

Abstract
Purpose/Hypothesis
The flexor-pronator mass of the forearm contributes dynamic stability to the medial elbow. Training this muscle group is essential for overhead athletes, however, there is lack of evidence supporting use of training exercises. The purpose of this study was to measure the extent of EMG activity of the flexor pronator musculature during two distinct forearm strengthening exercises using resistance bands. It was hypothesized that two exercises would elicit at least moderate level of muscle activity, but the activation would be different in the pronator versus the flexor muscles.
Materials/Methods
10 healthy subjects (all males, age 36±12 years) were included. Surface EMG activity was measured on three muscles of the dominant-side forearm: flexor carpi ulnaris (FCP), flexor digitorum superficialis (FDS), and pronator teres (PT). After measurement of maximal voluntary contraction (MVC) for each muscle, subjects performed wrist ulnar deviation and forearm pronation exercises using elastic band resistance. Resistance was set to elicit moderate exertion (5/10 on the Borg CR10 scale). Order of exercise was randomized and three repetitions of each exercise were performed. Mean peak EMG activity in each muscle across repetitions during the eccentric phase of each exercise was calculated and expressed as a percentage of MVC. Moderate level of activity was defined as 21% of MVC or higher. Peak normalized EMG activity in each muscle was compared using two-way (exercise x muscle) repeated-measures ANOVA with post-hoc pairwise comparisons if a significant interaction was found.
Results
There was an exercise by muscle interaction effect (p<0.001). The ulnar deviation exercise selectively activated FCU (40.3%) versus FDS (19.5%, p=0.009) and PT (21.5%, p=0.022). Conversely, the pronation exercise selectively activated FDS (63.8%, p=0.002) and PT (73.0%, p=0.001) versus FDS (27.4%).
Conclusion
The ulnar deviation and pronation exercises using elastic band resistance studied targeted and activated the flexor-pronator mass musculature. The ulnar deviation and pronation exercises using elastic band resistance are practical and effective means of training the flexor-pronator mass. These exercises can be readily prescribed to athletes and patients as part of their arm care program.
Keywords: elbow, forearm, emg, overhead athlete, rehabilitation
INTRODUCTION
Overhead throwing places an extreme amount of valgus stress on the medial elbow.1,2 This valgus stress is predominantly experienced during the late cocking and acceleration phases of throwing and is primarily resisted by the anterior bundle of the ulnar collateral ligament (UCL).2,3 This repetitive stress placed upon the UCL is considered a contributing factor to the increasing rate of UCL tears.4
The maximum force that the UCL is able to resist is about 54% of the valgus force experienced during pitching.2 Therefore, it has been postulated that dynamic elbow stability is provided by the flexor-pronator musculature of the medial elbow.5–11 Specifically, the flexor carpi ulnaris (FCU), flexor digitorum superficialis (FDS), and the pronator teres (PT) have been suggested as active stabilizers of the elbow during valgus stress.5,6,8,10,11 This suggestion is based on the anatomical location of the flexor-pronator mass being in close proximity to the UCL.5,10 It has also been shown that isometric contraction of the medial forearm musculature decreases humeral-ulnar joint space during a valgus stress11 and medial elbow stability decreases with fatigue of the forearm musculature,12 further suggesting their dynamic contributions to stability.
