006), Vertical Ratio (P = 0.000) and U6-PP (P = 0.007) showed between-group differences (Table 2).NA-PA, Go-Pog, Co-Pog and ANB were comparable for MA group and Vanbeek, Herbst and Twin-Block groups. Vertical Ratio and U6-PP of MA group differed significantly from the other groups.
Table 2.
Descriptive statistics and group comparison at T1
| Variable | Vanbeek | Herbst | Twin-Block | MA | Control | P |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| SNA | 82.93 ± 2.00 | 81.02 ± 2.13 | 81.71 ± 2.40 | 81.44 ± 3.31 | 81.06 ± 3.07 | 0.346 |
| SNB | 75.94 ± 1.80 | 73.66 ± 3.37 | 74.08 ± 2.34 | 75.72 ± 3.24 | 74.83 ± 2.68 | 0.172 |
| FH-NP | 83.63 ± 3.30 | 83.63 ± 4.49 | 83.25 ± 2.79 | 84.36 ± 3.01 | 84.53 ± 2.62 | 0.849 |
| NA-PA† | 15.65/3.70 | 19.10/11.10 | 16.25/4.70 | 11.55/3.60 | 13.60/4.90 | 0.004* |
| MP-FH | 30.31 ± 4.15 | 27.62 ± 7.09 | 29.71 ± 5.85 | 26.70 ± 5.16 | 29.67 ± 4.38 | 0.356 |
| MP-SN† | 35.65/6.40 | 35.50/10.0 | 33.80/9.60 | 35.05/4.60 | 36.40/4.60 | 0.847 |
| Co-Go | 52.87 ± 5.43 | 55.34 ± 6.10 | 54.18 ± 4.84 | 52.83 ± 3.67 | 53.52 ± 4.16 | 0.696 |
| Go-Pog | 59.59 ± 4.87 | 57.36 ± 4.71 | 57.14 ± 3.97 | 69.20 ± 3.33 | 56.50 ± 3.22 | 0.000* |
| Co-Pog | 95.83 ± 6.48 | 95.27 ± 5.91 | 94.58 ± 5.27 | 102.14 ± 4.06 | 93.96 ± 4.83 | 0.003* |
| Y Axis Angle | 72.54 ± 2.33 | 73.30 ± 3.86 | 72.68 ± 2.29 | 71.71 ± 3.06 | 73.57 ± 2.57 | 0.509 |
| ANB† | 7.20/1.60 | 7.70/3.70 | 7.80/1.40 | 5.80/1.40 | 6.05/1.60 | 0.006* |
| Lower Facial Height Ratio† | 53.60/2.3 | 52.40/2.90 | 53.05/3.30 | 53.25/3.80 | 53.75/3.9 | 0.302 |
| Vertical Ratio† | 1.15/0.10 | 1.10/0.10 | 1.10/0.10 | 1.50/0.20 | 1.10/0.40 | 0.000* |
| P-A Face Height† | 63.95/4.80 | 64.40/10.70 | 65.70/8.00 | 63.25/2.30 | 63.35/3.00 | 0.916 |
| U1-SN | 110.39 ± 6.37 | 109.81 ± 7.79 | 110.33 ± 7.43 | 107.61 ± 6.74 | 107.37 ± 6.53 | 0.671 |
| U1-PP† | 28.35/2.30 | 27.70/5.00 | 26.30/4.20 | 27.65/3.30 | 27.45/4.30 | 0.634 |
| U6-PP | 18.80 ± 3.31 | 20.11 ± 2.21 | 19.01 ± 2.16 | 16.58 ± 2.12 | 19.28 ± 1.83 | 0.007* |
| L1-MP | 99.37 ± 2.98 | 99.34 ± 5.80 | 97.89 ± 8.58 | 97.23 ± 6.28 | 97.95 ± 6.66 | 0.874 |
| U1-L1 | 113.10 ± 8.08 | 115.17 ± 8.22 | 114.84 ± 9.83 | 120.36 ± 7.37 | 116.48 ± 7.09 | 0.201 |
| OP-FH | 12.94 ± 3.64 | 11.53 ± 6.24 | 14.89 ± 3.58 | 13.99 ± 3.57 | 12.58 ± 4.23 | 0.374 |
†Non parametric test; *P < 0.05
The treatment changes showed significant differences in 11 variables (SNB, FH-NP, NA-PA, Co-Go, Co-Pog, ANB, lower facial height ratio, U1-PP, U6-PP, L1-MP and U1-L1) (Table 3, Fig. 2). In the four treatment groups, SNB, FH-NP and lower facial height ratio increased and NA-PA and ANB decreased, were all significantly different to the controls. In terms of the variables representing elongation of mandible, Co-Go of Twin-Block and MA groups increased significantly more than Vanbeek and control groups, meanwhile Co-Pog of Herbst, Twin-Block and MA groups increased significantly different to the controls and that of Twin-Block and MA groups was comparable for Vanbeek group. In the case of tooth movement, MA group showed significantly different changes for U1-PP than the other groups except Twin-Block; U6-PP of Herbst group decreased significantly while the others all increased and MA group was also comparable for Vanbeek and Twin-Block groups; L1-MP of Herbst group increased greatly and was significantly different to Vanbeek, MA and control groups while that of Vanbeek Activator group decreased slightly (mean = − 0.26°); and U1-L1 for Vanbeek and MA groups increased and significantly differed from Herbst group of which U1-L1 decreased about 3.4 degree.
Table 3.
Descriptive statistics and group comparison from T1 to T2
| Variable | Vanbeek | Herbst | Twin-Block | MA | Control | P |
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| SNA | − 0.11 ± 0.81 | − 0.01 ± 0.65 | 0.12 ± 1.11 | 0.18 ± 0.72 | 0.35 ± 0.84 | 0.692 |
| SNB† | 0.90/0.63a | 1.50/1.10a | 1.10/0.80a | 0.90/1.78a | 0.30/1.45b | 0.004* |
| FH-NP† | 1.00/0.95a | 2.00/2.40 a | 0.95/1.90 a | 1.00/1.80 a | − 0.05/0.93b | 0.003* |
| NA-PA | − 2.31 ± 1.87b | − 3.55 ± 2.38b | − 3.91 ± 3.03b | − 2.59 ± 2.85b | 0.43 ± 1.13a | 0.000* |
| MP-FH | − 0.15 ± 2.37 | − 0.15 ± 1.76 | 0.15 ± 1.38 | 0.41 ± 1.42 | − 0.34 ± 1.25 | 0.814 |
| MP-SN | 0.69 ± 2.97 | − 0.17 ± 1.57 | 0.20 ± 1.60 | 0.15 ± 1.58 | − 0.3 ± 1.15 | 0.725 |
| Co-Go | 2.21 ± 1.52b | 2.95 ± 2.42ab | 4.22 ± 2.39a | 4.49 ± 2.46a | 1.66 ± 2.09b | 0.006* |
| Go-Pog | 1.30 ± 0.98 | 1.82 ± 1.68 | 1.81 ± 1.58 | 2.25 ± 1.67 | 1.39 ± 1.38 | 0.425 |
| Co-Pog | 2.84 ± 1.23bc | 3.84 ± 2.31ab | 4.87 ± 2.26a | 4.93 ± 1.59a | 2.06 ± 1.35c | 0.015* |
| Y Axis Angle† | − 0.20/1.13 | − 0.60/1.00 | 0.10/0.98 | 0.25/0.87 | 0.05/0.75 | 0.327 |
| ANB† | − 1.00/1.35b | − 1.80/1.30b | − 1.10/1.20b | − 0.85/1.78b | 0.15/0.88a | 0.000* |
| Lower Facial Height Ratio | 0.63 ± 0.41 a | 0.86 ± 0.52a | 1.08 ± 0.72a | 0.84 ± 0.81a | − 0.16 ± 0.62b | 0.000* |
| Vertical Ratio† | 0.00/0.05 | 0.00/0.10 | 0.00/0.07 | 0.00/0.03 | 0.00/0.10 | 0.303 |
| P-A Face Height | 0.50 ± 1.50 | 0.98 ± 1.42 | 0.83 ± 1.19 | 0.56 ± 1.54 | 0.85 ± 1.12 | 0.891 |
| U1-SN | − 2.80 ± 4.74 | − 3.17 ± 3.90 | − 3.43 ± 4.35 | − 4.10 ± 6.00 | 0.13 ± 2.86 | 0.191 |
| U1-PP† | 0.00/0.80b | 0.10/0.70b | 0.45/1.22ab | 0.70/1.85a | 0.20/1.38b | 0.028* |
| U6-PP† | 0.45/1.80b | − 0.70/1.00c | 0.55/1.00b | 1.60/1.58a | 0.65/1.37ab | 0.000* |
| L1-MP† | 0.15/3.52b | 7.80/11.40a | 3.20/5.80ab | 0.95/4.05b | 0.30/1.28b | 0.027* |
| U1-L1† | 3.15/7.82a | − 3.40/7.60b | 0.85/3.52ab | 3.20/11.93a | 0.40/6.37ab | 0.034* |
| OP-FH | − 0.77 ± 1.61 | 0.74 ± 2.22 | − 0.11 ± 1.86 | 0.12 ± 2.05 | − 0.47 ± 1.43 | 0.328 |
†Non parametric test. Groups with the same letter indicated no statistically significant difference. *P < 0.05
Fig. 2.