The medial forearm musculature also demonstrates high electromyographic (EMG) activity during the throwing motion, specifically during the late cocking and early acceleration phases of pitching.13–16 These pitching phases have previously been demonstrated to involve the highest valgus stress on the medial elbow,2 leading researchers to suggest that the flexor-pronator mass provides dynamic stabilization of the medial elbow.13–15 Additionally, the forearm musculature is considered a key component to pitching accuracy and ball movement further establishing the importance of the flexor-pronator musculature to the throwing athlete.17,18
Based on the flexor-pronator musculature’s role during the throwing motion, strengthening these muscles have been deemed an important component of a rehabilitation program for overhead athletes and have a potential beneficial role of mitigating UCL injuries.5,6,8,16,19 To date, there is a paucity of evidence to suggest specific interventions that target the flexor-pronator forearm musculature. Elastic band resistance provides for a portable and convenient means of performing flexor-pronator muscle strengthening. However, the extent of EMG activity of the flexor-pronator musculature when using elastic resistance has not been reported. Therefore, the purpose of this study was to measure the extent of EMG activity of the flexor pronator musculature during two distinct forearm strengthening exercises using resistance bands. It was hypothesized that two exercises would elicit at least moderate level of muscle activity but the activation would be different between the pronator versus the flexor muscles
METHODS
Participants
Ten male subjects were recruited as a sample of convenience from the local community. All subjects were healthy at the time of testing, did not have a history of elbow or wrist pathology, and were confirmed to have normal, functional range of motion in their dominant wrist and forearm and were able to perform the tasks involved in this research study. Eight out of the ten subjects participated in regular strength training at least three times weekly; however, none of the subjects reported doing strengthening exercises specifically targeting the forearm musculature. Four out of the ten subjects had history of participation in throwing or overhead sports. Before participation in this research study, each subject provided written informed consent in accordance with institutional review board regulations (Northwell Health IRB # 19-0586)
Table 1. Subject characteristics.
| Number of subjects | 10 (all male) |
|---|---|
| Age | 36 ± 12 years |
| Height | 1.77 ± 0.04 m |
| Weight | 79 ± 5 kg |
Values are mean ± SD
Procedures
A 16-channel BTS FREEEMG 300 system, CMRR: >110 dB at 50–60 Hz; input impedance: >10 GΩ (BTS Bioengineering, Milan, Italy) was utilized for the EMG collection during this study.
Previously described anatomical landmarks for surface EMG placement were identified for FCU, FDS, and PT muscles.20,21 The subject’s exposed skin was prepared by shaving, cleaning, and lightly abrading. Disposable Ag/AgCl passive dual surface EMG electrodes (2.0 cm interelectrode distance; Noraxon, Scottsdale, AZ) were placed on the identified landmarks on the right proximal forearm of each subject (Figure 1). Muscle activity was sampled at 1000 Hz.
Figure 1. EMG Electrode Placement: (A) Pronator Teres, (B) Flexor Digitorum Superficialis, (C) Flexor Carpi Ulnaris.

Once the surface electrodes were attached to the subject, a maximum voluntary contraction (MVC) was performed, in the previously described manual muscle testing (MMT) position for each muscle.22 A single tester, a physical therapist with over 20 years of clinical experience, performed the MMT for all subjects.
Subjects then determined the level of resistance they would use for their trial by performing wrist ulnar deviation for five repetitions while holding a resistance band (Non-latex TheraBand, Hygenic Corporation, Akron, OH). The resistance band was cut to the length of each subject’s leg length, to provide extra length for wrapping around the hand. To standardize the level of resistance across the two exercises, subjects determined which resistance level elicited exertion of 5 out of 10 on the Borg CR10 Scale.23 This process was repeated for forearm pronation. Instructions were provided to each subject to ensure that there was no tension or slack in the resistance band at the start of the exercise, as elongation of the resistance band influences perceived resistance and associated muscle activity.24
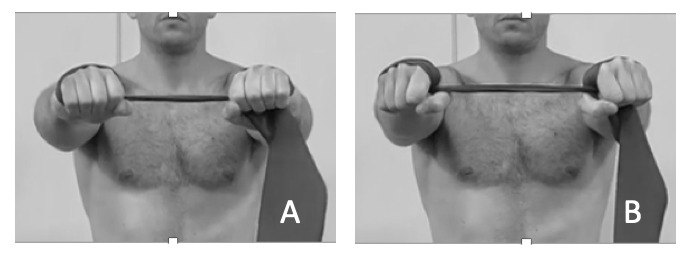
Two exercises, wrist ulnar deviation and forearm pronation were performed in random order. These exercises were included in the Evidence Based Arm Care program previously published with links to exercise videos.25 Randomization was done by pulling a card out of an opaque envelope with the exercise written on the chosen card to be done first. Wrist ulnar deviation was performed by the subject holding the resistance band with elbows extended, palms facing down, and arms held at shoulder height. The resistance band was wrapped twice around the subject’s hands, with the band resting without slack or tension when arms were kept shoulder-width apart (Figure 2A). The subject then moved his wrist into ulnar deviation (Figure 2B), performing this movement for three repetitions. The subject was asked to match movement speed to a metronome set to 20 beats/min, guiding the subject to move through a 3-second concentric phase and a 3-second eccentric phase, to enable controlled movement in both phases of the exercise.