Multiple comparisons between groups from T1 to T2
Class II correction
Descriptive statistics for the Johnston analysis variables are shown in Table 4, all variables except movement of maxillary osseous base were statistically different. Linear changes measured along the mean functional occlusal plane during treatment are depicted diagrammatically in the pitchforks (Fig. 3, 4, 5, 6, 7, 8, 9, 10, 11). In comparison of the four treatment groups, Herbst showed the most ABCH and Vanbeek Activator showed the least (Herbst > Twin-Block > MA > Vanbeek Activator) with no significance. Except for the MA group, the upper molars in the other groups moved positively distally and there were significant differences between MA group and Herbst & Vanbeek groups. Upper molar movement in Twin-Block group and lower one in MA and Vanbeek groups were significantly less than that in Herbst group. Lower incisor movement in MA and Vanbeek groups, which was negative, were significantly less than that in both Herbst and Twin-Block groups which were positive. Of all the groups, the MA group had the largest upper incisor movement, but it was not statistically significant.
Table 4.
Skeletal and dental changes in molar relationship and overjet
| Variable(mm) | Vanbeek | Herbst | Twin-Block | Ma | Control | P |
|---|---|---|---|---|---|---|
| Median/IQR | Median/IQR | Median/IQR | Median/IQR | Median/IQR | ||
| ABCH† | 2.05/0.90a | 3.60/1.40a | 2.65/2.20a | 2.59/3.20a | 0.20/1.40b | 0.000* |
| Maxillary Osseous base† | − 0.50/1.30 | − 0.80/2.00 | − 0.40/1.00 | − 0.98/3.00 | − 1.75/1.30 | 0.059 |
| Upper Molar† | 0.75/1.20ab | 1.30/1.00a | 0.00/1.60bc | − 1.58/2.80c | − 0.50/1.00c | 0.000* |
| Lower Molar† | 0.60/0.90b | 2.80/2.40a | 1.30/1.20ab | 0.37/2.90b | 0.40/1.50b | 0.008* |
| Upper Incisor† | 1.25/2.20a | 0.90/0.80ab | 0.90/1.70ab | 2.35/2.50a | 0.00/1.30b | 0.011* |
| Lower Incisor† | 0.00/0.90b | 1.20/1.60a | 1.25/1.20a | 0.10/3.50b | − 0.20/1.80b | 0.002* |
†Non parametric test. Groups with the same letter indicated no statistically significant difference. *P < 0.05
Fig. 3.

Overjet(left) and Molar Relationship (right) Analysis of C group
Fig. 4.

Overjet Analysis (left) and Corrected Analysis (right) of V group
Fig. 5.

Overjet Analysis (left) and Corrected Analysis (right) of H Group
Fig. 6.

Overjet Analysis (left) and Corrected Analysis (right) of TB Group
Fig. 7.

Overjet Analysis (left) and Corrected Analysis (right) of MA Group
Fig. 8.

Molar Relationship Analysis (left) and Corrected Analysis (right) of V Group
Fig. 9.

Molar Relationship Analysis (left) and Corrected Analysis (right) of H Group
Fig. 10.

Molar Relationship Analysis (left) and Corrected Analysis (right) of TB Group
Fig. 11.

Molar Relationship Analysis (left) and Corrected Analysis (right) of MA Group
Skeletal and dentoalveolar effect in four appliances
The skeletal effect of Vanbeek was more important in improving the deep overjet of anterior teeth, while in MA group dental changes accounted more (Table 5). In terms of correction of class II molar occlusion, Twin-Block and MA groups accounted for more bone effects among the four appliances.
Table 5.
Skeletal and Dentoalveolar Effect in V, H, TB, MA
| Groups | Overjet correction(%) | Molar relationship correction(%) | ||||||
|---|---|---|---|---|---|---|---|---|
| Skeletal effects (%) |
Skeletal effects (corrected) |
Dentoalveolar effects (%) |
Dentoalveolar effects (corrected) |
Skeletal effects (%) |
Skeletal effects (corrected) |
Dentoalveolar effects (%) |
Dentoalveolar effects (corrected) |
|
| Vanbeek | 69.93 | 74.73 | 30.07 | 25.27 | 57.22 | 60.00 | 42.78 | 40.00 |
| Herbst | 53.69 | 55.15 | 46.31 | 44.85 | 43.78 | 44.53 | 56.22 | 55.47 |
| Twin-Block | 55.98 | 57.93 | 44.02 | 42.07 | 74.54 | 78.74 | 25.46 | 21.26 |
| MA | 47.09 | 48.91 | 52.91 | 51.09 | 153.72 | 194.57 | − 53.72 | − 94.57 |
Discussion
As shown in the result, all the four appliances are effective in correcting class II malocclusion. Compared with the untreated group, Vanbeek Activator, Herbst, Twin-Block and MA created a significant orthopedic effect that mandible forward repositioning and facial profile improvement, which is consistent with previous studies [4, 12–14]. However, untreated children have no potential to correct class II malocclusion by themselves, so orthopedic treatment quietly benefits a lot[3, 4]. And there actually were differences in basal bone movements based on the Johnston’s Pitchfork Analysis [3, 15].
As for mandibular growth, supplementary mandibular elongation was found in Twin-Block and MA (Co-Go and Co-Pog) and Herbst (Co-Pog). This was in agreement with previous animal researches of animal models, that mandible growth was enhanced by functional appliances, especially in vertical direction [16, 17]. DAnto’s systematical review found that most studies reported significant mandibular length increasing when treated at the adolescent growth spurt [12], and Sabouni et.al also confirmed that the same result could be obtained after MA treatment [10]. Phan believed that fixed nature of Herbst made its action time longer than others, which brought about more mandibular length growth [18]. However, Johnston’s research didn’t support the point mentioned above [19].
Although with a lack of significant reduction of SNA in the four treatment groups, maxilla growth inhibition was observed in Vanbeek Activator via maxilla base bone movement in Pitchfork Analysis, which also suggested that the torque of upper incisor might interfere the position of A point and our distinguishment between dental and skeletal effects [3, 20]. This was consisted with previous studies that headgear had some effects in maxillary restrain [4, 21, 22]. However clinically significant restraint of maxillary growth was not clear in other functional appliances [23, 24]. Some studies have reported maxillary inhibition with Twin-Block and Herbst, but others supposed that was negligible, which might come from changes in A point.
Compared with controls, the four treatment groups all significantly increased the lower facial height and worsen the long face profile. That might come from the mandibular clockwise rotation during occlusion reconstruction [25]. Activator was reported a significant increase in the lower facial height, which was primarily because of the bite opening effect and guided extrusion of upper molars [26]. Vanbeek Activator presented the least increase in lower facial height among the four appliances since the high-pull headgear inhibited the downward growth of maxilla and resulted in the slightest mandible clockwise rotation, which was consistent with Spalj’s observation[4]. Brien’s research found that the high-pull headgear could make the mandible rotate forward [15], and the finite element analysis results of Gautam et al. also suggested that it could effectively carry out vertical control[27]. In addition, changes in vertical dimension were also related to molars’ vertical movements. Herbst and clear aligners were reported to give rise to molar intrusion [28, 29], which offset some mandibular clockwise rotation caused by bite opening effect. Even some studies observed a mandibular counterclockwise rotation in Herbst [30]. However, in current research, Herbst and MA didn’t induce any significant change in the inclination of the mandibular plane to the Frankfort horizontal plane or to SN plane, as also confirmed in Caruso’s research [7].
From our results, Activator, Herbst and Twin-Block had different levels of upper incisor retroclination and lower incisor proclination [4, 31–33], but decrease in upper incisor/Sella-Nasion plane angle (U1-SN) didn’t present significant difference. L1-MP in Herbst increased significantly more than that in Vanbeek Activator and MA. Herbst exerts the force directly on teeth without any effective control for lower incisors, except a lingual bar, thus produces the most evident labial movement as a result[31]. The headgear activator could effectively control the inclination of lower anterior teeth[25, 34]. In this study, Vanbeek appliance showed a slight proclination which was attributed to the counterclockwise rotation of lower incisors under the headgear’s extraoral forces in backward direction [34, 35]. That is consistent with some previous studies that inclination of lower incisors in Activator patients almost remain the same or changes a little [36]. Different from other three appliances, MA provided us with digital means to design the movement of teeth and the then produced corresponding aligners via 3D printing technology. Attributed to its surrounding of each teeth crown surface we could control orthodontic tooth movement while moving the mandible forward [7, 8]. Sabouni et.al reported the lower incisor angulation was maintained during class II correction [10]. In this sample, MA presents little compensatory proclination of lower incisors, which could provide more space for appliances to play the skeletal role of guiding the mandible forward.
As mentioned before, point A and B, which are broadly used as skeletal marks of maxilla and mandible, are likely affected by torque of upper and lower incisors [3]. In this way the real skeletal effects of functional appliances are easily biased by dental movements. Compared with conventional cephalometrics, Johnston’s Pitchfork Analysis is a better method to analyze skeletal and dentoalveolar changes separately and calculate their proportions [37].
Although all the four appliances greatly corrected molar relationship and decreased overjet, their effects were distinctly different. At the level of overjet reduction, Vanbeek activator accounted the highest proportion of skeletal effect (74.73%), which was consistent with previous researches [25, 38]. This could be owing to its structure characteristics that it entirely wrapped the whole upper and lower arch and high-pull headgear inhibited maxillary forward and vertical growth. For the MA group, Ravera et al. reported that if the patients were treated at CVM2 growth phase, the aligners showed mainly dentoalveolar effects while at CVM3 the skeletal components accounted for more [8], which was consistent with our results. Although dental effect shared higher proportion (51.09%), bone effect was still close to a half (48.91%). Blackham also supported that skeletally MA didn’t present outcomes significantly different from the Twin-Block [14]. Conversely, MA was more comfortable, less noticeable and easier to insert than TB, which could improve the degree of compliance [39]. Additionally clear aligners could realize the design of terminal occlusion in advance and have good control of teeth movement, which overcomes the common recognized limit of Class II conventional functional appliances and allow an optimization of clinical efficacy [7, 40]. Dental changes accounted for 44.85% and 42.07% in Herbst and Twin-Block in this sample. While the existing literature data, ranging from 40 to 65% [41–44], also have some differences on the weight of dentoalveolar effects caused by Herbst or Twin-Block, which may be due to the difference in the age of their cases.