Figure 2. Wrist ulnar deviation (A) starting position (B) end position.
Forearm pronation was performed with the subject in seated position. The resistance band was looped twice around the hand. The subject then tensioned the resistance band reaching halfway down their lower leg and stepping on the band with their right foot. Their forearm was placed on their right thigh, in supinated position, with their right wrist crease at the edge of their patella. (Figure 3A). The subject was instructed to move through the entire available range of forearm pronation motion for three repetitions (Figure 3B). Movement speed was matched to a metronome set to 20 beats/min, leading to a 3-second concentric phase and a 3-second eccentric phase.
Figure 3. Forearm pronation (A) starting position (B) end position.

Data Processing
All EMG data were processed according to previously described methods.26 Briefly, raw EMG signals were high-pass filtered at 10 Hz, full-wave rectified and smoothed using an RMS filter with a 100-ms window. For each muscle, the peak EMG activation level was identified during each exercise. The mean activation level of each muscle from 250 milliseconds before the peak to 250 milliseconds after the peak was then calculated. This was then averaged over the three repetitions for each exercise and each muscle. After processing, the EMG data were normalized to the maximum EMG activities recorded during maximal voluntary contractions (MVC) and expressed as a percent. Muscle activity level was classified according to the system of DiGiovine et al. as 0% to 20% MVC low activity, 21% to 40% MVC moderate activity, 41% to 60% MVC high activity, and greater than 60% MVC very high activity.14
Statistical Analysis
Descriptive statistics were calculated for mean normalized peak muscle activity for each muscle during each exercise. Effect of exercise and muscle on mean normalized peak EMG activity was compared using two-way (exercise x muscle) repeated-measures ANOVA. If an interaction effect was found, Bonferroni-adjusted post-hoc simple main effects were calculated. Significance level was set a priori at p = 0.05. All statistical analyses were performed using IBM SPSS Statistics 25 (IBM Corp, Armonk, NY).
RESULTS
Mean normalized muscle activity for each muscle during each exercise studied is shown in Table 2. There was an exercise by muscle interaction effect (p < 0.001). The ulnar deviation exercise selectively activated FCU (normalized peak EMG of 40.3%) versus FDS (19.5%, p = 0.009) and PT (21.5%, p = 0.022). Following the classification system of DiGiovine et al., the ulnar deviation exercise elicited moderate muscle activity in FCU, low activity in FDS, and moderate activity in PT. Conversely, the pronation exercise selectively activated FDS (63.9%, p = 0.002) and PT (73.0%, p = 0.001) versus FCU (27.4%). The pronation exercise elicited very high muscle activity in FDS and PT, and moderate muscle activity in FCU.
Table 2. Average muscle activity for the muscles and exercises studied.
| Ulnar Deviation Exercise | Pronation Exercise | |
|---|---|---|
| Flexor Carpi Ulnaris (FCU) | 40.3 ± 20.2* | 27.4 ± 11.7** |
| Flexor Digitorum Superficialis (FDS) | 19.5 ± 18.0* | 63.9 ± 31.4** |
| Pronator Teres (PT) | 21.5 ± 19.9* | 73.0 ± 32.1** |
All values are mean % MVC ± SD
* FCU significantly higher activity than FDS (p = 0.009) and PT (p = 0.022)
** FDS (p = 0.002) and PT (p = 0.001) significantly higher activity than FCU
DISCUSSION
The results of the current study demonstrate that exercises using elastic band resistance selectively targeted and elicited moderate to very high activity in the flexor-pronator musculature. The normalized peak EMG was significantly higher in the FCU compared to the FDS and PT during the ulnar deviation exercise, while the normalized peak EMG was significantly higher in the FDS and PT during the pronation exercise. Therefore, the FCU was predominantly activated during the ulnar deviation exercise, while FDS and PT were more active during the pronation exercise.