At the end of treatment, the molar relationship can be improved from the distal occlusal relationship to the neutral or even slightly mesial relationship [41, 45], and some of these improvements are contributed to the dental movement of the molars. In terms of molar relationship correction of this sample, the proportions of dentoalveolar effects are 40.00%, 55.47%, 21.26% and − 94.57% in Vanbeek Activator, Herbst, Twin-Block and MA. Lagerstrom et al. found that distal movement of the maxillary molars was almost entirely dental and mandibular advancement devoted most of lower molar mesial movement in Headgear-Activator treatment [46]. Jena et al. found that after Twin-Block treatment, the relationship of the molars that were originally distal was significantly corrected and had significant distal movement of the maxillary molars and proximal movement of the mandibular molars [47]. Several studies found that Herbst has a significant dental effect of pushing the maxillary molars backward [41, 48], and Tomblyn’s research on fixed Herbst showed that 60% of the molar relationship change was the molar movement factor [41, 44]. The above conclusions were basically consistent with the results of this study. MA adjusted the movement of the molars to establish a neutral occlusal relationship after several “bite jump” mandibular advancements. The maxillary molars moved mesially to adapt to the position of the mandibular molars after the mandibular lead, and MA enabled to distalize the lower molars, to establish a neutral molar relationship. Any distalization would result in a net negative movement with respect to initial maxillary molar position relative to the occlusal plane [14], as is shown in our sample (− 94.57% for dentoalveolar effect). Typically, children with class II malocclusion are associated with narrow arches, thus sometimes the upper arch expansion guided by the aligners, in order to create more room for alignment, leveling and the forwarded position of the mandible, can meanwhile promote posterior teeth buccal tipping as resulted[49].
The present results are limited by the small number of patients, the retrospective design and lack of MRI or CBCT to assess TMJ conditions. For this reason, further studies with a longitudinal randomized design on a larger sample and the changes of temporomandibular joint region are encouraged.
Strengths and limitations
The strength of this study is to compare the therapeutic effect of the clear aligners with the traditional one via both cephalometric analysis and Johnston Pitchfork analysis. On the other hand, due to the retrospective nature of this study, only limited data analysis could be performed with existing patient recordings. In addition, the number of patients enrolled in this study was small due to the single-center trial, with only more than 10 cases in each group, and no comparative analysis was conducted with other orthotics.
Conclusions
Four appliances are all effective in mandibular advancement, facial profile improvement, skeletal class II correction and modification of class II molar relationship and deep overjet, with unavoidable increase in lower facial ratio, however.
Vanbeek shows the highest proportion of skeletal changes, more significant maxillary growth inhibition and better control of lower incisor.
Herbst corrects the overjet of Class II patients more by skeletal changes accompanied with lower incisors proclination and has greater maxillary molar distalization.
Twin-Block shows lower incisors proclination and presents both skeletal and dentoalveolar effects.
MA corrects the overjet of Class II patients more by dentoalveolar effect. MA allows aligning and leveling to establish a good occlusal relationship while leading the mandible forward, which may save time for phase II orthodontics, and has good control of incisor inclination and enables to distalize molars.
Acknowledgements
We would like to thank Dr Xia and Wang for their support in gathering patients information and all the doctors in our department for advice during this study.
Author contributions
YW: conceptualization; data curation; formal analysis; investigation; project administration; visualization; writing-original draft; writing-review & editing. QY: conceptualization; data curation; investigation; visualization; writing-review & editing. YX: data curation; investigation. BW: data curation; investigation. SC: data curation; analysis; KG: validation, investigation; BZ: data curation. MZ: conceptualization; investigation; methodology; project administration; resources; supervision; validation; writing-original draft; writing-review and editing. All authors read and approved the final manuscript.
Funding
This work was supported by China Oral Health Foundation (A2021-145), Shanghai Pudong New Area Health and Family Planning Commission joint project (PW2018D-10), Clinical Research Program of 9th People’s Hospital, Shanghai Jiao Tong University School of Medicine (JYLJ202017).
Availability of data and materials
The data underlying this article will be shared on reasonable request to the corresponding author.
Declarations
Ethical approval and consent to participate
This study has been reviewed and approved by the Medical Ethics Committee of Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (SH9H-2020-T347-2). Informed consent was obtained from the legal guardians of the subjects for study. Our study has conformed to the STROBE guidelines. We confirm that all methods were carried out in accordance with relevant guidelines and regulations. Our study performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yanqi Wu and Qian Yu contributed equally to this study
References
- 1.Wadhawan N, Kumar S, Kharbanda O, Duggal R, Sharma R. Temporomandibular joint adaptations following two-phase therapy: an MRI study. Orthod Craniofac Res. 2008;11(4):235–250. doi: 10.1111/j.1601-6343.2008.00436.x. [DOI] [PubMed] [Google Scholar]
- 2.Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara J. Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthodont Dentofacial Orthop. 2006;129(5):599.e1–12; discussion e1–6. [DOI] [PubMed]
- 3.Martins R, da Rosa MJ, Martins L, Buschang P. Skeletal and dental components of Class II correction with the bionator and removable headgear splint appliances. Am J Orthodont Dentofacial Orthop. 2008;134(6):732–741. doi: 10.1016/j.ajodo.2007.07.022. [DOI] [PubMed] [Google Scholar]
- 4.Spalj S, Mroz Tranesen K, Birkeland K, Katic V, Pavlic A, Vandevska-Radunovic V. Comparison of activator-headgear and twin block treatment approaches in Class II Division 1 Malocclusion. Biomed Res Int. 2017;2017:4861924. doi: 10.1155/2017/4861924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Čirgić E, Kjellberg H, Hansen K. Treatment of large overjet in Angle Class II: division 1 malocclusion with Andresen activators versus prefabricated functional appliances-a multicenter, randomized, controlled trial. 2015;38(5):516. [DOI] [PubMed]
- 6.Uçüncü N, Türk T, Carels C. Comparison of modified Teuscher and van Beek functional appliance therapies in high-angle cases. J Orofacial Orthop. 2001;62(3):224–237. doi: 10.1007/pl00001930. [DOI] [PubMed] [Google Scholar]
- 7.Caruso S, Nota A, Caruso S, Severino M, Gatto R, Meuli S, et al. Mandibular advancement with clear aligners in the treatment of skeletal Class II. A retrospective controlled study. Eur J Paediatric Dent. 2021;22(1):26–30. doi: 10.23804/ejpd.2021.22.01.05. [DOI] [PubMed] [Google Scholar]
- 8.Ravera S, Castroflorio T, Galati F, Cugliari G, Garino F, Deregibus A, et al. Short term dentoskeletal effects of mandibular advancement clear aligners in Class II growing patients. A prospective controlled study according to STROBE Guidelines. Eur J Paediatric Dent. 2021;22(2):119–124. doi: 10.23804/ejpd.2021.22.02.6. [DOI] [PubMed] [Google Scholar]
- 9.Koukou M, Damanakis G, Tsolakis A. Orthodontic management of skeletal Class II malocclusion with the invisalign mandibular advancement feature appliance: a case report and review of the literature. Case Rep Dent. 2022;2022:7095467. doi: 10.1155/2022/7095467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sabouni W, Hansa I, Al Ali S, Adel S, Vaid N. Invisalign treatment with mandibular advancement: a retrospective cohort cephalometric appraisal. J Clin Imaging Sci. 2022;12:42. doi: 10.25259/JCIS_64_2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Johnston L. Balancing the books on orthodontic treatment: an integrated analysis of change. Br J Orthod. 1996;23(2):93–102. doi: 10.1179/bjo.23.2.93. [DOI] [PubMed] [Google Scholar]
- 12.D'Anto V, Bucci R, Franchi L, Rongo R, Michelotti A, Martina R. Class II functional orthopaedic treatment: a systematic review of systematic reviews. J Oral Rehabil. 2015;42(8):624–642. doi: 10.1111/joor.12295. [DOI] [PubMed] [Google Scholar]
- 13.Pacha M, Fleming P, Johal A. A comparison of the efficacy of fixed versus removable functional appliances in children with Class II malocclusion: a systematic review. Eur J Orthod. 2016;38(6):621–630. doi: 10.1093/ejo/cjv086. [DOI] [PubMed] [Google Scholar]
- 14.Blackham SS. A study of short-term skeletal, dental, and soft tissue effects of Class II malocclusions treated with InvisalignⓇ with Mandibular Advancement Feature or Twin Block appliance compared with historical controls, University of British Columbia, 2020.