The flexor-pronator mass is an important muscle group in overhead athletes, as it provides dynamic stability to the elbow to resist valgus forces.5–11 This dynamic stabilization is critical, as pitching places high degrees of stress on the UCL,1,2 and UCL tear rates are rising.4 Additionally, the flexor-pronator muscles have high levels of activity during overhead throwing13–16 and are important toward control and velocity of pitches.17,18 Despite their role in overhead throwing, minimal evidence exists in how to effectively train these muscles and if these muscles can be targeted with strengthening exercises.
The knowledge that these exercises selectively activate the flexor-pronator muscles is important for overhead athletes, as well as strength and conditioning and rehabilitation personnel, due to the potential for increasing dynamic stability of the elbow and potentially decreasing the stress on the UCL.5,6,8,16,19 These results can influence clinical decision making as more than one exercise is required to strengthen all muscles of the flexor pronator mass and to best strengthen the dynamic stabilizers of the medial elbow.
This research study had several limitations. The study sample included only healthy male participants and this limits generalizability of its findings, particularly to injured patient populations as patients with a history of UCL injury demonstrate alterations of musculature activity.19 The cross-sectional nature of this research study precludes study of training effects of these exercises. Future studies are needed to elucidate their training effects on muscle strength, muscle activation during overhead throwing, and medial elbow stability.
CONCLUSION
The findings of the current study suggest that ulnar deviation and pronation exercise using resistance bands can target and activate the flexor-pronator mass. This information is useful for clinicians and strength and conditioning specialists who work with overhead athletes, as these exercises may be prescribed as an effective component of an arm care exercise program.
Conflict of Interest Statement
The authors declare that there is no conflict of interest.
References
- Biomechanics of the elbow during baseball pitching. Werner Sherry L., Fleisig Glenn S., Dillman Charles J., Andrews James R. Jun;1993 Journal of Orthopaedic & Sports Physical Therapy. 17(6):274–278. doi: 10.2519/jospt.1993.17.6.274. doi: 10.2519/jospt.1993.17.6.274. [DOI] [PubMed] [Google Scholar]
- Kinetics of baseball pitching with implications about injury mechanisms. Fleisig Glenn S., Andrews James R., Dillman Charles J., Escamilla Rafael F. Mar;1995 The American Journal of Sports Medicine. 23(2):233–239. doi: 10.1177/036354659502300218. doi: 10.1177/036354659502300218. [DOI] [PubMed] [Google Scholar]
- Articular and ligamentous contributions to the stability of the elbow joint. Morrey Bernard F., An Kai-Nan. Sep;1983 The American Journal of Sports Medicine. 11(5):315–319. doi: 10.1177/036354658301100506. doi: 10.1177/036354658301100506. [DOI] [PubMed] [Google Scholar]
- Prevalence of medial ulnar collateral ligament surgery in 6135 urrent professional baseball players: A 2018 Update. Leland D.P., Conte S., Flynn N.., et al. 2019Orthop J Sports Med. 7(9):2325967119871442. doi: 10.1177/2325967119871442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Functional anatomy of the flexor pronator muscle group in relation to the medial collateral ligament of the elbow. Davidson Philip A., Pink Marilyn, Perry Jacquelin, Jobe Frank W. Mar;1995 The American Journal of Sports Medicine. 23(2):245–250. doi: 10.1177/036354659502300220. doi: 10.1177/036354659502300220. [DOI] [PubMed] [Google Scholar]