- 15.O'Brien K, Wright J, Conboy F, Sanjie Y, Mandall N, Chadwick S, et al. Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am J Orthodont Dentofacial Orthop. 2003;124(3):234–43; quiz 339. [DOI] [PubMed]
- 16.Wang J, Yuan L, Liu J, Mao L, Xia L, Fang B. Hemifacial microsomia treated with a hybrid technique combining distraction osteogenesis and a mandible-guided functional appliance: Pilot study. Am J Orthodont Dentofacial Orthop. 2019;155(6):801–811. doi: 10.1016/j.ajodo.2018.06.020. [DOI] [PubMed] [Google Scholar]
- 17.Kim I, Duncan WJ, Farella M. Evaluation of mandibular growth using cone-beam computed tomography in a rabbit model: A pilot study. NZ Dent J. 2012;108(1):9–12. [PubMed] [Google Scholar]
- 18.Phan KL, Bendeus M, Hagg U, Hansen K, Rabie AB. Comparison of the headgear activator and Herbst appliance-effects and post-treatment changes. Eur J Orthod. 2006;28(6):594–604. doi: 10.1093/ejo/cjl052. [DOI] [PubMed] [Google Scholar]
- 19.Johnston LE. If wishes were horses: functional appliances and growth modification. Prog Orthod. 2005;6(1):36–47. [PubMed] [Google Scholar]
- 20.Schiavon Gandini M, Gandini L, Da Rosa Martins J, Del Santo M. Effects of cervical headgear and edgewise appliances on growing patients. Am J Orthodont Dentofacial Orthop 2001;119(5):531–8; discussion 8–9. [DOI] [PubMed]
- 21.Lerstol M, Torget O, Vandevska-Radunovic V. Long-term stability of dentoalveolar and skeletal changes after activator-headgear treatment. Eur J Orthod. 2010;32(1):28–35. doi: 10.1093/ejo/cjp042. [DOI] [PubMed] [Google Scholar]
- 22.Antonarakis G, Kiliaridis S. Short-term anteroposterior treatment effects of functional appliances and extraoral traction on class II malocclusion. A meta-analysis. Angle Orthodontist. 2007;77(5):907–914. doi: 10.2319/061706-244. [DOI] [PubMed] [Google Scholar]
- 23.Ehsani S, Nebbe B, Normando D, Lagravere M, Flores-Mir C. Short-term treatment effects produced by the Twin-block appliance: a systematic review and meta-analysis. Eur J Orthod. 2015;37(2):170–176. doi: 10.1093/ejo/cju030. [DOI] [PubMed] [Google Scholar]
- 24.Atresh A, Cevidanes L, Yatabe M, Muniz L, Nguyen T, Larson B, et al. Three-dimensional treatment outcomes in Class II patients with different vertical facial patterns treated with the Herbst appliance. Am J Orthodont Dentofacial Orthop. 2018;154(2):238–48.e1. doi: 10.1016/j.ajodo.2017.11.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Türkkahraman H, Sayin M. Effects of activator and activator headgear treatment: comparison with untreated Class II subjects. Eur J Orthod. 2006;28(1):27–34. doi: 10.1093/ejo/cji062. [DOI] [PubMed] [Google Scholar]
- 26.Idris G, Hajeer MY, Al-Jundi A. Soft- and hard-tissue changes following treatment of Class II division 1 malocclusion with Activator versus Trainer: a randomized controlled trial. Eur J Orthod. 2019;41(1):21–28. doi: 10.1093/ejo/cjy014. [DOI] [PubMed] [Google Scholar]
- 27.Gautam P, Valiathan A, Adhikari R. Craniofacial displacement in response to varying headgear forces evaluated biomechanically with finite element analysis. Am J Orthodont Dentofacial Orthop. 2009;135(4):507–515. doi: 10.1016/j.ajodo.2007.02.059. [DOI] [PubMed] [Google Scholar]
- 28.Harris K, Ojima K, Dan C, Upadhyay M, Alshehri A, Kuo C, et al. Evaluation of open bite closure using clear aligners: a retrospective study. Prog Orthod. 2020;21(1):23. doi: 10.1186/s40510-020-00325-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Talens-Cogollos L, Vela-Hernández A, Peiró-Guijarro M, García-Sanz V, Montiel-Company J, Gandía-Franco J, et al. Unplanned molar intrusion after Invisalign treatment. Am J Orthodont Dentofacial Orthop. 2022;162(4):451–458. doi: 10.1016/j.ajodo.2021.03.019. [DOI] [PubMed] [Google Scholar]
- 30.Change in mandibular growth direction by means of a Herbst appliance? A case report. Am J Orthod Dentofacial Orthop. 1992;102(5):456–63. [DOI] [PubMed]
- 31.Barnett G, Dw, Major P, Flores-Mir C. immediate skeletal and dentoalveolar effects of the crown- or banded type herbst appliance on Class II division 1 Malocclusion. Angle Orthodontist. 2008;78(2):361. [DOI] [PubMed]
- 32.Gülnaz MA. Effects of activator and high-pull headgear combination therapy: skeletal, dentoalveolar, and soft tissue profile changes. Eur J Orthod. 2007;29(2):140–148. doi: 10.1093/ejo/cjm003. [DOI] [PubMed] [Google Scholar]