- Dynamic contributions of the flexor-pronator mass to elbow valgus stability. Park Maxwell C., Ahmad Christopher S. Oct;2004 The Journal of Bone & Joint Surgery. 86(10):2268–2274. doi: 10.2106/00004623-200410000-00020. doi: 10.2106/00004623-200410000-00020. [DOI] [PubMed] [Google Scholar]
- Muscle contribution to elbow joint valgus stability. Lin Fang, Kohli Navjot, Perlmutter Sam, Lim Dohyung, Nuber Gordon W., Makhsous Mohsen. Nov;2007 Journal of Shoulder and Elbow Surgery. 16(6):795–802. doi: 10.1016/j.jse.2007.03.024. doi: 10.1016/j.jse.2007.03.024. [DOI] [PubMed] [Google Scholar]
- Effects of flexor-pronator muscle loading on valgus stability of the elbow with an intact, stretched, and resected medial ulnar collateral ligament. Udall John H., Fitzpatrick Michael J., McGarry Michelle H., Leba Thu-Ba, Lee Thay Q. Sep;2009 Journal of Shoulder and Elbow Surgery. 18(5):773–778. doi: 10.1016/j.jse.2009.03.008. doi: 10.1016/j.jse.2009.03.008. [DOI] [PubMed] [Google Scholar]
- Medial elbow injury in young throwing athletes. Gregory B., Nyland J. 2013Muscle Ligaments and Tendons Journal. 3(2):91–100. doi: 10.32098/mltj.02.2013.06. doi: 10.32098/mltj.02.2013.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The proximal origins of the flexor–pronator muscles and their role in the dynamic stabilization of the elbow joint: an anatomical study. Otoshi Kenichi, Kikuchi Shinichi, Shishido Hiroaki, Konno Shinichi. 2014Surgical and Radiologic Anatomy. 36(3):289–294. doi: 10.1007/s00276-013-1168-3. doi: 10.1007/s00276-013-1168-3. [DOI] [PubMed] [Google Scholar]
- Flexor pronator muscles' contribution to elbow joint valgus stability: ultrasonographic analysis in high school pitchers with and without symptoms. Tajika Tsuyoshi, Oya Noboru, Ichinose Tsuyoshi, Hamano Noritaka, Sasaki Tsuyoshi, Shimoyama Daisuke, Shitara Hitoshi, Yamamoto Atsushi, Kobayashi Tsutomu, Sakamoto Masaaki, Takagishi Kenji, Chikuda Hirotaka. Mar;2020 JSES International. 4(1):9–14. doi: 10.1016/j.jses.2019.10.003. doi: 10.1016/j.jses.2019.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wrist flexion exercise increases the width of the medial elbow joint space during a valgus stress test. Millard Nathaniel, DeMoss Andrew, McIlvain Gary, Beckett Joseph A., Jasko John J., Timmons Mark K. 2019Journal of Ultrasound in Medicine. 38(4):959–966. doi: 10.1002/jum.14779. doi: 10.1002/jum.14779. [DOI] [PubMed] [Google Scholar]
- An electromyographic analysis of the elbow in pitching. Sisto Domenick J., Jobe Frank W., Moynes Diane Radovich, Antonelli Daniel J. May;1987 The American Journal of Sports Medicine. 15(3):260–263. doi: 10.1177/036354658701500314. doi: 10.1177/036354658701500314. [DOI] [PubMed] [Google Scholar]
- An electromyographic analysis of the upper extremity in pitching. Digiovine Nick M., Jobe Frank W., Pink Marilyn, Perry Jacquelin. Jan;1992 Journal of Shoulder and Elbow Surgery. 1(1):15–25. doi: 10.1016/s1058-2746(09)80011-6. doi: 10.1016/s1058-2746(09)80011-6. [DOI] [PubMed] [Google Scholar]
- Dynamic stability of the elbow: electromyographic analysis of the flexor pronator group and the extensor group in pitchers with valgus instability. Hamilton Christopher D., Glousman Ronald E., Jobe Frank W., Brault John, Pink Marilyn, Perry Jacquelin. Sep;1996 Journal of Shoulder and Elbow Surgery. 5(5):347–354. doi: 10.1016/s1058-2746(96)80065-6. doi: 10.1016/s1058-2746(96)80065-6. [DOI] [PubMed] [Google Scholar]