- 33.Jacobson A. Proportional changes in cephalometric distances during Twin Block appliance therapy. Eur J Orthod. 2002;24(3):360–361. doi: 10.1093/ejo/24.5.485. [DOI] [PubMed] [Google Scholar]
- 34.Margareta B, Urban HG, Bakr R. Growth and treatment changes in patients treated with a headgear-activator appliance. Am J Orthod Dentofac Orthop. 2002;121(4):376–384. doi: 10.1067/mod.2002.122177. [DOI] [PubMed] [Google Scholar]
- 35.Hakan TM, Ozgür S. Effects of activator and activator headgear treatment: comparison with untreated Class II subjects. Eur J Orthodont. 2006;28(1):27. doi: 10.1093/ejo/cji062. [DOI] [PubMed] [Google Scholar]
- 36.Hourfar J, Kinzinger GSM, Euchner L, Lisson JA. Differential skeletal and dental effects after orthodontic treatment with bite jumping appliance or activator: a retrospective cephalometric study. Clin Oral Investig. 2019. [DOI] [PubMed]
- 37.Pancherz H. A cephalometric analysis of skeletal and dental changes contributing to Class II correction in activator treatment. Am J Orthod. 1984;85(2):125–134. doi: 10.1016/0002-9416(84)90004-6. [DOI] [PubMed] [Google Scholar]
- 38.Bendeus M, Hägg U, Rabie B. Growth and treatment changes in patients treated with a headgear-activator appliance. Am J Orthodont Dentofacial Orthop. 2002;121(4):376–384. doi: 10.1067/mod.2002.122177. [DOI] [PubMed] [Google Scholar]
- 39.Zybutz T, Drummond R, Lekic M, Brownlee M. Investigation and comparison of patient experiences with removable functional appliances. Angle Orthod. 2021;91(4):490–495. doi: 10.2319/050520-393.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Monaco A, Petrucci A, Marzo G, Necozione S, Gatto R, Sgolastra F. Effects of correction of Class II malocclusion on the kinesiographic pattern of young adolescents: a case- control study. Eur J Paediatr Dent. 2013;14(2):131–134. [PubMed] [Google Scholar]
- 41.Tomblyn T, Rogers M, Andrews L, Martin C, Tremont T, Gunel E, et al. Cephalometric study of Class II Division 1 patients treated with an extended-duration, reinforced, banded Herbst appliance followed by fixed appliances. Am J Orthodont Dentofacial Orthop. 2016;150(5):818–830. doi: 10.1016/j.ajodo.2016.04.020. [DOI] [PubMed] [Google Scholar]
- 42.Kevin OB, Jean W, Frances C, Stephen C, Ivan C, Paul C, et al. Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicenter, randomized, controlled trial Part 2: Psychosocial effects. Am J Orthod Dentofacial Orthop. 2003;124(5):488–494. doi: 10.1016/S0889540603006425. [DOI] [PubMed] [Google Scholar]
- 43.Sidlauskas A. The effects of the Twin-block appliance treatment on the skeletal and dentolaveolar changes in Class II Division 1 malocclusion. Medicina (Kaunas) 2005;41(5):392–400. [PubMed] [Google Scholar]
- 44.Booij J, Goeke J, Bronkhorst E, Katsaros C, Ruf S. Class II treatment by extraction of maxillary first molars or Herbst appliance: dentoskeletal and soft tissue effects in comparison. J Orofacial Orthop. 2013;74(1):52–63. doi: 10.1007/s00056-012-0112-1. [DOI] [PubMed] [Google Scholar]
- 45.Zymperdikas V, Koretsi V, Papageorgiou S, Papadopoulos M. Treatment effects of fixed functional appliances in patients with Class II malocclusion: a systematic review and meta-analysis. Eur J Orthod. 2016;38(2):113–126. doi: 10.1093/ejo/cjv034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lagerström LO, Nielsen IL, Lee R, Isaacson RJ. Dental and skeletal contributions to occlusal correction in patients treated with the high-pull headgear–activator combination. Am J Orthod Dentofacial Orthop. 1990;97(6):495–504. doi: 10.1016/S0889-5406(05)80030-7. [DOI] [PubMed] [Google Scholar]
- 47.Jena A, Duggal R, Parkash H. Skeletal and dentoalveolar effects of Twin-block and bionator appliances in the treatment of Class II malocclusion: a comparative study. Am J Orthodont Dentofacial Orthop. 2006;130(5):594–602. doi: 10.1016/j.ajodo.2005.02.025. [DOI] [PubMed] [Google Scholar]
- 48.Pancherz H, Anehus-Pancherz M. The headgear effect of the Herbst appliance: a cephalometric long-term study. Am J Orthod Dentofacial Orthop. 1993;103(6):510–520. doi: 10.1016/0889-5406(93)70090-B. [DOI] [PubMed] [Google Scholar]
- 49.Zhou N, Guo J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthod. 2020;90(1):23–30. doi: 10.2319/022719-151.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.