- Surface electromyography of the forearm musculature during an overhead throwing rehabilitation progression program. Lipinski Cassandra L., Donovan Luke, McLoughlin Thomas J., Armstrong Charles W., Norte Grant E. Sep;2018 Physical Therapy in Sport. 33:109–116. doi: 10.1016/j.ptsp.2018.07.006. doi: 10.1016/j.ptsp.2018.07.006. [DOI] [PubMed] [Google Scholar]
- Sequential muscle activity and its functional role in the upper extremity and trunk during overarm throwing. Hirashima Masaya, Kadota Hiroshi, Sakurai Shizuka, Kudo Katzutoshi, Ohtsuki Tatsuyuki. Jan;2002 Journal of Sports Sciences. 20(4):301–310. doi: 10.1080/026404102753576071. doi: 10.1080/026404102753576071. [DOI] [PubMed] [Google Scholar]
- Biomechanical analysis of forearm pronation and its relationship to ball movement for the two-seam and four-seam fastball pitches. Keeley David W, Wicke Jason, Alford Ken, Oliver Gretchen D. Sep;2010 Journal of Strength and Conditioning Research. 24(9):2366–2371. doi: 10.1519/jsc.0b013e3181b22aea. doi: 10.1519/jsc.0b013e3181b22aea. [DOI] [PubMed] [Google Scholar]
- An electromyographic analysis of the elbow in normal and injured pitchers with medial collateral ligament insufficiency. Glousman Ronald E., Barron Jerry, Jobe Frank W., Perry Jacquelin, Pink Marilyn. May;1992 The American Journal of Sports Medicine. 20(3):311–317. doi: 10.1177/036354659202000313. doi: 10.1177/036354659202000313. [DOI] [PubMed] [Google Scholar]
- Recommendations for the standardization of lead positions in surface electromyography. Zipp P. 1982European Journal of Applied Physiology and Occupational Physiology. 50(1):41–54. doi: 10.1007/bf00952243. doi: 10.1007/bf00952243. [DOI] [Google Scholar]
- Surface electromyography of the forearm musculature during the windmill softball pitch. Remaley D. Trey, Fincham Bryce, McCullough Bryan, Davis Kirk, Nofsinger Charles, Armstrong Charles, Stausmire Julie M. Jan 1;2015 Orthopaedic Journal of Sports Medicine. 3(1):232596711456679. doi: 10.1177/2325967114566796. doi: 10.1177/2325967114566796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendall F.P., Kendall McCreary E., Provance P.G., Rodgers M., Romani W. Muscles: Testing and Function, with Posture and Pain. Wolters Kluwer Health; Philadelphia, PA: [Google Scholar]
- Muscle activation and perceived loading during rehabilitation exercises: comparison of dumbbells and elastic resistance. Andersen Lars L., Andersen Christoffer H., Mortensen Ole S., Poulsen Otto M., Bjørnlund Inger Birthe, Zebis Mette K. Apr 1;2010 Physical Therapy. 90(4):538–549. doi: 10.2522/ptj.20090167. doi: 10.2522/ptj.20090167. [DOI] [PubMed] [Google Scholar]
- EMG of shoulder muscles during reactive isometric elastic resistance exercises. Mullaney M.J., Perkinson C., Kremenic I., Tyler T.F., Orishimo K., Johnson C. 2017Int J Sports Phys Ther. 12(3):417–424. [PMC free article] [PubMed] [Google Scholar]
- Evidence based arm care: the throwers 10 revisited. Mullaney Michael, Nicholas Stephen, Tyler Timothy, Fukunaga Takumi, McHugh Malachy. Dec 1;2021 International Journal of Sports Physical Therapy. 16(6):1379–1386. doi: 10.26603/001c.29900. doi: 10.26603/001c.29900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effect of an eccentrically biased hamstring strengthening home program on knee flexor strength and the length-tension relationship. Orishimo Karl F., McHugh Malachy P. Mar;2015 Journal of Strength and Conditioning Research. 29(3):772–778. doi: 10.1519/jsc.0000000000000666. doi: 10.1519/jsc.0000000000000666. [DOI] [PubMed] [Google Scholar]